
“Vaccine Passports” May Backfire: Findings from a Cross-Sectional Study in the UK and Israel on Willingness to Get Vaccinated against COVID-19

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Participants
2.3. Main Outcome Measures
2.3.1. Psychological Need Satisfaction and Frustration
2.3.2. Vaccination Behaviour
2.3.3. Willingness to Get vaccinated
2.3.4. Attitudes towards “COVID Passports”
2.3.5. Motivations to Get Vaccinated/Not to Get Vaccinated
2.3.6. Demographics
2.4. Power Calculation
2.5. Statistical Analysis
2.6. Pilot Studies
3. Results
3.1. Demographics, Vaccination Status and Willingness to Get Vaccinated
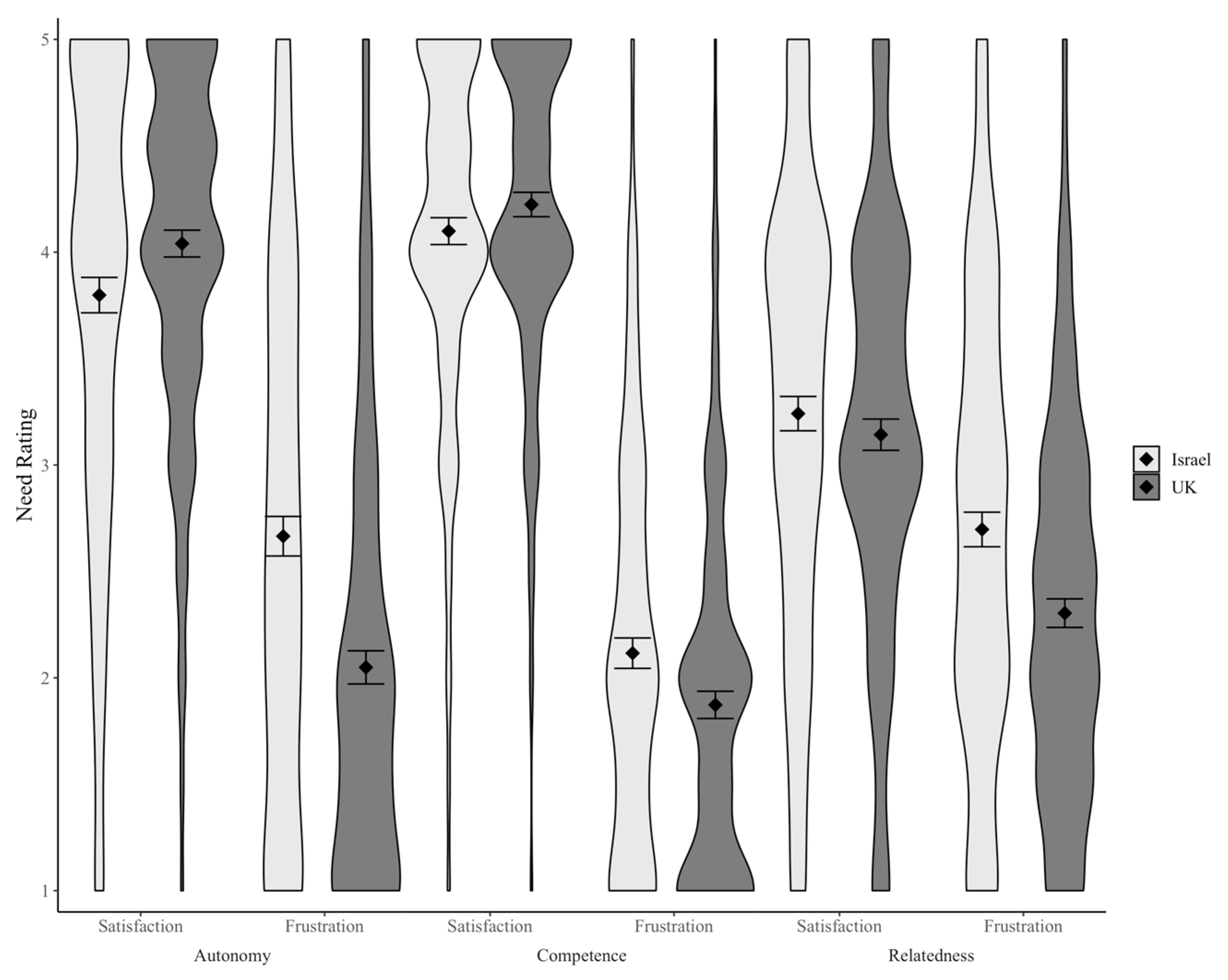
3.2. Psychological Needs
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Roo, S.S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 vaccination program. JAMA 2020, 323, 2458–2459. [Google Scholar]
- Our World in Data (OWiD). Coronavirus (Covid-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 10 May 2021).
- Rosen, B.; Waitzberg, R.; Israeli, A. Israel’s rapid rollout of vaccinations for COVID-19. Isr. J. Health Policy Res. 2021, 6, 10. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Roma, P.; De Giglio, O.; Caggiano, G.; Tafuri, S.; Da Molin, G.; Ferracuti, S.; Montagna, M.T.; Liguori, G.; et al. Knowledge and Acceptance of COVID-19 Vaccination among Undergraduate Students from Central and Southern Italy. Vaccines 2021, 9, 638. [Google Scholar] [CrossRef]
- Balicer, R.D.; Ohana, R. Israel’s COVID-19 endgame. Science 2021, 372, 663. [Google Scholar] [CrossRef]
- Gov.UK Coronavirus (Covid-19) in the UK. Vaccinations in United Kingdom. Available online: https://coronavirus.data.gov.uk/details/vaccinations (accessed on 3 August 2021).
- Voo, T.C.; Reis, A.A.; Thomé, B.; Ho, C.W.; Tam, C.C.; Kelly-Cirino, C.; Emanuel, E.; Beca, J.P.; Littler, K.; Smith, M.J.; et al. Immunity certification for COVID-19: Ethical considerations. Bull. World Health Organ. 2021, 99, 155. [Google Scholar] [CrossRef] [PubMed]
- KFF. Vaccine Passports: What We Know and What to Consider. Available online: https://www.kff.org/coronavirus-covid-19/press-release/vaccine-passports-what-we-know-and-what-to-consider/ (accessed on 15 April 2021).
- The Local Denmark. Denmark Launches New Corona Passport: Here’s What You Need to Know about ‘Coronapas’ App. Available online: https://www.thelocal.dk/20210528/denmark-launches-new-corona-passport-heres-what-you-need-to-know-about-coronapas-app/ (accessed on 28 May 2021).
- Brown, R.C.; Kelly, D.; Wilkinson, D.; Savulescu, J. The scientific and ethical feasibility of immunity passports. Lancet Infect. Dis. 2020, 21, e58–e63. [Google Scholar] [CrossRef]
- Demasi, M.; Gotzsche, P. Rapid Response: Covid-19 vaccine passports are not evidence-based and violate people’s freedom of choice. BMJ 2021, 373, n861. [Google Scholar] [CrossRef]
- Kofler, N.; Baylis, F. Ten reasons why immunity passports are a bad idea. Nature 2020, 581, 379–381. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness; Guilford Press: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Ryan, R.; Patrick, H.; Deci, E.L.; Williams, G.C. Facilitating health behaviour change and its maintenance: Interventions based on self- determination theory. Eur. Health Psychol. 2008, 10, 2–5. [Google Scholar] [CrossRef]
- Ng, J.Y.; Ntoumanis, N.; Thøgersen-Ntoumani, C.; Deci, E.L.; Ryan, R.M.; Duda, J.L.; Williams, G.C. Self-determination theory applied to health contexts: A meta-analysis. Persp. Psychol. Sci. 2012, 7, 325–340. [Google Scholar] [CrossRef]
- Porat, T.; Nyrup, R.; Calvo, R.A.; Paudyal, P.; Ford, E. Public Health and Risk Communication During COVID-19-Enhancing Psychological Needs to Promote Sustainable Behavior Change. Front. Public Health 2020, 8, 637. [Google Scholar] [CrossRef]
- Martela, F.; Hankonen, N.; Ryan, R.M.; Vansteenkiste, M. Motivating voluntary compliance to behavioural restrictions: Self-determination theory-based checklist of principles for COVID-19 and other emergency communications. Eur. Rev. Soc. Psychol. (Print Ed.) 2020, 17, 1–43. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Vansteenkiste, M.; Ryan, R.M. On psychological growth and vulnerability: Basic psychological need satisfaction and need frustration as a unifying principle. J. Psychother. Integr. 2013, 23, 263–280. [Google Scholar] [CrossRef] [Green Version]
- Douglas, K.M.; Sutton, R.M.; Cichocka, A. The psychology of conspiracy theories. Curr. Dir. Psychol. Sci. 2017, 26, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Haerens, L.; Aelterman, N.; Vansteenkiste, M.; Soenens, B.; Van Petegem, S. Do perceived autonomy-supportive and controlling teaching relate to physical education students’ motivational experiences through unique pathways? Distinguishing between the bright and dark side of motivation. Psychol. Sport Exerc. 2015, 16, 26–36. [Google Scholar] [CrossRef]
- Markland, D.; Tobin, V.J. Need support and behavioural regulations for exercise among exercise referral scheme clients: The mediating role of psychological need satisfaction. Psychol. Sport Exerc. 2010, 11, 91–99. [Google Scholar] [CrossRef]
- Pelletier, L.G.; Fortier, M.S.; Vallerand, R.J.; Briere, N.M. Associations among perceived autonomy support, forms of self-regulation, and persistence: A prospective study. Motiv. Emot. 2001, 25, 279–306. [Google Scholar] [CrossRef]
- Prolific. How It Works. Available online: https://www.prolific.co/#researcher-content (accessed on 20 June 2021).
- PanelView. Available online: https://www.panelview-il.com/ (accessed on 10 May 2021).
- Chen, B.; Vansteenkiste, M.; Beyers, W.; Boone, L.; Deci, E.L.; Van der Kaap-Deeder, J.; Duriez, B.; Lens, W.; Matos, L.; Mouratidis, A.; et al. Basic psychological need satisfaction, need frustration, and need strength across four cultures. Motiv. Emot. 2015, 39, 216–236. [Google Scholar] [CrossRef]
- Benita, M.; Benish-Weisman, M.; Matos, L.; Torres, C. Integrative and suppressive emotion regulation differentially predict well-being through basic need satisfaction and frustration: A test of three countries. Motiv. Emot. 2020, 44, 67–81. [Google Scholar] [CrossRef]
- Levesque, C.S.; Williams, G.C.; Elliot, D.; Pickering, M.A.; Bodenhamer, B.; Finley, P.J. Validating the theoretical structure of the Treatment Self-Regulation Questionnaire (TSRQ) across three different health behaviors. Health Educ. Res. 2007, 22, 691–702. [Google Scholar] [CrossRef]
- Ryan, R.M.; Connell, J.P. Perceived locus of causality and internalization: Examining reasons for acting in two domains. J. Pers. Soc. Psychol. 1989, 57, 749–761. [Google Scholar] [CrossRef]
- Carmi, R.; Kasher, A.; Friedman, E.; Yehazkelli, Y.; Qimron, U. Vaccine passports backfire—The case of Israel shows that. The Telegraph, 27 May 2021.
- Del Riccio, M.; Boccalini, S.; Rigon, L.; Biamonte, M.A.; Albora, G.; Giorgetti, D.; Bonanni, P.; Bechini, A. Factors Influencing SARS-CoV-2 Vaccine Acceptance and Hesitancy in a Population-Based Sample in Italy. Vaccines 2021, 9, 633. [Google Scholar] [CrossRef]
- Vansteenkiste, M.; Ryan, R.M.; Soenens, B. Basic psychological need theory: Advancements, critical themes, and future directions. Motiv. Emot. 2020, 44, 1–31. [Google Scholar] [CrossRef] [Green Version]
- Pfefferbaum, B.; North, C.S. Mental health and the Covid-19 pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Psychological Need Satisfaction and Frustration | Cronbach’s Alpha |
|---|---|
| Autonomy satisfaction | α = 0.76 |
| I feel [felt] a sense of choice and freedom in the decision to get vaccinated | |
| I feel [felt] that my decision to get vaccinated reflects what I really want | |
| Autonomy frustration | α = 0.81 |
| I feel [felt] forced to get vaccinated | |
| I feel [felt] that I will [would] be ‘punished’ if I didn’t get vaccinated | |
| Competence satisfaction | α = 0.79 |
| I feel [felt] confident that I could get vaccinated if I wanted to | |
| I feel [felt] capable of getting vaccinated if I wanted to | |
| Competence frustration | α = 0.71 |
| I have [had] serious doubts about whether I could get vaccinated if I wanted to | |
| I feel [felt] that it would be difficult for me to get vaccinated if I wanted to | |
| Relatedness satisfaction | α = 0.85 |
| I feel [felt] that the official authorities care about me | |
| I feel [felt] that the official authorities understand [understood] my needs | |
| Relatedness frustration (α = 0.76) | α = 0.76 |
| I feel [felt] excluded by the official authorities | |
| I feel [felt] that the official authorities are [were] cold and distant |
| Motivations to Get Vaccinated/Not Get Vaccinated | Cronbach’s Alpha |
|---|---|
| Identified motivation | α = 0.72 |
| Because I feel that I want to take responsibility for my own health Because I have carefully thought about it and believe this decision is very important for many aspects of my life | |
| Introjected motivation | α = 0.73 |
| Because I would feel bad about myself if I did [didn’t] get vaccinated | |
| Because I would feel guilty or ashamed of myself if I did [didn’t] get vaccinated | |
| External motivation | α = 0.70 |
| Because I feel under pressure from others [not] to get vaccinated | |
| Because other people would be upset if I do [don’t] get vaccinated | |
| Amotivation | α = 0.58 |
| I really don’t think about it | |
| I don’t really care |
| Characteristics | UK | Israel |
|---|---|---|
| n | 681 | 677 |
| Age | ||
| 18–29 | 18% | 29% |
| 30–59 | 53% | 56% |
| 60+ | 29% | 15% |
| Gender | ||
| Man | 48.5% | 48.5% |
| Woman | 51% | 51.5% |
| Non-binary | 0.5% | 0% |
| Education (Highest Level) | ||
| No formal education | 1% | 1% |
| Primary school | 0% | 1% |
| Secondary school | 34% | 41% |
| Undergraduate degree | 43% | 38% |
| Postgraduate degree | 22% | 19% |
| Vaccination Status | ||
| Unvaccinated | 34% | 14% |
| Single dose | 41% | 4% |
| Two doses | 25% | 82% |
| Coefficients from Linear Regression | |||
|---|---|---|---|
| Term | β | t-Statistic | p |
| autonomy_satisfaction | 0.17 | 5.35 | <0.001 |
| autonomy_frustration | −0.47 | −15.79 | <0.001 |
| competence_satisfaction | 0.05 | 1.52 | 0.128 |
| competence_frustration | 0.07 | 2.66 | 0.008 |
| relatedness_satisfaction | 0.24 | 7.94 | <0.001 |
| relatedness_frustration | 0.09 | 2.88 | 0.004 |
| Coefficients from Logistic Regression | |||
|---|---|---|---|
| Term | Odds Ratio | Statistic | p |
| (Intercept) | −2.83 | −3.28 | <0.001 |
| autonomy_satisfaction | 0.84 | 5.62 | <0.001 |
| autonomy_frustration | 1.21 | 9.08 | <0.001 |
| competence_satisfaction | −0.36 | −2.19 | 0.03 |
| competence_frustration | −0.09 | −0.68 | 0.49 |
| relatedness_satisfaction | −1.13 | −7.74 | <0.001 |
| relatedness_frustration | −0.37 | −2.44 | 0.01 |
| Motivation | Autonomy Frustration | Competence Frustration | Relatedness Frustration |
|---|---|---|---|
| External | 0.32 ** | 0.17 ** | 0.09 * |
| Amotivation | 0.24 ** | 0.17 ** | 0.21 ** |
| Identified | −0.46 ** | −0.24 ** | −0.34 ** |
| Introjected | −0.19 ** | −0.05 | −0.19 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porat, T.; Burnell, R.; Calvo, R.A.; Ford, E.; Paudyal, P.; Baxter, W.L.; Parush, A. “Vaccine Passports” May Backfire: Findings from a Cross-Sectional Study in the UK and Israel on Willingness to Get Vaccinated against COVID-19. Vaccines 2021, 9, 902. https://doi.org/10.3390/vaccines9080902
Porat T, Burnell R, Calvo RA, Ford E, Paudyal P, Baxter WL, Parush A. “Vaccine Passports” May Backfire: Findings from a Cross-Sectional Study in the UK and Israel on Willingness to Get Vaccinated against COVID-19. Vaccines. 2021; 9(8):902. https://doi.org/10.3390/vaccines9080902
Chicago/Turabian StylePorat, Talya, Ryan Burnell, Rafael A. Calvo, Elizabeth Ford, Priya Paudyal, Weston L. Baxter, and Avi Parush. 2021. "“Vaccine Passports” May Backfire: Findings from a Cross-Sectional Study in the UK and Israel on Willingness to Get Vaccinated against COVID-19" Vaccines 9, no. 8: 902. https://doi.org/10.3390/vaccines9080902