
Diagnosis, Investigation and Management of Patients with Acute and Chronic Myocardial Injury


Abstract
:1. Introduction
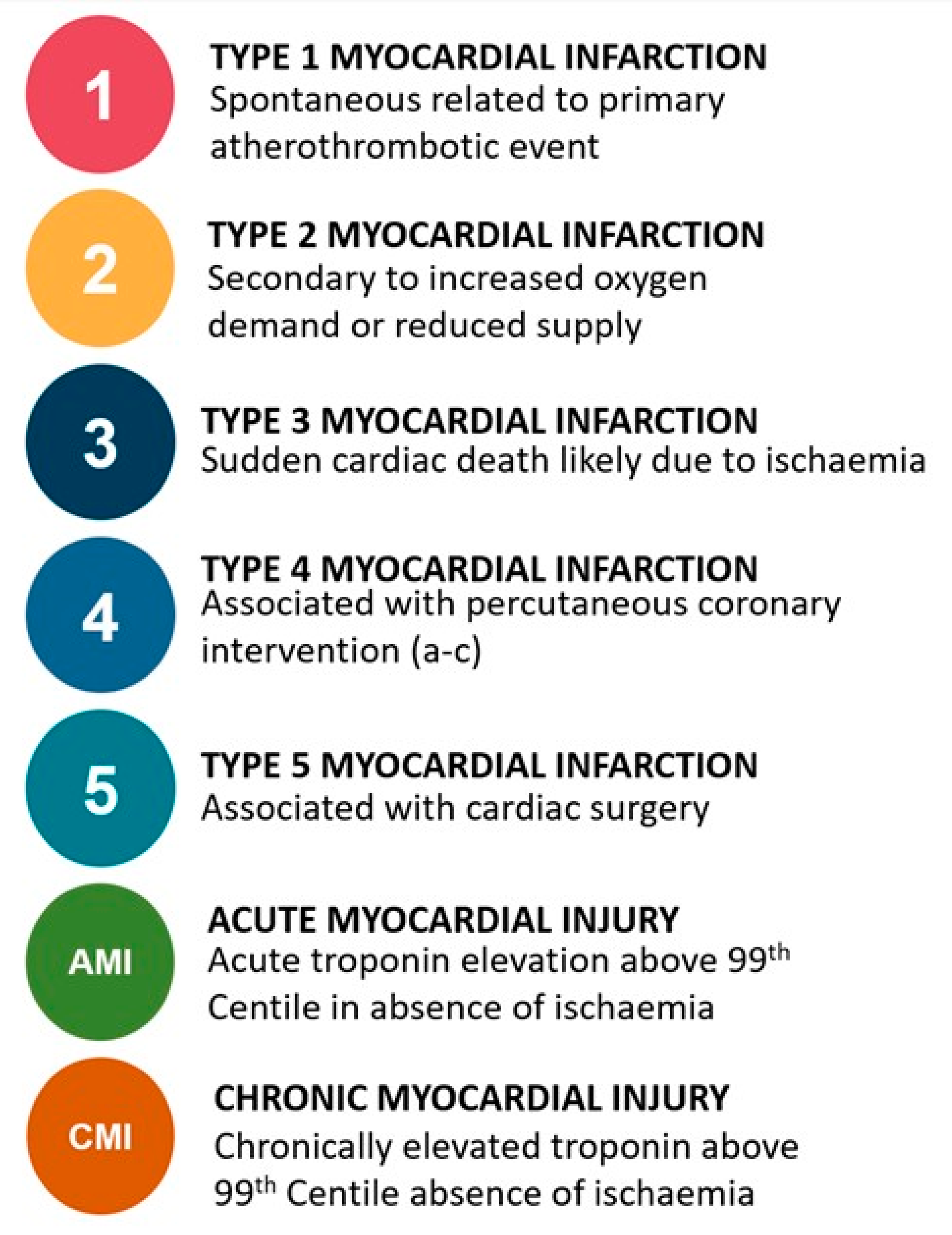
2. Classification of Myocardial Injury and Infarction
3. Detecting Myocardial Injury in Clinical Practice
4. Epidemiology of Acute and Chronic Myocardial Injury
5. Mechanisms of Myocardial Injury
5.1. Acute Myocardial Injury: Cardiac Mechanisms
5.2. Acute Myocardial Injury: Non-Cardiac Mechanisms
5.3. Chronic Myocardial Injury: Cardiac Mechanisms
5.4. Chronic Myocardial Injury: Non-Cardiac Mechanisms
6. Clinical Outcomes in Patients with Myocardial Injury
6.1. Mortality Outcomes
6.2. Cardiovascular Outcomes
7. Investigation and Management Strategies for Acute Myocardial Injury
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth universal definition of myocardial infarction. Eur Heart J. 2018, 40, 237–269. [Google Scholar] [CrossRef] [Green Version]
- Chapman, A.R.; Adamson, P.D.; Mills, N.L. Assessment and classification of patients with myocardial injury and infarction in clinical practice. Heart 2017, 103, 10–18. [Google Scholar] [CrossRef]
- Collet, J.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST elevation. Eur Heart J. 2020, ehaa575. [Google Scholar] [CrossRef]
- DeFilippis, A.P.; Chapman, A.R.; Mills, N.L.; de Lemos, J.A.; Arbab-Zadeh, A.; Newby, K.; Morrow, D.A. Assessment and Treatment of Patients With Type 2 Myocardial Infarction and Acute Nonischemic Myocardial Injury. Circulation 2019, 140, 1661–1678. [Google Scholar] [CrossRef]
- Chapman, A.R.; Shah, A.S.V.; Lee, K.K.; Anand, A.; Francis, O.; Adamson, P.; McAllister, D.A.; Strachan, F.E.; Newby, D.E.; Mills, N.L. Long-Term Outcomes in Patients with Type 2 Myocardial Infarction and Myocardial Injury. Circulation 2018, 137, 1236–1245. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, Y.; Jaffe, A.S. Type 2 Myocardial Infarction. J. Am. Coll. Cardiol. 2019, 73, 1846–1860. [Google Scholar] [CrossRef]
- Danese, E.; Montagnana, M. An historical approach to the diagnostic biomarkers of acute coronary syndrome. Ann. Transl. Med. 2016, 4, 194–205. [Google Scholar] [CrossRef] [Green Version]
- Ebashi, S. Third Component Participating in the Superprecipitation of “Natural Actomyosin. Nature 1963, 200, 1010. [Google Scholar] [CrossRef] [PubMed]
- Brekke, C.J.; Greaser, M.L. Separation and Characterization of the Troponin from Bovine Cardiac Muscle. J. Biol. Chem. 1976, 251, 866–871. [Google Scholar] [CrossRef]
- Cummins, B.; Auckland, M.L.; Cummins, P.; Birmingham, P.D. Cardiac-specific troponin radioimmunoassay in the diagnosis of acute myocardial infarction. Am. Heart J. 1987, 113, 1333–1344. [Google Scholar] [CrossRef]
- Park, K.C.; Gaze, D.C.; Collinson, P.O.; Marber, M.S. Cardiac troponins: From myocardial infarction to chronic disease. Cardiovasc. Res. 2017, 113, 1708–1718. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, O.; Bhardwaj, R.D.; Bernard, S.; Zdunek, S.; Barnabé-Heider, F.; Walsh, S.; Zupicich, J.; Alkass, K.; Buchholz, B.A.; Druid, H.; et al. Evidence for Cardiomyocyte Renewal in Humans. Science 2009, 324, 98–102. [Google Scholar] [CrossRef] [Green Version]
- White, H.D. Pathobiology of Troponin Elevations. Do Elevations Occur with Myocardial Ischemia as Well as Necrosis? J. Am. Coll. Cardiol. 2011, 57, 2406–2408. [Google Scholar] [CrossRef] [Green Version]
- Árnadóttir, Á.; Pedersen, S.; Hasselbalch, R.B.; Goetze, J.P.; Friis-Hansen, L.J.; Bloch-Münster, A-M.; Jensen, J.S.; Bundgaard, H.; Iversen, K. Temporal Release of High-Sensitivity Cardiac Troponin T and I and Copeptin After Brief Induced Coronary Artery Balloon Occlusion in Humans. Circulation 2021, 143, 1095–1104. [Google Scholar] [CrossRef]
- Apple, F.S.; Collinson, P.O. Analytical Characteristics of High-Sensitivity Cardiac Troponin Assays: For the IFCC Task Force on Clinical Applications of Cardiac Biomarkers. Clin. Chem. 2012, 58, 54–61. [Google Scholar] [CrossRef] [Green Version]
- Apple, F.S.; Ler, R.; Murakami, M.M. Determination of 19 Cardiac Troponin I and T Assay 99th Percentile Values from a Common Presumably Healthy Population. Clin. Chem. 2012, 58, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Anand, A.; Shah, A.S.V.; Beshiri, A.; Jaffe, A.S.; Mills, N.L. Global Adoption of High-Sensitivity Cardiac Troponins and the Universal Definition of Myocardial Infarction. Clin. Chem. 2019, 65, 484–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apple, F.S.; Wu, A.H.B.; Sandoval, Y.; Sexter, A.; Love, S.A.; Myers, G.; Schulz, K.; Show-Hong, D.; Christenson, R.H. Sex-Specific 99th Percentile Upper Reference Limits for High Sensitivity Cardiac Troponin Assays Derived Using a Universal Sample Bank. Clin. Chem. 2020, 66, 434–444. [Google Scholar] [CrossRef]
- Sarkisian, L.; Saaby, L.; Poulsen, T.S.; Gerke, O.; Jangaard, N.; Hosbond, S.; Diederichsen, A.C.P.; Thygesen, K.; Mickley, H.; Diederichsen, A.C.P. Clinical Characteristics and Outcomes of Patients with Myocardial Infarction, Myocardial Injury, and Nonelevated Troponins. Am. J. Med. 2016, 129, 446.e5–446.e21. [Google Scholar] [CrossRef] [PubMed]
- Smilowitz, N.R.; Subramanyam, P.; Gianos, E.; Reynolds, H.R.; Shah, B.; Sedlis, S.P. Treatment and Outcomes of Type 2 Myocardial Infarction and Myocardial Injury Compared to Type 1 Myocardial Infarction. Coron. Artery Dis. 2018, 29, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Chapman, A.R.; Admanson, P.D.; Shah, A.S.V.; Anand, A.; Strachan, F.E.; Ferry, A.V.; Lee, K.K.; Berry, C.; Findlay, I.; Cruikshank, A.; et al. High-Sensitivity Cardiac Troponin and the Universal Definition of Myocardial Infarction. Circualtion 2020, 141, 161–171. [Google Scholar] [CrossRef]
- Kadesjö, E.; Roos, A.; Siddiqui, A.; Desta, L.; Lundbäck, M.; Holzmann, M.J. Acute versus chronic myocardial injury and long term outcomes. Heart 2019, 105, 1905–1912. [Google Scholar] [CrossRef] [PubMed]
- Kadesjö, E.; Roos, A.; Siddiqui, A.J.; Sartipy, U.; Holzmann, M.J. Causes of Death in Patients with Acute and Chronic Myocardial Injury. Am. J. Med. 2020, 133, 590–598. [Google Scholar] [CrossRef]
- Bardají, A.; Bonet, G.; Carrasquer, A.; Gonz, M.; Ali, S.; Boqu, C. Clinical Features and Prognosis of Patients with Acute and Chronic Myocardial Injury Admitted to the Emergency Department. Am. J. Med. 2019, 132, 614–621. [Google Scholar] [CrossRef]
- Sandoval, Y.; Smith, S.W.; Sexter, A.; Thordsen, S.E.; Bruen, C.A.; Carlson, M.D.; Dodd, K.W.; Driver, B.E.; Hu, Y.; Jacoby, K.; et al. Type 1 and 2 Myocardial Infarction and Myocardial Injury: Clinical Transition to High-Sensitivity Cardiac Troponin, I. Am. J. Med. 2017, 130, 1431–1439.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cediel, G.; Gonzalez-del-Hoyo, M.; Carrasquer, A.; Sanchez, R.; Boqué, C.; Bardají, A. Outcomes with type 2 myocardial infarction compared with non-ischaemic myocardial injury. Heart 2017, 103, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.S.V.; McAllister, D.A.; Mills, R.; Lee, K.; Churchhouse, A.M.D.; Fleming, K.M.; Layden, E.; Anand, A.; Fersia, O.; Joshi, N.; et al. Sensitive Troponin Assay and the Classification of Myocardial Infarction. Am. J. Med. 2015, 128, 493–501.e3. [Google Scholar] [CrossRef] [Green Version]
- Meigher, S.; Thode, H.C.; Peacock, W.F.; Bock, J.L.; Gruberg, L.; Singer, A.J. Causes of Elevated Cardiac Troponins in the Emergency Department and their associated mortality. Acedemic Emerg. Med. 2016, 23, 1267–1273. [Google Scholar] [CrossRef]
- Lee, K.K.; Noaman, A.; Vaswani, A.; Gibbins, M.; Griffiths, M.; Chapman, A.R.; Strachan, F.E.; Anand, A.; McAllister, D.A.; Newby, D.E.; et al. Prevalence, Determinants, and Clinical Associations of High-Sensitivity Cardiac Troponin in Patients Attending Emergency Departments. Am. J. Med. 2018, 132, 110-e8. [Google Scholar] [CrossRef] [Green Version]
- Lambrecht, S.; Sarkisian, L.; Saaby, L.; Poulsen, T.S.; Thygesen, K.; Mickley, H. Different Causes of Death in Patients with Myocardial Infarction Type 1, Type 2, and Myocardial Injury. Am. J. Med. 2018, 131, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.S.V.; Sandoval, Y.; Noaman, A.; Sexter, A.; Vaswani, A.; Smith, S.W.; Gibbins, M.; Griffiths, M.; Chapman, A.R.; Strachan, E.F. Patient selection for high sensitivity cardiac troponin testing and diagnosis of myocardial infarction: Prospective cohort study. BMJ 2017, 359, j4788. [Google Scholar]
- Peacock IV, W.F.; De Marco, T.; Fonarow, G.C.; Diercks, D.; Wynne, J.; Apple, F.S.; Wu, A.H.B. Cardiac troponin and outcome in acute heart failure. N. Engl. J. Med. 2008, 358, 2117–2126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selvanayagam, J.B.; Petersen, S.E.; Francis, J.M.; Robson, M.D.; Kardos, A.; Neubauer, S.; Taggart, D. Effects of Off-Pump Versus On-Pump Coronary Surgery on Reversible and Irreversible Myocardial Injury. Circulation 2004, 109, 345–350. [Google Scholar] [CrossRef] [Green Version]
- Müllner, M.; Oschatz, E.; Sterz, F.; Pirich, C.; Exner, M.; Schörkhuber, W.; Laggner, A.N.; Hirschl, M.M. The influence of chest compressions and external defibrillation on the release of creatine kinase-MB and cardiac troponin T in patients resuscitated from out-of-hospital cardiac arrest. Resuscitation 1998, 38, 99–105. [Google Scholar] [CrossRef]
- Agewall, S.; Giannitsis, E.; Jernberg, T.; Katus, H. Troponin elevation in coronary vs. non-coronary disease. Eur. Heart J. 2011, 32, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Brandt, R.R.; Filzmaier, K.; Hanrath, P. Circulating Cardiac Troponin I in Acute Pericarditis. Am. J. Cardiol. 2001, 87, 1326–1328. [Google Scholar] [CrossRef]
- Siciliano, R.F.; Gualandro, D.M.; Sommer-Bittencourt, M.; Paixão, M.; Marcondes-Braga, F.; de Matos Soeiro, A.; Strunz, C.; Pacanaro, A.P.; Puelacher, C.; Tarasoutchi, F.; et al. Biomarkers for prediction of mortality in left-sided infective endocarditis. Int. J. Infect. Dis. 2020, 96, 25–30. [Google Scholar] [CrossRef]
- Fröhlich, G.M.; Schoch, B.; Schmid, F.; Keller, P.; Sudano, I.; Lüscher, T.F.; Noll, G.; Ruschitzka, F.; Enseleit, F. Takotsubo cardiomyopathy has a unique cardiac biomarker profile: NT-proBNP/myoglobin and NT-proBNP/troponin T ratios for the differential diagnosis of acute coronary syndromes and stress induced cardiomyopathy. Int. J. Cardiol. 2012, 154, 328–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharkey, S.W.; Lesser, J.R.; Menon, M.; Parpart, M.; Maron, M.S.; Maron, B.J. Spectrum and Significance of Electrocardiographic Patterns, Troponin Levels, and Thrombolysis in Myocardial Infarction Frame Count in Patients With Stress (Tako-tsubo) Cardiomyopathy and Comparison to Those in Patients With ST- Elevation Anterior Wall. Am. J. Cardiol. 2008, 101, 1723–1728. [Google Scholar] [CrossRef]
- Ammirati, E.; Frigerio, M.; Adler, E.D.; Basso, C.; Birnie, D.H.; Brambatti, M.; Freidrich, M.G.; Klingel, K.; Lehtonen, J.; Moslehi, J.J.; et al. Management of Acute Myocarditis and Chronic Inflammatory Cardiomyopathy. Circ. Hear. Fail. 2020, 13, e007405. [Google Scholar] [CrossRef] [PubMed]
- Vagnarelli, F.; Corsini, A.; Bugani, G.; Lorenzini, M.; Longhi, S.; Letizia, M.; Biagini, E.; Graziosi, M.; Cinti, L.; Norscini, G.; et al. Troponin T elevation in acute aortic syndromes: Frequency and impact on diagnostic delay and misdiagnosis. Eur. Hear. J. Acute Cardiovasc. Care 2016, 5, 61–71. [Google Scholar] [CrossRef]
- Woods, D.R.; O’Hara, J.P.; Boos, C.J.; Hodkinson, P.D.; Tsakirides, C.; Hill, N.E.; Jose, D.; Hawkins, A.; Phillipson, K.; Hazelrigg, A.; et al. Markers of physiological stress during exercise under conditions of normoxia, normobaric hypoxia, hypobaric hypoxia, and genuine high altitude. Eur. J. Appl. Physiol. 2017, 117, 893–900. [Google Scholar] [CrossRef] [Green Version]
- Konstantinides, S.V.; Becattini, C.; Meyer, G.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed]
- Lankeit, M.; Jiménez, D.; Kostrubiec, M.; Dellas, C.; Hasenfuss, G.; Pruszczyk, P.; Konstantinides, S.V. Predictive Value of the High-Sensitivity Troponin T Assay and the Simplified Pulmonary Embolism Severity Index in Heamodynamically Stable Patients with Acute Pulmonary Embolism. Circulation 2011, 124, 2716–2724. [Google Scholar] [CrossRef] [Green Version]
- Jensen, J.K.; Kristensen, S.R.; Bak, S.; Atar, D.; Høilund-Carlsen, P.F.; Mickley, H. Frequency and Significance of Troponin T Elevation in Acute Ischemic Stroke. Am. J. Cardiol. 2007, 99, 108–112. [Google Scholar] [CrossRef]
- Salem, R.; Vallée, F.; Dépret, F.; Callebert, J.; Maurice, J.P.S.; Marty, P.; Matéo, J.; Madadaki, C.; Houdart, E.; Bresson, D.; et al. Subarachnoid hemorrhage induces an early and reversible cardiac injury associated with catecholamine release: One-week follow-up study. Crit. Care 2014, 18, 558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madan, N.; Lee, A.K.; Matsushita, K.; Hoogeveen, R.C.; Ballantyne, C.M.; Selvin, E.; McEvoy, J.W. Relation of Isolated Systolic Hypertension and Pulse Pressure to High Sensitivity Cardiac Troponin-T and N-terminal pro-B-type natriuretic peptide in Older Adults (From the Atherosclerosis Risk in Communities Study). Am. J. Cardiol. 2019, 124, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Ammann, P.; Fehr, T.; Minder, E.I.; Günter, C.; Bertel, O. Elevation of troponin I in sepsis and septic shock. Intensive Care Med. 2001, 27, 965–969. [Google Scholar] [CrossRef]
- Altmann, D.R.; Korte, W.; Maeder, M.T.; Fehr, T.; Haager, P.; Rickli, H. Elevated Cardiac Troponin I in Sepsis and Septic Shock: No Evidence for Thrombus Associated Myocardial Necrosis. PLoS ONE 2010, 5, e9017. [Google Scholar] [CrossRef]
- Gunnewiek, K.J.M.T.; Van der Leur, J.J.J.P.M. Elevated troponin T concentrations in critically ill patients. Intensive Care Med. 2003, 29, 2317–2322. [Google Scholar] [CrossRef]
- Adamcová, M.; Šterba, M.; Šimunek, T.; Potácová, A.; Mazurová, Y.; Geršl, V. Troponin as a marker of myocardiac damage in drug-induced cardiotoxicity Troponin as a marker of myocardiac damage in drug-induced cardiotoxicity. Expert Opin. Drug Saf. 2005, 4, 457–472. [Google Scholar] [CrossRef] [PubMed]
- Sedaghat-Hamedani, F.; Kayvanpour, E.; Frankenstein, L.; Mereles, D.; Amr, A.; Buss, A.S.; Keller, C.; Giannitsis, E.; Jensen, K.; Katus, H.A.; et al. Review Biomarker Changes after Strenuous Exercise Can Mimic Pulmonary Embolism and Cardiac Injury—A Metaanalysis of 45 Studies. Clin. Chem. 2015, 61, 1246–1255. [Google Scholar] [CrossRef] [Green Version]
- Marshall, L.; Lee, K.K.; Stewart, S.D.; Wild, A.; Fujisawa, T.; Ferry, A.V.; Stables, C.L.; Lithgow, H.; Chapman, A.R.; Anand, A.; et al. Effect of Exercise Intensity and Duration on Cardiac Troponin Release. Circulation 2020, 141, 83–85. [Google Scholar] [CrossRef]
- Kaleta-Duss, A.M.; Lewicka-Potocka, Z.; Dabrowska-Kugacka, A.; Raczak, G.; Lewicka, E. Myocardial Injury and Overload among Amateur Marathoners as Indicated by Changes in Concentrations of Cardiovascular Biomarkers. Int. J. Environ. Res. Public Health 2020, 17, 6191. [Google Scholar] [CrossRef] [PubMed]
- Zebrowska, A.; Waskiewicz, Z.; Nikolaidis, P.T.; Mikołajczyk, R.; Kawecki, D.; Rosemann, T.; Knechtle, B. Acute Responses of Novel Cardiac Biomarkers to a 24-h Ultra-Marathon. J. Clin. Med. 2019, 8, 57. [Google Scholar] [CrossRef] [Green Version]
- Roca, E.; Nescolarde, L.; Lupón, J.; Barallat, J.; Januzzi, J.L.; Liu, P.; Pastor, M.C.; Bayes-Genis, A. The Dynamics of Cardiovascular Biomarkers in non-Elite Marathon Runners. J. Cardiovasc. Trans. Res. 2017, 10, 206–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Punukollu, G.; Gowda, R.M.; Khan, I.A.; Mehta, N.J.; Navarro, V.; Vasavada, B.C.; Sachi, T.J. Elevated serum cardiac troponin I in rhabdomyolysis. Int. J. Cardiol. 2004, 96, 35–40. [Google Scholar] [CrossRef]
- Giger, R.D.; du Fay de Lavallaz, J.; Prepoudis, A.; Stoll, T.; Lopez-Ayala, P.; Glarner, N.; Boeddinghaus, J.; Puelacher, C.; Nestelberger, T.; Mueller, C. Rhabdomyolysis A Noncardiac Source of Increased Circulating Concentrations of Cardiac Troponin T? J. Am. Coll. Cardiol. 2020, 76, 2685–2687. [Google Scholar] [CrossRef] [PubMed]
- Aengevaeren, V.L.; Froeling, M.; Hooijmans, M.T.; Monte, J.R.; Van denBerg-Faay, S.; Hopman, M.T.E.; Eijsvogels, T.M.H. Myocardial Injury and Compromised Cardiomyocyte Integrity Following a Marathon Run. JACC Cardiovasc. Imaging 2020, 13, 1445–1447. [Google Scholar] [CrossRef]
- Aengevaeren, V.L.; Hopman, M.T.E.; Thompson, P.D.; Bakker, E.A.; George, K.P.; Thijssen, D.H.J.; Strijkers, G.J.; Nederveen, A.J.; Bakermans, A.J.; Eijsvogels, T.M.H. Exercise-Induced Cardiac Troponin I Increase and Incident Mortality and Cardiovascular Events. Circulation 2019, 140, 804–814. [Google Scholar] [CrossRef] [PubMed]
- Missov, E.; Mair, J. A novel biochemical approach to congestive heart failure: Cardiac troponin T. Am. Heart J. 1999, 138, 95–99. [Google Scholar] [CrossRef]
- Nagarajan, V.; Hernandez, A.V.; Wilson Tang, W.H. Prognostic value of cardiac troponin in chronic stable heart failure: A systematic review. Heart 2012, 98, 1778–1786. [Google Scholar] [CrossRef]
- Sato, Y.; Yamada, T.; Taniguchi, R.; Nagai, K.; Makiyama, T.; Okada, H.; Kataoka, K.; Ito, H.; Matsumori, A.; Sasayama, S. Persistently increased serum concentrations of cardiac troponin T in patients with idiopathic dilated cardiomyopathy are predictive of adverse outcomes. Circulation 2001, 103, 369–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, Y.; Taniguchi, R.; Nagai, K.; Makiyama, T.; Okada, H.; Yamada, T.; Matsumori, A.; Takatsu, Y. Measurements of cardiac troponin T in patients with hypertrophic cardiomyopathy. Heart 2003, 89, 659–660. [Google Scholar] [CrossRef]
- Baba, Y.; Kubo, T.; Kitaoka, H.; Okawa, M.; Yamanaka, S.; Kawada, Y.; Yamasaki, N.; Matsumura, Y.; Furuno, T.; Sugiura, T.; et al. Usefulness of high-sensitive cardiac troponin T for evaluating the activity of cardiac sarcoidosis. Int. Heart J. 2012, 53, 287–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dispenzieri, A.; Kyle, R.A.; Gertz, M.A.; Therneau, T.M.; Miller, W.L.; Chandrasekaran, K.; McConnell, J.P.; Burritt, M.F.; Jaffe, A. Survival in patients with primary systemic amyloidosis and raised serum cardiac troponins. Lancet 2003, 361, 1787–1789. [Google Scholar] [CrossRef]
- Aeschbacher, S.; Schoen, T.; Bossard, M.; Van Der Lely, S; Glättli, K.; Todd, J.; Estis, J.; Risch, M.; Mueller, C.; Risch, L.; et al. Relationship Between High-Sensitivity Cardiac Troponin I and Blood Pressure Among Young and Healthy Adults. Am. J. Hypertens. 2015, 28, 789–796. [Google Scholar] [CrossRef] [Green Version]
- Moss, A.; Dweck, M.; Doris, M.; Andrews, J.; Bing, R.; Forsythe, R.O.; Cartlidge, T.R.; Pawade, T.; Daghem, M.; Raftis, J.B.; et al. Ticagrelor to Reduce Myocardial Injury in Patients with High-Risk Coronary Artery Plaque. JACC Cardiovasc Imaging 2020, 13, 1549–1560. [Google Scholar] [CrossRef] [PubMed]
- Ford, I.; Shah, A.S.V.; Zhang, R.; McAllister, D.A.; Strachan, F.E.; Caslake, M.; Newby, D.E.; Packcard, C.J.; Mills, N.L. High-Sensitivity Cardiac Troponin, Statin Therapy, and Risk of Coronary Heart Disease. J. Am. Coll. Cardiol. 2016, 68, 2719–2728. [Google Scholar] [CrossRef] [PubMed]
- Eggers, K.M.; Lindahl, B. Application of Cardiac Troponin in Cardiovascular Diseases Other Than Acute Coronary Syndrome. Clin. Chem. 2017, 63, 223–235. [Google Scholar] [CrossRef]
- Parik, N.I.; Hwang, S.J.; Larson, M.G.; Meigs, J.B.; Levy, D.; Fox, C.S. Cardiovascular Disease Risk Factors in Chronic Kidney Disease. JAMA. 2006, 166, 1884–1891. [Google Scholar] [CrossRef] [Green Version]
- Plüddemann, A.; Neyen, C.; Gordon, S. Macrophage scavenger receptors and host-derived ligands. Methods 2007, 43, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Fridén, V.; Starnberg, K.; Muslimovic, A.; Ricksten, S.E.; Bjurman, C.; Forsgard, N.; Wickman, A.; Hammarsten, O. Clearance of cardiac troponin T with and without kidney function. Clin. Biochem. 2017, 50, 468–474. [Google Scholar] [CrossRef]
- Muslimovic, A.; Fridén, V.; Tenstad, O.; Starnberg, K.; Nyström, S.; Wesén, E.; Esbjörner, E.K.; Granholm, K.; Lindahl, B.; Hammarsten, O. The Liver and Kidneys mediate clearance of cardiac troponin in the rat. Sci. Rep. 2020, 10, 6791. [Google Scholar] [CrossRef] [PubMed]
- Sarkisian, L.; Saaby, L.; Poulsen, T.S.; Gerke, O. Prognostic Impact of Myocardial Injury Related to Various Cardiac and Noncardiac Conditions. Am. J. Med. 2016, 129, 506–514.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandoval, Y.; Smith, S.W.; Sexter, A.; Schulz, K.; Apple, F.S. Use of objective evidence of myocardial ischemia to facilitate the diagnostic and prognostic distinction between type 2 myocardial infarction and myocardial injury. Eur. Hear. J. Acute Cardiovasc. Care. 2018, 9, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Chin, C.W.L.; Messika-Zeitoun, D.; Shah, A.S.V.; Lefevre, G.; Bailleul, S.; Yeung, E.N.W.; Koo, M.; Mirsadraee, S.; Mathieu, T.; Semple, S.; et al. A clinical risk score of myocardial fibrosis predicts adverse outcomes in aortic stenosis. Eur. Heart J. 2016, 37, 713–723. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Lead Author and Year | Population Size | Total Incidence Myocardial Injury (Available for Adjudication) | Total Incidence Non-Ischaemic Myocardial Injury (% of Total Myocardial Injury) | Incidence Acute Myocardial Injury (%) | Incidence Chronic Myocardial Injury (%) | Patient Population | Total All-Cause Mortality Acute Myocardial Injury | Cardiovascular Outcomes and Mortality | Type 1 Myocardial Infarction Mortality (%) |
|---|---|---|---|---|---|---|---|---|---|
| 4th Definition | |||||||||
| Chapman 2020 [21] | 48,282 | 9115 | 2963 (33%) | 1676 (18%) | 1287 (14%) | Patients presenting to ED with chest pain. | 1 year Acute: 33% Chronic: 29% | 1 year CV death + MI Acute: 16% Chronic: 16% | 1 year 14% |
| Kadesjö 2019 [22] Kadesjö 2020 [23] | 22,589 | 3853 | 2491 (65%) | 1144 (30%) | 1347 (35%) | Patients presenting to ED with clinical indication, single centre with troponin >99th percentilecentile URL. | 2 year Acute: 27% Chronic: 25% 4 year Acute: 53% Chronic: 52% | Median 4.0 ± 1.3 years CV death Acute: 19% Chronic: 20% | 2 year 12% 4 year 35% |
| Bardají 2019 [24] | 3701 | - | 368 | 261 | 107 | Patients presenting to ED, clinical discretion to rule out ACS. | 4 year Acute: 48% Chronic: 54% | 4 year MACE Acute: 53% Chronic: 64% | N/A |
| 3rd Definition | |||||||||
| Cediel 2017 [25] | 3790 | 1010 | 440 (44%) | - | - | Retrospective cohort of patients presenting to ED with suspected ACS. | 2 year 40% | - | 2 year 19.7% |
| Sandoval 2017 [26] | 1640 | 497 | 280 (56%) | - | - | Unselected patients presenting to the ED with troponin measured on clinical indication. | 180 day 11% 2 year 26% | 180 day MACE: 19% | 180 day 8% 2 year 16% |
| Shah 2015 Chapman 2018 [5,27] | 2122 | 2122 | 522 (25%) | - | - | Hospitalised patients with troponins taken for clinical indication. | 1 year 37% 5 year 72% | 1 year MACE: 18% 5 year 31% | 1 year 16% 5 year 37% |
| Smilowitz 2018 [20] | Unknown | 768 | 420 (55%) | - | - | Single centre with all troponin levels taken on clinical indication that were elevated. | In hospital 9% 2 year 30% | In hospital + 2 year follow up CV death 11% | In hospital 13% 2 year 30% |
| Meigher 2016 [28] | 13,502 | 1283 | 458 (35.7%) | - | - | Single centre with patients presenting with suspected ACS. | Index hospitalisation 11% | - | Index hospitalisation 7% |
| Lee 2018 [29] | 918 | 114 | 109 (96%) | - | - | Patients presenting to ED without suspicion of ACS. | Top quartile of troponin concentrations 1 year 37.7% | - | - |
| 2nd Definition | |||||||||
| Sarkisian 2016 Lambrecht 2018 [19,30] | 3762 | 1577 | 1089 (69%) | - | - | Hospitalised patients who had troponins taken as per clinical indication. | 3.2 year median 59% | - | 3.2 year median 39% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taggart, C.; Wereski, R.; Mills, N.L.; Chapman, A.R. Diagnosis, Investigation and Management of Patients with Acute and Chronic Myocardial Injury. J. Clin. Med. 2021, 10, 2331. https://doi.org/10.3390/jcm10112331
Taggart C, Wereski R, Mills NL, Chapman AR. Diagnosis, Investigation and Management of Patients with Acute and Chronic Myocardial Injury. Journal of Clinical Medicine. 2021; 10(11):2331. https://doi.org/10.3390/jcm10112331
Chicago/Turabian StyleTaggart, Caelan, Ryan Wereski, Nicholas L. Mills, and Andrew R. Chapman. 2021. "Diagnosis, Investigation and Management of Patients with Acute and Chronic Myocardial Injury" Journal of Clinical Medicine 10, no. 11: 2331. https://doi.org/10.3390/jcm10112331