
Humoral Response to SARS-Cov-2 Vaccination in Liver Transplant Recipients–A Single-Center Experience

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Characteristics
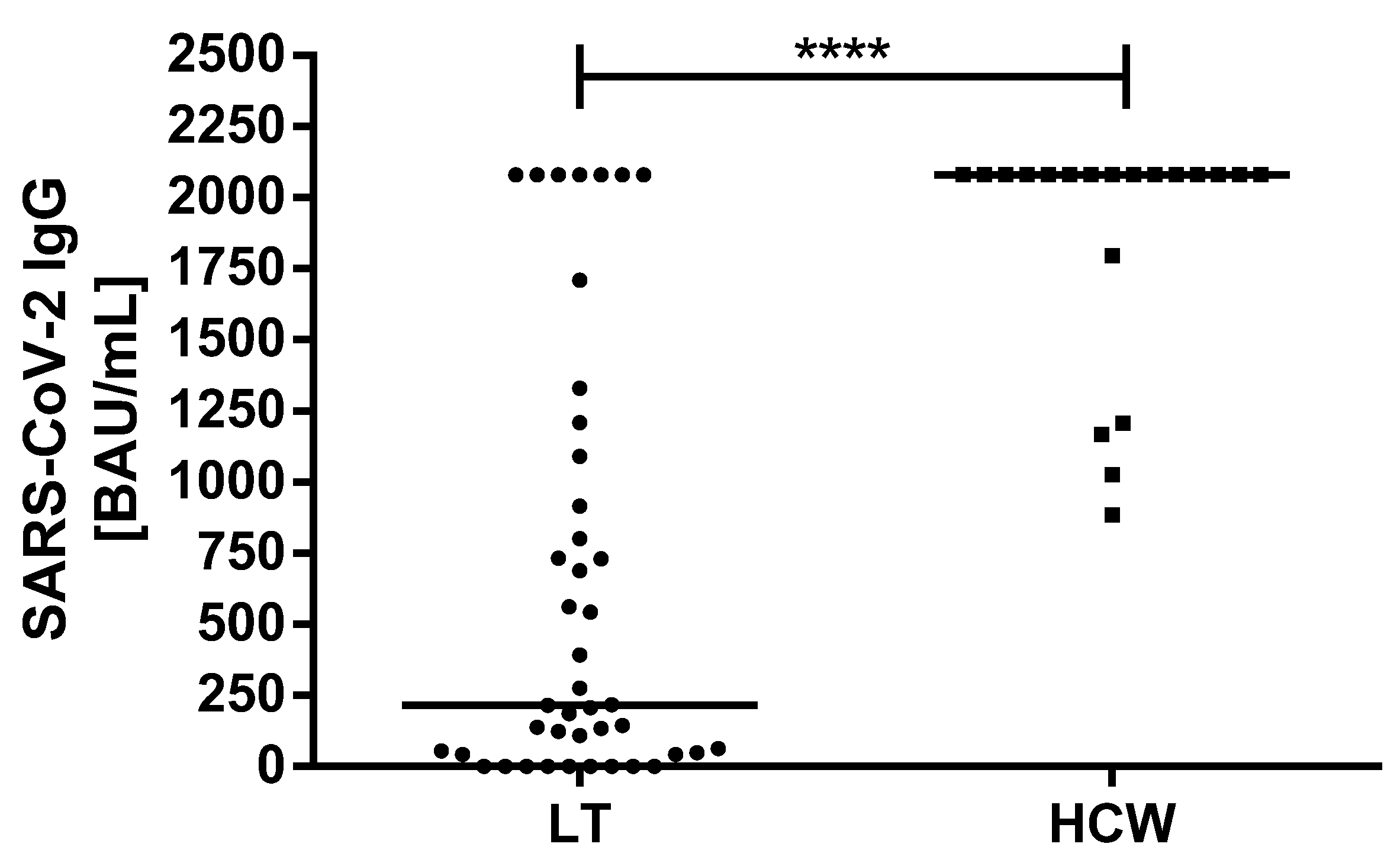
3.2. Antibody Response and Titer after SARS-CoV-2 Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Coronavirus Disease (COVID-2019) Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 10 August 2020).
- Kates, O.S.; Fisher, C.E.; Stankiewicz-Karita, H.C.; Shepherd, A.K.; Church, E.C.; Kapnadak, S.G.; Lease, E.D.; Riedo, F.X.; Rakita, R.M.; Limaye, A.P. Earliest cases of coronavirus disease 2019 (COVID-19) identified in solid organ transplant recipients in the United States. Arab. Archaeol. Epigr. 2020, 20, 1885–1890. [Google Scholar] [CrossRef] [PubMed]
- Hugo, C.; Stecher, M.; Dolff, S.; Nattermann, J.; Vehreschild, J.; Hippchen, T.; Westhoff, T.; Bertolo, M.; Hohenstein, B.; Hanses, F.; et al. Solid organ transplantation is not a risk factor for COVID-19 disease outcome. Transpl. Int. 2021, 34, 378–381. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.J.; Rouphael, N.G.; Widge, A.T.; Jackson, L.A.; Roberts, P.C.; Makhene, M.; Chapell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Safety and Immunogenicity of SARS-CoV-2 mRNA-1273 Vaccine in Older Adults. N. Engl. J. Med. 2020, 383, 2427–2438. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Eckerle, I.; Rosenberger, K.D.; Zwahlen, M.; Junghanss, T. Serologic Vaccination Response after Solid Organ Transplantation: A Systematic Review. PLoS ONE 2013, 8, e56974. [Google Scholar] [CrossRef] [Green Version]
- Kumar, D.; Blumberg, E.A.; Danziger-Isakov, L.; Kotton, C.; Halasa, N.B.; Ison, M.G.; Avery, R.K.; Green, M.; Allen, U.D.; Edwards, K.M.; et al. Influenza Vaccination in the Organ Transplant Recipient: Review and Summary Recommendations. Arab. Archaeol. Epigr. 2011, 11, 2020–2030. [Google Scholar] [CrossRef]
- Stucchi, R.S.; Lopes, M.H.; Kumar, D.; Manuel, O. Vaccine Recommendations for Solid-Organ Transplant Recipients and Donors. Transplant. 2018, 102, S72–S80. [Google Scholar] [CrossRef] [PubMed]
- Cornberg, M.; Buti, M.; Eberhardt, C.S.; Grossi, P.A.; Shouval, D. EASL position paper on the use of COVID-19 vaccines in patients with chronic liver diseases, hepatobiliary cancer and liver transplant recipients. J. Hepatol. 2021, 74, 944–951. [Google Scholar] [CrossRef]
- Fix, O.K.; Blumberg, E.A.; Chang, K.; Chu, J.; Chung, R.T.; Goacher, E.K.; Hameed, B.; Kaul, D.R.; Kulik, L.M.; Kwok, R.M.; et al. AASLD Expert Panel Consensus Statement: Vaccines to Prevent COVID-19 Infection in Patients with Liver Disease. Hepatology 2021. [Google Scholar] [CrossRef] [PubMed]
- Tacke, F.; Cornberg, M.; Sterneck, M.; Trebicka, J.; Settmacher, U.; Bechstein, W.O.; Berg, T.; Gastroenterologie, D.G.; Stoffwechselkrankheiten, V.; Tacke, V.D.F.; et al. S1-Leitlinie zur Versorgung von Lebertransplantierten während der COVID-19-Pandemie—AWMF-Register Nr. 021-031—Stand: 07.01.21. Zeitschrift für Gastroenterologie 2021, 59, 345–359. [Google Scholar] [CrossRef]
- Korth, J.; Jahn, M.; Dorsch, O.; Anastasiou, O.E.; Sorge-Hädicke, B.; Eisenberger, U.; Gäckler, A.; Dittmer, U.; Witzke, O.; Wilde, B.; et al. Impaired Humoral Response in Renal Transplant. Recipients to SARS-CoV-2 Vaccination with BNT162b2 (Pfiz-er-BioNTech). Viruses 2021, 13, 756. [Google Scholar] [CrossRef] [PubMed]
- Marinaki, S.; Adamopoulos, S.; Degiannis, D.; Roussos, S.; Pavlopoulou, I.D.; Hatzakis, A.; Boletis, I.N. Immunogenicity of SARS-CoV-2 BNT162b2 vaccine in solid organ transplant recipients. Arab. Archaeol. Epigr. 2021. [Google Scholar] [CrossRef]
- Rabinowich, L.; Grupper, A.; Baruch, R.; Ben-Yehoyada, M.; Halperin, T.; Turner, D.; Katchman, E.; Levi, S.; Houri, I.; Lubezky, N.; et al. Low Immunogenicity to SARS-CoV-2 Vaccination among Liver Transplant Recipients. J. Hepatol. Available online: https://www.sciencedirect.com/science/article/abs/pii/S0168827821002555 (accessed on 1 July 2021).
- Rozen-Zvi, B.; Yahav, D.; Agur, T.; Zingerman, B.; Ben-Zvi, H.; Atamna, A.; Tau, N.; Mashraki, T.; Nesher, E.; Rahamimov, R. Antibody response to SARS-CoV-2 mRNA vaccine among kidney transplant recipients: A prospective cohort study. Clin. Microbiol. Infect. 2021, 21. [Google Scholar] [CrossRef]
- Benseler, V.; Mccaughan, G.; Schlitt, H.J.; Bishop, G.A.; Bowen, D.G.; Bertolino, P. The Liver: A Special Case in Transplantation Tolerance. Semin. Liver Dis. 2007, 27, 194–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clavien, P.-A.; Muller, X.; de Oliveira, M.L.; Dutkowski, P.; Sanchez-Fueyo, A. Can immunosuppression be stopped after liver transplantation? Lancet Gastroenterol. Hepatol. 2017, 2, 531–537. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Immunogenicity of a single dose of SARS-CoV-2 messenger RNA vaccine in solid organ transplant recipients. Jama 2021, 325, 1784–1786. [Google Scholar] [CrossRef] [PubMed]
- Fischinger, S.; Boudreau, C.; Butler, A.L.; Streeck, H.; Alter, G. Sex differences in vaccine-induced humoral immunity. Semin. Immunopathol. 2019, 41, 239–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Bello, A.; Marion, O.; Delas, A.; Congy-Jolivet, N.; Colombat, M.; Kamar, N. Acute rejection after anti-SARS-CoV-2 mRNA vaccination in a kidney-transplant patient. Kidney Int. 2021, 100, 238–239. [Google Scholar] [CrossRef] [PubMed]
- Vyhmeister, R.; Enestvedt, C.K.; VanSandt, M.; Schlansky, B. Steroid-resistant acute cellular rejection of the liver after SARS-CoV-2 mRNA vaccination. Liver Transplant. 2021. [Google Scholar] [CrossRef]


{kind=link}
| Patient Characteristics | LT Recipients n/(%) | HCWs n/(%) | p-Value |
|---|---|---|---|
| Total patient number | 43 | 20 | - |
| Sex (male/female) | 26(60.5)/17 (39.5) | 9 (45)/11 (55) | 0.286 |
| SARS-CoV-2 IgG detectability rate | 34 (79) | 20 (100) | 0.047 |
| Median (IQR) | Median (IQR) | ||
| Age of recipient at LT [years] | 47 (36–54) | - | - |
| Time between LT and first dose [years] | 8 (4–12) | - | - |
| Age at first dose [years] | 57 (49–64) | 43.5 (38–53.5) | 0.002 |
| Time between first and second doses [days] | 26 (21–37) | 22 | 0.448 |
| Time between second dose and SARS-CoV-2 Ab detection [days] | 15 (12–24) | 13 | 0.033 |
| SARS-CoV-2 IgG (BAU/mL) | 216 (43.4–1090) | >2080 (1865.5 to >2080) | 0.0001 |
| Indication for LT | n (%) |
|---|---|
| Hepatocellular carcinoma | 10 (23) |
| Primary sclerosing cholangitis | 7 (16) |
| Alcohol-induced liver cirrhosis | 6 (14) |
| Hepatitis C virus-induced liver cirrhosis | 3 (7) |
| Acute liver failure | 3 (7) |
| Wilson’s disease | 3 (7) |
| Cryptogenic liver cirrhosis | 2 (4.7) |
| α-1 antitrypsin deficiency | 2 (4.7) |
| Others 1 | 7 (16) |
| Immunosuppressive Therapy | n (%) |
|---|---|
| Tacrolimus-based | 40 (93) |
| Tacrolimus + everolimus | 22 (55) |
| Tacrolimus + MMF | 11 (28) |
| Tacrolimus monotherapy | 7 (18) |
| Cyclosporine A | 2 (5) |
| Everolimus | 1 (2) |
| Patient Characteristics | LT Recipients SARS-CoV-2 IgG Positive n/(%) | LT Recipients SARS-CoV-2 IgG Negative n/(%) | p-Value |
|---|---|---|---|
| Total patient number | 34 (79) | 9 (21) | - |
| Sex (male/female) | 20 (59)/14 (41) | 6 (67)/3 (33) | 1.00 |
| Immunosuppression | |||
| Tacrolimus (n = 40) | 31 (77.5) | 9 (22.5) | 1.00 |
| No Tacrolimus (n = 3) | 3 (100) | - | |
| Everolimus (n = 23) | 20 (87) | 3 (13) | 0.26 |
| No Everolimus (n = 20) | 14 (70) | 6 (30) | |
| MMF (n = 11) | 5 (45.5) | 6 (54.5) | 0.004 |
| No MMF (n = 32) | 29 (90.6) | 3 (9.4) | |
| Median (IQR) | Median (IQR) | ||
| Age of recipient at LT [years] | 48.5 (36–54) | 45 (40–55) | 0.97 |
| Time between LT and first dose [years] | 6.5 (3.7-12) | 12 (5.5-14.5) | 0.10 |
| Age at first dose [years] | 56.5 (46–64) | 59 (53.5-64.5) | 0.35 |
| Time between first and second doses [days] | 28 (21–37) | 21 (21–40) | 0.55 |
| Time between second dose and SARS-CoV-2 Ab detection [days] | 14 (12–25) | 15 (13–25) | 0.85 |
| SARS-CoV-2 IgG (BAU/mL) | 552.7 (137.3-1425) | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rashidi-Alavijeh, J.; Frey, A.; Passenberg, M.; Korth, J.; Zmudzinski, J.; Anastasiou, O.E.; Saner, F.H.; Jahn, M.; Lange, C.M.; Willuweit, K. Humoral Response to SARS-Cov-2 Vaccination in Liver Transplant Recipients–A Single-Center Experience. Vaccines 2021, 9, 738. https://doi.org/10.3390/vaccines9070738
Rashidi-Alavijeh J, Frey A, Passenberg M, Korth J, Zmudzinski J, Anastasiou OE, Saner FH, Jahn M, Lange CM, Willuweit K. Humoral Response to SARS-Cov-2 Vaccination in Liver Transplant Recipients–A Single-Center Experience. Vaccines. 2021; 9(7):738. https://doi.org/10.3390/vaccines9070738
Chicago/Turabian StyleRashidi-Alavijeh, Jassin, Alexandra Frey, Moritz Passenberg, Johannes Korth, Jaqueline Zmudzinski, Olympia E. Anastasiou, Fuat H. Saner, Michael Jahn, Christian M. Lange, and Katharina Willuweit. 2021. "Humoral Response to SARS-Cov-2 Vaccination in Liver Transplant Recipients–A Single-Center Experience" Vaccines 9, no. 7: 738. https://doi.org/10.3390/vaccines9070738