
Changes in Mental Health and Preventive Behaviors before and after COVID-19 Vaccination: A Propensity Score Matching (PSM) Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
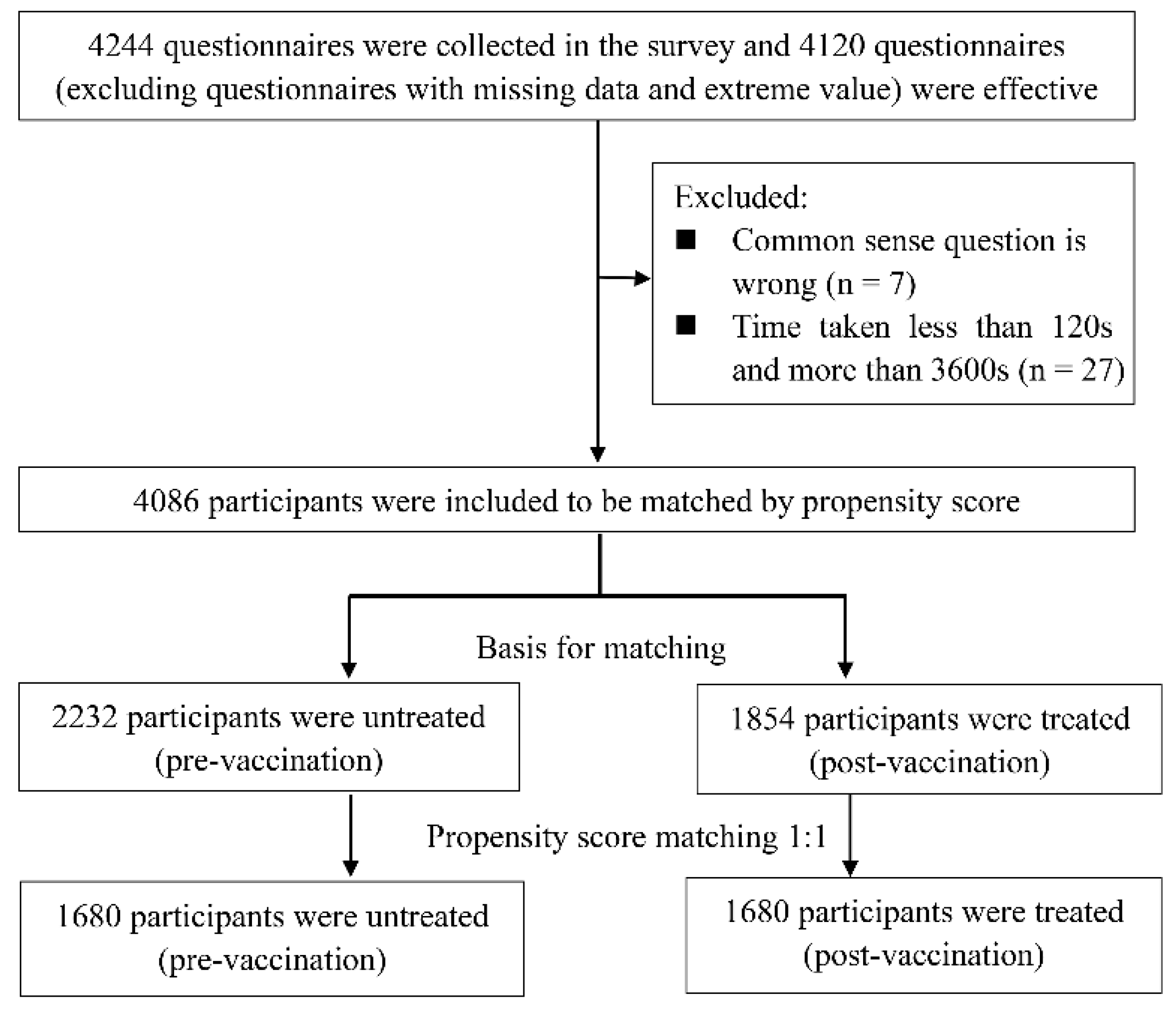
2.1. Study Design and Participants
2.2. Survey Tools
2.3. Definition of Subgroups
2.4. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Associations between Demographic Characteristics with Health Belief, Mental Health, and Preventive Behavior before PSM Treatment
3.3. PSM Treatment to Balance the Participant Characteristics between Pre-Vaccination and Post-Vaccination Groups
3.4. Analysis of Health Belief, Mental Health, and Preventive Behavior between the Pre-Vaccination and Post-Vaccination Groups after PSM Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Davies, N.G.; Abbott, S.; Barnard, R.C.; Jarvis, C.I.; Kucharski, A.J.; Munday, J.D.; Pearson, C.A.B.; Russell, T.W.; Tully, D.C.; Washburne, A.D.; et al. Estimated transmissibility and impact of SARS-CoV-2 lineage B.1.1.7 in England. Science 2021, 372, eabg3055. [Google Scholar] [CrossRef]
- Campbell, F.; Archer, B.; Laurenson-Schafer, H.; Jinnai, Y.; Konings, F.; Batra, N.; Pavlin, B.; Vandemaele, K.; Van Kerkhove, M.D.; Jombart, T.; et al. Increased transmissibility and global spread of SARS-CoV-2 variants of concern as at June 2021. Eurosurveillance 2021, 26, 2100509. [Google Scholar] [CrossRef]
- Lai, S.; Ruktanonchai, N.W.; Zhou, L.; Prosper, O.; Luo, W.; Floyd, J.R.; Wesolowski, A.; Santillana, M.; Zhang, C.; Du, X.; et al. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature 2020, 585, 410–413. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Marziano, V.; Deng, X.; Guzzetta, G.; Zhang, J.; Trentini, F.; Cai, J.; Poletti, P.; Zheng, W.; Wang, W.; et al. Despite vaccination, China needs non-pharmaceutical interventions to prevent widespread outbreaks of COVID-19 in 2021. Nat. Hum. Behav. 2021, 5, 1009–1020. [Google Scholar] [CrossRef] [PubMed]
- Government Council. Press Conference of the Joint Prevention and Control Mechanism of the State Council. Available online: http://www.gov.cn/xinwen/gwylflkjz160/index.htm (accessed on 21 June 2021). (In Chinese)
- Hannah Ritchie, E.O.-O.; Beltekian, D.; Mathieu, E.; Hasell, J.; Macdonald, B.; Giattino, C.; Appel, C.; Rodés-Guirao, L.; Roser, M. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 12 September 2021).
- Chen, M.; Yuan, Y.; Zhou, Y.; Deng, Z.; Zhao, J.; Feng, F.; Zou, H.; Sun, C. Safety of SARS-CoV-2 vaccines: A systematic review and meta-analysis of randomized controlled trials. Infect. Dis. Poverty 2021, 10, 94. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, risk of hospital admission, and vaccine effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Simpson, C.R.; Shi, T.; Vasileiou, E.; Katikireddi, S.V.; Kerr, S.; Moore, E.; McCowan, C.; Agrawal, U.; Shah, S.A.; Ritchie, L.D.; et al. First-dose ChAdOx1 and BNT162b2 COVID-19 vaccines and thrombocytopenic, thromboembolic and hemorrhagic events in Scotland. Nat. Med. 2021, 27, 1–8. [Google Scholar] [CrossRef]
- Wang, R.; Zhang, Q.; Ge, J.; Ren, W.; Zhang, R.; Lan, J.; Ju, B.; Su, B.; Yu, F.; Chen, P.; et al. Analysis of SARS-CoV-2 variant mutations reveals neutralization escape mechanisms and the ability to use ACE2 receptors from additional species. Immunity 2021, 54, 1611–1621. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Chemaitelly, H.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Tang, P.; Hasan, M.R.; Malek, J.A.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. mRNA-1273 COVID-19 vaccine effectiveness against the B.1.1.7 and B.1.351 variants and severe COVID-19 disease in Qatar. Nat. Med. 2021, 27, 1614–1621. [Google Scholar] [CrossRef]
- Chodick, G.; Tene, L.; Rotem, R.S.; Patalon, T.; Gazit, S.; Ben-Tov, A.; Weil, C.; Goldshtein, I.; Twig, G.; Cohen, D.; et al. The effectiveness of the TWO-DOSE BNT162b2 vaccine: Analysis of real-world data. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. Covid-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Tam, C.C.; Li, X.; Li, X.; Wang, Y.; Lin, D. Adherence to preventive behaviors among college students during COVID-19 pandemic in China: The role of health beliefs and COVID-19 stressors. Curr. Psychol. 2021, 11. [Google Scholar] [CrossRef]
- Nochaiwong, S.; Ruengorn, C.; Thavorn, K.; Hutton, B.; Awiphan, R.; Phosuya, C.; Ruanta, Y.; Wongpakaran, N.; Wongpakaran, T. Global prevalence of mental health issues among the general population during the coronavirus disease-2019 pandemic: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 10173. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef] [PubMed]
- Xia Juntao, W.X. Effect of HPV vaccination on psyche and quality of life of patients with HPV infection. Chin. J. Woman Child Health Res. 2020, 31, 399–403. (In Chinese) [Google Scholar]
- Gazibara, T.; Thygesen, L.C.; Algren, M.H.; Tolstrup, J.S. Human Papillomavirus Vaccination and Physical and Mental Health Complaints among Female Students in Secondary Education Institutions in Denmark. J. Gen. Intern. Med. 2020, 35, 2647–2654. [Google Scholar] [CrossRef] [PubMed]
- Harper, J.A.; South, C.; Trivedi, M.H.; Toups, M.S. Pilot investigation into the sickness response to influenza vaccination in adults: Effect of depression and anxiety. Gen. Hosp. Psychiatry 2017, 48, 56–61. [Google Scholar] [CrossRef]
- Santos, A.J.; Kislaya, I.; Machado, A.; Nunes, B. Beliefs and attitudes towards the influenza vaccine in high-risk individuals. Epidemiol. Infect. 2017, 145, 1786–1796. [Google Scholar] [CrossRef] [Green Version]
- Wong, M.C.S.; Wong, E.L.Y.; Huang, J.; Cheung, A.W.L.; Law, K.; Chong, M.K.C.; Ng, R.W.Y.; Lai, C.K.C.; Boon, S.S.; Lau, J.T.F.; et al. Acceptance of the COVID-19 vaccine based on the health belief model: A population-based survey in Hong Kong. Vaccine 2021, 39, 1148–1156. [Google Scholar] [CrossRef]
- Shahnazi, H.; Ahmadi-Livani, M.; Pahlavanzadeh, B.; Rajabi, A.; Hamrah, M.S.; Charkazi, A. Assessing preventive health behaviors from COVID-19: A cross sectional study with health belief model in Golestan Province, Northern of Iran. Infect. Dis. Poverty 2020, 9, 157. [Google Scholar] [CrossRef]
- Chen, M.; Li, Y.; Chen, J.; Wen, Z.; Feng, F.; Zou, H.; Fu, C.; Chen, L.; Shu, Y.; Sun, C. An online survey of the attitude and willingness of Chinese adults to receive COVID-19 vaccination. Hum. Vaccin. Immunother. 2021, 17, 2279–2288. [Google Scholar] [CrossRef]
- Hirschtritt, M.E.; Kroenke, K. Screening for Depression. JAMA 2017, 318, 745–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mercadante, A.R.; Law, A.V. Will they, or Won’t they? Examining patients’ vaccine intention for flu and COVID-19 using the Health Belief Model. Res. Soc. Adm. Pharm. 2020, 17, 1596–1605. [Google Scholar] [CrossRef]
- Scholz, U. It’s Time to Think about Time in Health Psychology. Appl. Psychol. Health Well Being 2019, 11, 173–186. [Google Scholar] [CrossRef]
- Inauen, J.; Bolger, N.; Shrout, P.E.; Stadler, G.; Amrein, M.; Rackow, P.; Scholz, U. Using Smartphone-Based Support Groups to Promote Healthy Eating in Daily Life: A Randomised Trial. Appl. Psychol. Health Well Being 2017, 9, 303–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomes, A.C.R.; Cardoso, G.C. The lag-time constraint for behavioural plasticity. Proc. Biol. Sci. 2020, 287, 20200525. [Google Scholar] [CrossRef] [PubMed]
- Morsky, B.; Akçay, E. Evolution of social norms and correlated equilibria. Proc. Natl. Acad. Sci. USA 2019, 116, 8834–8839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borah, B.J.; Moriarty, J.P.; Crown, W.H.; Doshi, J.A. Application of propensity score methods in observational studies. Chin. J. Evid.-Based Med. 2021, 21, 469–474. (In Chinese) [Google Scholar]
- Wong, L.P.; Alias, H.; Wong, P.F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccin. Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef] [PubMed]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A decade later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.C.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.; Zhou, X.; Wang, Z. Behavioral Intention to Receive a COVID-19 Vaccination Among Chinese Factory Workers: Cross-sectional Online Survey. J. Med. Internet Res. 2021, 23, e24673. [Google Scholar] [CrossRef]
- Saeed, H.; Osama, H.; Madney, Y.M.; Harb, H.S.; Abdelrahman, M.A.; Ehrhardt, C.; Abdelrahim, M.E.A. COVID-19; current situation and recommended interventions. Int. J. Clin. Pract. 2021, 75, e13886. [Google Scholar] [CrossRef]
- Wu, J.; Wang, J.; Nicholas, S.; Maitland, E.; Fan, Q. Application of Big Data Technology for COVID-19 Prevention and Control in China: Lessons and Recommendations. J. Med. Internet Res. 2020, 22, e21980. [Google Scholar] [CrossRef]
- Goularte, J.F.; Serafim, S.D.; Colombo, R.; Hogg, B.; Caldieraro, M.A.; Rosa, A.R. COVID-19 and mental health in Brazil: Psychiatric symptoms in the general population. J. Psychiatr. Res. 2021, 132, 32–37. [Google Scholar] [CrossRef]
- Ames-Guerrero, R.J.; Barreda-Parra, V.A.; Huamani-Cahua, J.C.; Banaszak-Holl, J. Self-reported psychological problems and coping strategies: A web-based study in Peruvian population during COVID-19 pandemic. BMC Psychiatry 2021, 21, 351. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.-W.; Dawei, W.; Majeed, M.T.; Sohail, S. COVID-19 and international trade: Insights and policy challenges in China and USA. Econ. Res.-Ekonomska Istrazivanja 2021. accepted. [Google Scholar] [CrossRef]
- Guangzhou Statistics Bureau. Administrative Division. Available online: http://tjj.gz.gov.cn/gzsq/content/post_2786710.html (accessed on 16 April 2021). (In Chinese)
- Liu, L. The Vaccination Coverage Rate of the Target Population of Suishen Buddha Is More Than 70%. Available online: https://m.gmw.cn/baijia/2021-06/03/1302337056.html (accessed on 21 June 2021). (In Chinese).


{kind=link}
| Demographics | N (%) or Mean (SD) | |
|---|---|---|
| Biological sex | ||
| Male | 2236 (54.7%) | |
| Female | 1850 (45.3%) | |
| Age | 34.23 (10.48) | |
| Education | ||
| Junior high school or below | 655 (16.0%) | |
| High school degree | 952 (23.3%) | |
| Bachelor’s degree | 2243 (54.9%) | |
| Master’s degree or above | 236 (5.8%) | |
| Family monthly per capita income | ||
| RMB <5000 | 1616 (39.5%) | |
| RMB 5000–10,000 | 1491 (36.5%) | |
| RMB 10,001–15,000 | 507 (12.4%) | |
| RMB >15,000 | 472 (11.6%) | |
| Health condition | ||
| Very good | 2588 (63.3%) | |
| Good | 1295 (31.7%) | |
| Average | 203 (5.0%) | |
| Influenza vaccination status (nearly 3 years) | ||
| No vaccination | 3853 (94.3%) | |
| Vaccination, discontinuous | 194 (4.7%) | |
| Vaccination, continuous | 39 (1.0%) | |
| Domestic business trip frequency | ||
| At least twice a month | 120 (2.9%) | |
| About once a month | 187 (4.6%) | |
| About once every 3 months | 295 (7.2%) | |
| About once every 6 months | 526 (12.9%) | |
| Barely | 2958 (72.4%) | |
| Foreign business trip frequency | ||
| At least once every 3 months | 7 (0.2%) | |
| About once every 6 months | 15 (0.4%) | |
| About once a year | 27 (0.7%) | |
| Barely | 4037 (98.8%) | |
| Demographics | HBM | Mental Health | Preventive Behavior | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| M (Q1, Q3) | Z | p-Value | M (Q1, Q3) | Z | p-Value | M (Q1, Q3) | Z | p-Value | ||
| Biological sex | ||||||||||
| Male | 62 (57, 66) | −2.23 | 0.026 | 23 (20, 27) | −1.72 ** | 0.085 | 35 (31, 36) | −2.87 | 0.004 | |
| Female | 61 (56, 66) | 22 (22, 27) | 35 (32, 37) | |||||||
| Education | ||||||||||
| Junior high school or below | 60 (54, 64) | 53.39 | <0.001 | 24 (21, 27) | 65.20 * | <0.001 | 36 (33, 36) | 69.75 | <0.010 | |
| High school degree | 61 (56, 66) | 23 (20, 27) | 36 (33, 37) | |||||||
| Bachelor’s degree | 62 (57, 66) | 22 (19, 26) | 34 (30, 36) | |||||||
| Master’s degree or above | 62 (58, 66) | 22 (19, 25) | 34 (30, 36) | |||||||
| Family monthly per capita income | ||||||||||
| RMB <5000 | 60 (56, 64) | 76.62 | <0.010 | 23 (20, 27) | 38.35 * | <0.001 | 35 (32, 36) | 17.29 | <0.001 | |
| RMB 5000−10,000 | 62 (57, 66) | 22 (20, 26) | 35 (31, 37) | |||||||
| RMB 10,001–15,000 | 62 (58, 66) | 22 (20, 25) | 34 (30, 36) | |||||||
| RMB >15,000 | 63 (58, 67) | 22 (19, 25) | 34 (30, 37) | |||||||
| Influenza vaccination status (nearly 3 years) | ||||||||||
| No vaccination | 61 (57, 66) | 1.46 | 0.482 | 23 (20, 27) | 4.57 * | 0.102 | 35 (31, 36) | 4.91 | 0.086 | |
| Vaccination, discontinuous | 61 (56, 65) | 22 (19, 26) | 34 (30, 36) | |||||||
| Vaccination, continuous | 61 (55, 64) | 24 (20, 28) | 35 (33, 39) | |||||||
| Domestic business trip frequency (nearly 1 year) | ||||||||||
| At least twice a month | 62 (57, 65) | 23.79 | <0.001 | 23 (19, 27) | 7.08 * | 0.132 | 33 (28, 36) | 46.50 | <0.001 | |
| At least once a month | 62 (57, 66) | 23 (20, 26) | 34 (30, 36) | |||||||
| At least once every 3 months | 63 (58, 67) | 22 (19, 26) | 34 (29, 36) | |||||||
| At least once every 6 months | 62 (58, 67) | 23 (20, 26) | 34 (31, 36) | |||||||
| Barely | 61 (56, 65) | 23 (20, 27) | 35 (32, 37) | |||||||
| Foreign business trip frequency (nearly 1 year) | ||||||||||
| At least once every 3 months | 58 (54, 69) | 0.92 | 0.821 | 28 (20, 31) | 15.73 * | <0.001 | 38 (22, 39) | 0.67 | 0.879 | |
| At least once every 6 months | 62 (58, 67) | 27 (23, 30) | 34 (29, 36) | |||||||
| At least once a year | 59 (55, 66) | 24 (21, 27) | 34 (31, 36) | |||||||
| Barely | 61 (57, 66) | 23 (20, 27) | 35 (31, 36) | |||||||
| Vaccination | ||||||||||
| Pre-vaccination | 61 (57, 65) | −0.46 | 0.643 | 23 (20, 26) | −3.01 ** | 0.003 | 35 (31, 36) | −0.67 | 0.500 | |
| Post-vaccination | 62 (55, 67) | 24 (20, 27) | 36 (30, 36) | |||||||
| Demographic Characteristics | Before PSM Treatment | SMD | p-Value | After PSM Treatment | SMD | p-Value | |||
|---|---|---|---|---|---|---|---|---|---|
| Pre-Vaccination | Post-Vaccination | Pre-Vaccination | Post-Vaccination | ||||||
| n = 2232 (%) | n = 1854 (%) | n = 1680 (%) | n = 1680 (%) | ||||||
| Biological sex | |||||||||
| Male | 1190 (53.3) | 1046 (56.4) | 0.06 | 0.041 | 912 (54.3) | 944 (56.2) | 0.02 | 0.508 | |
| Female | 1042 (46.7) | 808 (43.6) | 768 (45.7) | 736 (43.8) | |||||
| Age | 32.9 | 35.8 | 0.28 | <0.001 | 32.50 | 35.25 | 0.01 | 0.822 | |
| Education | |||||||||
| Junior high school or below | 286 (12.8) | 370 (19.9) | 0.28 | <0.001 | 224 (13.3) | 330 (19.6) | 0.02 | 0.617 | |
| High school degree | 438 (19.6) | 514 (27.7) | 345 (20.5) | 460 (27.4) | |||||
| Bachelor’s degree | 1372 (61.4) | 872 (47.0) | 1056 (62.9) | 819 (48.8) | |||||
| Master’s degree or above | 137 (6.1) | 99 (5.3) | 55 (3.3) | 71 (4.2) | |||||
| Family monthly per capita income | |||||||||
| RMB <5000 | 772 (34.6) | 845 (45.6) | 0.24 | <0.001 | 682 (40.6) | 799 (47.6) | 0.01 | 0.715 | |
| RMB 5000–10,000 | 847 (37.9) | 644 (34.7) | 651 (38.8) | 572 (34.0) | |||||
| RMB 10,001–15,000 | 308 (13.8) | 200 (10.8) | 196 (11.7) | 160 (9.5) | |||||
| RMB >15,000 | 306 (13.7) | 166 (8.9) | 151 (9.0) | 149 (8.9) | |||||
| Variable | Vaccination Status | Z | p-Value | ||
|---|---|---|---|---|---|
| Pre-Vaccination (n = 1680) | Post-Vaccination (n = 1680) | ||||
| HBM | 62 (57, 66) | 61 (56, 65) | −2.37 | 0.018 | |
| Perceived susceptibility | 11 (8, 12) | 11 (8, 12) | −3.27 | <0.001 | |
| Perceived severity | 22 (20, 25) | 21 (20, 25) | −1.25 | 0.210 | |
| Perceived benefits | 12 (12, 15) | 12 (12, 15) | −1.33 | 0.182 | |
| Perceived barriers | 12 (11, 14) | 13 (12, 14) | −6.87 | <0.001 | |
| Perceived self-efficacy | 12 (12, 14) | 12 (12, 14) | −3.09 | 0.002 | |
| Mental health | 27 (23, 30) | 26 (22, 29) | −2.59 | 0.010 | |
| Preventive behavior | 36 (34, 40) | 36 (35, 41) | −3.67 | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuan, Y.; Deng, Z.; Chen, M.; Yin, D.; Zheng, J.; Liu, Y.; Liu, X.; Zou, H.; Zhang, C.; Sun, C. Changes in Mental Health and Preventive Behaviors before and after COVID-19 Vaccination: A Propensity Score Matching (PSM) Study. Vaccines 2021, 9, 1044. https://doi.org/10.3390/vaccines9091044
Yuan Y, Deng Z, Chen M, Yin D, Zheng J, Liu Y, Liu X, Zou H, Zhang C, Sun C. Changes in Mental Health and Preventive Behaviors before and after COVID-19 Vaccination: A Propensity Score Matching (PSM) Study. Vaccines. 2021; 9(9):1044. https://doi.org/10.3390/vaccines9091044
Chicago/Turabian StyleYuan, Yue, Zhaomin Deng, Musha Chen, Di Yin, Jiazhen Zheng, Yajie Liu, Xinglai Liu, Huachun Zou, Chunhuan Zhang, and Caijun Sun. 2021. "Changes in Mental Health and Preventive Behaviors before and after COVID-19 Vaccination: A Propensity Score Matching (PSM) Study" Vaccines 9, no. 9: 1044. https://doi.org/10.3390/vaccines9091044