
A National Survey to Assess the COVID-19 Vaccine-Related Conspiracy Beliefs, Acceptability, Preference, and Willingness to Pay among the General Population of Pakistan

 , , , , , , , and
, , , , , , , and  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Sampling, and Study Participants
2.2. Ethical Considerations
2.3. Survey Tool
2.4. Data Collection
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Recommendations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Situation Report. WHO: Geneva, Switzerland, 2020; p. 172. Available online: https://apps.who.int/iris/bitstream/handle/10665/333297/nCoVsitrep10Jul2020-eng.pdf (accessed on 21 February 2021).
- Tuite, A.R.; Bogoch, I.I.; Sherbo, R.; Watts, A.; Fisman, D.; Khan, K. Estimation of Coronavirus Disease 2019 (COVID-19) Burden and Potential for International Dissemination of Infection From Iran. Ann. Intern. Med. 2020, 172, 699–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, I.F.; Becker, A.D.; Grenfell, B.T.; Metcalf, C.J.E. Disease and healthcare burden of COVID-19 in the United States. Nat. Med. 2020, 26, 1212–1217. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Situation Reports. Available online: https://covid19.who.int/table (accessed on 23 June 2021).
- Chakraborty, I.; Maity, P. COVID-19 outbreak: Migration, effects on society, global environment and prevention. Sci. Total Environ. 2020, 728, 138882. [Google Scholar] [CrossRef] [PubMed]
- Gouglas, D.; Le, T.T.; Henderson, K.; Kaloudis, A.; Danielsen, T.; Hammersland, N.C.; Robinson, J.M.; Heaton, P.M.; Røttingen, J.-A. Estimating the cost of vaccine development against epidemic infectious diseases: A cost minimisation study. Lancet Glob. Heal. 2018, 6, e1386–e1396. [Google Scholar] [CrossRef] [Green Version]
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing Covid-19 Vaccines at Pandemic Speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef]
- DeRoo, S.S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 Vaccination Program. JAMA 2020, 323, 2458. [Google Scholar] [CrossRef]
- Maurer, J.; Harris, K.M.; Parker, A.; Lurie, N. Does receipt of seasonal influenza vaccine predict intention to receive novel H1N1 vaccine: Evidence from a nationally representative survey of U.S. adults. Vaccine 2009, 27, 5732–5734. [Google Scholar] [CrossRef] [Green Version]
- Eastwood, K.; Durrheim, D.N.; Jones, A.; Butler, M. Acceptance of pandemic (H1N1) 2009 influenza vaccination by the Australian public. Med. J. Aust. 2010, 192, 33–36. [Google Scholar] [CrossRef]
- Rubin, G.J.; Potts, H.W.W.; Michie, S. The impact of communications about swine flu (influenza A H1N1v) on public responses to the outbreak: Results from 36 national telephone surveys in the UK. Health Technol. Assess. 2010, 14, 183–266. [Google Scholar] [CrossRef] [Green Version]
- Raude, J.; Caille-Brillet, A.-L.; Setbon, M. The 2009 pandemic H1N1 influenza vaccination in France: Who accepted to receive the vaccine and why? PLoS Curr. 2010, 2, RRN1188. [Google Scholar] [CrossRef]
- Ahmed, A.; Lee, K.S.; Bukhsh, A.; Al-Worafi, Y.M.; Sarker, M.R.; Ming, L.C.; Khan, T.M. Outbreak of vaccine-preventable diseases in Muslim majority countries. J. Infect. Public Health 2018, 11, 153–155. [Google Scholar] [CrossRef]
- Khan, T.M.; Sahibzada, M.U.K. Challenges to health workers and their opinions about parents’ refusal of oral polio vaccination in the Khyber Pakhtoon Khawa (KPK) province, Pakistan. Vaccine 2016, 34, 2074–2081. [Google Scholar] [CrossRef]
- Akbar, R. Ten Threats to Global Health in 2019; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int/newsroom/spotlight/ten-threats-to-global-health-in-2019 (accessed on 22 February 2021).
- Peretti-Watel, P.; Seror, V.; Cortaredona, S.; Launay, O.; Raude, J.; Verger, P.; Fressard, L.; Beck, F.; Legleye, S.; L’Haridon, O.; et al. A future vaccination campaign against COVID-19 at risk of vaccine hesitancy and politicisation. Lancet Infect. Dis. 2020, 20, 769–770. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2021, 9, 16. [Google Scholar] [CrossRef]
- Koslap-Petraco, M. Vaccine hesitancy: Not a new phenomenon, but a new threat. J. Am. Assoc. Nurse Pr. 2019, 31, 624–626. [Google Scholar] [CrossRef]
- Andrade, G.E.; Hussain, A. Polio in Pakistan: Political, Sociological, and Epidemiological Factors. Cureus 2018, 10, 10. [Google Scholar] [CrossRef] [Green Version]
- Khattak, F.A.; Rehman, K.; Shahzad, M.; Arif, N.; Ullah, N.; Kibria, Z.; Arshad, M.; Afaq, S.; Ibrahimzai, A.K.; Haq, Z.U. Prevalence of Parental refusal rate and its associated factors in routine immunization by using WHO Vaccine Hesitancy tool: A Cross sectional study at district Bannu, KP, Pakistan. Int. J. Infect. Dis. 2021, 104, 117–124. [Google Scholar] [CrossRef]
- Khan, M.A.; Kanwal, N. Is unending polio because of religious militancy in Pakistan? A case of federally administrated tribal areas. Int. J. Dev. Confl. 2015, 5, 32–47. [Google Scholar]
- Khan, S.; Khan, M.; Maqsood, K.; Hussain, T.; Zeeshan, M. Is Pakistan prepared for the COVID-19 epidemic? A questionnaire-based survey. J. Med. Virol. 2020, 92, 824–832. [Google Scholar] [CrossRef] [Green Version]
- Afzal, M.S.; Khan, A.; Qureshi, U.U.R.; Saleem, S.; Saqib, M.A.; Shabbir, R.M.K.; Naveed, M.; Jabbar, M.; Zahoor, S.; Ahmed, H. Community-Based Assessment of Knowledge, Attitude, Practices and Risk Factors Regarding COVID-19 Among Pakistanis Residents During a Recent Outbreak: A Cross-Sectional Survey. J. Community Health 2021, 46, 476–486. [Google Scholar] [CrossRef]
- Uscinski, J.E.; Enders, A.M.; Klofstad, C.; Seelig, M.; Funchion, J.; Everett, C.; Wuchty, S.; Premaratne, K.; Murthi, M. Why do people believe COVID-19 conspiracy theories? Harv. Kennedy Sch. Misinformation Rev. 2020, 1, 1. [Google Scholar] [CrossRef]
- Romer, D.; Jamieson, K.H. Conspiracy theories as barriers to controlling the spread of COVID-19 in the U.S. Soc. Sci. Med. 2020, 263, 113356. [Google Scholar] [CrossRef]
- Enders, A.M.; Uscinski, J.E.; Klofstad, C.; Stoler, J. The different forms of COVID-19 misinformation and their consequences. Harv. Kennedy Sch. Misinform. Rev. 2020, 8, 1–21. [Google Scholar] [CrossRef]
- Chou, W.-Y.S.; Budenz, A. Considering Emotion in COVID-19 Vaccine Communication: Addressing Vaccine Hesitancy and Fostering Vaccine Confidence. Health Commun. 2020, 35, 1718–1722. [Google Scholar] [CrossRef] [PubMed]
- Abbas, Q.; Mangrio, F.; Kumar, S. Myths, beliefs, and conspiracies about COVID-19 Vaccines in Sindh, Pakistan: An online cross-sectional survey. Authorea Prepr. 2021. [Google Scholar] [CrossRef]
- Suarez-Lledo, V.; Alvarez-Galvez, J. Prevalence of Health Misinformation on Social Media: Systematic Review. J. Med. Internet Res. 2021, 23, 17187. [Google Scholar] [CrossRef] [PubMed]
- Cameron, M.P.; Newman, P.A.; Roungprakhon, S.; Scarpa, R. The marginal willingness-to-pay for attributes of a hypothetical HIV vaccine. Vaccine 2013, 31, 3712–3717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, K.; Francis, M.; Zhang, R.; Wang, Q.; Xia, A.; Lu, L.; Yang, B.; Hou, Z. Confidence, Acceptance and Willingness to Pay for the COVID-19 Vaccine among Migrants in Shanghai, China: A Cross-Sectional Study. Vaccines 2021, 9, 443. [Google Scholar] [CrossRef]
- Worldbank. Data for Lower middle income, Pakistan. Available online: https://data.worldbank.org/?locations=XN-PK (accessed on 23 June 2021).
- Rubinstein, H.; Marcu, A.; Yardley, L.; Michie, S. Public preferences for vaccination and antiviral medicines under different pandemic flu outbreak scenarios. BMC Public Heal. 2015, 15, 190. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]
- Khan, Y.H.; Mallhi, T.H.; Alotaibi, N.H.; AlZarea, A.I.; Alanazi, A.S.; Tanveer, N.; Hashmi, F.K. Threat of COVID-19 Vaccine Hesitancy in Pakistan: The Need for Measures to Neutralize Misleading Narratives. Am. J. Trop. Med. Hyg. 2020, 103, 603–604. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef]
- Healthline. How Much Will It Cost to Get a COVID-19 Vaccine? Available online: https://www.healthline.com/health-news/how-much-will-it-cost-to-get-a-covid-19-vaccine (accessed on 22 February 2021).
- UK ER. US Dollar (USD) to Pakistani Rupee (PKR) Exchange Rate History. Available online: https://www.exchangerates.org.uk/USD-PKR-exchange-rate-history.html (accessed on 22 February 2020).
- DRAP. Approval of COVID-19 Vaccine. Available online: https://www.dra.gov.pk/Home/covid (accessed on 23 June 2021).
- Lu, J.; Lu, G.; Tan, S.; Xia, J.; Xiong, H.; Yu, X.; Qi, Q.; Yu, X.; Li, L.; Yu, H. A COVID-19 mRNA vaccine encoding SARS-CoV-2 virus-like particles induces a strong antiviral-like immune response in mice. Cell Res. 2020, 30, 936–939. [Google Scholar] [CrossRef]
- Eysenbach, G. Correction: Improving the Quality of Web Surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2012, 14, 8. [Google Scholar] [CrossRef]
- PBS. Population Census. Available online: https://www.pbs.gov.pk/content/final-results-census-2017 (accessed on 24 June 2021).
- Garon, J.R.; Orenstein, W.A. Overcoming barriers to polio eradication in conflict areas. Lancet Infect. Dis. 2015, 15, 1122–1124. [Google Scholar] [CrossRef]
- Hussain, S.F.; Boyle, P.; Patel, P.; Sullivan, R. Eradicating polio in Pakistan: An analysis of the challenges and solutions to this security and health issue. Glob. Health 2016, 12, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ali, M.; Ahmad, N.; Khan, H.; Ali, S.; Akbar, F.; Hussain, Z. Polio vaccination controversy in Pakistan. Lancet 2019, 394, 915–916. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Bravo, M.; Stegmann, A. In Vaccines We Trust? The Effects of the CIA’s Vaccine Ruse on Immunization in Pakistan. J. Eur. Econ. Assoc. 2021, jvab018. [Google Scholar] [CrossRef]
- Costill, D.; Orenstein, W.A. Health workers identify motivators for OPV refusal in Pakistan. Infect. Diss Child. 2016, 29, 1. [Google Scholar]
- Freeman, D.; Waite, F.; Rosebrock, L.; Petit, A.; Causier, C.; East, A.; Jenner, L.; Teale, A.-L.; Carr, L.; Mulhall, S.; et al. Coronavirus conspiracy beliefs, mistrust, and compliance with government guidelines in England. Psychol. Med. 2020, 2020. [Google Scholar] [CrossRef]
- Khan, T.M.; Chiau, L.M. Polio vaccination in Pakistan: By force or by volition? Lancet 2015, 386, 1733. [Google Scholar] [CrossRef]
- Shahsavari, S.; Holur, P.; Wang, T.; Tangherlini, T.R.; Roychowdhury, V. Conspiracy in the time of corona: Automatic detection of emerging COVID-19 conspiracy theories in social media and the news. J. Comput. Soc. Sci. 2020, 3, 279–317. [Google Scholar] [CrossRef]
- Islam, S.; Sarkar, T.; Khan, S.H.; Kamal, A.-H.M.; Hasan, S.M.M.; Kabir, A.; Yeasmin, D.; Islam, M.A.; Chowdhury, K.I.A.; Anwar, K.S.; et al. COVID-19–Related Infodemic and Its Impact on Public Health: A Global Social Media Analysis. Am. J. Trop. Med. Hyg. 2020, 103, 1621–1629. [Google Scholar] [CrossRef]
- Broniatowski, D.A.; Kerchner, D.; Farooq, F.; Huang, X.; Jamison, A.M.; Dredze, M.; Quinn, S.C. The covid-19 social media infodemic reflects uncertainty and state-sponsored propaganda. arXiv 2020, arXiv:2007.09682. [Google Scholar]
- Jamison, A.M.; Broniatowski, D.A.; Dredze, M.; Sangraula, A.; Smith, M.C.; Quinn, S.C. Not just conspiracy theories: Vaccine opponents and proponents add to the COVID-19 ‘infodemic’on Twitter. Harv. Kennedy Sch. Misinform. Rev. 2020, 1. [Google Scholar] [CrossRef]
- Jennings, W.; Stoker, G.; Willis, H.; Valgardsson, V.; Gaskell, J.; Devine, D.; Mckay, L.; Mills, M.C. Lack of trust and social media echo chambers predict COVID-19 vaccine hesitancy. medRxiv 2021. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Bakri, F.G.; Mahafzah, A. Conspiracy Beliefs are Associated with Lower Knowledge and Higher Anxiety Levels Regarding COVID-19 among Students at the University of Jordan. Int. J. Environ. Res. Public Health 2020, 17, 4915. [Google Scholar]
- Pogue, K.; Jensen, J.L.; Stancil, C.K.; Ferguson, D.G.; Hughes, S.J.; Mello, E.J.; Burgess, R.; Berges, B.K.; Quaye, A.; Poole, B.D. Influences on Attitudes Regarding Potential COVID-19 Vaccination in the United States. Vaccines 2020, 8, 582. [Google Scholar] [CrossRef] [PubMed]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes toward a potential SARS-CoV-2 vaccine: A survey of US adults. Ann. Intern. Med 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 27, 225–228. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Groenewoud, R.; Rachor, G.S.; Asmundson, G.J. A proactive approach for managing COVID-19: The importance of understanding the motivational roots of vaccination hesitancy for SARS-CoV2. Front. Psychol. 2020, 11, 2890. [Google Scholar] [CrossRef]
- Graffigna, G.; Palamenghi, L.; Boccia, S.; Barello, S. Relationship between Citizens’ Health Engagement and Intention to Take the COVID-19 Vaccine in Italy: A Mediation Analysis. Vaccines 2020, 8, 576. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Salik, A.N.; Rafique, N. Impact of COVID-19 on Economy of Pakistan. Inst. Strateg. Stud. 2020, 31, 1–3. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Frequency or Mean | Percentage or ± SD | |
|---|---|---|---|
| Gender | Male | 1192 | 55.2% |
| Female | 966 | 44.8% | |
| Age (years) | 23.87 | 6.23 | |
| Age groups | 18–30 years | 1984 | 91.9% |
| 31–50 Years | 150 | 7.0% | |
| >50 years | 24 | 1.1% | |
| Marital status | Unmarried | 1764 | 81.7% |
| Married | 384 | 17.8% | |
| Divorced | 10 | 0.5% | |
| Education level | Primary | 12 | 0.6% |
| Secondary | 14 | 0.6% | |
| Intermediate | 206 | 9.5% | |
| Bachelor | 1322 | 61.3% | |
| Master or above | 604 | 28.0% | |
| Occupation | Student | 1550 | 71.8% |
| Govt. Employee | 134 | 6.2% | |
| Non-Govt. Employee | 196 | 9.1% | |
| Businessman | 60 | 2.8% | |
| Unemployment | 132 | 6.1% | |
| Housewife | 86 | 4.0% | |
| Profession | Not related to health | 1144 | 53.0% |
| Health related | 1014 | 47.0% | |
| Monthly income (PKR) | <20,000 | 156 | 7.2% |
| 20,000 to 40,000 | 178 | 8.2% | |
| 40,001 to 60,000 | 102 | 4.7% | |
| >60,000 | 172 | 8.0% | |
| No income | 1550 | 71.8% | |
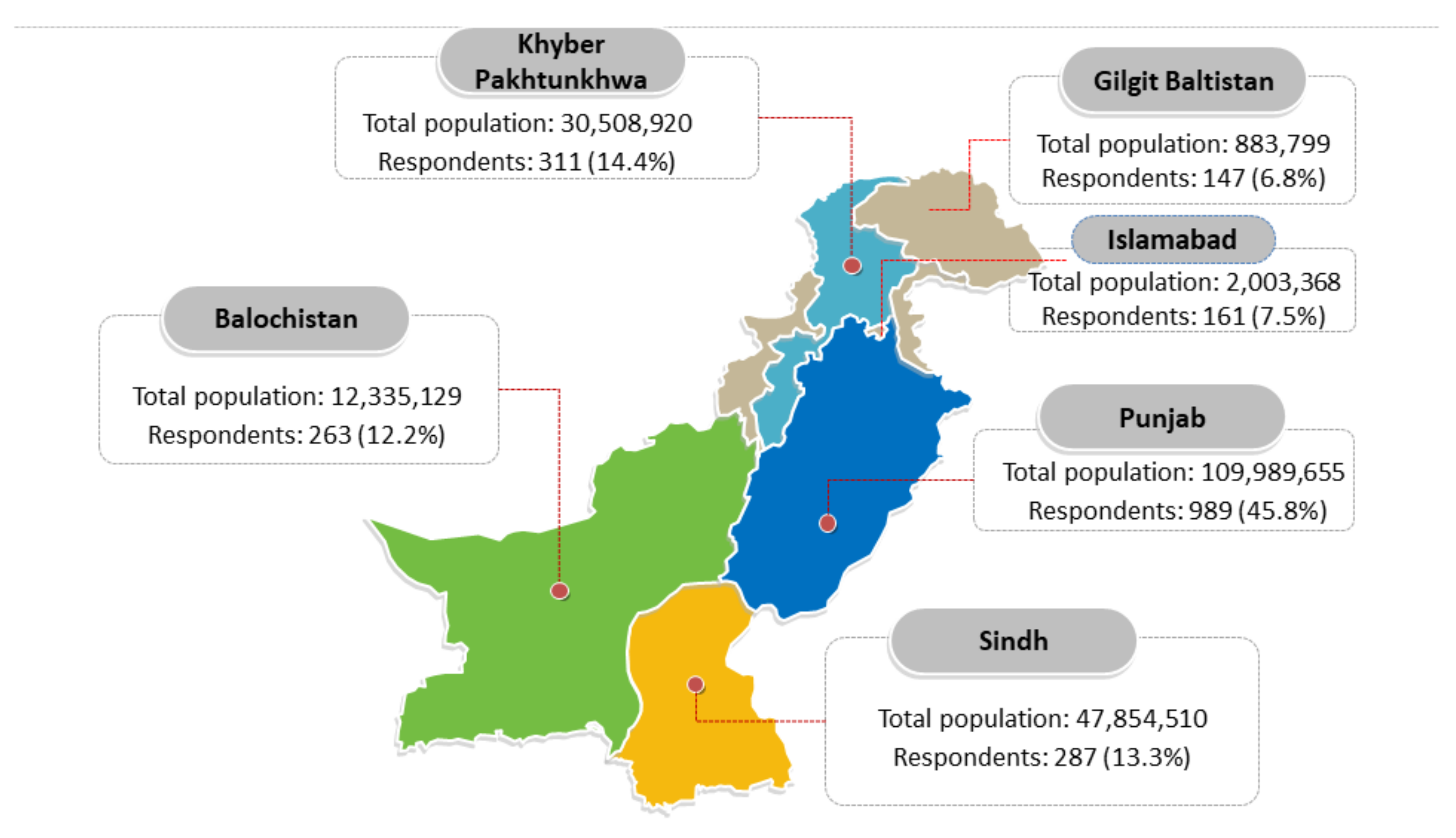
| Province | Punjab | 989 | 45.8% |
| Sindh | 287 | 13.3% | |
| KPK | 311 | 14.4% | |
| Baluchistan | 263 | 12.2% | |
| Gilgit-Baltistan | 147 | 6.8% | |
| Capital Islamabad | 161 | 7.5% | |
| Residence | Rural | 580 | 26.9% |
| Urban | 1578 | 73.1% | |
| Myths or Conspiracy Theories | No n (%) | Maybe n (%) | Yes n (%) | |
|---|---|---|---|---|
| M 1 | Do you believe that the COVID-19 vaccine has safety issues, which can kill people? | 732 (33.9%) | 1016 (47.1%) | 410 (19.0%) |
| M 2 | Do you believe that the COVID-19 vaccine contains any 5G Nano-chips to control people? | 1232 (57.1%) | 726 (33.6%) | 200 (9.3%) |
| M 3 | Do you believe that the COVID-19 vaccine could take away reproducibility (or cause infertility)? | 1110 (51.4%) | 790 (36.6%) | 258 (12.0%) |
| M 4 | Do you believe that COVID-19 and its vaccine are created to control the world population? | 1154 (53.5%) | 606 (28.1%) | 398 (18.4%) |
| M 5 | Do you believe that COVID-19 and its vaccine is designed to harm the Muslim nations? | 1424 (66.0%) | 452 (20.9%) | 282 (13.1%) |
| M 6 | Do you believe that the COVID-19 vaccine can harm people’s health as this has been developed in a very short period? | 636 (29.5%) | 910 (42.2%) | 612 (28.4%) |
| M 7 | Do you believe COVID-19 and its vaccine are non-Muslims’ propaganda to rule the world? | 1232 (57.1%) | 572 (26.5%) | 354 (16.4%) |
| Frequency | Percentage | ||
|---|---|---|---|
| Vaccine Acceptance | No | 556 | 25.8% |
| Maybe | 562 | 26.0% | |
| Yes | 1040 | 48.2% | |
| Willingness to pay | <500 PKR (3.12 USD) | 1138 | 52.7% |
| 500 to 1001 PKR (3.12 to 6.25 USD) | 654 | 30.3% | |
| 1001 to 2000 PKR (6.26 to 12.50 USD) | 146 | 6.8% | |
| 2001 to 3000 PKR (12.51 to 18.75 USD) | 76 | 3.5% | |
| >3000 PKR (18.75 USD) | 144 | 6.7% | |
| Preference | American Vaccine (Pfizer-biotech vaccine) | 630 | 29.2% |
| European vaccine (Oxford-AstraZeneca vaccine) | 594 | 27.5% | |
| Chinese vaccine (Sino pharm) | 934 | 43.3% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arshad, M.S.; Hussain, I.; Mahmood, T.; Hayat, K.; Majeed, A.; Imran, I.; Saeed, H.; Iqbal, M.O.; Uzair, M.; Rehman, A.u.; et al. A National Survey to Assess the COVID-19 Vaccine-Related Conspiracy Beliefs, Acceptability, Preference, and Willingness to Pay among the General Population of Pakistan. Vaccines 2021, 9, 720. https://doi.org/10.3390/vaccines9070720
Arshad MS, Hussain I, Mahmood T, Hayat K, Majeed A, Imran I, Saeed H, Iqbal MO, Uzair M, Rehman Au, et al. A National Survey to Assess the COVID-19 Vaccine-Related Conspiracy Beliefs, Acceptability, Preference, and Willingness to Pay among the General Population of Pakistan. Vaccines. 2021; 9(7):720. https://doi.org/10.3390/vaccines9070720
Chicago/Turabian StyleArshad, Muhammad Subhan, Iltaf Hussain, Tahir Mahmood, Khezar Hayat, Abdul Majeed, Imran Imran, Hamid Saeed, Muhammad Omer Iqbal, Muhammad Uzair, Anees ur Rehman, and et al. 2021. "A National Survey to Assess the COVID-19 Vaccine-Related Conspiracy Beliefs, Acceptability, Preference, and Willingness to Pay among the General Population of Pakistan" Vaccines 9, no. 7: 720. https://doi.org/10.3390/vaccines9070720