
Baseline Peritoneal Membrane Transport Characteristics Are Associated with Peritonitis Risk in Incident Peritoneal Dialysis Patients

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
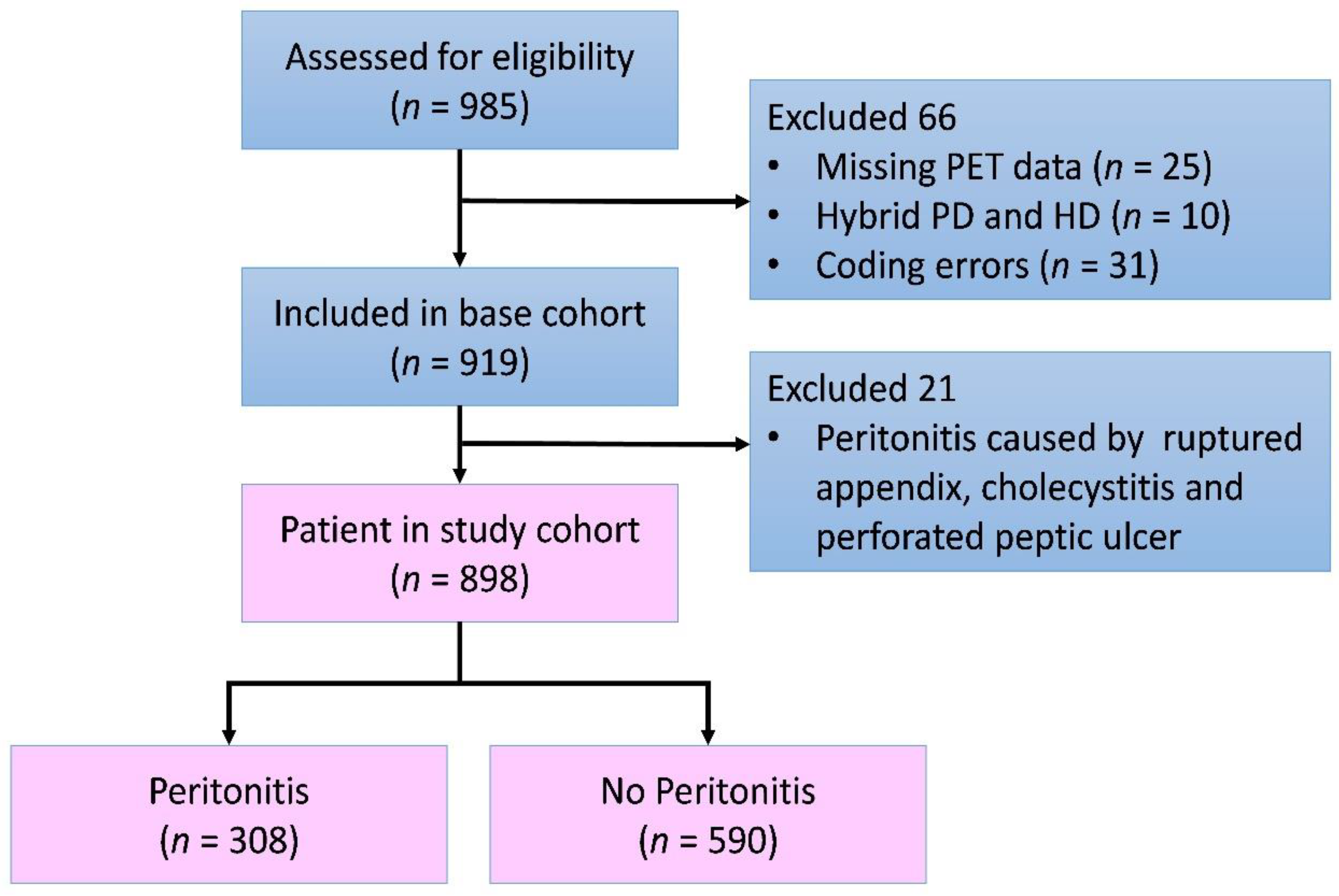
2.1. Study Design
2.2. Peritoneal-Membrane Equilibration Test
2.3. Diagnosis of Peritonitis
2.4. Statistics
3. Results
3.1. Demographics of Study Cohort
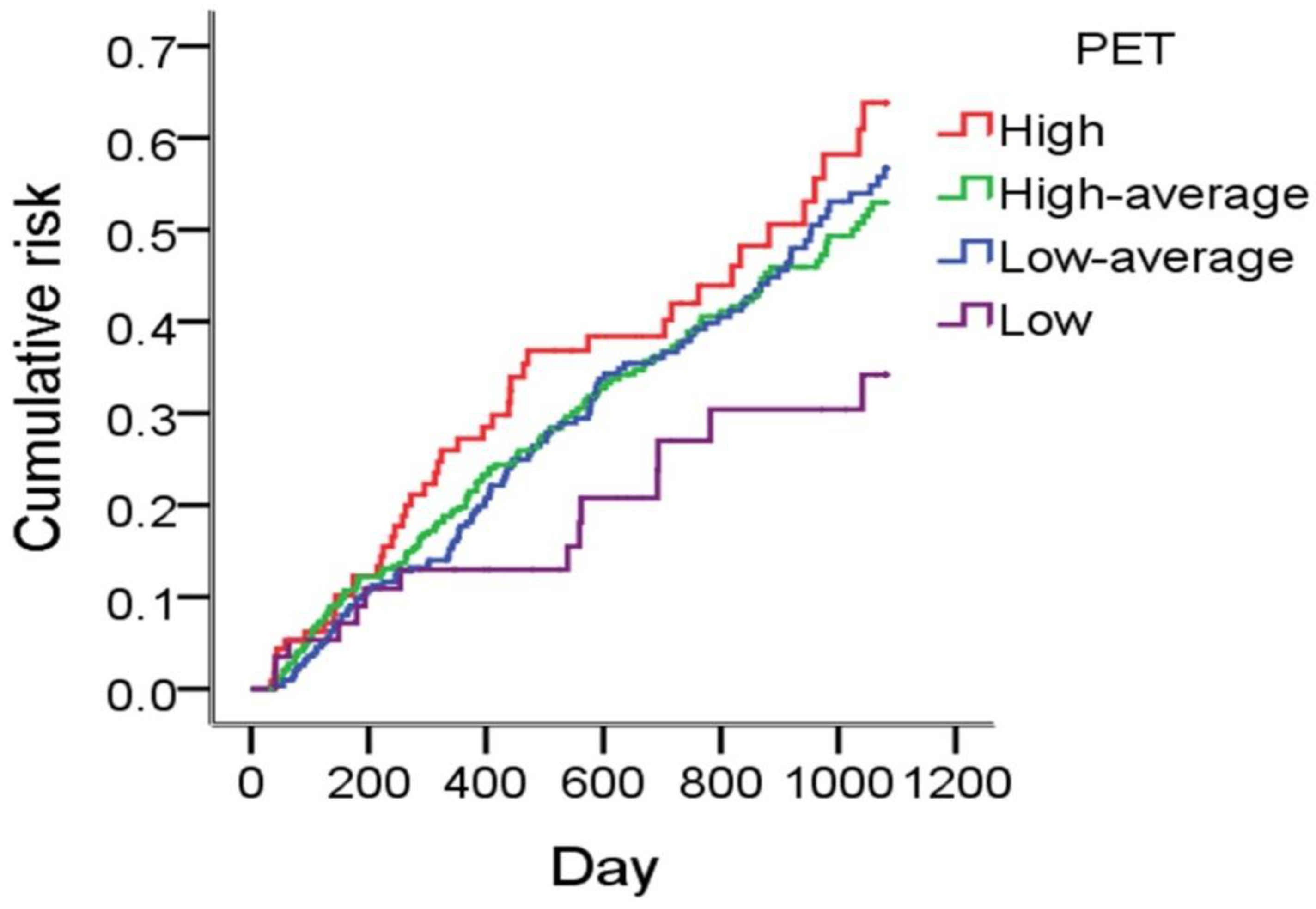
3.2. Peritoneal Membrane Transport Characteristics and Peritonitis Rate
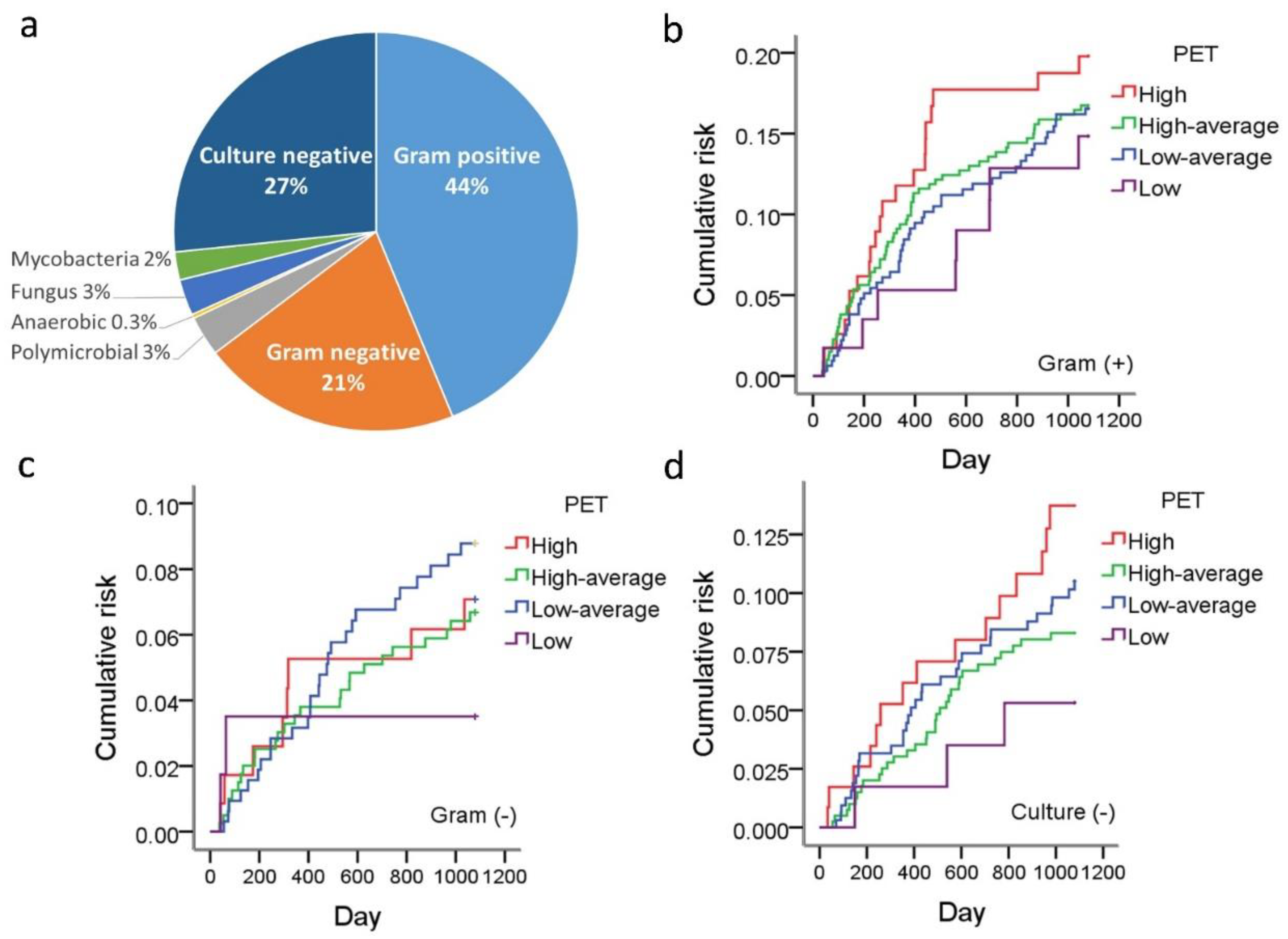
3.3. Peritoneal Membrane Transport Characteristics and Peritonitis Microbiology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PET | Peritoneal equilibration test |
| PD | PD Peritoneal dialysis |
| HR | HR hazard ratio |
| HR hazard ratio | HR hazard ratio |
| CI | Confidence interval |
| HD | Hemodialysis |
| IRB | Institute Review Board |
| WBC | White blood cells |
| H | High |
| HA | High average |
| LA | Low average |
| L | Low |
| CAPD | Continuous ambulatory peritoneal dialysis |
References
- Kalantar-Zadeh, K.; Rhee, C.M.; Joshi, S.; Brown-Tortorici, A.; Kramer, H.M. Chronic kidney disease. Lancet 2021, 309, 786–802. [Google Scholar] [CrossRef]
- El Nahas, A.M.; Bello, A.K. Chronic kidney disease: The global challenge. Lancet 2005, 365, 331–340. [Google Scholar] [CrossRef]
- Cousin Sobrinho, E.L.P.; Duncan, B.B.; Schmidt, M.I.; GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar]
- Teitelbaum, I.; Burkart, J. Peritoneal dialysis. Am. J. Kidney Dis. 2003, 42, 1082–1096. [Google Scholar] [CrossRef]
- Tokgoz, B. Clinical advantages of peritoneal dialysis. Perit. Dial. Int. 2009, 29 (Suppl. 2), S59–S61. [Google Scholar] [CrossRef]
- Teitelbaum, I. Peritoneal Dialysis. N. Engl. J. Med. 2021, 385, 1786–1795. [Google Scholar] [CrossRef]
- Karl, Z.J.T.; Khanna, O.N.R.; Leonor, B.F.P.; Ryan, P.; Moore, H.L.; Nielsen, M.P. Peritoneal equilibration test. Perit. Dial. Int. 1987, 7, 138–148. [Google Scholar] [CrossRef]
- Pannekeet, M.M.; Imholz, A.L.; Struijk, D.G.; Koomen, G.C.; Langedijk, M.J.; Schouten, N.; De Waart, R.; Hiralall, J.; Krediet, R.T. The standard peritoneal permeability analysis: A tool for the assessment of peritoneal permeability characteristics in CAPD patients. Kidney Int. 1995, 48, 866–875. [Google Scholar] [CrossRef] [Green Version]
- Trivedi, H.; Khanna, R.; Lo, W.-K.; Prowant, B.F.; Nolph, K.D. Reproducibility of the peritoneal equilibration test in CAPD patients. ASAIO J. 1994, 40, M892–M895. [Google Scholar] [CrossRef]
- Davies, S.J. Monitoring of long-term peritoneal membrane function. Perit. Dial. Int. 2001, 21, 225–230. [Google Scholar] [CrossRef]
- Boudville, N.; Kemp, A.; Clayton, P.; Lim, W.; Badve, S.V.; Hawley, C.M.; McDonald, S.P.; Wiggins, K.J.; Bannister, K.M.; Brown, F.G.; et al. Recent peritonitis associates with mortality among patients treated with peritoneal dialysis. J. Am. Soc. Nephrol. 2012, 23, 1398–1405. [Google Scholar] [CrossRef] [Green Version]
- Htay, H.; Cho, Y.; Pascoe, E.M.; Darssan, D.; Nadeau-Fredette, A.-C.; Hawley, C.; Clayton, P.A.; Borlace, M.; Badve, S.; Sud, K.; et al. Multicenter registry analysis of center characteristics associated with technique failure in patients on incident peritoneal dialysis. Clin. J. Am. Soc. Nephrol. 2017, 12, 1090–1099. [Google Scholar] [CrossRef] [Green Version]
- McDonald, S.P.; Collins, J.F.; Rumpsfeld, M.; Johnson, D.W. Obesity is a risk factor for peritonitis in the Australian and New Zealand peritoneal dialysis patient populations. Perit. Dial. Int. 2004, 24, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Nessim, S.J.; Bargman, J.M.; Austin, P.C.; Nisenbaum, R.; Jassal, S.V. Predictors of peritonitis in patients on peritoneal dialysis: Results of a large, prospective Canadian database. Clin. J. Am. Soc. Nephrol. 2009, 4, 1195–1200. [Google Scholar] [CrossRef] [Green Version]
- Ros, S.; Remón, C.; Qureshi, A.R.; Quiros, P.; Lindholm, B.; Carrero, J.J. Increased risk of fatal infections in women starting peritoneal dialysis. Perit. Dial. Int. 2013, 33, 487–494. [Google Scholar] [CrossRef] [Green Version]
- Fontán, M.P.; Rodríguez-Carmona, A.; García-Naveiro, R.; Rosales, M.; Villaverde, P.; Valdés, F. Peritonitis-related mortality in patients undergoing chronic peritoneal dialysis. Perit. Dial. Int. 2005, 25, 274–284. [Google Scholar] [CrossRef]
- Ghali, J.R.; Bannister, K.M.; Brown, F.G.; Rosman, J.B.; Wiggins, K.J.; Johnson, D.W.; McDonald, S.P. Microbiology and outcomes of peritonitis in Australian peritoneal dialysis patients. Perit. Dial. Int. 2011, 31, 651–662. [Google Scholar] [CrossRef]
- Cho, Y.; Johnson, D.W. Peritoneal dialysis-related peritonitis: Towards improving evidence, practices, and outcomes. Am. J. Kidney Dis. 2014, 64, 278–289. [Google Scholar] [CrossRef]
- Kerschbaum, J.; König, P.; Rudnicki, M. Risk factors associated with peritoneal-dialysis-related peritonitis. Int. J. Nephrol. 2012, 2012, 483250. [Google Scholar] [CrossRef] [Green Version]
- Chow, K.M.; Szeto, C.C.; Leung, C.B.; Kwan, B.C.; Law, M.C.; Li, P.K.-T. A risk analysis of continuous ambulatory peritoneal dialysis-related peritonitis. Perit. Dial. Int. 2005, 25, 374–379. [Google Scholar] [CrossRef]
- Li, P.K.-T.; Szeto, C.C.; Piraino, B.; De Arteaga, J.; Fan, S.; Figueiredo, A.E.; Fish, D.N.; Goffin, E.; Kim, Y.-L.; Salzer, W.; et al. ISPD Peritonitis Recommendations: 2016 Update on Prevention and Treatment. Perit. Dial. Int. 2016, 36, 481–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krediet, R.T. Evaluation of peritoneal membrane integrity. J. Nephrol. 1997, 10, 238–244. [Google Scholar] [PubMed]
- Devuyst, O.; Rippe, B. Water transport across the peritoneal membrane. Kidney Int. 2014, 85, 750–758. [Google Scholar] [CrossRef] [Green Version]
- Williams, J.D.; Craig, K.J.; Topley, N.; Von Ruhland, C.; Fallon, M.; Newman, G.R.; Mackenzie, R.K.; Williams, G.T. Morphologic changes in the peritoneal membrane of patients with renal disease. J. Am. Soc. Nephrol. 2002, 13, 470–479. [Google Scholar] [CrossRef]
- Davies, S.J.; Bryan, J.; Phillips, L.; Russell, G.I. Longitudinal changes in peritoneal kinetics: The effects of peritoneal dialysis and peritonitis. Nephrol. Dial. Transplant. 1996, 11, 498–506. [Google Scholar] [CrossRef]
- Churchill, D.N.; Thorpe, K.; Nolph, K.D.; Keshaviah, P.R.; Oreopoulos, D.G.; Pagé, D. Increased peritoneal membrane transport is associated with decreased patient and technique survival for continuous peritoneal dialysis patients. The Canada-USA (CANUSA) Peritoneal Dialysis Study Group. J. Am. Soc. Nephrol. 1998, 9, 1285–1292. [Google Scholar] [CrossRef]
- Mehrotra, R.; Ravel, V.; Streja, E.; Kuttykrishnan, S.; Adams, S.V.; Katz, R.; Molnar, M.Z.; Kalantar-Zadeh, K. Peritoneal equilibration test and patient outcomes. Clin. J. Am. Soc. Nephrol. 2015, 10, 1990–2001. [Google Scholar] [CrossRef] [Green Version]
- So, S.; Aw, L.; Sud, K.; Lee, V.W. Membrane transport status does not predict peritonitis risk in patients on peritoneal dialysis. Nephrology 2018, 23, 633–639. [Google Scholar] [CrossRef]
- Wu, H.; Huang, R.; Yi, C.; Wu, J.; Guo, Q.; Zhou, Q.; Yu, X.; Yang, X. Risk factors for early-onset peritonitis in Southern Chinese peritoneal dialysis patients. Perit. Dial. Int. 2016, 36, 640–646. [Google Scholar] [CrossRef]
- Wanten, G.J.; Van Oost, P.; Schneeberger, P.M.; Koolen, M.I. Nasal carriage and peritonitis by Staphylococcus aureus in patients on continuous ambulatory peritoneal dialysis: A prospective study. Perit. Dial. Int. 1996, 16, 352–356. [Google Scholar] [CrossRef] [Green Version]
- Russo, R.; Manili, L.; Tiraboschi, G.; Amar, K.; De Luca, M.; Alberghini, E.; Ghiringhelli, P.; De Vecchi, A.; Porri, M.; Marinangeli, G.; et al. Patient re-training in peritoneal dialysis: Why and when it is needed. Kidney Int. 2006, 70, S127–S132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, K.M.; Szeto, C.C.; Law, M.C.; Fung, J.S.F.; Kam-Tao Li, P. Influence of peritoneal dialysis training nurses’ experience on peritonitis rates. Clin. J. Am. Soc. Nephrol. 2007, 2, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Holloway, M.; Mujais, S.; Kandert, M.; Warady, B.A. Pediatric peritoneal dialysis training: Characteristics and impact on peritonitis rates. Perit. Dial. Int. 2001, 21, 401–404. [Google Scholar] [CrossRef]
- Cho, J.-H.; Hur, I.-K.; Kim, C.-D.; Park, S.-H.; Ryu, H.-M.; Yook, J.-M.; Choi, J.-Y.; Choi, H.J.; Park, J.-W.; Do, J.-Y.; et al. Impact of systemic and local peritoneal inflammation on peritoneal solute transport rate in new peritoneal dialysis patients: A 1-year prospective study. Nephrol. Dial. Transplant. 2010, 25, 1964–1973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, Y.; Johnson, D.W.; Vesey, D.A.; Hawley, C.M.; Pascoe, E.M.; Clarke, M.; Topley, N. Dialysate interleukin-6 predicts increasing peritoneal solute transport rate in incident peritoneal dialysis patients. BMC Nephrol. 2014, 15, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.; Heimburger, O.; Cheng, H.H.; Bergstrom, J.; Lindholm, B. Does a high peritoneal transport rate reflect a state of chronic inflammation? Perit. Dial. Int. 1999, 19, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Lambie, M.; Chess, J.; Williams, A.; Do, J.Y.; Topley, N.; Davies, S.J. Peritoneal protein clearance is a function of local inflammation and membrane area whereas systemic inflammation and comorbidity predict survival of incident peritoneal dialysis patients. Front. Physiol. 2019, 10, 105. [Google Scholar] [CrossRef]
- Sawai, A.; Ito, Y.; Mizuno, M.; Suzuki, Y.; Toda, S.; Ito, I.; Hattori, R.; Matsukawa, Y.; Gotoh, M.; Takei, Y.; et al. Peritoneal macrophage infiltration is correlated with baseline peritoneal solute transport rate in peritoneal dialysis patients. Nephrol. Dial. Transplant. 2010, 26, 2322–2332. [Google Scholar] [CrossRef] [Green Version]
- Pecoits-Filho, R.; Araújo, M.R.T.; Lindholm, B.; Stenvinkel, P.; Abensur, H.; Romão, J.E.; Marcondes, M.; De Oliveira, A.H.F.; Noronha, I.L. Plasma and dialysate IL-6 and VEGF concentrations are associated with high peritoneal solute transport rate. Nephrol. Dial. Transplant. 2002, 17, 1480–1486. [Google Scholar] [CrossRef] [Green Version]
- Guedes, A.M. Peritoneal protein loss, leakage or clearance in peritoneal dialysis, where do we stand? Perit. Dial. Int. 2019, 39, 201–209. [Google Scholar] [CrossRef]
- Lu, W.; Pang, W.-F.; Jin, L.; Li, H.; Chow, K.M.; Kwan, B.C.; Leung, C.B.; Li, P.K.-T.; Szeto, C.C. Peritoneal protein clearance predicts mortality in peritoneal dialysis patients. Clin. Exp. Nephrol. 2018, 23, 551–560. [Google Scholar] [CrossRef] [PubMed]
- Cooper, S.; Iliescu, E.A.; Morton, A.R. The relationship between dialysate protein loss and membrane transport status in peritoneal dialysis patients. Adv. Perit. Dial. 2001, 17, 244–247. [Google Scholar] [PubMed]
- Andronesi, A.; Iliuta, L.; Patruleasa, M.; Achim, C.; Ismail, G.; Bobeica, R.; Rusu, E.; Zilisteanu, D.; Andronesi, D.; Motoi, O.; et al. Predictive factors for coronary artery disease among peritoneal dialysis patients without diabetic nephropathy. Maedica 2012, 7, 227–235. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Overall | H | HA | LA | L |
|---|---|---|---|---|---|
| Patients (n) | 898 | 117 | 402 | 321 | 58 |
| Age (%) <20 20–39 40–59 60–79 ≧80 | 0.9 21.5 43.9 30.5 3.2 | 0 17.9 39.3 39.4 3.4 | 1.0 22.6 43.8 28.1 4.5 | 0.6 20.9 47.4 29.3 1.8 | 3.4 24.1 34.5 36.2 1.8 |
| Gender (% men) | 46.2 | 57.3 | 49.8 | 40.2 | 32.8 |
| Diabetes mellitus (%) | 41.9 | 56.4 | 43.0 | 34.9 | 43.1 |
| Hypertension (%) | 63.0 | 63.2 | 63.2 | 64.2 | 55.2 |
| Coronary artery disease (%) | 3.6 | 2.6 | 3.7 | 3.4 | 6.9 |
| Congestive heart failure (%) | 5.2 | 3.4 | 6.5 | 4.7 | 3.4 |
| Cirrhosis (%) | 1.7 | 5.1 | 1.7 | 0.3 | 1.7 |
| Malignancy (%) | 2.0 | 4.3 | 1.7 | 1.6 | 1.7 |
| Modality at initiation of PD (% CAPD) | 90.3 | 85.5 | 91.0 | 91.0 | 91.4 |
| Serum albumin (g/dL) | 3.7 ± 0.6 | 3.7 ± 0.6 | 3.7 ± 0.6 | 3.7 ± 0.6 | 3.7 ± 0.6 |
| Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | |
| PET L | Reference | - | - | Reference | - | - |
| LA | 1.72 | 0.99–3.02 | 0.057 | 1.71 | 0.98–2.99 | 0.060 |
| HA | 1.59 | 0.91–2.76 | 0.105 | 1.61 | 0.93–2.81 | 0.091 |
| H | 1.90 | 1.04–3.50 | 0.038 | 1.98 | 1.08–3.62 | 0.026 |
| Coronary artery disease | 1.95 | 1.15–3.32 | 0.013 | 2.07 | 1.23–3.49 | 0.006 |
| Congestive heart failure | 1.50 | 0.94–2.38 | 0.086 | 1.55 | 0.98–2.46 | 0.063 |
| Hypertension | 0.80 | 0.63–1.01 | 0.056 | 0.84 | 0.66–1.06 | 0.131 |
| Cirrhosis | 3.46 | 1.61–7.42 | 0.001 | 3.40 | 1.60–7.23 | 0.002 |
| Age | 1.01 | 1.00–1.01 | 0.211 | |||
| Male gender | 1.13 | 0.89–1.42 | 0.315 | |||
| Diabetes Mellitus | 1.04 | 0.82–1.32 | 0.766 | |||
| Malignancy | 0.71 | 0.26–1.91 | 0.496 | |||
| CAPD | 1.36 | 0.87–2.13 | 0.175 | |||
| Plasma albumin | 0.80 | 0.61–1.05 | 0.105 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, Y.-H.; Chen, Y.-T.; Chen, J.-Y.; Tarng, D.-C.; Lin, C.-C.; Li, S.-Y. Baseline Peritoneal Membrane Transport Characteristics Are Associated with Peritonitis Risk in Incident Peritoneal Dialysis Patients. Membranes 2022, 12, 276. https://doi.org/10.3390/membranes12030276
Chou Y-H, Chen Y-T, Chen J-Y, Tarng D-C, Lin C-C, Li S-Y. Baseline Peritoneal Membrane Transport Characteristics Are Associated with Peritonitis Risk in Incident Peritoneal Dialysis Patients. Membranes. 2022; 12(3):276. https://doi.org/10.3390/membranes12030276
Chicago/Turabian StyleChou, Yi-Hsin, Yung-Tai Chen, Jinn-Yang Chen, Der-Cherng Tarng, Chih-Ching Lin, and Szu-Yuan Li. 2022. "Baseline Peritoneal Membrane Transport Characteristics Are Associated with Peritonitis Risk in Incident Peritoneal Dialysis Patients" Membranes 12, no. 3: 276. https://doi.org/10.3390/membranes12030276