
Impact of Hydrophilic Modification of Synthetic Dialysis Membranes on Hemocompatibility and Performance
 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. The Importance of Dialyzer Performance and Hemocompatibility for the Treatment of ESKD Patients
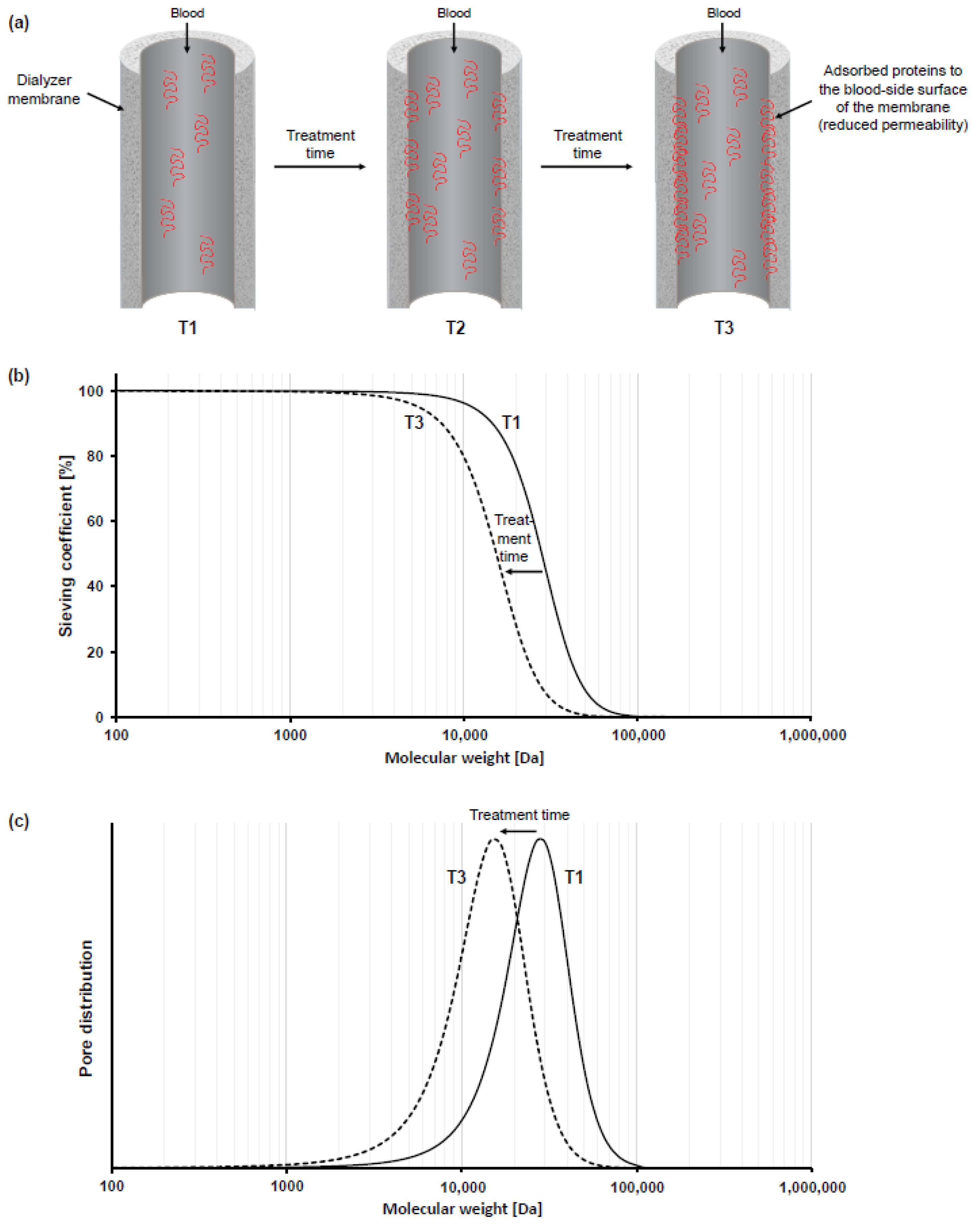
3. Impact of Membrane Fouling on Dialyzers’ Performance and Hemocompatibility
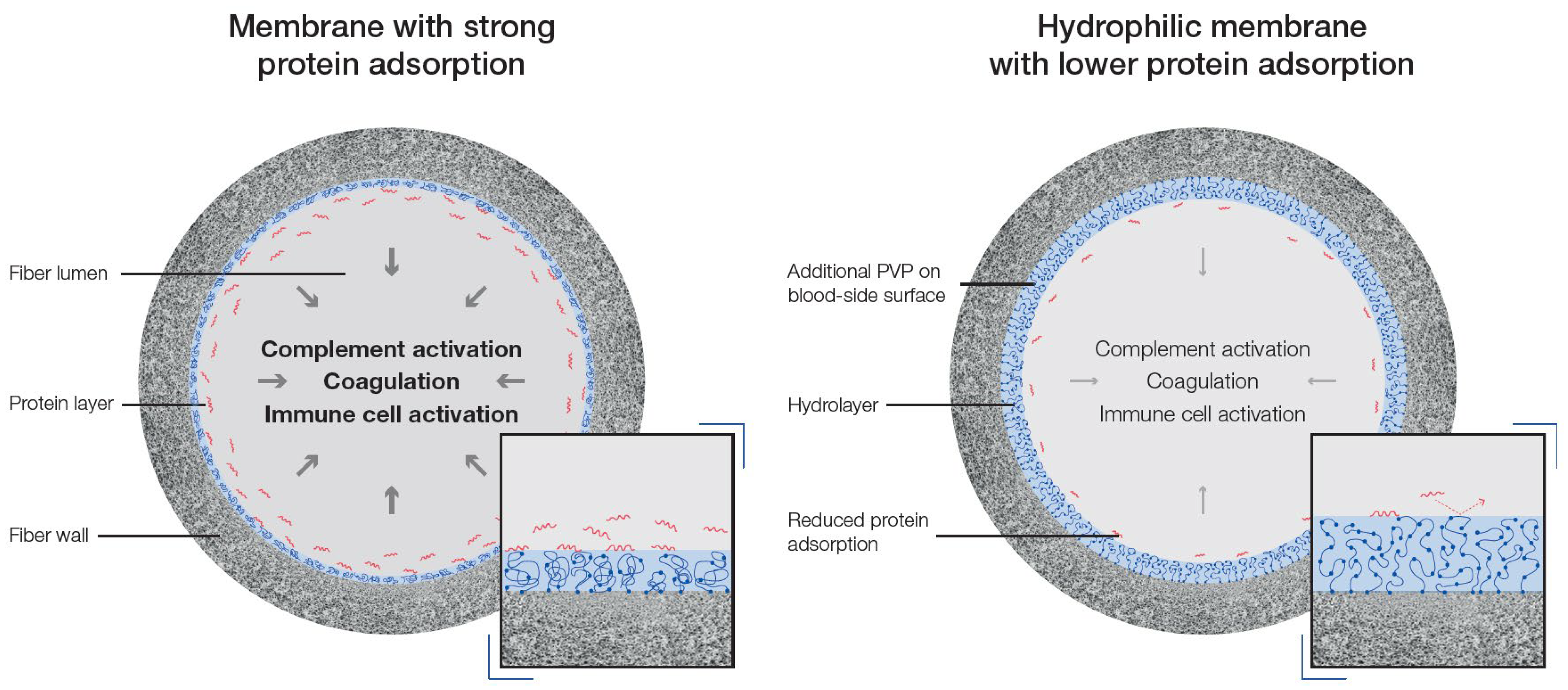
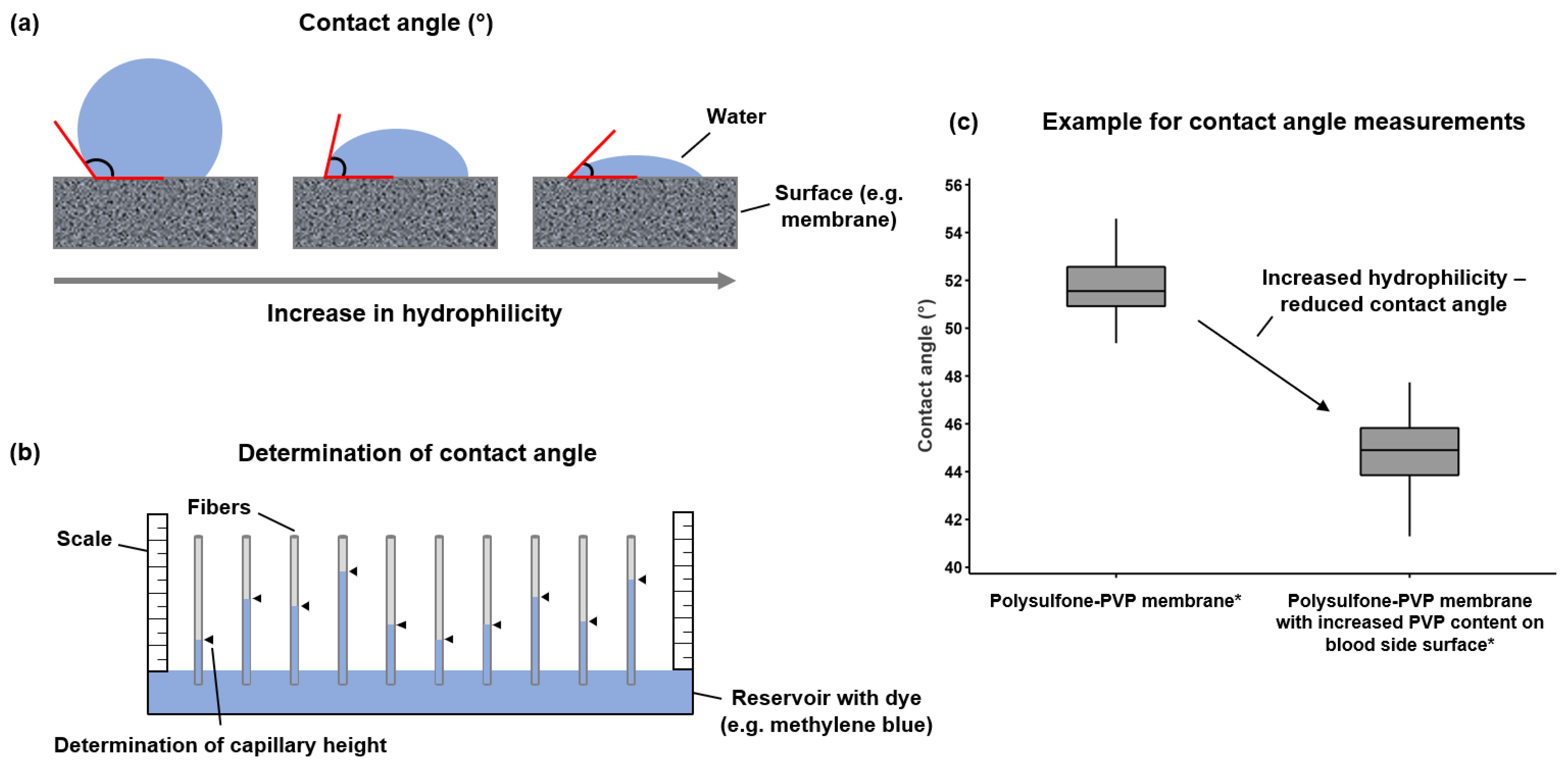
4. Reduction in Membrane Fouling by Hydrophilic Modifications
5. Maintaining Hydrophilic Modification of Dialysis Membranes
5.1. Undesirable Effects of Elutable PVP
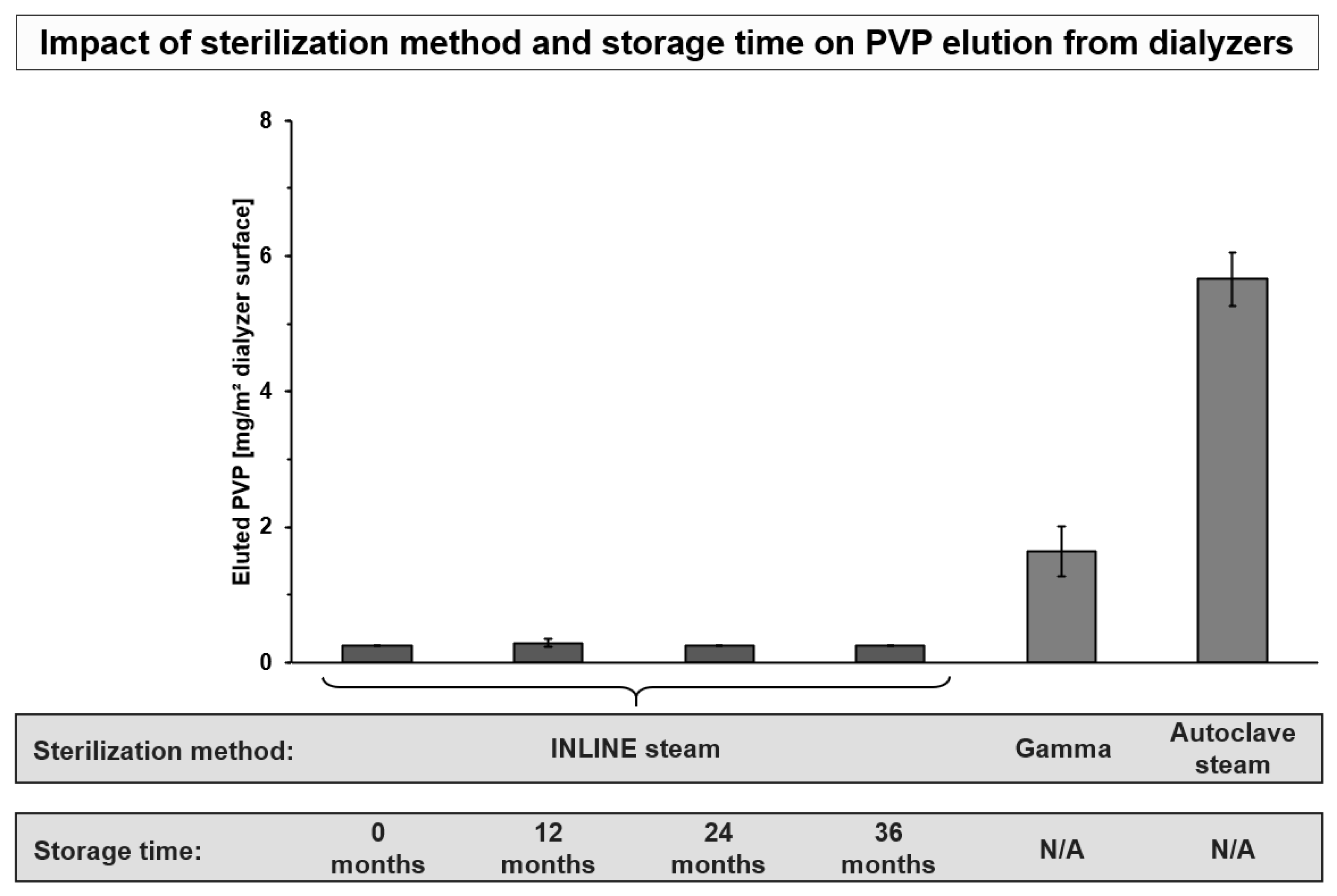
5.2. Factors Influencing PVP Elution
6. Discussion, Conclusions, and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thurlow, J.S.; Joshi, M.; Yan, G.; Norris, K.C.; Agodoa, L.Y.; Yuan, C.M.; Nee, R. Global Epidemiology of End-Stage Kidney Disease and Disparities in Kidney Replacement Therapy. Am. J. Nephrol. 2021, 52, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Saran, R.; Robinson, B.; Abbott, K.C.; Bragg-Gresham, J.; Chen, X.; Gipson, D.; Gu, H.; Hirth, R.A.; Hutton, D.; Jin, Y.; et al. US Renal Data System 2019 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2020, 75, A6–A7. [Google Scholar] [CrossRef]
- Benabed, A.; Henri, P.; Lobbedez, T.; Goffin, E.; Baluta, S.; Benziane, A.; Rachi, A.; van der Pijl, J.W.; Bechade, C.; Ficheux, M. Hémodialyse quotidienne à bas débit de dialysat à domicile: Résultats cliniques et biologiques des 62 premiers patients traités en France et en Belgique. Nephrol. Ther. 2017, 13, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Pattharanitima, P.; El Shamy, O.; Chauhan, K.; Saha, A.; Wen, H.H.; Sharma, S.; Uribarri, J.; Chan, L. The Association between Prevalence of Peritoneal Dialysis versus Hemodialysis and Patients’ Distance to Dialysis-Providing Facilities. Kidney360 2021, 2, 1908–1916. [Google Scholar] [CrossRef] [PubMed]
- Bello, A.K.; Okpechi, I.G.; Osman, M.A.; Cho, Y.; Htay, H.; Jha, V.; Wainstein, M.; Johnson, D.W. Epidemiology of Haemodialysis Outcomes. Nat. Rev. Nephrol. 2022, 18, 378–395. [Google Scholar] [CrossRef]
- Said, N.; Lau, W.J.; Ho, Y.-C.; Lim, S.K.; Zainol Abidin, M.N.; Ismail, A.F. A Review of Commercial Developments and Recent Laboratory Research of Dialyzers and Membranes for Hemodialysis Application. Membranes 2021, 11, 767. [Google Scholar] [CrossRef]
- Bowry, S.K.; Kircelli, F.; Nandakumar, M.; Vachharajani, T.J. Clinical Relevance of Abstruse Transport Phenomena in Haemodialysis. Clin. Kidney J. 2021, 14, i85–i97. [Google Scholar] [CrossRef]
- Makarov, I.S.; Golova, L.K.; Vinogradov, M.I.; Mironova, M.V.; Anokhina, T.S.; Arkharova, N.A. Morphology and Transport Properties of Membranes Obtained by Coagulation of Cellulose Solutions in Isobutanol. Carbohydr. Polym. 2021, 254, 117472. [Google Scholar] [CrossRef]
- Yamashita, A.C.; Sakurai, K. Dialysis Membranes—Physicochemical Structures and Features. In Updates in Hemodialysis; Suzuki, H., Ed.; IntechOpen: London, UK, 2015. [Google Scholar] [CrossRef]
- Bowry, S.K. Dialysis Membranes Today. Int. J. Artif. Organs 2002, 25, 447–460. [Google Scholar] [CrossRef]
- Bowry, S.K.; Chazot, C. The Scientific Principles and Technological Determinants of Haemodialysis Membranes. Clin. Kidney J. 2021, 14, i5–i16. [Google Scholar] [CrossRef]
- Ronco, C.; Clark, W.R. Haemodialysis Membranes. Nat. Rev. Nephrol. 2018, 14, 394–410. [Google Scholar] [CrossRef] [PubMed]
- Canaud, B. Recent Advances in Dialysis Membranes. Curr. Opin. Nephrol. Hypertens. 2021, 30, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Poppelaars, F.; Faria, B.; Gaya da Costa, M.; Franssen, C.F.M.; van Son, W.J.; Berger, S.P.; Daha, M.R.; Seelen, M.A. The Complement System in Dialysis: A Forgotten Story? Front. Immunol. 2018, 9, 71. [Google Scholar] [CrossRef] [PubMed]
- Losappio, V.; Franzin, R.; Infante, B.; Godeas, G.; Gesualdo, L.; Fersini, A.; Castellano, G.; Stallone, G. Molecular Mechanisms of Premature Aging in Hemodialysis: The Complex Interplay between Innate and Adaptive Immune Dysfunction. Int. J. Mol. Sci. 2020, 21, 3422. [Google Scholar] [CrossRef]
- Ekdahl, K.N.; Soveri, I.; Hilborn, J.; Fellström, B.; Nilsson, B. Cardiovascular Disease in Haemodialysis: Role of the Intravascular Innate Immune System. Nat. Rev. Nephrol. 2017, 13, 285–296. [Google Scholar] [CrossRef]
- Campo, S.; Lacquaniti, A.; Trombetta, D.; Smeriglio, A.; Monardo, P. Immune System Dysfunction and Inflammation in Hemodialysis Patients: Two Sides of the Same Coin. J. Clin. Med. 2022, 11, 3759. [Google Scholar] [CrossRef]
- Raharjo, Y.; Zainol Abidin, M.N.; Ismail, A.F.; Fahmi, M.Z.; Saiful; Elma, M.; Santoso, D.; Haula’, H.; Habibi, A.R. Dialysis Membranes for Acute Kidney Injury. Membranes 2022, 12, 325. [Google Scholar] [CrossRef]
- Kohlová, M.; Amorim, C.G.; Araújo, A.; Santos-Silva, A.; Solich, P.; Montenegro, M.C.B.S.M. The Biocompatibility and Bioactivity of Hemodialysis Membranes: Their Impact in End-Stage Renal Disease. J. Artif. Organs 2019, 22, 14–28. [Google Scholar] [CrossRef]
- Vienken, J. Polymers in Nephrology Characteristics and Needs. Int. J. Artif. Organs 2002, 25, 470–479. [Google Scholar] [CrossRef]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C. Chronic Kidney Disease and the Risks of Death, Cardiovascular Events, and Hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef]
- Goodkin, D.A.; Bragg-Gresham, J.L.; Koenig, K.G.; Wolfe, R.A.; Akiba, T.; Andreucci, V.E.; Saito, A.; Rayner, H.C.; Kurokawa, K.; Port, F.K.; et al. Association of Comorbid Conditions and Mortality in Hemodialysis Patients in Europe, Japan, and the United States: The Dialysis Outcomes and Practice Patterns Study (DOPPS). J. Am. Soc. Nephrol. 2003, 14, 3270–3277. [Google Scholar] [CrossRef] [PubMed]
- Robinson, B.M.; Akizawa, T.; Jager, K.J.; Kerr, P.G.; Saran, R.; Pisoni, R.L. Factors Affecting Outcomes in Patients Reaching End-Stage Kidney Disease Worldwide: Differences in Access to Renal Replacement Therapy, Modality Use, and Haemodialysis Practices. Lancet 2016, 388, 294–306. [Google Scholar] [CrossRef]
- Ahmadmehrabi, S.; Tang, W.H.W. Hemodialysis-Induced Cardiovascular Disease. Semin. Dial. 2018, 31, 258–267. [Google Scholar] [CrossRef]
- Ritz, E.; Bommer, J. Cardiovascular Problems on Hemodialysis: Current Deficits and Potential Improvement. Clin. J. Am. Soc. Nephrol. 2009, 4, S71–S78. [Google Scholar] [CrossRef] [PubMed]
- Mavrakanas, T.A.; Charytan, D.M. Cardiovascular Complications in Chronic Dialysis Patients. Curr. Opin. Nephrol. Hypertens. 2016, 25, 536–544. [Google Scholar] [CrossRef]
- Cozzolino, M.; Mangano, M.; Stucchi, A.; Ciceri, P.; Conte, F.; Galassi, A. Cardiovascular Disease in Dialysis Patients. Nephrol. Dial. Transplant. 2018, 33, iii28–iii34. [Google Scholar] [CrossRef] [PubMed]
- USRDS 2018 Volume 2: ESRD in the United States. 2018, 2, 412. Available online: https://www.usrds.org/media/1736/v2_c01_incprev_18_usrds.pdf (accessed on 1 August 2022).
- Wolley, M.; Jardine, M.; Hutchison, C.A. Exploring the Clinical Relevance of Providing Increased Removal of Large Middle Molecules. Clin. J. Am. Soc. Nephrol. 2018, 13, 805–814. [Google Scholar] [CrossRef]
- Okuno, S.; Ishimura, E.; Kohno, K.; Fujino-Katoh, Y.; Maeno, Y.; Yamakawa, T.; Inaba, M.; Nishizawa, Y. Serum 2-Microglobulin Level Is a Significant Predictor of Mortality in Maintenance Haemodialysis Patients. Nephrol. Dial. Transplant. 2008, 24, 571–577. [Google Scholar] [CrossRef]
- Cheung, A.K.; Rocco, M.V.; Yan, G.; Leypoldt, J.K.; Levin, N.W.; Greene, T.; Agodoa, L.; Bailey, J.; Beck, G.J.; Clark, W.; et al. Serum β-2 Microglobulin Levels Predict Mortality in Dialysis Patients: Results of the HEMO Study. J. Am. Soc. Nephrol. 2006, 17, 546–555. [Google Scholar] [CrossRef] [Green Version]
- Henderson, L.W.; Clark, W.R.; Cheung, A.K. Quantification of Middle Molecular Weight Solute Removal in Dialysis. Semin. Dial. 2001, 14, 294–299. [Google Scholar] [CrossRef]
- Kuragano, T.; Kida, A.; Furuta, M.; Nanami, M.; Otaki, Y.; Hasuike, Y.; Nonoguchi, H.; Nakanishi, T. The Impact of Β2-Microglobulin Clearance on the Risk Factors of Cardiovascular Disease in Hemodialysis Patients. ASAIO J. 2010, 56, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Pifer, T.B.; Mccullough, K.P.; Port, F.K.; Goodkin, D.A.; Maroni, B.J.; Held, P.J.; Young, E.W. Mortality Risk in Hemodialysis Patients and Changes in Nutritional Indicators: DOPPS. Kidney Int. 2002, 62, 2238–2245. [Google Scholar] [CrossRef]
- Canaud, B.; Ye, X.; Usvyat, L.; Kooman, J.; van der Sande, F.; Raimann, J.; Wang, Y.; Kotanko, P. Clinical and Predictive Value of Simplified Creatinine Index Used as Muscle Mass Surrogate in End-Stage Kidney Disease Haemodialysis Patients—Results from the International MONitoring Dialysis Outcome Initiative. Nephrol. Dial. Transplant. 2020, 35, 2161–2171. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Ficociello, L.H.; Bazzanella, J.; Mullon, C.; Anger, M.S. Slipping Through the Pores: Hypoalbuminemia and Albumin Loss During Hemodialysis. Int. J. Nephrol. Renov. Dis. 2021, 14, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Ehlerding, G.; Ries, W.; Kempkes-Koch, M.; Ziegler, E.; Erlenkoetter, A.; Zawada, A.M.; Kennedy, J.; Ottillinger, B.; Stauss-Grabo, M.; Lang, T. Randomized Comparison of Three High-Flux Dialyzers during High Volume Online Hemodiafiltration—The ComPERFORM Study. Clin. Kidney J. 2021, 15, 672–680. [Google Scholar] [CrossRef]
- de Borst, M.H. The Complement System in Hemodialysis Patients: Getting to the Heart of the Matter. Nephron 2016, 132, 1–4. [Google Scholar] [CrossRef]
- Carroll, M.C.; Isenman, D.E. Regulation of Humoral Immunity by Complement. Immunity 2012, 37, 199–207. [Google Scholar] [CrossRef]
- Kiss, M.G.; Binder, C.J. The Multifaceted Impact of Complement on Atherosclerosis. Atherosclerosis 2022, 351, 29–40. [Google Scholar] [CrossRef]
- Hakim, R.M. Clinical Implications of Biocompatibility in Blood Purification Membranes. Nephrol. Dial. Transplant. 2000, 15, 16–20. [Google Scholar] [CrossRef] [Green Version]
- Ehlerding, G.; Erlenkötter, A.; Gauly, A.; Griesshaber, B.; Kennedy, J.; Rauber, L.; Ries, W.; Schmidt-Gürtler, H.; Stauss-Grabo, M.; Wagner, S.; et al. Performance and Hemocompatibility of a Novel Polysulfone Dialyzer: A Randomized Controlled Trial. Kidney360 2021, 2, 937–947. [Google Scholar] [CrossRef]
- Krieter, D.H.; Morgenroth, A.; Barasinski, A.; Lemke, H.-D.; Schuster, O.; von Harten, B.; Wanner, C. Effects of a Polyelectrolyte Additive on the Selective Dialysis Membrane Permeability for Low-Molecular-Weight Proteins. Nephrol. Dial. Transplant. 2007, 22, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Stefoni, S.; Colì, L.; Cianciolo, G.; Donati, G.; Ruggeri, G.; Ramazzotti, E.; Pohlmeier, R.; Lang, D. Inflammatory Response of a New Synthetic Dialyzer Membrane. a Randomised Cross-over Comparison between Polysulfone and Helixone. Int. J. Artif. Organs 2003, 26, 26–32. [Google Scholar] [CrossRef]
- Hertle, E.; van Greevenbroek, M.M.; Arts, I.C.; van der Kallen, C.J.; Geijselaers, S.L.; Feskens, E.J.; Jansen, E.H.; Schalkwijk, C.G.; Stehouwer, C.D. Distinct Associations of Complement C3a and Its Precursor C3 with Atherosclerosis and Cardiovascular Disease. The CODAM Study. Thromb. Haemost. 2014, 111, 1102–1111. [Google Scholar] [CrossRef] [PubMed]
- Hertle, E.; van Greevenbroek, M.M.J.; Arts, I.C.W.; van der Kallen, C.J.H.; Feskens, E.J.M.; Schalkwijk, C.G.; Stehouwer, C.D.A. Complement Activation Products C5a and SC5b-9 Are Associated with Low-Grade Inflammation and Endothelial Dysfunction, but Not with Atherosclerosis in a Cross-Sectional Analysis: The CODAM Study. Int. J. Cardiol. 2014, 174, 400–403. [Google Scholar] [CrossRef] [PubMed]
- Hertle, E.; Stehouwer, C.D.A.; van Greevenbroek, M.M.J. The Complement System in Human Cardiometabolic Disease. Mol. Immunol. 2014, 61, 135–148. [Google Scholar] [CrossRef]
- Vogel, C.-W. The Role of Complement in Myocardial Infarction Reperfusion Injury: An Underappreciated Therapeutic Target. Front. Cell Dev. Biol. 2020, 8, 606407. [Google Scholar] [CrossRef]
- Hakim, R.M. Clinical Sequelae of Complement Activation in Hemodialysis. Clin. Nephrol. 1986, 26 (Suppl. 1), S9–S12. [Google Scholar]
- Lines, S.W.; Richardson, V.R.; Thomas, B.; Dunn, E.J.; Wright, M.J.; Carter, A.M. Complement and Cardiovascular Disease—The Missing Link in Haemodialysis Patients? Nephron 2016, 132, 5–14. [Google Scholar] [CrossRef]
- Poppelaars, F.; Gaya da Costa, M.; Faria, B.; Berger, S.P.; Assa, S.; Daha, M.R.; Medina Pestana, J.O.; van Son, W.J.; Franssen, C.F.M.; Seelen, M.A. Intradialytic Complement Activation Precedes the Development of Cardiovascular Events in Hemodialysis Patients. Front. Immunol. 2018, 9, 2070. [Google Scholar] [CrossRef]
- Manthey, H.D.; Thomas, A.C.; Shiels, I.A.; Zernecke, A.; Woodruff, T.M.; Rolfe, B.; Taylor, S.M. Complement C5a Inhibition Reduces Atherosclerosis in ApoE –/– Mice. FASEB J. 2011, 25, 2447–2455. [Google Scholar] [CrossRef]
- Daugirdas, J.T.; Bernardo, A.A. Hemodialysis Effect on Platelet Count and Function and Hemodialysis-Associated Thrombocytopenia. Kidney Int. 2012, 82, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Melchior, P.; Erlenkötter, A.; Zawada, A.M.; Delinski, D.; Schall, C.; Stauss-Grabo, M.; Kennedy, J.P. Complement Activation by Dialysis Membranes and Its Association with Secondary Membrane Formation and Surface Charge. Artif. Organs 2021, 45, 770–778. [Google Scholar] [CrossRef] [PubMed]
- Bergesio, F.; Monzani, G.; Manescalchi, F.; Boccabianca, I.; Passaleva, A.; Frizzi, V. Leukocytes, Eosinophils and Complement Function during Hemodialysis with Polysulphone and Polymethylmethacrylate Membranes: Comparison with Cuprophan and Polyacrylonitrile. Blood Purif. 1988, 6, 16–26. [Google Scholar] [CrossRef]
- Martin-Malo, A.; Castillo, D.; Castro, M.; Pérez, R.; Rios, A.; Jaraba, M.; Aljama, P. Biocompatibility of Dialysis Membranes: A Comparative Study. Nephrol. Dial. Transplant. 1991, 6 (Suppl. 2), 55–58. [Google Scholar] [PubMed]
- Grooteman, M.P.; Nubé, M.J.; van Limbeek, J.; van Houte, A.J.; Daha, M.R.; van Geelen, J.A. Biocompatibility and Performance of a Modified Cellulosic and a Synthetic High Flux Dialyzer. A Randomized Crossover Comparison between Cellulose Triacetate and Polysulphon. ASAIO J. 1995, 41, 215–220. [Google Scholar] [CrossRef]
- Zawada, A.M.; Melchior, P.; Schall, C.; Erlenkötter, A.; Lang, T.; Keller, T.; Stauss-Grabo, M.; Kennedy, J.P. Time-resolving Characterization of Molecular Weight Retention Changes among Three Synthetic High-flux Dialyzers. Artif. Organs 2022, 46, 1318–1327. [Google Scholar] [CrossRef]
- Röckel, A.; Hertel, J.; Fiegel, P.; Abdelhamid, S.; Panitz, N.; Walb, D. Permeability and Secondary Membrane Formation of a High Flux Polysulfone Hemofilter. Kidney Int. 1986, 30, 429–432. [Google Scholar] [CrossRef]
- Kim, T.R.; Hadidi, M.; Motevalian, S.P.; Sunohara, T.; Zydney, A.L. Effects of Plasma Proteins on the Transport and Surface Characteristics of Polysulfone/Polyethersulfone and Asymmetric Cellulose Triacetate High Flux Dialyzers. Artif. Organs 2018, 42, 1070–1077. [Google Scholar] [CrossRef]
- Langsdorf, L.J.; Zydney, A.L. Effect of Blood Contact on the Transport Properties of Hemodialysis Membranes: A Two-Layer Membrane Model. Blood Purif. 1994, 12, 292–307. [Google Scholar] [CrossRef]
- Morti, S.M.; Zydney, A.L. Protein-Membrane Interactions during Hemodialysis: Effects on Solute Transport. ASAIO J. 1998, 44, 319–326. [Google Scholar] [CrossRef]
- Boschetti-de-Fierro, A.; Voigt, M.; Storr, M.; Krause, B. MCO Membranes: Enhanced Selectivity in High-Flux Class. Sci. Rep. 2015, 5, 18448. [Google Scholar] [CrossRef] [PubMed]
- Kiguchi, T.; Ito, H.; Yamashita, A.C. Effect of Membrane Surface Area on Solute Removal Performance of Dialyzers with Fouling. Membranes 2022, 12, 684. [Google Scholar] [CrossRef] [PubMed]
- Urbani, A.; Sirolli, V.; Lupisella, S.; Levi-Mortera, S.; Pavone, B.; Pieroni, L.; Amoroso, L.; Di Vito, R.; Bucci, S.; Bernardini, S.; et al. Proteomic Investigations on the Effect of Different Membrane Materials on Blood Protein Adsorption during Haemodialysis. Blood Transfus. Trasfus. Sangue 2012, 10 (Suppl. 2), s101–s112. [Google Scholar] [CrossRef]
- Andersson, J.; Ekdahl, K.N.; Larsson, R.; Nilsson, U.R.; Nilsson, B. C3 Adsorbed to a Polymer Surface Can Form an Initiating Alternative Pathway Convertase. J. Immunol. 2002, 168, 5786–5791. [Google Scholar] [CrossRef]
- Hayama, M.; Yamamoto, K.; Kohori, F.; Uesaka, T.; Ueno, Y.; Sugaya, H.; Itagaki, I.; Sakai, K. Nanoscopic Behavior of Polyvinylpyrrolidone Particles on Polysulfone/Polyvinylpyrrolidone Film. Biomaterials 2004, 25, 1019–1028. [Google Scholar] [CrossRef]
- Koga, Y.; Fujieda, H.; Meguro, H.; Ueno, Y.; Aoki, T.; Miwa, K.; Kainoh, M. Biocompatibility of Polysulfone Hemodialysis Membranes and Its Mechanisms: Involvement of Fibrinogen and Its Integrin Receptors in Activation of Platelets and Neutrophils. Artif. Organs 2018, 42, E246–E258. [Google Scholar] [CrossRef]
- Zawada, A.M.; Melchior, P.; Erlenkötter, A.; Delinski, D.; Stauss-Grabo, M.; Kennedy, J.P. Polyvinylpyrrolidone in Hemodialysis Membranes: Impact on Platelet Loss during Hemodialysis. Hemodial. Int. 2021, 25, 498–506. [Google Scholar] [CrossRef]
- Zhu, L.; Song, H.; Wang, J.; Xue, L. Polysulfone Hemodiafiltration Membranes with Enhanced Anti-Fouling and Hemocompatibility Modified by Poly(Vinyl Pyrrolidone) via in Situ Cross-Linked Polymerization. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 74, 159–166. [Google Scholar] [CrossRef]
- Jiang, J.; Zhu, L.; Zhu, L.; Zhang, H.; Zhu, B.; Xu, Y. Antifouling and Antimicrobial Polymer Membranes Based on Bioinspired Polydopamine and Strong Hydrogen-Bonded Poly( N -Vinyl Pyrrolidone). ACS Appl. Mater. Interfaces 2013, 5, 12895–12904. [Google Scholar] [CrossRef]
- Ran, F.; Nie, S.; Zhao, W.; Li, J.; Su, B.; Sun, S.; Zhao, C. Biocompatibility of Modified Polyethersulfone Membranes by Blending an Amphiphilic Triblock Co-Polymer of Poly(Vinyl Pyrrolidone)-b-Poly(Methyl Methacrylate)-b-Poly(Vinyl Pyrrolidone). Acta Biomater. 2011, 7, 3370–3381. [Google Scholar] [CrossRef]
- Hayama, M.; Yamamoto, K.; Kohori, F.; Sakai, K. How Polysulfone Dialysis Membranes Containing Polyvinylpyrrolidone Achieve Excellent Biocompatibility? J. Membr. Sci. 2004, 234, 41–49. [Google Scholar] [CrossRef]
- Wang, H.; Yu, T.; Zhao, C.; Du, Q. Improvement of Hydrophilicity and Blood Compatibility on Polyethersulfone Membrane by Adding Polyvinylpyrrolidone. Fibers Polym. 2009, 10, 1–5. [Google Scholar] [CrossRef]
- Matsuda, M.; Sato, M.; Sakata, H.; Ogawa, T.; Yamamoto, K.; Yakushiji, T.; Fukuda, M.; Miyasaka, T.; Sakai, K. Effects of Fluid Flow on Elution of Hydrophilic Modifier from Dialysis Membrane Surfaces. J. Artif. Organs 2008, 11, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Namekawa, K.; Matsuda, M.; Fukuda, M.; Kaneko, A.; Sakai, K. Poly(N-Vinyl-2-Pyrrolidone) Elution from Polysulfone Dialysis Membranes by Varying Solvent and Wall Shear Stress. J. Artif. Organs 2012, 15, 185–192. [Google Scholar] [CrossRef]
- Hulme, B.; Dykes, P.W.; Appleyard, I.; Arkell, D.W. Retention and Storage Sites of Radioactive Polyvinylpyrrolidone. J. Nucl. Med. 1968, 9, 389–393. [Google Scholar]
- Takahashi, K.; Eto, K.; Takeya, M.; Naito, M.; Yaginuma, Y.; Ichihara, A. Long-Term Polyvinylpyrrolidone Storage. Pathol. Int. 1983, 33, 985–997. [Google Scholar] [CrossRef]
- Shu, K.-H.; Kao, T.-W.; Chiang, W.-C.; Wu, V.-C. A Case of Anaphylactic Shock Induced by FX60 Polysulfone Hemodialyzer but Not F6-HPS Polysulfone Hemodialyzer: Polysulfone Hemodialyzer Anaphylaxis. Hemodial. Int. 2014, 18, 841–845. [Google Scholar] [CrossRef]
- Bacelar Marques, I.D.; Pinheiro, K.F.; de Freitas do Carmo, L.P.; Costa, M.C.; Abensur, H. Anaphylactic Reaction Induced by a Polysulfone/Polyvinylpyrrolidone Membrane in the 10th Session of Hemodialysis with the Same Dialyzer. Hemodial. Int. 2011, 15, 399–403. [Google Scholar] [CrossRef]
- Martin-Navarro, J.; Esteras, R.; Castillo, E.; Carriazo, S.; Fernández-Prado, R.; Gracia-Iguacel, C.; Mas Fontao, S.; Ortíz, A.; González-Parra, E. Reactions to Synthetic Membranes Dialyzers: Is There an Increase in Incidence? Kidney Blood Press. Res. 2019, 44, 907–914. [Google Scholar] [CrossRef]
- Alvarez-de Lara, M.A.; Martín-Malo, A. Hypersensitivity Reactions to Synthetic Haemodialysis Membranes’ an Emerging Issue? Nefrologia 2014, 34, 698–702. [Google Scholar] [CrossRef]
- Ohashi, N.; Yonemura, K.; Goto, T.; Suzuki, H.; Fujigaki, Y.; Yamamoto, T.; Hishida, A. A Case of Anaphylactoid Shock Induced by the BS Polysulfone Hemodialyzer but Not by the F8-HPS Polysulfone Hemodialyzer. Clin. Nephrol. 2003, 60, 214–217. [Google Scholar] [CrossRef] [PubMed]
- Konishi, S.; Fukunaga, A.; Yamashita, H.; Miyata, M.; Usami, M. Eluted Substances from Hemodialysis Membranes Elicit Positive Skin Prick Tests in Bioincompatible Patients. Artif. Organs 2015, 39, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Miyata, M.; Konishi, S.; Shimamoto, Y.; Kamada, A.; Umimoto, K. Influence of Sterilization and Storage Period on Elution of Polyvinylpyrrolidone from Wet-Type Polysulfone Membrane Dialyzers. ASAIO J. 2015, 61, 468–473. [Google Scholar] [CrossRef]
- Allard, B.; Begri, R.; Potier, J.; Coupel, S. Dialyzers Biocompatibility and Efficiency Determinants of Sterilization Method Choice. Pharm. Hosp. Clin. 2013, 48, e15–e21. [Google Scholar] [CrossRef]
- Namekawa, K.; Kaneko, A.; Sakai, K.; Kunikata, S.; Matsuda, M. Longer Storage of Dialyzers Increases Elution of Poly(N-Vinyl-2-Pyrrolidone) from Polysulfone-Group Dialysis Membranes. J. Artif. Organs 2011, 14, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Kiaii, M.; Aritomi, M.; Nagase, M.; Farah, M.; Jung, B. Clinical Evaluation of Performance, Biocompatibility, and Safety of Vitamin E-Bonded Polysulfone Membrane Hemodialyzer Compared to Non-Vitamin E-Bonded Hemodialyzer. J. Artif. Organs 2019, 22, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Calò, L.A.; Naso, A.; D’Angelo, A.; Pagnin, E.; Zanardo, M.; Puato, M.; Rebeschini, M.; Landini, S.; Feriani, M.; Perego, A.; et al. Molecular Biology-Based Assessment of Vitamin E-Coated Dialyzer Effects on Oxidative Stress, Inflammation, and Vascular Remodeling: THOUGHTS AND PROGRESS. Artif. Organs 2011, 35, E33–E39. [Google Scholar] [CrossRef]
- Kensinger, C.; Karp, S.; Kant, R.; Chui, B.W.; Goldman, K.; Yeager, T.; Gould, E.R.; Buck, A.; Laneve, D.C.; Groszek, J.J.; et al. First Implantation of Silicon Nanopore Membrane Hemofilters. ASAIO J. 2016, 62, 491–495. [Google Scholar] [CrossRef]
- Fissell, W.H.; Dubnisheva, A.; Eldridge, A.N.; Fleischman, A.J.; Zydney, A.L.; Roy, S. High-Performance Silicon Nanopore Hemofiltration Membranes. J. Membr. Sci. 2009, 326, 58–63. [Google Scholar] [CrossRef]
- Kim, S.; Feinberg, B.; Kant, R.; Chui, B.; Goldman, K.; Park, J.; Moses, W.; Blaha, C.; Iqbal, Z.; Chow, C.; et al. Diffusive Silicon Nanopore Membranes for Hemodialysis Applications. PLoS ONE 2016, 11, e0159526. [Google Scholar] [CrossRef]
- Laville, M.; Dorval, M.; Fort Ros, J.; Fay, R.; Cridlig, J.; Nortier, J.L.; Juillard, L.; Dębska-Ślizień, A.; Fernández Lorente, L.; Thibaudin, D.; et al. Results of the HepZero Study Comparing Heparin-Grafted Membrane and Standard Care Show That Heparin-Grafted Dialyzer Is Safe and Easy to Use for Heparin-Free Dialysis. Kidney Int. 2014, 86, 1260–1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossignol, P.; Dorval, M.; Fay, R.; Ros, J.; Loughraieb, N.; Moureau, F.; Laville, M. Rationale and Design of the HepZero Study: A Prospective, Multicenter, International, Open, Randomized, Controlled Clinical Study with Parallel Groups Comparing Heparin-Free Dialysis with Heparin-Coated Dialysis Membrane (Evodial) versus Standard Care: Study Protocol for a Randomized Controlled Trial. Trials 2013, 14, 163. [Google Scholar] [CrossRef] [PubMed]
- Meijers, B.K.I.; Poesen, R.; Evenepoel, P. Heparin-Coated Dialyzer Membranes: Is Non-Inferiority Good Enough? Kidney Int. 2014, 86, 1084–1086. [Google Scholar] [CrossRef]
- Biran, R.; Pond, D. Heparin Coatings for Improving Blood Compatibility of Medical Devices. Adv. Drug Deliv. Rev. 2017, 112, 12–23. [Google Scholar] [CrossRef]
- Fisher, C.; Shao, H.; Ho, C. Improved Hemocompatibility of Polysulfone Hemodialyzers with Endexo® Surface Modifying Molecules. J. Biomed. Mater. Res. B Appl. Biomater. 2022, 110, 1335–1343. [Google Scholar] [CrossRef]
- Meyer, J.M.; Steer, D.; Weber, L.A.; Zeitone, A.A.; Thakuria, M.; Ho, C.-H.; Aslam, S.; Mullon, C.; Kossmann, R.J. Safety of a Novel Dialyzer Containing a Fluorinated Polyurethane Surface-Modifying Macromolecule in Patients with End-Stage Kidney Disease. Blood Purif. 2021, 50, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Donaire, M.L.; Santerre, J.P. Surface Modifying Oligomers Used to Functionalize Polymeric Surfaces: Consideration of Blood Contact Applications. J. Appl. Polym. Sci. 2014, 131. [Google Scholar] [CrossRef]
- Niwa, T. Removal of Protein-Bound Uraemic Toxins by Haemodialysis. Blood Purif. 2013, 35, 20–25. [Google Scholar] [CrossRef]
- Tijink, M.S.L.; Wester, M.; Glorieux, G.; Gerritsen, K.G.F.; Sun, J.; Swart, P.C.; Borneman, Z.; Wessling, M.; Vanholder, R.; Joles, J.A.; et al. Mixed Matrix Hollow Fiber Membranes for Removal of Protein-Bound Toxins from Human Plasma. Biomaterials 2013, 34, 7819–7828. [Google Scholar] [CrossRef]
- Stiapis, C.; Skouras, E.; Pavlenko, D.; Stamatialis, D.; Burganos, V. Evaluation of the Toxin-to-Protein Binding Rates during Hemodialysis Using Sorbent-Loaded Mixed-Matrix Membranes. Appl. Sci. 2018, 8, 536. [Google Scholar] [CrossRef]
- Yamamoto, S.; Ito, T.; Sato, M.; Goto, S.; Kazama, J.J.; Gejyo, F.; Narita, I. Adsorption of Protein-Bound Uremic Toxins Using Activated Carbon through Direct Hemoperfusion in Vitro. Blood Purif. 2019, 48, 215–222. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zawada, A.M.; Lang, T.; Ottillinger, B.; Kircelli, F.; Stauss-Grabo, M.; Kennedy, J.P. Impact of Hydrophilic Modification of Synthetic Dialysis Membranes on Hemocompatibility and Performance. Membranes 2022, 12, 932. https://doi.org/10.3390/membranes12100932
Zawada AM, Lang T, Ottillinger B, Kircelli F, Stauss-Grabo M, Kennedy JP. Impact of Hydrophilic Modification of Synthetic Dialysis Membranes on Hemocompatibility and Performance. Membranes. 2022; 12(10):932. https://doi.org/10.3390/membranes12100932
Chicago/Turabian StyleZawada, Adam M., Thomas Lang, Bertram Ottillinger, Fatih Kircelli, Manuela Stauss-Grabo, and James P. Kennedy. 2022. "Impact of Hydrophilic Modification of Synthetic Dialysis Membranes on Hemocompatibility and Performance" Membranes 12, no. 10: 932. https://doi.org/10.3390/membranes12100932