
COVID-19 Vaccine Donations—Vaccine Empathy or Vaccine Diplomacy? A Narrative Literature Review

 ,
,  , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
1.1. Vaccine Availability Equals to Vaccine Accessibility, Only for the Global North
1.2. The Humanitarian Imperative of Vaccine Empathy
2. Methods
Inclusion and Exclusion Criteria
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| COVID-19 | The coronavirus disease 2019 |
| UAE | United Arab Emirates |
| U.S. | The United States |
| WHO | World Health Organization |
References
- Duke Global Health Innovation Center. Interactive COVAX Map. Available online: https://launchandscalefaster.org/COVID-19 (accessed on 28 June 2021).
- Su, Z.; Chengbo, Z.; Mackert, M. Understanding the influenza vaccine as a consumer health technology: A structural equation model of motivation, behavioral expectation, and vaccine adoption. J. Commun. Healthc. 2019, 12, 170–179. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of Covid-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Oli, S.; Nepal Is Being Overwhelmed by Covid. We Need Help. Available online: https://www.theguardian.com/commentisfree/2021/may/10/nepal-covid-uk-g7 (accessed on 12 May 2021).
- The Lancet. COVID-19 in India: The dangers of false optimism. Lancet 2020, 396, 867. [Google Scholar] [CrossRef]
- Our World in Data. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 28 June 2021).
- Johns Hopkins University. The COVID-19 Global Map. Available online: https://coronavirus.jhu.edu/map.html (accessed on 2 August 2021).
- Su, Z.; McDonnell, D.; Cheshmehzangi, A.; Li, X.; Maestro, D.; Šegalo, S.; Ahmad, J. With great hopes come great expectations: Access and adoption issues associated with COVID-19 vaccines. JMIR Public Health Surveill 2021, 10, 26111. [Google Scholar] [CrossRef] [PubMed]
- Su, Z.; Wen, J.; Abbas, J.; McDonnell, D.; Cheshmehzangi, A.; Li, X.; Ahmad, J.; Šegalo, S.; Maestro, D.; Cai, Y. A race for a better understanding of COVID-19 vaccine non-adopters. Brain Behav. Immun. Health 2020, 9, 100159. [Google Scholar] [CrossRef]
- Su, Z.; Wen, J.; McDonnell, D.; Goh, E.; Li, X.; Šegalo, S.; Ahmad, J.; Cheshmehzangi, A.; Xiang, Y.-T. Vaccines are not yet a silver bullet: The imperative of continued communication about the importance of COVID-19 safety measures. Brain Behav. Immun. Health 2021, 12, 100204. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVAX: Working for Global Equitable Access to COVID-19 Vaccines. Available online: https://www.who.int/initiatives/act-accelerator/covax (accessed on 9 May 2021).
- Nhamo, G.; Chikodzi, D.; Kunene, H.P.; Mashula, N. COVID-19 vaccines and treatments nationalism: Challenges for low-income countries and the attainment of the SDGs. Glob. Public Health 2021, 16, 319–339. [Google Scholar] [CrossRef] [PubMed]
- The Economist. Covid-19 Vaccine Donations Have Yet to Take Off. Available online: https://www.economist.com/graphic-detail/2021/05/05/covid-19-vaccine-donations-have-yet-to-take-off (accessed on 8 May 2021).
- Mueller, B.; Robbins, R. Where a Vast Global Vaccination Program Went Wrong. Available online: https://www.nytimes.com/2021/08/02/world/europe/covax-covid-vaccine-problems-africa.html (accessed on 3 August 2021).
- Eaton, L. Covid-19: WHO warns against “vaccine nationalism” or face further virus mutations. BMJ 2021, 372, n292. [Google Scholar] [CrossRef] [PubMed]
- Corum, J.; Zimmer, C. Coronavirus Variants and Mutations. Available online: https://nyti.ms/3jue0k1 (accessed on 2 July 2021).
- Guidry, J.P.D.; Perrin, P.B.; Laestadius, L.I.; Vraga, E.K.; Miller, C.A.; Fuemmeler, B.F.; Burton, C.W.; Ryan, M.; Carlyle, K.E. U.S. public support for COVID-19 vaccine donation to low- and middle-income countries during the COVID-19 pandemic. Vaccine 2021, 39, 2452–2457. [Google Scholar] [CrossRef] [PubMed]
- Kobierecka, A.; Kobierecki, M.M. Coronavirus diplomacy: Chinese medical assistance and its diplomatic implications. Int. Politics 2021, 1–18. [Google Scholar] [CrossRef]
- Baraniuk, C. Covid-19: What do we know about Sputnik V and other Russian vaccines? BMJ 2021, 372, n743. [Google Scholar] [CrossRef] [PubMed]
- Aisha Ibrahim Mohammed, D.S.C.C. The global vaccine competitions: An overview of COVID-19. Eur. J. Mol. Clin. Med. 2021, 7, 3882–3898. [Google Scholar]
- Usher, A.D. Uncertainties over EU COVID-19 vaccine sharing scheme. Lancet 2021, 397, 1171. [Google Scholar] [CrossRef]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Ramírez, J.; Valdivia, L.; Rivera, E.; da Silva Santos, M.; Sepúlveda, D.; Labonté, R.; Ruckert, A. Chile’s role in global health diplomacy: A narrative literature review. Glob. Health 2018, 14, 108. [Google Scholar] [CrossRef] [PubMed]
- AlKhaldi, M.; James, N.; Chattu, V.K.; Ahmed, S.; Meghari, H.; Kaiser, K.; Ijsselmuiden, C.; Tanner, M. Rethinking and strengthening the global health diplomacy through triangulated nexus between policy makers, scientists and the community in light of COVID-19 global crisis. Glob. Health Res. Policy 2021, 6, 12. [Google Scholar] [CrossRef] [PubMed]
- Bollyky, T.J. A Year Out: Addressing International Impacts of the COVID-19 Pandemic; Council on Foreign Relations: New York, NY, USA, 2021. [Google Scholar]
- Chattu, V.K.; Pooransingh, S.; Allahverdipour, H. Global health diplomacy at the intersection of trade and health in the COVID-19 era. Health Promot. Perspect. 2021, 11, 1–4. [Google Scholar] [CrossRef]
- Javed, S.; Chattu, V.K. Strengthening the COVID-19 pandemic response, global leadership, and international cooperation through global health diplomacy. Health Promot. Perspect. 2020, 10, 300–305. [Google Scholar] [CrossRef]
- Lancet Commission on Covid-Vaccines Therapeutics Task Force Members. Operation Warp Speed: Implications for global vaccine security. Lancet Glob Health 2021, 9, e1017–e1021. [CrossRef]
- Pannu, J.; Barry, M. The state inoculates: Vaccines as soft power. Lancet Glob. Health 2021, 9, e744–e745. [Google Scholar] [CrossRef]
- Sharun, K.; Dhama, K. COVID-19 vaccine diplomacy and equitable access to vaccines amid ongoing pandemic. Arch. Med. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Sharun, K.; Dhama, K. India’s role in COVID-19 vaccine diplomacy. J. Travel Med. 2021. [Google Scholar] [CrossRef]
- Vanderslott, S.; Marks, T. Health diplomacy across borders: The case of yellow fever and COVID-19. J. Travel Med. 2020, 27, taaa112. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, N.; Saaliq, S. Vaccine Inequality in India Sends Many Falling through Gaps. Available online: https://apnews.com/article/india-technology-coronavirus-pandemic-business-health-9fc262598b4a6e1fc5ff223fdd748cea (accessed on 29 May 2021).
- Palmer, J. China’s Vaccine Diplomacy Has Mixed Results. Available online: https://foreignpolicy.com/2021/04/07/china-coronavirus-vaccine-diplomacy-sinovac-sinopharm-mixed-results/ (accessed on 12 May 2021).
- Jennings, M. Vaccine Diplomacy: How Some Countries Are Using COVID to Enhance Their Soft Power. Available online: https://theconversation.com/vaccine-diplomacy-how-some-countries-are-using-covid-to-enhance-their-soft-power-155697 (accessed on 12 May 2021).
- Hui, M. China’s Vaccine Diplomacy Has an Aggressive Anti-Vax Element. Available online: https://qz.com/1959855/chinas-coronavirus-vaccine-diplomacy-is-anti-vax/ (accessed on 12 May 2021).
- Lagman, J.D.N. Vaccine nationalism: A predicament in ending the COVID-19 pandemic. J. Public Health 2021, 43, e375–e376. [Google Scholar] [CrossRef] [PubMed]
- Agren, D.; Cecco, L. US to Send 4m AstraZeneca Vaccine Doses to Mexico and Canada. Available online: https://www.theguardian.com/world/2021/mar/18/us-astrazeneca-vaccine-doses-mexico-canada (accessed on 12 May 2021).
- Muthanna, K.A. Military diplomacy. J. Def. Stud. 2011, 5, 1–15. [Google Scholar]
- Amiruddin, A.; Fueggle, S.N.; Nguyen, A.T.; Gignac, G.E.; Clunies-Ross, K.L.; Fox, A.M. Error monitoring and empathy: Explorations within a neurophysiological context. Psychophysiology 2017, 54, 864–873. [Google Scholar] [CrossRef] [PubMed]
- The Times of India. WHO Chief Slams ‘Vaccine Diplomacy’ in Covid Fight. Available online: https://timesofindia.indiatimes.com/world/europe/who-chief-slams-vaccine-diplomacy-in-covid-fight/articleshow/82542370.cms (accessed on 12 May 2021).
- Hotez, P.J. Peace through vaccine diplomacy. Science 2010, 327, 1301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotez, P.J. “Vaccine diplomacy”: Historical perspectives and future directions. PLoS Negl. Trop. Dis. 2014, 8, e2808. [Google Scholar] [CrossRef]
- Hotez, P.J. Russian–United States vaccine science diplomacy: Preserving the legacy. PLoS Negl. Trop. Dis. 2017, 11, e0005320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhuyan, A. Experts criticise India’s complacency over COVID-19. Lancet 2021, 397, 1611–1612. [Google Scholar] [CrossRef]


{kind=link}
| Theme | Search String |
|---|---|
| Vaccine Diplomacy | diplomacy(MeSH) OR diplomacy(TIAB) OR “health diplomacy” (MeSH) OR “health diplomacy” (TIAB) OR “medical diplomacy” (MeSH) OR “medical diplomacy”(TIAB) OR “vaccine diplomacy” (MeSH) OR “vaccine diplomacy” (TIAB) OR “science diplomacy” (MeSH) OR “science diplomacy” (TIAB) |
| COVID-19 | ((coronavirus OR “corona virus” OR coronavirinae OR coronaviridae OR betacoronavirus OR covid19 OR “covid 19” OR nCoV OR “CoV 2” OR CoV2 OR sarscov2 OR 2019nCoV OR “novel CoV” AND (“severe acute respiratory” OR pneumonia) AND (outbreak)) OR “Coronavirus”(Mesh) OR “Coronavirus Infections”(Mesh) OR “COVID-19” (Supplementary Concept) OR “severe acute respiratory syndrome coronavirus 2” (Supplementary Concept) OR “Betacoronavirus”(Mesh)) |
| Data Type | Inclusion Criteria |
|---|---|
| Language | English |
| Study context | Vaccine diplomacy in the wake of COVID-19 |
| Vaccine type | COVID-19 vaccines |
| Study design | Provides detailed information on the attributes and effects of vaccine diplomacy in the context of COVID-19 |
| Author | Year | Country * | Title | Policy Focus | Vaccine Diplomacy Position |
|---|---|---|---|---|---|
| AlKhaldi et al. [25] | 2021 | Canada | Rethinking and strengthening the Global Health Diplomacy through triangulated nexus between policy makers, scientists, and the community in light of the COVID-19 global crisis | Global | For |
| Bollyky et al. [26] | 2021 | U.S. | A year out: Addressing international impacts of the COVID-19 pandemic | U.S. | For |
| Chattu et al. [27] | 2021 | Canada | Global health diplomacy at the intersection of trade and health in the COVID-19 era | Global | For |
| Guidry et al. [18] | 2021 | U.S. | U.S. public support for COVID-19 vaccine donation to low- and middle-income countries during the COVID-19 pandemic | U.S. | For |
| Javed et al. [28] | 2020 | China | Strengthening the COVID-19 pandemic response, global leadership, and international cooperation through global health diplomacy | Global | For |
| Kobierecka et al. [19] | 2021 | Poland | Coronavirus diplomacy: Chinese medical assistance and its diplomatic implications | China | For |
| Lancet Commission on COVID-19 Vaccines and Therapeutics Task Force Members [29] | 2021 | U.K. | Operation Warp Speed: Implications for global vaccine security | Global | For |
| Pannu et al. [30] | 2021 | U.S. | The state inoculates: Vaccines as soft power | Global | Against |
| Sharun et al. [31] | 2021 | India | COVID-19 vaccine diplomacy and equitable access to vaccines amid ongoing pandemic | India | For |
| Sharun et al. [32] | 2021 | India | India’s role in COVID-19 vaccine diplomacy | India | For |
| Usher et al. [22] | 2021 | U.K. | Uncertainties over EU COVID-19 vaccine sharing scheme | EU | Against |
| Vanderslott et al. [33] | 2020 | U.K. | Health diplomacy across borders: The case of yellow fever and COVID-19 | Global | For |
| Empathy | Vaccine Empathy | Diplomacy | Vaccine Diplomacy | |
|---|---|---|---|---|
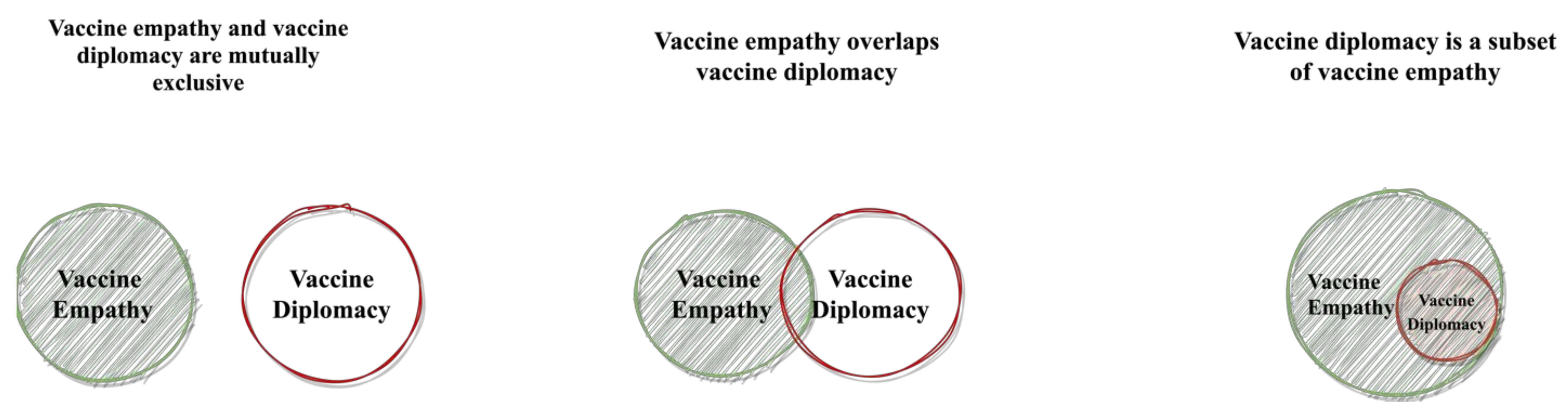
| Definition | Empathy is “noticing another person’s feelings, making an inference of the mental state of another, and responding appropriately to that person’s state of mind.” [41] | Vaccine empathy is an individual or a nation’s capability to sympathize with other individuals or nations’ vaccine wants and needs. | Diplomacy is defined as “the art of conducting relationships for gain without conflict.” [40] | Vaccine diplomacy is a nation’s vaccine efforts that aim to build mutually beneficial relationships with other nations. |
| Key Stakeholder | Individuals and/or nations | Individuals and/or nations | Nations | Nations |
| Defining Attribute | People or nations act out of (vaccine) empathy are:
| Nations act out of (vaccine) diplomacy considerations are:
| ||
| Outcome |
|
| ||
| Strength & Shortcoming |
|
| ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, Z.; McDonnell, D.; Li, X.; Bennett, B.; Šegalo, S.; Abbas, J.; Cheshmehzangi, A.; Xiang, Y.-T. COVID-19 Vaccine Donations—Vaccine Empathy or Vaccine Diplomacy? A Narrative Literature Review. Vaccines 2021, 9, 1024. https://doi.org/10.3390/vaccines9091024
Su Z, McDonnell D, Li X, Bennett B, Šegalo S, Abbas J, Cheshmehzangi A, Xiang Y-T. COVID-19 Vaccine Donations—Vaccine Empathy or Vaccine Diplomacy? A Narrative Literature Review. Vaccines. 2021; 9(9):1024. https://doi.org/10.3390/vaccines9091024
Chicago/Turabian StyleSu, Zhaohui, Dean McDonnell, Xiaoshan Li, Bindi Bennett, Sabina Šegalo, Jaffar Abbas, Ali Cheshmehzangi, and Yu-Tao Xiang. 2021. "COVID-19 Vaccine Donations—Vaccine Empathy or Vaccine Diplomacy? A Narrative Literature Review" Vaccines 9, no. 9: 1024. https://doi.org/10.3390/vaccines9091024