
Quality and Safety of Vaccines Manufacturing: An Online Survey on Attitudes and Perceptions of Italian Internet Users

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Questionnaire Dissemination
- Sociodemographic information: age (analyzed by age group: 20–29 years, 30–39 years, 40–49 years, >49 years), sex, work or education in the healthcare setting (work/education: HC or not HC) and having offspring (minors/no minors);
- Perceptions and attitudes towards vaccine production: this section included four 5-point Likert scale statements ranging from “totally disagree” to “totally agree” and one open question;
- Perceptions and attitudes towards vaccine components: this section included yes/no and multiple-choice questions;
- Information about vaccines and their production: included one yes/no and one multiple-choice question.
- Questionnaire is available as a Supplementary Materials File S1: Informed Consent, Questionnaire and Tables.
2.2. Statistical Analysis
- For affirmative statements, “1” corresponded to “totally disagree and “5” corresponded to “totally agree”;
- For negative statements, “1” corresponded to “totally agree” and “5” corresponded to “totally disagree.
2.3. Multivariate Logistic Regression Models
3. Results
3.1. Study Population
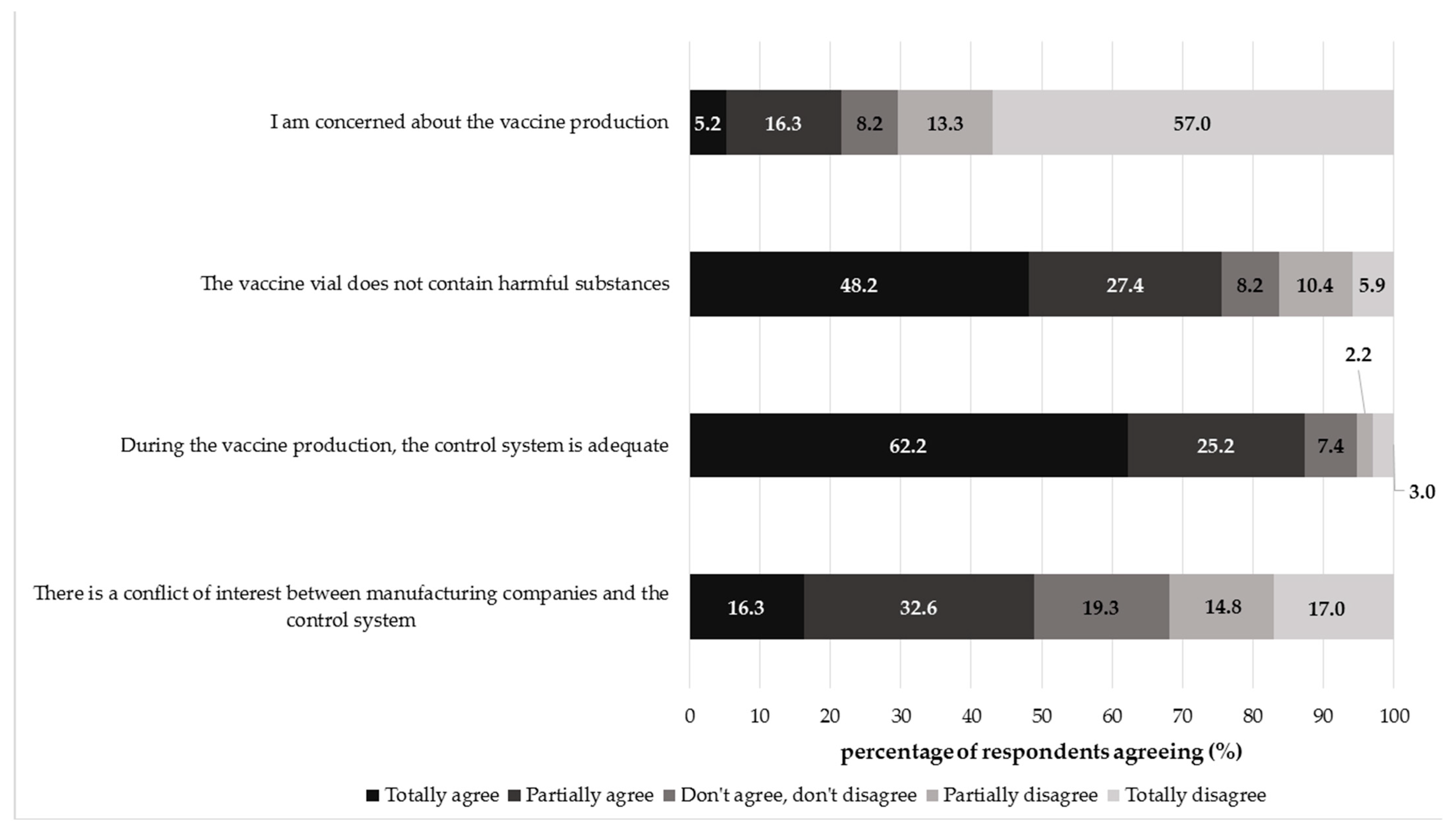
3.2. Perceptions and Attitudes toward the Vaccine Production Process
3.3. Perceptions and Attitudes towards Vaccine Components
3.4. Information about Vaccines and Their Production
3.5. Multivariate Logistic Regression Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO) Immunization. Available online: https://www.who.int/news-room/facts-in-pictures/detail/immunization (accessed on 22 August 2020).
- WHO. International Travel and Health Assessment. Chapter 6—Vaccine-Preventable Diseases and Vaccines (2019 Update). Available online: https://cdn.who.int/media/docs/default-source/travel-and-health/9789241580472-eng-chapter-6.pdf? (accessed on 21 May 2021).
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J.A. Vaccine hesitancy: An overview. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Giambi, C.; Fabiani, M.; D’Ancona, F.; Ferrara, L.; Fiacchini, D.; Gallo, T.; Martinelli, D.; Pascucci, M.G.; Prato, R.; Filia, A.; et al. Parental vaccine hesitancy in Italy—Results from a national survey. Vaccine 2018, 36, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Bechini, A.; Bonanni, P.; Zanella, B.; Di Pisa, G.; Moscadelli, A.; Paoli, S.; Ancillotti, L.; Bonito, B.; Boccalini, S. Vaccine Production Process: How Much Does the General Population Know about This Topic? A Web-Based Survey. Vaccines 2021, 9, 564. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). The Journey of Your Child’s Vaccine. Available online: https://www.cdc.gov/vaccines/parents/infographics/journey-of-child-vaccine.html (accessed on 27 May 2021).
- European Commission. Good Manufacturing Practices (GMP) Guidelines. Available online: https://ec.europa.eu/health/documents/eudralex/vol-4_en (accessed on 27 May 2021).
- Preiss, S.; Garçon, N.; Cunningham, A.L.; Strugnell, R.; Friedland, L.R. Vaccine provision: Delivering sustained & widespread use. Vaccine 2016, 34, 6665–6671. [Google Scholar] [CrossRef] [PubMed]
- WHO. Regulation and Quality Control of Vaccines. Available online: https://www.who.int/biologicals/vaccines/regulation_and_quality_control_vaccines/en/ (accessed on 29 December 2020).
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; De Figueiredo, A.; Xiahong, Z.; Schulz, W.S.; Verger, P.; Johnston, I.; Cook, A.; Jones, N.S. The State of Vaccine Confidence 2016: Global Insights Through a 67-Country Survey. EBioMedicine 2016, 12, 295–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karafillakis, E.; Larson, H.J. The benefit of the doubt or doubts over benefits? A systematic literature review of perceived risks of vaccines in European populations. Vaccine 2017, 35, 4840–4850. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.; Zaytseva, A.; Bocquier, A.; Nokri, A.; Fressard, L.; Chamboredon, P.; Carbonaro, C.; Bernardi, S.; Dubé, E.; Verger, P. Vaccine hesitancy and self-vaccination behaviors among nurses in southeastern France. Vaccine 2020, 38, 1144–1151. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.E. What are the factors that contribute to parental vaccine-hesitancy and what can we do about it? Hum. Vaccines Immunother. 2014, 10, 2584–2596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paterson, P.; Meurice, F.; Stanberry, L.R.; Glismann, S.; Rosenthal, S.L.; Larson, H.J. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to vaccination: A critical review. Soc. Sci. Med. 2014, 112, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ECDC. Let’s Talk about Hesitancy. 2016. Available online: https://www.ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/lets-talk-about-hesitancy-vaccination-guide.pdf (accessed on 21 May 2021).
- Geoghegan, S.; O’Callaghan, K.P.; Offit, P.A. Vaccine Safety: Myths and Misinformation. Front. Microbiol. 2020, 11, 372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caudal, H.; Briend-Godet, V.; Caroff, N.; Moret, L.; Navas, D.; Huon, J. Vaccine distrust: Investigation of the views and attitudes of parents in regard to vaccination of their children. Ann. Pharm. Françaises 2020, 78, 294–302. [Google Scholar] [CrossRef] [PubMed]
- WHO Vaccine Safety Advisory Committee. Macrophagic myofasciitis and aluminum-containing vaccines. Wkly. Epidemiol. Rec. 1999, 74, 338–340. [Google Scholar]
- Baylor, N.W.; Egan, W.; Richman, P. Aluminum salts in vaccines: US perspective. Vaccine 2002, 20, S18–S23. [Google Scholar] [CrossRef]
- Descamps, D.; Hardt, K.; Spiessens, B.; Izurieta, P.; Verstraeten, T.; Breuer, T.; Dubin, G. Safety of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine for cervical cancer prevention: A pooled analysis of 11 clinical trials. Hum. Vaccines 2009, 5, 332–340. [Google Scholar] [CrossRef] [PubMed]
- Salk, J.E.; Bailey, M.L.; Laurent, A.M. The use of adjuvants in studies on influenza immunization: II. increased antibody formation in human subjects inoculated with influenza virus vaccine in a water-in-oil emulsioN123. Am. J. Epidemiol. 1952, 55, 439–456. [Google Scholar] [CrossRef] [PubMed]
- Boccalini, S.; Bonanni, P.; Chiesi, F.; Di Pisa, G.; Furlan, F.; Giammarco, B.; Zanella, B.; Tacconi, F.M.; Bechini, A. The Experience of VaccinarSinToscana Website and the Role of New Media in Promoting Vaccination. Vaccines 2020, 8, 644. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.L.; Zollo, F.; Scala, A.; Betsch, C.; Quattrociocchi, W. Polarization of the vaccination debate on Facebook. Vaccine 2018, 36, 3606–3612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, e210–e221. [Google Scholar] [CrossRef]


{kind=link}
| Sociodemographic Characteristics of the Respondents. | |||
|---|---|---|---|
| n | % (n/N) | ||
| Age group (years) | 20–29 | 48 | 35.6 |
| 30–39 | 51 | 37.8 | |
| 40–49 | 18 | 13.3 | |
| >49 | 18 | 13.3 | |
| Sex | Male | 47 | 34.8 |
| Female | 88 | 65.2 | |
| Work or education in the healthcare setting | Yes | 47 | 34.8 |
| No | 88 | 65.2 | |
| Minor offspring | Yes | 38 | 28.1 |
| No | 97 | 71.9 | |
| Question | Response | Male (n = 47) | Female (n = 88) | Work/Education: HC (n = 47) | Work/Education: not HC (n = 88) | Minor Offspring (n = 38) | No Minor Offspring (n = 97) | Total (n = 135) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | ||
| I am concerned about the vaccine production | Totally agree | 2 | 4.26 | 5 | 5.68 | 1 | 2.13 | 6 | 6.82 | 3 | 7.89 | 4 | 4.12 | 7 | 5.19 |
| Partially agree | 8 | 17.02 | 14 | 15.91 | 5 | 10.64 | 17 | 19.32 | 6 | 15.79 | 16 | 16.49 | 22 | 16.30 | |
| Do not agree, do not disagree | 4 | 8.51 | 7 | 7.95 | 5 | 10.64 | 6 | 6.82 | 4 | 10.53 | 7 | 7.22 | 11 | 8.15 | |
| Partially disagree | 4 | 8.51 | 14 | 15.91 | 7 | 14.89 | 11 | 12.50 | 5 | 13.16 | 13 | 13.40 | 18 | 13.33 | |
| Totally disagree | 29 | 61.70 | 48 | 54.55 | 29 | 61.70 | 48 | 54.55 | 20 | 52.63 | 57 | 58.76 | 77 | 57.04 | |
| p-value | 0.79 | 0.45 | 0.86 | ||||||||||||
| The vaccine vial does not contain harmful substances | Totally agree | 28 | 59.57 | 37 | 42.05 | 28 | 59.57 | 37 | 42.05 | 16 | 42.11 | 49 | 50.52 | 65 | 48.15 |
| Partially agree | 6 | 12.77 | 31 | 35.23 | 8 | 17.02 | 29 | 32.95 | 11 | 28.95 | 26 | 26.80 | 37 | 27.41 | |
| Do not agree, do not disagree | 3 | 6.38 | 8 | 9.09 | 3 | 6.38 | 8 | 9.09 | 4 | 10.53 | 7 | 7.22 | 11 | 8.15 | |
| Partially disagree | 6 | 12.77 | 8 | 9.09 | 3 | 6.38 | 11 | 12.50 | 6 | 15.79 | 8 | 8.25 | 14 | 10.37 | |
| Totally disagree | 4 | 8.51 | 4 | 4.55 | 5 | 10.64 | 3 | 3.41 | 1 | 2.63 | 7 | 7.22 | 8 | 5.93 | |
| p-value | 0.06 | 0.06 | 0.51 | ||||||||||||
| During the vaccine production, the control system is adequate | Totally agree | 34 | 72.34 | 50 | 56.82 | 34 | 72.34 | 50 | 56.82 | 22 | 57.89 | 62 | 63.92 | 84 | 62.22 |
| Partially agree | 7 | 14.89 | 27 | 30.68 | 9 | 19.15 | 25 | 28.41 | 7 | 18.42 | 27 | 27.84 | 34 | 25.19 | |
| Do not agree, do not disagree | 4 | 8.51 | 6 | 6.82 | 1 | 2.13 | 9 | 10.23 | 6 | 15.79 | 4 | 4.12 | 10 | 7.41 | |
| Partially disagree | 1 | 2.13 | 2 | 2.27 | 1 | 2.13 | 2 | 2.27 | 2 | 5.26 | 1 | 1.03 | 3 | 2.22 | |
| Totally disagree | 1 | 2.13 | 3 | 3.41 | 2 | 4.26 | 2 | 2.27 | 1 | 2.63 | 3 | 3.09 | 4 | 2.96 | |
| p-value | 0.34 | 0.25 | 0.08 | ||||||||||||
| There is a conflict of interest between manufacturing companies and control systems | Totally agree | 8 | 17.02 | 14 | 15.91 | 2 | 4.26 | 20 | 22.73 | 11 | 28.95 | 11 | 11.34 | 22 | 16.30 |
| Partially agree | 15 | 31.91 | 29 | 32.95 | 12 | 25.53 | 32 | 36.36 | 13 | 34.21 | 31 | 31.96 | 44 | 32.59 | |
| Do not agree, do not disagree | 10 | 21.28 | 16 | 18.18 | 11 | 23.40 | 15 | 17.05 | 8 | 21.05 | 18 | 18.56 | 26 | 19.26 | |
| Partially disagree | 7 | 14.89 | 13 | 14.77 | 7 | 14.89 | 13 | 14.77 | 4 | 10.53 | 16 | 16.49 | 20 | 14.81 | |
| Totally disagree | 7 | 14.89 | 16 | 18.18 | 15 | 31.91 | 8 | 9.09 | 2 | 5.26 | 21 | 21.65 | 23 | 17.04 | |
| p-value | 0.98 | <0.001 | 0.04 | ||||||||||||
| Question | Response | Male (n = 47) | Female (n = 88) | Work/Education: HC (n = 47) | Work/Education: Not HC (n = 88) | Minor Offpsring (n = 38) | No Minor Offspring (n = 97) | Total (n = 135) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | ||
| Do you think that the microorganism from which the vaccine is derived is treated in a way that makes it harmless and unable to cause the disease? | Yes | 42 | 89.36 | 69 | 78.41 | 45 | 95.74 | 66 | 75.0 | 30 | 78.95 | 81 | 83.51 | 111 | 82.22 |
| No | 5 | 10.64 | 19 | 21.59 | 2 | 4.26 | 22 | 25.0 | 8 | 21.05 | 16 | 16.49 | 24 | 17.78 | |
| p-value | 0.11 | <0.001 | 0.53 | ||||||||||||
| Do you think that the amount of adjuvants (e.g., aluminum salts) in some vaccines is dangerous? | Yes | 4 | 8.51 | 14 | 15.91 | 6 | 12.76 | 12 | 13.64 | 7 | 18.42 | 11 | 11.34 | 18 | 13.33 |
| No | 27 | 57.45 | 51 | 57.95 | 40 | 85.11 | 38 | 43.18 | 20 | 52.63 | 58 | 59.79 | 78 | 57.78 | |
| I do not know what an adjuvant is | 16 | 34.04 | 23 | 26.14 | 1 | 2.13 | 38 | 43.18 | 11 | 28.95 | 28 | 28.87 | 39 | 28.89 | |
| p-value | 0.38 | <0.001 | 0.53 | ||||||||||||
| In your opinion, the precautionary withdrawal of some batches of vaccines indicates that the controls are: | Ineffective and inadequate | 5 | 10.64 | 17 | 19.3 | 2 | 4.26 | 20 | 22.73 | 5 | 13.16 | 17 | 17.53 | 22 | 16.30 |
| High effective so that suspect batches are immediately withdrawn | 42 | 89.36 | 71 | 80.7 | 45 | 95.74 | 68 | 77.27 | 33 | 86.84 | 80 | 82.47 | 113 | 83.70 | |
| p-value | 0.19 | 0.01 | 0.54 | ||||||||||||
| Disagreement toward the Possibility of a Conflict Interest between Manufacturing Companies and the Control System | |||||
|---|---|---|---|---|---|
| Socio-Demographic Characteristic | β | AOR | SE | 95% CI | p-Value |
| AGE (years) | |||||
| 20–29 | 0.208 | 1.23 | 0.69 | 0.32–4.73 | 0.76 |
| 30–39 | 0.743 | 2.10 | 0.71 | 0.53–8.37 | 0.29 |
| 40–49 | 0.472 | 1.60 | 0.87 | 0.29–8.74 | 0.59 |
| >49 | Reference group | - | - | - | - |
| SEX | |||||
| Male | −0.046 | 0.95 | 0.43 | 0.41–2.2 | 0.91 |
| Female | Reference group | - | - | - | - |
| HEALTHCARE WORK/EDUCATION | |||||
| Yes | 0.889 | 2.43 | 0.41 | 1.08–5.48 | 0.03 |
| No | Reference group | - | - | - | |
| MINOR OFFSPRING | |||||
| Yes | −1.387 | 0.25 | 0.56 | 0.08–0.74 | 0.01 |
| No | Reference group | - | - | - | - |
| Significance value H-L test = 0.462 | |||||
| The Microorganism from Which the Vaccine Is Derived Is Treated in a Way That Makes It Harmless and Unable to Cause the Disease | ||||||
|---|---|---|---|---|---|---|
| Socio-Demographic Characteristic | β | AOR | SE | 95% CI | p-Value | |
| AGE (years) | ||||||
| 20–29 | −0.243 | 0.78 | 0.74 | 0.19–3.31 | 0.74 | |
| 30–39 | 1.031 | 2.80 | 0.85 | 0.53–14.73 | 0.22 | |
| 40–49 | 0.814 | 2.26 | 0.96 | 0.35–14.69 | 0.39 | |
| >49 | Reference group | - | - | - | - | |
| SEX | ||||||
| Male | 1.284 | 3.61 | 0.61 | 1.10–11.84 | 0.03 | |
| Female | Reference group | - | - | - | - | |
| HEALTHCARE WORK/EDUCATION | ||||||
| Yes | 2.283 | 9.80 | 0.80 | 2.05–46.92 | 0.004 | |
| No | Reference group | - | - | - | - | |
| MINOR OFFSPRING | ||||||
| Yes | −0.802 | 0.45 | 0.65 | 0.13–1.59 | 0.21 | |
| No | Reference group | - | - | - | - | |
| Significance value H-L test = 0.970 | ||||||
| The Amount of Adjuvants in Some Vaccines Is Not Dangerous | ||||||
| β | AOR | SE | 95% CI | p-value | ||
| AGE (years) | ||||||
| 20–29 | 0.454 | 1.58 | 0.62 | 0.47–5.32 | 0.46 | |
| 30–39 | 1.006 | 2.73 | 0.66 | 0.75–9.98 | 0.13 | |
| 40–49 | −0.361 | 0.70 | 0.78 | 0.15–3.2 | 0.64 | |
| >49 | Reference group | - | - | - | - | |
| SEX | ||||||
| Male | 1.284 | 1.64 | 0.44 | 0.69–3.91 | 0.26 | |
| Female | Reference group | - | - | - | - | |
| HEALTHCARE WORK/EDUCATION | ||||||
| Yes | 1.923 | 6.84 | 0.49 | 2.63–17.82 | <0.001 | |
| No | Reference group | - | - | - | - | |
| MINOR OFFSPRING | ||||||
| Yes | −0.154 | 0.86 | 0.50 | 0.32–2.31 | 0.32 | |
| No | Reference group | - | - | - | - | |
| Significance value H-L test = 0.701 | ||||||
| The Precautionary Withdrawal of Some Batches of Vaccines Indicates That the Controls Are High Effective | ||||||
| β | AOR | SE | 95% CI | p-value | ||
| AGE (years) | ||||||
| 20–29 | −0.468 | 0.63 | 0.778 | 0.14–2.88 | 0.548 | |
| 30–39 | 0.002 | 1.002 | 0.848 | 0.19–5.28 | 0.998 | |
| 40–49 | −0.217 | 0.80 | 0.977 | 0.12–5.46 | 0.824 | |
| >49 | Reference group | - | - | - | - | |
| SEX | ||||||
| Male | 0.922 | 2.51 | 0.588 | 0.79–7.96 | 0.117 | |
| Female | Reference group | - | - | - | - | |
| HEALTHCARE WORK/EDUCATION | ||||||
| Yes | 2.126 | 8.38 | 0.789 | 1.79–39.31 | 0.007 | |
| No | Reference group | - | - | - | - | |
| MINOR OFFSPRING | ||||||
| Yes | 0.397 | 1.49 | 0.657 | 0.41–5.39 | 0.545 | |
| No | Reference group | - | - | - | - | |
| Significance value H-L test = 0.887 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bechini, A.; Zanella, B.; Bonito, B.; Paoli, S.; Di Pisa, G.; Moscadelli, A.; Ancillotti, L.; Bonanni, P.; Boccalini, S. Quality and Safety of Vaccines Manufacturing: An Online Survey on Attitudes and Perceptions of Italian Internet Users. Vaccines 2021, 9, 1015. https://doi.org/10.3390/vaccines9091015
Bechini A, Zanella B, Bonito B, Paoli S, Di Pisa G, Moscadelli A, Ancillotti L, Bonanni P, Boccalini S. Quality and Safety of Vaccines Manufacturing: An Online Survey on Attitudes and Perceptions of Italian Internet Users. Vaccines. 2021; 9(9):1015. https://doi.org/10.3390/vaccines9091015
Chicago/Turabian StyleBechini, Angela, Beatrice Zanella, Benedetta Bonito, Sonia Paoli, Giulia Di Pisa, Andrea Moscadelli, Leonardo Ancillotti, Paolo Bonanni, and Sara Boccalini. 2021. "Quality and Safety of Vaccines Manufacturing: An Online Survey on Attitudes and Perceptions of Italian Internet Users" Vaccines 9, no. 9: 1015. https://doi.org/10.3390/vaccines9091015