
AN69 Filter Membranes with High Ultrafiltration Rates during Continuous Venovenous Hemofiltration Reduce Mortality in Patients with Sepsis-Induced Multiorgan Dysfunction Syndrome

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
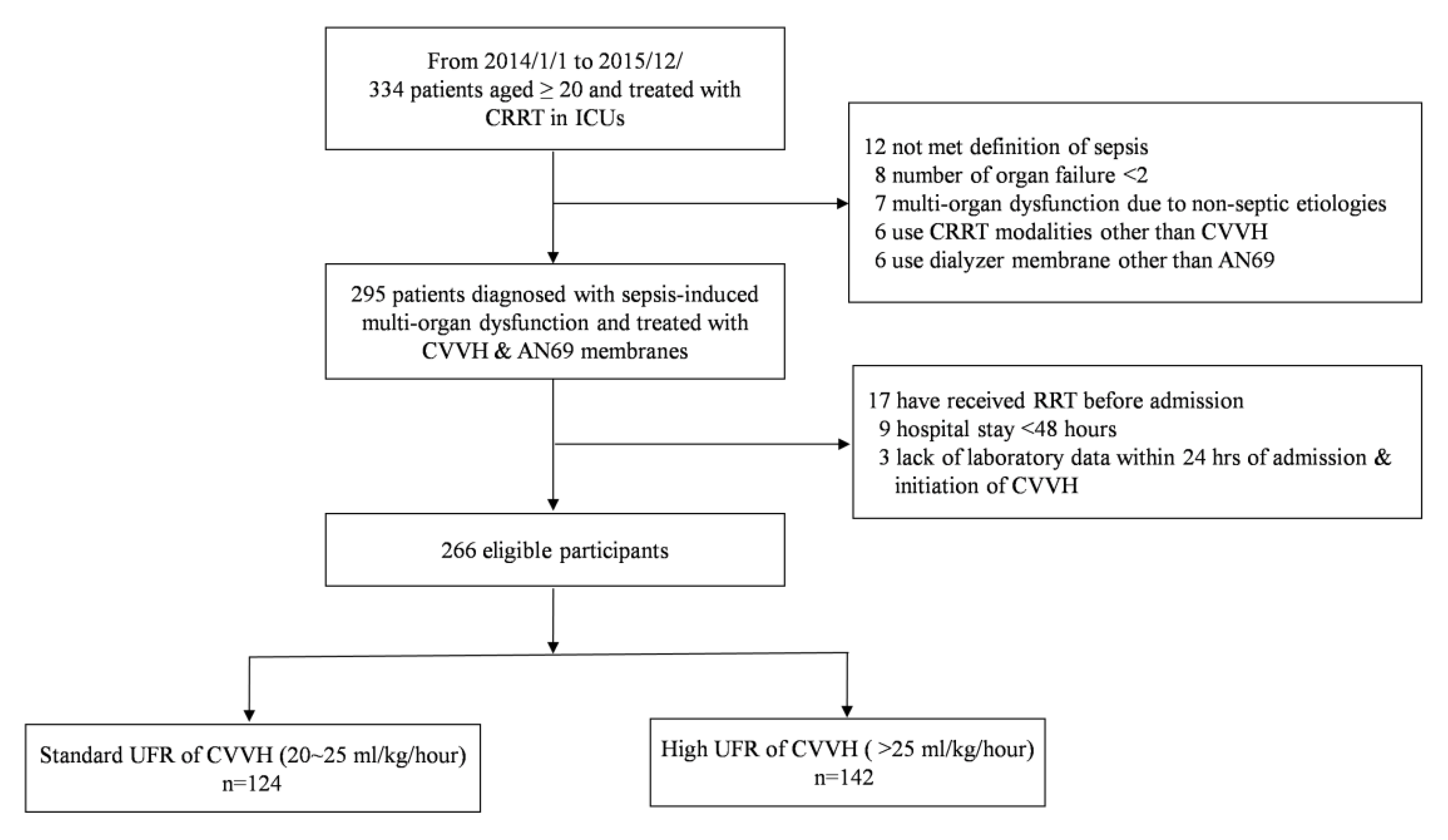
2.2. Participants
2.3. Data Collection and Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Clinical Variables and Laboratory Values at the Initiation of CVVH
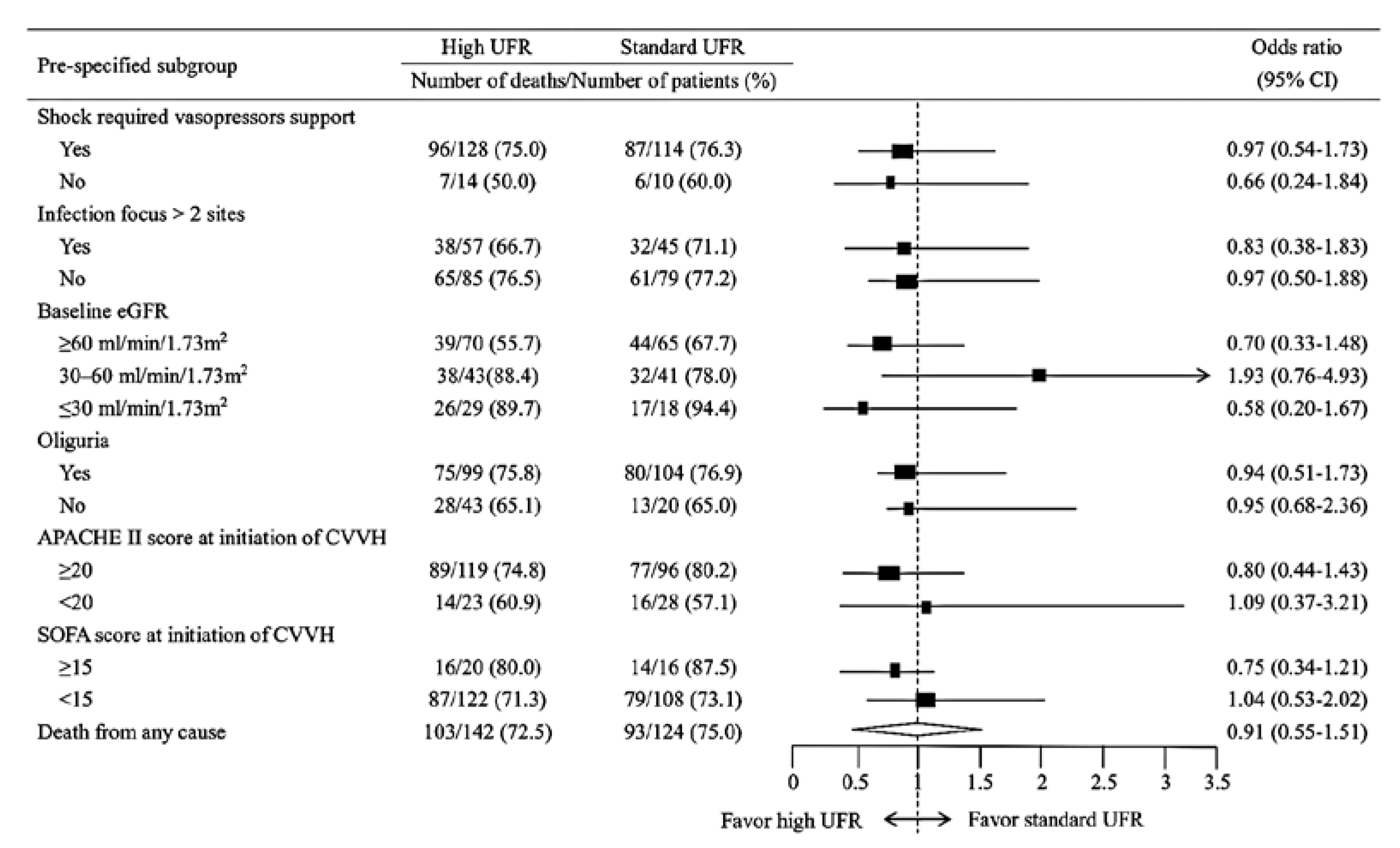
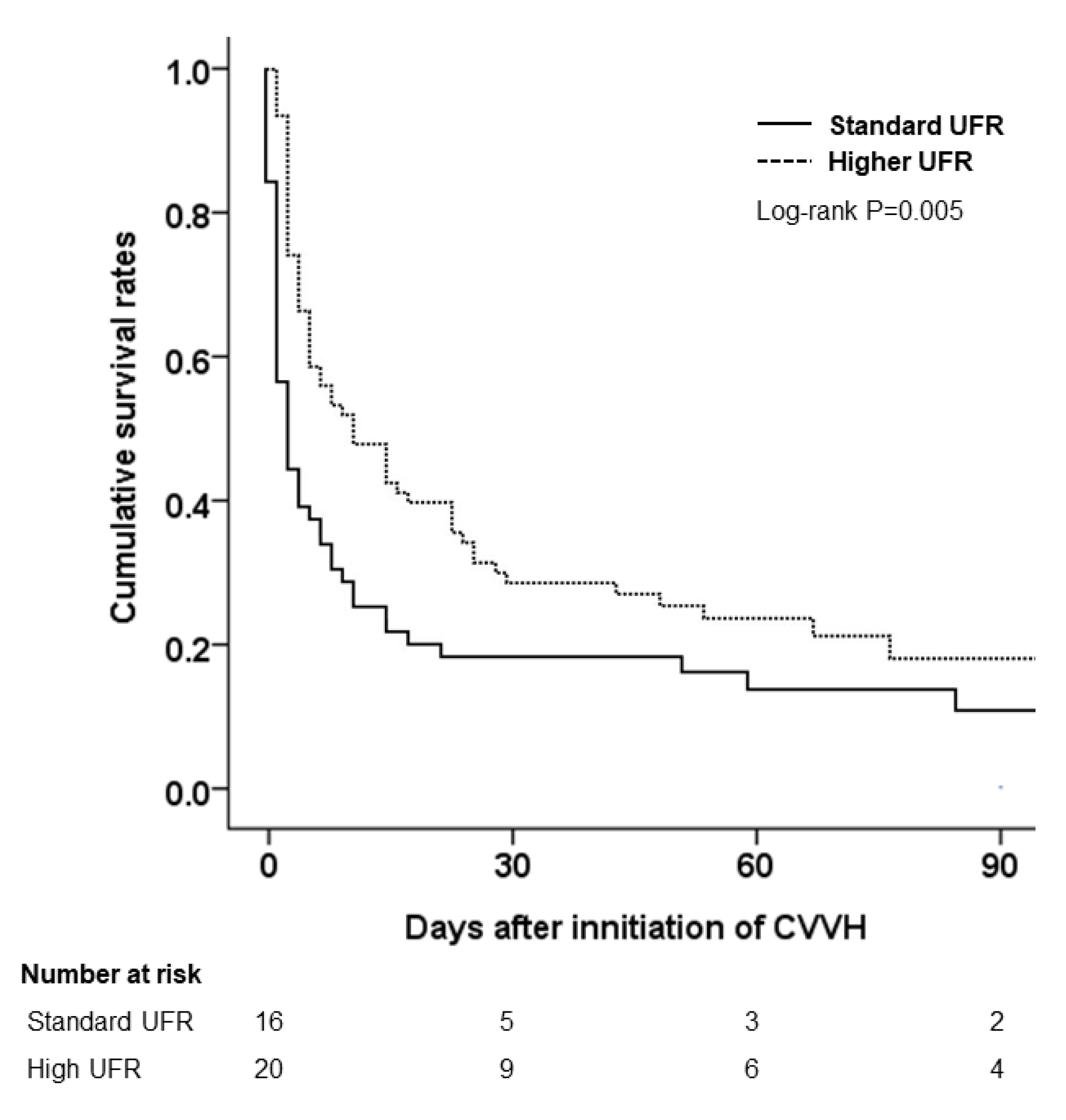
3.3. Risk of In-Hospital Mortality in the Standard and High UFR Groups
3.4. Clinical Determinants of Mortality Risk among Patients with Sepsis-Induced MODS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Doi, K.; Rabb, H. Impact of acute kidney injury on distant organ function: Recent findings and potential therapeutic targets. Kidney Int. 2016, 89, 555–564. [Google Scholar] [CrossRef] [Green Version]
- Hoste, E.A.; Bagshaw, S.M.; Bellomo, R.; Cely, C.M.; Colman, R.; Cruz, D.N.; Edipidis, K.; Forni, L.G.; Gomersall, C.D.; Govil, D.; et al. Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensive Care Med. 2015, 41, 1411–1423. [Google Scholar] [CrossRef]
- Uchino, S.; Kellum, J.A.; Bellomo, R.; Doig, G.S.; Morimatsu, H.; Morgera, S.; Schetz, M.; Tan, I.; Bouman, C.; Macedo, E.; et al. Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA 2005, 294, 813–818. [Google Scholar] [CrossRef] [Green Version]
- Tatum, J.M.; Barmparas, G.; Ko, A.; Dhillon, N.; Smith, E.; Margulies, D.R.; Ley, E.J. Analysis of Survival After Initiation of Continuous Renal Replacement Therapy in a Surgical Intensive Care Unit. JAMA Surg. 2017, 152, 938–943. [Google Scholar] [CrossRef]
- Tandukar, S.; Palevsky, P.M. Continuous Renal Replacement Therapy: Who, When, Why, and How. Chest 2019, 155, 626–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellomo, R.; Tipping, P.; Boyce, N. Continuous veno-venous hemofiltration with dialysis removes cytokines from the circulation of septic patients. Crit. Care Med. 1993, 21, 522–526. [Google Scholar] [CrossRef]
- Heering, P.; Morgera, S.; Schmitz, F.J.; Schmitz, G.; Willers, R.; Schultheiss, H.P.; Strauer, B.E.; Grabensee, B. Cytokine removal and cardiovascular hemodynamics in septic patients with continuous venovenous hemofiltration. Intensive Care Med. 1997, 23, 288–296. [Google Scholar] [CrossRef]
- Clark, E.; Molnar, A.O.; Joannes-Boyau, O.; Honore, P.M.; Sikora, L.; Bagshaw, S.M. High-volume hemofiltration for septic acute kidney injury: A systematic review and meta-analysis. Crit. Care 2014, 18, R7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.T.; Lee, H.; Kee, Y.K.; Park, S.; Oh, H.J.; Han, S.H.; Joo, K.W.; Lim, C.S.; Kim, Y.S.; Kang, S.W.; et al. High-Dose Versus Conventional-Dose Continuous Venovenous Hemodiafiltration and Patient and Kidney Survival and Cytokine Removal in Sepsis-Associated Acute Kidney Injury: A Randomized Controlled Trial. Am. J. Kidney Dis. 2016, 68, 599–608. [Google Scholar] [CrossRef]
- Cole, L.; Bellomo, R.; Davenport, P.; Tipping, P.; Ronco, C. Cytokine removal during continuous renal replacement therapy: An ex vivo comparison of convection and diffusion. Int. J. Artif. Organs 2004, 27, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Moriyama, K.; Shimomura, Y.; Kato, Y.; Kuriyama, N.; Hara, Y.; Yamada, S.; Nishida, O. Adsorption kinetics of high mobility group box 1 protein in a polyacrylonitrile hemofiltration membrane. Ther. Apher. Dial. 2021, 25, 66–72. [Google Scholar] [CrossRef]
- Goldfarb, S.; Golper, T.A. Proinflammatory cytokines and hemofiltration membranes. J. Am. Soc. Nephrol. 1994, 5, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Bellomo, R.; Homel, P.; Brendolan, A.; Dan, M.; Piccinni, P.; La Greca, G. Effects of different doses in continuous veno-venous haemofiltration on outcomes of acute renal failure: A prospective randomised trial. Lancet 2000, 356, 26–30. [Google Scholar] [CrossRef]
- Network, V.N.A.R.F.T.; Palevsky, P.M.; Zhang, J.H.; O’Connor, T.Z.; Chertow, G.M.; Crowley, S.T.; Choudhury, D.; Finkel, K.; Kellum, J.A.; Paganini, E.; et al. Intensity of renal support in critically ill patients with acute kidney injury. N. Engl. J. Med. 2008, 359, 7–20. [Google Scholar] [CrossRef]
- Investigators, R.R.T.S.; Bellomo, R.; Cass, A.; Cole, L.; Finfer, S.; Gallagher, M.; Lo, S.; McArthur, C.; McGuinness, S.; Myburgh, J.; et al. Intensity of continuous renal-replacement therapy in critically ill patients. N. Engl. J. Med. 2009, 361, 1627–1638. [Google Scholar] [CrossRef] [Green Version]
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron. Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P.; Acute Dialysis Quality Initiative Workgroup. Acute renal failure-definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [Green Version]
- Rossaint, J.; Zarbock, A. Pathogenesis of Multiple Organ Failure in Sepsis. Crit. Rev. Immunol. 2015, 35, 277–291. [Google Scholar] [CrossRef]
- Vincent, J.L. Metabolic support in sepsis and multiple organ failure: More questions than answers. Crit. Care Med. 2007, 35, S436–S440. [Google Scholar] [CrossRef]
- Servillo, G.; Vargas, M.; Pastore, A.; Procino, A.; Iannuzzi, M.; Capuano, A.; Memoli, A.; Riccio, E.; Memoli, B. Immunomodulatory effect of continuous venovenous hemofiltration during sepsis: Preliminary data. Biomed. Res. Int. 2013, 2013, 108951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sieberth, H.G.; Kierdorf, H.P. Is cytokine removal by continuous hemofiltration feasible? Kidney Int. Suppl. 1999, 56, S79–S83. [Google Scholar] [CrossRef]
- De Vriese, A.S.; Colardyn, F.A.; Philippe, J.J.; Vanholder, R.C.; De Sutter, J.H.; Lameire, N.H. Cytokine removal during continuous hemofiltration in septic patients. J. Am. Soc. Nephrol. 1999, 10, 846–853. [Google Scholar] [CrossRef]
- Ratanarat, R.; Brendolan, A.; Piccinni, P.; Dan, M.; Salvatori, G.; Ricci, Z.; Ronco, C. Pulse high-volume haemofiltration for treatment of severe sepsis: Effects on hemodynamics and survival. Crit. Care 2005, 9, R294–R302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronco, C.; Tetta, C.; Mariano, F.; Wratten, M.L.; Bonello, M.; Bordoni, V.; Cardona, X.; Inguaggiato, P.; Pilotto, L.; d’Intini, V.; et al. Interpreting the mechanisms of continuous renal replacement therapy in sepsis: The peak concentration hypothesis. Artif. Organs. 2003, 27, 792–801. [Google Scholar] [CrossRef]
- Rimes-Stigare, C.; Frumento, P.; Bottai, M.; Martensson, J.; Martling, C.R.; Bell, M. Long-term mortality and risk factors for development of end-stage renal disease in critically ill patients with and without chronic kidney disease. Crit. Care 2015, 19, 383. [Google Scholar] [CrossRef] [Green Version]
- Abdalrahim, M.S.; Khalil, A.A.; Alramly, M.; Alshlool, K.N.; Abed, M.A.; Moser, D.K. Pre-existing chronic kidney disease and acute kidney injury among critically ill patients. Heart Lung 2020, 49, 626–629. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Huang, T.M.; Lai, C.F.; Shiao, C.C.; Lin, Y.F.; Chu, T.S.; Wu, P.C.; Chao, C.T.; Wang, J.Y.; Kao, T.W.; et al. Acute-on-chronic kidney injury at hospital discharge is associated with long-term dialysis and mortality. Kidney Int. 2011, 80, 1222–1230. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- Aird, W.C. The hematologic system as a marker of organ dysfunction in sepsis. Mayo Clin. Proc. 2003, 78, 869–881. [Google Scholar] [CrossRef] [Green Version]
- Vincent, J.L.; de Mendonca, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M.; Sprung, C.L.; Colardyn, F.; Blecher, S. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: Results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Melot, C.; Vincent, J.L. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA 2001, 286, 1754–1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, J.L.; Jones, G.; David, S.; Olariu, E.; Cadwell, K.K. Frequency and mortality of septic shock in Europe and North America: A systematic review and meta-analysis. Crit. Care 2019, 23, 196. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Standard UFR (n = 124) | High UFR (n = 142) | p Value | |
|---|---|---|---|
| Background | |||
| Male, n (%) | 83 (66.9) | 95 (66.9) | 0.383 |
| Age (years) | 68.09 ± 14.12 | 65.97 ± 15.52 | 0.264 |
| BMI (kg/m2) | 25.83 ± 4.50 | 23.66 ± 4.58 | <0.001 * |
| Baseline sCr (mg/dL) | 1.55 ± 1.36 | 1.55 ± 1.36 | 0.992 |
| Baseline eGFR (mL/min/1.73 m2) † | 65.32 ± 32.89 | 63.02 ± 38.41 | 0.813 |
| Comorbidity | |||
| Hypertension, n (%) | 80 (64.5) | 70 (49.3) | 0.015 * |
| Diabetes mellitus, n (%) | 62 (50.0) | 12461 (43.0) | 0.286 |
| Liver cirrhosis, n (%) | 16 (12.9) | 21 (14.8) | 0.665 |
| Coronary artery disease, n (%) | 30 (24.2) | 35 (24.6) | 0.982 |
| Congestive heart failure, n (%) | 34 (27.4) | 39 (27.5) | 0.998 |
| COPD/Chronic lung disease, n (%) | 7 (5.6) | 12 (8.5) | 0.425 |
| Cerebrovascular disease, n (%) | 15 (12.1) | 16 (11.3) | 0.965 |
| Advanced CKD ‡, n (%) | 32 (25.8) | 30 (21.1) | 0.434 |
| Malignancy, n (%) | 24 (19.4) | 36 (25.4) | 0.309 |
| Charlson comorbidity index | 6.42 ± 3.25 | 62.23 ± 3.00 | 0.600 |
| Primary ICU service received | |||
| Medical, n (%) | 94 (75.8) | 98 (69.0) | 0.248 |
| Surgical, n (%) | 30 (24.2) | 44 (31.0) | |
| Etiology of acute kidney injury | |||
| Shock, n (%) | 112 (90.3) | 122 (85.9) | 0.310 |
| Sepsis, n (%) | 91 (73.4) | 101 (71.1) | 0.699 |
| Nephrotoxins, n (%) | 18 (14.5) | 13 (9.2) | 0.163 |
| Hepatorenal, n (%) | 7 (5.6) | 12 (8.5) | 0.425 |
| Cardiorenal, n (%) | 4 (3.2) | 5 (3.5) | 0.753 |
| Rhabdomyolysis, n (%) | 5 (4.0) | 5 (3.5) | 0.702 |
| Others, n (%) | 4 (3.2) | 5 (3.5) | 0.753 |
| Outcomes | |||
| Length of hospital stay (days) | 31.23 ± 32.37 | 30.34 ± 32.11 | 0.808 |
| Length of ICU stay (days) | 16.71 ± 19.71 | 16.36 ± 19.84 | 0.877 |
| Death or critical AAD, n (%) | 93 (75.0) | 103 (72.5) | 0.720 |
| Standard UFR (n = 124) | High UFR (n = 142) | p Value | |
|---|---|---|---|
| Clinical variables | |||
| UFR of CVVH (mL/kg/h) | 22.99 ± 1.97 | 35.14 ± 8.69 | <0.001 * |
| CVVH blood flow (mL/min) | 159.8 ± 23.42 | 158.6 ± 24.67 | 0.735 |
| Interval between admission and CVVH initiation (days) | 4.13 ±1.80 | 2.57 ± 0.38 | 0.024 * |
| Cumulative fluid balance (kg) | 4.41 ± 5.85 | 4.23 ± 8.08 | 0.870 |
| Urine output (mL/kg/hr) | 0.24 ± 0.32 | 0.30 ± 0.53 | 0.242 |
| Body temperature (°C) | 36.65 ± 1.35 | 36.57 ± 1.44 | 0.657 |
| Systolic blood pressure (mmHg) | 82.53 ± 11.99 | 84.34 ± 13.17 | 0.838 |
| Diastolic blood pressure (mmHg) | 42.38 ± 10.21 | 39.06 ± 8.79 | 0.571 |
| MAP (mmHg) | 55.76 ± 10.83 | 54.15 ± 12.72 | 0.747 |
| CVP (mmHg) | 15.41 ± 6.24 | 16.50 ± 6.52 | 0.244 |
| Vasoactive drug use, n (%) | 115 (92.7) | 135 (95.1) | 0.720 |
| PaO2/FIO2 ratio (mmHg) | 218.21 ± 139.03 | 240.52 ± 144.21 | 0.222 |
| MV use, n (%) | 113 (91.1) | 125 (88.0) | 0.389 |
| Diuretic use, n (%) | 72 (58.1) | 83 (58.5) | 0.932 |
| IABP use, n (%) | 13 (10.5) | 11 (7.7) | 0.429 |
| ECMO use, n (%) | 12 (9.7) | 15 (10.6) | 0.752 |
| Indications for CVVH | |||
| Azotemia (BUN > 80 and sCr of >2 mg/dL) with uremic symptoms | 59 (47.58) | 47 (33.10) | 0.252 |
| Oliguria (UO < 100 mL for 8 h) | 111 (89.52) | 121 (85.21) | 0.716 |
| Diuretic-refractory fluid overload (CVP > 12 mmHg or BW increase >10%) | 106 (85.48) | 117 (82.39) | 0.406 |
| Treatment-refractory hyperkalemia (serum potassium >5.5 mmol/L) | 63 (50.81) | 57 (40.14) | 0.195 |
| Treatment-refractory acidosis (HCO3 < 15 mmol/L or pH < 7.25) | 95 (76.61) | 103 (72.54) | 0.628 |
| Laboratory data | |||
| Lactate (mmol/L) | 7.63 ± 5.71 | 7.26 ± 6.53 | 0.682 |
| Albumin (g/dL) | 2.80 ± 0.67 | 2.73 ± 0.69 | 0.464 |
| White blood cell (×103/μL) | 15.57 ± 10.63 | 14.21 ± 12.32 | 0.357 |
| Hemoglobin (g/dL) | 10.15 ± 2.71 | 10.11 ± 2.38 | 0.897 |
| Platelet (×103/μL) | 136.83 ± 100.58 | 133.67 ± 99.53 | 0.804 |
| Arterial blood pH | 7.32 ± 0.12 | 7.33 ± 0.12 | 0.329 |
| Bicarbonate (mmol/L) | 16.65 ± 5.11 | 17.15 ± 5.56 | 0.460 |
| Sodium (mmol/L) | 140.9 ± 8.00 | 139.6 ± 10.09 | 0.280 |
| Potassium (mmol/L) | 4.61 ± 1.15 | 4.51 ± 1.09 | 0.453 |
| Blood urea nitrogen (mg/dL) | 63.65 ± 38.99 | 66.82 ± 43.29 | 0.546 |
| sCr (mg/dL) | 3.47 ± 1.88 | 3.60 ± 2.18 | 0.612 |
| Severity of illness | |||
| SOFA score | 10.37 ± 5.89 | 10.97 ± 6.28 | 0.525 |
| APACHE II score | 22.24 ± 8.13 | 23.39 ± 7.85 | 0.203 |
| Variables | Univariate Analysis | Multivariate Analysis † | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age, years | ||||
| <65 | 1 | |||
| ≥65 | 0.9 (0.66–1.22) | 0.498 | ||
| BMI, kg/m2 | ||||
| <25 | 1 | |||
| ≥25 | 1.31 (0.96–1.79) | 0.584 | ||
| Oliguria | ||||
| No | 1 | |||
| Yes | 1.07 (0.75–1.54) | 0.708 | ||
| Baseline eGFR, mL/min/1.73 m2 | ||||
| ≥60 | 1 | |||
| <60 | 1.93 (1.48–2.88) | 0.005 * | 1.77(1.49–1.92) | 0.017 * |
| Hemoglobin, g/dL | ||||
| ≥10 | 1 | |||
| <10 | 1.43 (1.04–1.96) | 0.029 * | 1.53 (1.10–2.13) | 0.012 * |
| Lactate, mmol/L | ||||
| <4 | 1 | |||
| ≥4 | 1.56 (1.07–2.27) | 0.021 * | 1.28 (0.86–1.89) | 0.227 |
| Albumin, g/dL | ||||
| ≥3.5 | 1 | |||
| <3.5 | 1.74 (0.98–3.06) | 0.057 | 1.43 (0.80–2.55) | 0.225 |
| SOFA score | ||||
| <10 | 1 | |||
| 10–14 | 1.83 (0.92–3.66) | 0.087 | ||
| ≥15 | 2.85 (1.44–5.65) | 0.003 * | 1.92 (1.31–2.83) | <0.001 * |
| APACHE II score | ||||
| <10 | 1 | |||
| 10–19 | 0.92 (0.56–1.50) | 0.737 | ||
| 20–29 | 0.80 (0.59–1.08) | 0.142 | ||
| ≥30 | 1.32 (0.97–1.81) | 0.076 * | 1.16 (0.84–1.60) | 0.360 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.-H.; Ou, S.-M.; Tsai, M.-T.; Tseng, W.-C.; Yang, C.-Y.; Lin, Y.-P.; Tarng, D.-C. AN69 Filter Membranes with High Ultrafiltration Rates during Continuous Venovenous Hemofiltration Reduce Mortality in Patients with Sepsis-Induced Multiorgan Dysfunction Syndrome. Membranes 2021, 11, 837. https://doi.org/10.3390/membranes11110837
Lee K-H, Ou S-M, Tsai M-T, Tseng W-C, Yang C-Y, Lin Y-P, Tarng D-C. AN69 Filter Membranes with High Ultrafiltration Rates during Continuous Venovenous Hemofiltration Reduce Mortality in Patients with Sepsis-Induced Multiorgan Dysfunction Syndrome. Membranes. 2021; 11(11):837. https://doi.org/10.3390/membranes11110837
Chicago/Turabian StyleLee, Kuo-Hua, Shuo-Ming Ou, Ming-Tsun Tsai, Wei-Cheng Tseng, Chih-Yu Yang, Yao-Ping Lin, and Der-Cherng Tarng. 2021. "AN69 Filter Membranes with High Ultrafiltration Rates during Continuous Venovenous Hemofiltration Reduce Mortality in Patients with Sepsis-Induced Multiorgan Dysfunction Syndrome" Membranes 11, no. 11: 837. https://doi.org/10.3390/membranes11110837