
Healthcare Providers’ Vaccine Perceptions, Hesitancy, and Recommendation to Patients: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
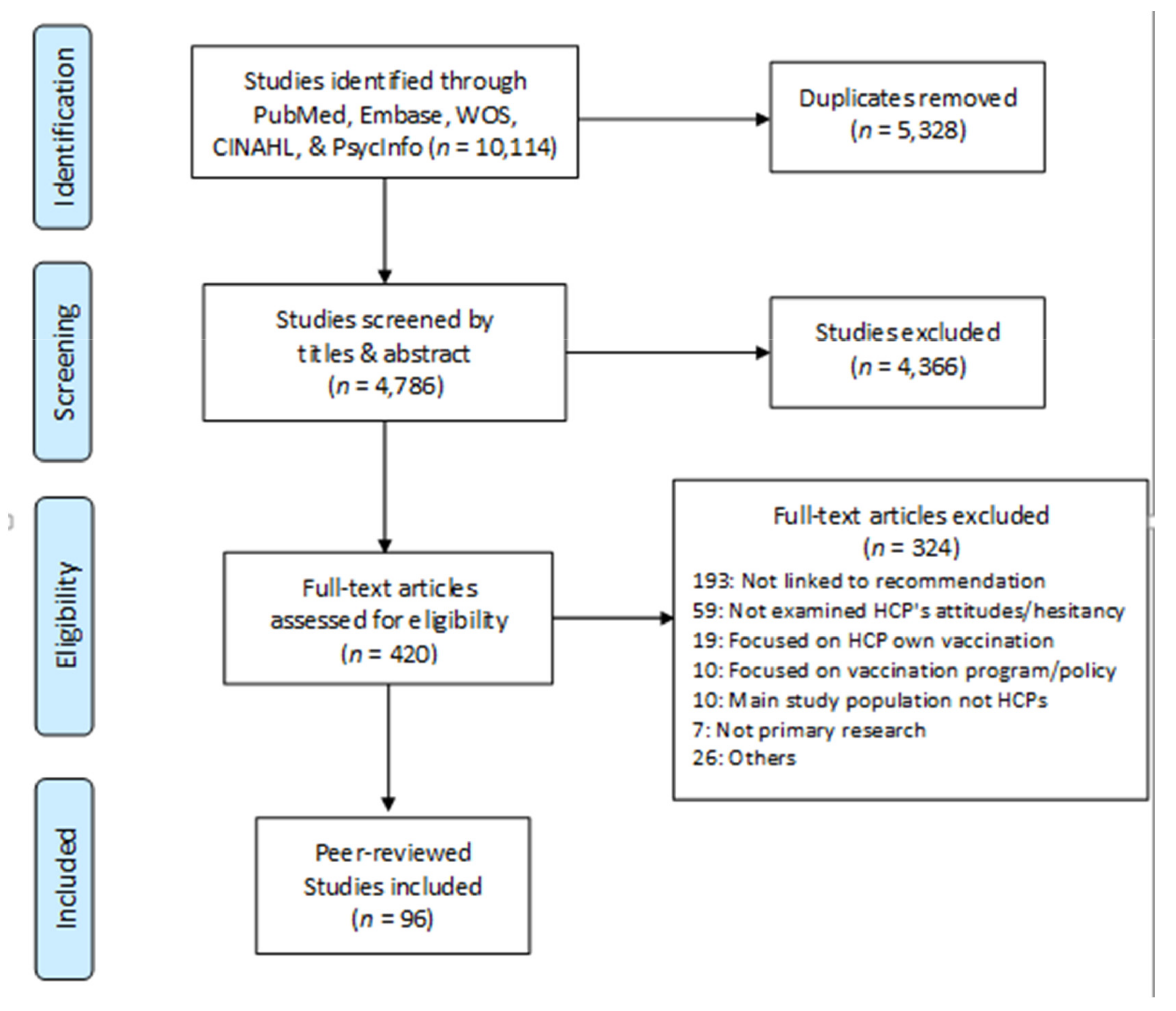
3.1. Search Results and Study Characteristics
3.2. HCP Attitudes, Perceptions, and Knowledge
3.2.1. Vaccine and Disease Attributes
3.2.2. HCP Characteristics
3.2.3. HCP Knowledge
3.2.4. Provider Uptake
3.3. Patient and Contextual Factors
3.3.1. Patient Characteristics
3.3.2. System Factors
3.3.3. HPV-Specific Behavior
4. Discussion
5. Conclusions and Future Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stern, A.M.; Markel, H. The History Of Vaccines And Immunization: Familiar Patterns, New Challenges. Health Aff. 2005, 24, 611–621. [Google Scholar] [CrossRef]
- Deogaonkar, R.; Hutubessy, R.; van der Putten, I.; Evers, S.; Jit, M. Systematic Review of Studies Evaluating the Broader Economic Impact of Vaccination in Low and Middle Income Countries. BMC Public Health 2012, 12, 878. [Google Scholar] [CrossRef] [Green Version]
- Andre, F.E.; Booy, R.; Bock, H.L.; Clemens, J.; Datta, S.K.; John, T.J.; Lee, B.W.; Lolekha, S.; Peltola, H.; Ruff, T.A.; et al. Vaccination Greatly Reduces Disease, Disability, Death and Inequity Worldwide. Bull. World Health Organ. 2008, 86, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Doherty, M.; Buchy, P.; Standaert, B.; Giaquinto, C.; Prado-Cohrs, D. Vaccine Impact: Benefits for Human Health. Vaccine 2016, 34, 6707–6714. [Google Scholar] [CrossRef] [PubMed]
- Karafillakis, E.; Larson, H.J. The Benefit of the Doubt or Doubts over Benefits? A Systematic Literature Review of Perceived Risks of Vaccines in European Populations. Vaccine 2017, 35, 4840–4850. [Google Scholar] [CrossRef]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J.; SAGE Working Group on Vaccine Hesitancy. Strategies for Addressing Vaccine Hesitancy-A Systematic Review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [Green Version]
- National Center for Health Statistics NHIS Early Release of Selected Estimates Based on Data from the 2018 National Health Interview Survey. Available online: https://www.cdc.gov/nchs/nhis/releases/released201905.htm (accessed on 20 September 2020).
- National Center for Health Statistics FastStats-Influenza Vaccination. Available online: https://www.cdc.gov/nchs/fastats/flu.htm (accessed on 20 September 2020).
- Wilder-Smith, A.B.; Qureshi, K. Resurgence of Measles in Europe: A Systematic Review on Parental Attitudes and Beliefs of Measles Vaccine. J. Epidemiol. Glob. Health 2020, 10, 46–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabacchi, G.; Costantino, C.; Napoli, G.; Marchese, V.; Cracchiolo, M.; Casuccio, A.; Vitale, F.; The Esculapio Working Group. Determinants of European Parents’ Decision on the Vaccination of Their Children against Measles, Mumps and Rubella: A Systematic Review and Meta-Analysis. Hum. Vaccines Immunother. 2016, 12, 1909–1923. [Google Scholar] [CrossRef] [Green Version]
- Lo, N.C.; Hotez, P.J. Public Health and Economic Consequences of Vaccine Hesitancy for Measles in the United States. JAMA Pediatr. 2017, 171, 887–892. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- WHO Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 25 September 2020).
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine: A Survey of U.S. Adults. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef]
- Jennings, W.; Stoker, G.; Bunting, H.; Valgarðsson, V.O.; Gaskell, J.; Devine, D.; McKay, L.; Mills, M.C. Lack of Trust, Conspiracy Beliefs, and Social Media Use Predict COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 593. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Albertin, C.S.; Gurfinkel, D.; Saville, A.W.; Vangala, S.; Rice, J.D.; Helmkamp, L.; Zimet, G.D.; Valderrama, R.; Breck, A.; et al. Prevalence and Characteristics of HPV Vaccine Hesitancy among Parents of Adolescents across the US. Vaccine 2020, 38, 6027–6037. [Google Scholar] [CrossRef]
- Kreidl, P.; Breitwieser, M.-M.; Würzner, R.; Borena, W. 14-Year-Old Schoolchildren Can Consent to Get Vaccinated in Tyrol, Austria: What Do They Know about Diseases and Vaccinations? Vaccines 2020, 8, 610. [Google Scholar] [CrossRef]
- Lama, Y.; Hancock, G.R.; Freimuth, V.S.; Jamison, A.M.; Quinn, S.C. Using Classification and Regression Tree Analysis to Explore Parental Influenza Vaccine Decisions. Vaccine 2020, 38, 1032–1039. [Google Scholar] [CrossRef] [PubMed]
- Eilers, R.; Krabbe, P.F.M.; de Melker, H.E. Factors Affecting the Uptake of Vaccination by the Elderly in Western Society. Prev. Med. 2014, 69, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Gargano, L.M.; Herbert, N.L.; Painter, J.E.; Sales, J.M.; Morfaw, C.; Rask, K.; Murray, D.; DiClemente, R.; Hughes, J.M. Impact of a Physician Recommendation and Parental Immunization Attitudes on Receipt or Intention to Receive Adolescent Vaccines. Hum. Vaccines Immunother. 2013, 9, 2627–2633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brewer, N.T.; Fazekas, K.I. Predictors of HPV Vaccine Acceptability: A Theory-Informed, Systematic Review. Prev. Med. 2007, 45, 107–114. [Google Scholar] [CrossRef]
- Smith, P.J.; Kennedy, A.M.; Wooten, K.; Gust, D.A.; Pickering, L.K. Association between Health Care Providers’ Influence on Parents Who Have Concerns about Vaccine Safety and Vaccination Coverage. Pediatrics 2006, 118, e1287–e1292. [Google Scholar] [CrossRef]
- Paterson, P.; Meurice, F.; Stanberry, L.R.; Glismann, S.; Rosenthal, S.L.; Larson, H.J. Vaccine Hesitancy and Healthcare Providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, B.L.; Shepard, A.; Kahn, J.A. US Health Care Clinicians’ Knowledge, Attitudes, and Practices Regarding Human Papillomavirus Vaccination: A Qualitative Systematic Review. Acad. Pediatr. 2018, 18, S53–S65. [Google Scholar] [CrossRef] [Green Version]
- Hofmann, F.; Ferracin, C.; Marsh, G.; Dumas, R. Influenza Vaccination of Healthcare Workers: A Literature Review of Attitudes and Beliefs. Infection 2006, 34, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Leung, S.O.A.; Akinwunmi, B.; Elias, K.M.; Feldman, S. Educating Healthcare Providers to Increase Human Papillomavirus (HPV) Vaccination Rates: A Qualitative Systematic Review. Vaccine X 2019, 3, 100037. [Google Scholar] [CrossRef]
- Vasilevska, M.; Ku, J.; Fisman, D.N. Factors Associated with Healthcare Worker Acceptance of Vaccination: A Systematic Review and Meta-Analysis. Infect. Control Hosp. Epidemiol. 2014, 35, 699–708. [Google Scholar] [CrossRef]
- Covidence Systematic Review Software; Veritas Health Innovation: Melbourne, Australia, 2021.
- Gauthier, B.; Circum Network Inc. Assessing Survey Research—A Principled Approach. Available online: https://circum.com/index.cgi?en:appr (accessed on 28 December 2020).
- Best Evidence Topics (BestBETs). Survey Checklinst__Critical Appraisal. Available online: https://bestbets.org/ca/pdf/survey.pdf (accessed on 28 October 2020).
- Best Evidence Topics (BestBETs). Qualitative Checklist-Critical Appraisal. Available online: https://bestbets.org/ca/pdf/qualitative.pdf (accessed on 28 October 2020).
- Joanna Briggs Institute (JBI). Checklist for Qualitative Research. Available online: https://joannabriggs.org/sites/default/files/2020-08/Checklist_for_Qualitative_Research.pdf (accessed on 28 October 2020).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Perkins, R.B.; Clark, J.A. What Affects Human Papillomavirus Vaccination Rates? A Qualitative Analysis of Providers’ Perceptions. Womens Health Issues 2012, 22, e379–e386. [Google Scholar] [CrossRef]
- Bean, S.J.; Catania, J.A. Vaccine Perceptions among Oregon Health Care Providers. Qual. Health Res. 2013, 23, 1251–1266. [Google Scholar] [CrossRef] [PubMed]
- Lutringer-Magnin, D.; Kalecinski, J.; Barone, G.; Leocmach, Y.; Regnier, V.; Jacquard, A.C.; Soubeyrand, B.; Vanhems, P.; Chauvin, F.; Lasset, C. Human Papillomavirus (HPV) Vaccination: Perception and Practice among French General Practitioners in the Year since Licensing. Vaccine 2011, 29, 5322–5328. [Google Scholar] [CrossRef]
- MacDougall, D.; Halperin, B.A.; MacKinnon-Cameron, D.; Li, L.; McNeil, S.A.; Langley, J.M.; Halperin, S.A. Universal Tetanus, Diphtheria, Acellular Pertussis (Tdap) Vaccination of Adults: What Canadian Health Care Providers Know and Need to Know. Hum. Vaccines Immunother. 2015, 11, 2167–2179. [Google Scholar] [CrossRef] [Green Version]
- Dubé, E.; Fannie, D.; Vladimir, G.; Julie, B.A.; Chantal, S.; France, L.; François, B.D.; Shelly, M.; Ian, G.; Nicole, B. A(H1N1) Pandemic Influenza and Its Prevention by Vaccination: Paediatricians’ Opinions before and after the Beginning of the Vaccination Campaign. BMC Public Health 2011, 11, 128. [Google Scholar] [CrossRef] [Green Version]
- Dubé, E.; Gilca, V.; Sauvageau, C.; Bradet, R.; Bettinger, J.A.; Boulianne, N.; Boucher, F.D.; McNeil, S.; Gemmill, I.; Lavoie, F. Canadian Paediatricians’ Opinions on Rotavirus Vaccination. Vaccine 2011, 29, 3177–3182. [Google Scholar] [CrossRef]
- Duval, B.; Gilca, V.; Boulianne, N.; Pielak, K.; Halperin, B.; Simpson, M.A.; Sauvageau, C.; Ouakki, M.; Dube, E.; Lavoie, F. Cervical Cancer Prevention by Vaccination: Nurses’ Knowledge, Attitudes and Intentions. J. Adv. Nurs. 2009, 65, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Kempe, A.; Daley, M.F.; Parashar, U.D.; Crane, L.A.; Beaty, B.L.; Stokley, S.; Barrow, J.; Babbel, C.; Dickinson, L.M.; Widdowson, M.-A.; et al. Will Pediatricians Adopt the New Rotavirus Vaccine? Pediatrics 2007, 119, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Massin, S.; Ventelou, B.; Nebout, A.; Verger, P.; Pulcini, C. Cross-Sectional Survey: Risk-Averse French General Practitioners Are More Favorable toward Influenza Vaccination. Vaccine 2015, 33, 610–614. [Google Scholar] [CrossRef] [PubMed]
- Vezzosi, L.; Riccò, M.; Agozzino, E.; Odone, A.; Signorelli, C. Knowledge, Attitudes, and Practices of General Practitioners from the Province of Parma (Northern Italy) towards Vaccinations in Adults ≥65 Year-Old. Acta Biol. Medica Atenei Parm. 2019, 90, 71–75. [Google Scholar] [CrossRef]
- Young, J.L.; Bernheim, R.G.; Korte, J.E.; Stoler, M.H.; Guterbock, T.M.; Rice, L.W. Human Papillomavirus Vaccination Recommendation May Be Linked to Reimbursement: A Survey of Virginia Family Practitioners and Gynecologists. J. Pediatr. Adolesc. Gynecol. 2011, 24, 380–385. [Google Scholar] [CrossRef]
- Zimmerman, R.K. A National Survey to Understand Why Physicians Defer Childhood Immunizations. Arch. Pediatr. Adolesc. Med. 1997, 151, 657. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, R. Understanding Physician Agreement with Varicella Immunization Guidelines. Prev. Med. 2002, 35, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, R.K.; Schlesselman, J.J.; Mieczkowski, T.A.; Medsger, A.R.; Raymund, M. Physician Concerns About Vaccine Adverse Effects and Potential Litigation. Arch. Pediatr. Adolesc. Med. 1998, 152. [Google Scholar] [CrossRef] [PubMed]
- Kahn, J.A.; Zimet, G.D.; Bernstein, D.I.; Riedesel, J.M.; Lan, D.; Huang, B.; Rosenthal, S.L. Pediatricians’ Intention to Administer Human Papillomavirus Vaccine: The Role of Practice Characteristics, Knowledge, and Attitudes. J. Adolesc. Health 2005, 37, 502–510. [Google Scholar] [CrossRef]
- Riedesel, J.M.; Rosenthal, S.L.; Zimet, G.D.; Bernstein, D.I.; Huang, B.; Lan, D.; Kahn, J.A. Attitudes about Human Papillomavirus Vaccine among Family Physicians. J. Pediatr. Adolesc. Gynecol. 2005, 18, 391–398. [Google Scholar] [CrossRef]
- Kassianos, G.; Kuchar, E.; Nitsch-Osuch, A.; Kyncl, J.; Galev, A.; Humolli, I.; Falup-Pecurariu, O.; Thomson, A.; Klein, C.; Vallée-Tourangeau, G. Motors of Influenza Vaccination Uptake and Vaccination Advocacy in Healthcare Workers: A Comparative Study in Six European Countries. Vaccine 2018, 36, 6546–6552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vadaparampil, S.T.; Malo, T.L.; Sutton, S.K.; Ali, K.N.; Kahn, J.A.; Casler, A.; Salmon, D.; Walkosz, B.; Roetzheim, R.G.; Zimet, G.D.; et al. Missing the Target for Routine Human Papillomavirus Vaccination: Consistent and Strong Physician Recommendations Are Lacking for 11- to 12-Year-Old Males. Cancer Epidemiol. Biomark. Prev. 2016, 25, 1435–1446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klett-Tammen, C.J.; Krause, G.; von Lengerke, T.; Castell, S. Advising Vaccinations for the Elderly: A Cross-Sectional Survey on Differences between General Practitioners and Physician Assistants in Germany. BMC Fam. Pract. 2016, 17, 98. [Google Scholar] [CrossRef] [Green Version]
- Collange, F.; Fressard, L.; Pulcini, C.; Sebbah, R.; Peretti-Watel, P.; Verger, P. General Practitioners’ Attitudes and Behaviors toward HPV Vaccination: A French National Survey. Vaccine 2016, 34, 762–768. [Google Scholar] [CrossRef]
- Dubé, E.; Gagnon, D.; Kaminsky, K.; Green, C.R.; Ouakki, M.; Bettinger, J.A.; Brousseau, N.; Castillo, E.; Crowcroft, N.S.; Driedger, S.M.; et al. Vaccination Against Influenza in Pregnancy: A Survey of Canadian Maternity Care Providers. J. Obstet. Gynaecol. Can. JOGC 2019, 41, 479–488. [Google Scholar] [CrossRef]
- Torun, S.D.; Torun, F. Vaccination against Pandemic Influenza A/H1N1 among Healthcare Workers and Reasons for Refusing Vaccination in Istanbul in Last Pandemic Alert Phase. Vaccine 2010, 28, 5703–5710. [Google Scholar] [CrossRef]
- Gilca, V.; Boulianne, N.; Dubé, E.; Sauvageau, C.; Ouakki, M. Attitudes of Nurses toward Current and Proposed Vaccines for Public Programs: A Questionnaire Survey. Int. J. Nurs. Stud. 2009, 46, 1219–1235. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, L.C.; Lewandowsky, S.; Antfolk, J.; Salo, P.; Lindfelt, M.; Oksanen, T.; Kivimäki, M.; Soveri, A. The Association between Vaccination Confidence, Vaccination Behavior, and Willingness to Recommend Vaccines among Finnish Healthcare Workers. PLoS ONE 2019, 14, e0224330. [Google Scholar] [CrossRef]
- Agrinier, N.; Le Maréchal, M.; Fressard, L.; Verger, P.; Pulcini, C. Discrepancies between General Practitioners’ Vaccination Recommendations for Their Patients and Practices for Their Children. Clin. Microbiol. Infect. 2017, 23, 311–317. [Google Scholar] [CrossRef] [Green Version]
- Davis, M.M.; Ndiaye, S.M.; Freed, G.L.; Clark, S.J. One-Year Uptake of Pneumococcal Conjugate Vaccine: A National Survey of Family Physicians and Pediatricians. J. Am. Board Fam. Med. 2003, 16, 363–371. [Google Scholar] [CrossRef] [Green Version]
- Farias, A.J.; Savas, L.S.; Fernandez, M.E.; Coan, S.P.; Shegog, R.; Healy, C.M.; Lipizzi, E.; Vernon, S.W. Association of Physicians Perceived Barriers with Human Papillomavirus Vaccination Initiation. Prev. Med. 2017, 105, 219–225. [Google Scholar] [CrossRef]
- Raude, J.; Fressard, L.; Gautier, A.; Pulcini, C.; Peretti-Watel, P.; Verger, P. Opening the ‘Vaccine Hesitancy’ Black Box: How Trust in Institutions Affects French GPs’ Vaccination Practices. Expert Rev. Vaccines 2016, 15, 937–948. [Google Scholar] [CrossRef] [Green Version]
- Böhm, S.; Röbl-Mathieu, M.; Scheele, B.; Wojcinski, M.; Wichmann, O.; Hellenbrand, W. Influenza and Pertussis Vaccination during Pregnancy–Attitudes, Practices and Barriers in Gynaecological Practices in Germany. BMC Health Serv. Res. 2019, 19, 616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verger, P.; Fressard, L.; Collange, F.; Gautier, A.; Jestin, C.; Launay, O.; Raude, J.; Pulcini, C.; Peretti-Watel, P. Vaccine Hesitancy Among General Practitioners and Its Determinants During Controversies: A National Cross-Sectional Survey in France. EBioMedicine 2015, 2, 891–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, L.; Chen, J.; Fang, T.; Cui, J.; Li, H.; Ma, R.; Sun, Y.; Li, P.; Dong, H.; Xu, G. Determinants of Healthcare Workers’ Willingness to Recommend the Seasonal Influenza Vaccine to Diabetic Patients: A Cross-Sectional Survey in Ningbo, China. Hum. Vaccines Immunother. 2018, 14, 2979–2986. [Google Scholar] [CrossRef]
- Bynum, S.A.; Staras, S.A.S.; Malo, T.L.; Giuliano, A.R.; Shenkman, E.; Vadaparampil, S.T. Factors Associated With Medicaid Providers’ Recommendation of the HPV Vaccine to Low-Income Adolescent Girls. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2014, 54, 190–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mui, L.W.H.; Chan, A.Y.S.; Lee, A.; Lee, J. Cross-Sectional Study on Attitudes among General Practitioners towards Pneumococcal Vaccination for Middle-Aged and Elderly Population in Hong Kong. PLoS ONE 2013, 8, e78210. [Google Scholar] [CrossRef] [Green Version]
- Praphasiri, P.; Ditsungneon, D.; Greenbaum, A.; Dawood, F.S.; Yoocharoen, P.; Stone, D.M.; Olsen, S.J.; Lindblade, K.A.; Muangchana, C. Do Thai Physicians Recommend Seasonal Influenza Vaccines to Pregnant Women? A Cross-Sectional Survey of Physicians’ Perspectives and Practices in Thailand. PLoS ONE 2017, 12, e0169221. [Google Scholar] [CrossRef] [PubMed]
- Suryadevara, M.; Handel, A.; Bonville, C.A.; Cibula, D.A.; Domachowske, J.B. Pediatric Provider Vaccine Hesitancy: An under-Recognized Obstacle to Immunizing Children. Vaccine 2015, 33, 6629–6634. [Google Scholar] [CrossRef]
- Taylor, K.A.; Stocks, N.; Marshall, H.S. The Missing Link: Family Physician Perspectives on Barriers and Enablers to Prescribing a New Meningococcal B Vaccine and Other Recommended, Non-Government Funded Vaccines. Vaccine 2014, 32, 4214–4219. [Google Scholar] [CrossRef]
- Tuckerman, J.; Crawford, N.W.; Marshall, H.S. Seasonal Influenza Vaccination for Children with Special Risk Medical Conditions: Does Policy Meet Practice? J. Paediatr. Child Health 2020, 56, 1388–1395. [Google Scholar] [CrossRef]
- Napolitano, F.; Navaro, M.; Vezzosi, L.; Santagati, G.; Angelillo, I.F. Primary Care Pediatricians’ Attitudes and Practice towards HPV Vaccination: A Nationwide Survey in Italy. PLoS ONE 2018, 13, e0194920. [Google Scholar] [CrossRef]
- Esteves-Jaramillo, A.; Omer, S.B.; Gonzalez-Diaz, E.; Salmon, D.A.; Hixson, B.; Navarro, F.; Kawa-Karasik, S.; Frew, P.; Morfin-Otero, R.; Rodriguez-Noriega, E.; et al. Acceptance of a Vaccine against Novel Influenza A (H1N1) Virus among Health Care Workers in Two Major Cities in Mexico. Arch. Med. Res. 2009, 40, 705–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubé, E.; Gilca, V.; Sauvageau, C.; Bradet, R.; Lavoie, F.; Boulianne, N.; Boucher, F.D.; Bettinger, J.A.; McNeil, S.; Gemmill, I. Acute Otitis Media and Its Prevention by Immunization: A Survey of Canadian Pediatricians’ Knowledge, Attitudes and Beliefs. Hum. Vaccines 2011, 7, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, B.A.; Eilers, R.; Mollema, L.; Ferreira, J.; de Melker, H.E. The Intention of Dutch General Practitioners to Offer Vaccination against Pneumococcal Disease, Herpes Zoster and Pertussis to People Aged 60 Years and Older. BMC Geriatr. 2017, 17, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allison, M.A.; Dunne, E.F.; Markowitz, L.E.; O’Leary, S.T.; Crane, L.A.; Hurley, L.P.; Stokley, S.; Babbel, C.I.; Brtnikova, M.; Beaty, B.L.; et al. HPV Vaccination of Boys in Primary Care Practices. Acad. Pediatr. 2013, 13, 466–474. [Google Scholar] [CrossRef] [Green Version]
- Feemster, K.A.; Winters, S.E.; Fiks, A.G.; Kinsman, S.; Kahn, J.A. Pediatricians’ Intention to Recommend Human Papillomavirus (HPV) Vaccines to 11- to 12-Year-Old Girls Postlicensing. J. Adolesc. Health 2008, 43, 408–411. [Google Scholar] [CrossRef]
- Nikolic, Z.; Matejic, B.; Kesic, V.; Eric Marinkovic, J.; Jovic Vranes, A. Factors Influencing the Recommendation of the Human Papillomavirus Vaccine by Serbian Pediatricians. J. Pediatr. Adolesc. Gynecol. 2015, 28, 12–18. [Google Scholar] [CrossRef]
- Le Maréchal, M.; Agrinier, N.; Fressard, L.; Verger, P.; Pulcini, C. Low Uptake of Meningococcal C Vaccination in France: A Cross-Sectional Nationwide Survey of General Practitioners’ Perceptions, Attitudes and Practices. Pediatr. Infect. Dis. J. 2017, 36, e181. [Google Scholar] [CrossRef]
- Yang, T.U.; Cheong, H.J.; Choi, W.S.; Song, J.Y.; Noh, J.Y.; Kim, W.J. Physician Attitudes toward the Herpes Zoster Vaccination in South Korea. Infect. Chemother. 2014, 46, 194. [Google Scholar] [CrossRef] [Green Version]
- Esposito, S.; Bosis, S.; Pelucchi, C.; Begliatti, E.; Rognoni, A.; Bellasio, M.; Tel, F.; Consolo, S.; Principi, N. Pediatrician Knowledge and Attitudes Regarding Human Papillomavirus Disease and Its Prevention. Vaccine 2007, 25, 6437–6446. [Google Scholar] [CrossRef] [PubMed]
- Glavier, M.; Puyade, M.; Roblot, F.; Rammaert, B. Vaccination of Cancer Patients Treated with Chemotherapy: A Survey among General Practitioners. Med. Mal. Infect. 2019, 49, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Allison, M.A.; Hurley, L.P.; Markowitz, L.; Crane, L.A.; Brtnikova, M.; Beaty, B.L.; Snow, M.; Cory, J.; Stokley, S.; Roark, J.; et al. Primary Care Physicians’ Perspectives about HPV Vaccine. Pediatrics 2016, 137, e20152488. [Google Scholar] [CrossRef] [Green Version]
- Ehresmann, K.; Mills, W.; Moore, K. Attitudes and Practices Regarding Varicella Vaccination among Physicians in Minnesota: Implications for Public Health and Provider Education. Am. J. Public Health 2000, 90, 1917–1920. [Google Scholar] [CrossRef] [Green Version]
- Hurley, L.P.; Harpaz, R.; Daley, M.F.; Crane, L.A.; Beaty, B.L.; Barrow, J.; Babbel, C.; Marin, M.; Steiner, J.F.; Davidson, A.; et al. National Survey of Primary Care Physicians Regarding Herpes Zoster and the Herpes Zoster Vaccine. J. Infect. Dis. 2008, 197, S216–S223. [Google Scholar] [CrossRef] [Green Version]
- Wilcox, C.R.; Calvert, A.; Metz, J.; Kilich, E.; MacLeod, R.; Beadon, K.; Heath, P.T.; Khalil, A.; Finn, A.; Snape, M.D.; et al. Attitudes of Pregnant Women and Healthcare Professionals Toward Clinical Trials and Routine Implementation of Antenatal Vaccination against Respiratory Syncytial Virus: A Multicenter Questionnaire Study. Pediatr. Infect. Dis. J. 2019, 38, 944–951. [Google Scholar] [CrossRef]
- Newman, R.D.; Taylor, J.A. Reactions of Pediatricians to the Recommendation for Universal Varicella Vaccination. Arch. Pediatr. Adolesc. Med. 1998, 152. [Google Scholar] [CrossRef]
- Gesser-Edelsburg, A.; Shir-Raz, Y.; Hayek, S.; Aassaraf, S.; Lowenstein, L. Despite Awareness of Recommendations, Why Do Health Care Workers Not Immunize Pregnant Women? Am. J. Infect. Control 2017, 45, 436–439. [Google Scholar] [CrossRef] [PubMed]
- Flicoteaux, R.; Pulcini, C.; Carrieri, P.; Schwarzinger, M.; Leport, C.; Verger, P. Correlates of General Practitioners’ Recommendations to Patients Regarding Vaccination for the 2009–2010 Pandemic Influenza (A/H1N1) in France: Implications for Future Vaccination Campaigns. Vaccine 2014, 32, 2281–2287. [Google Scholar] [CrossRef] [PubMed]
- Bruno, D.M.; Wilson, T.E.; Gany, F.; Aragones, A. Identifying Human Papillomavirus Vaccination Practices among Primary Care Providers of Minority, Low-Income and Immigrant Patient Populations. Vaccine 2014, 32, 4149–4154. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; While, A.E.; Norman, I.J. Nurses’ Vaccination against Pandemic H1N1 Influenza and Their Knowledge and Other Factors. Vaccine 2012, 30, 4813–4819. [Google Scholar] [CrossRef]
- Dubé, E.; Gilca, V.; Sauvageau, C.; Boulianne, N.; Boucher, F.D.; Bettinger, J.A.; McNeil, S.; Gemmill, I.; Lavoie, F.; Ouakki, M. Canadian Family Physicians’ and Paediatricians’ Knowledge, Attitudes and Practices Regarding A(H1N1) Pandemic Vaccine. BMC Res. Notes 2010, 5, 102. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, P.; Stromillo, L.; Albano, L. Awareness, Attitudes, and Practices Toward Meningococcal B Vaccine among Pediatricians in Italy. Med. Kaunas Lith. 2018, 54, 100. [Google Scholar] [CrossRef] [Green Version]
- Bovier, P.A.; Bouvier Gallacdhi, M.; Chamot, E. Swiss Primary Care Physicians Reporting of Utility and Use of Recommended Vaccinations for Adults. Swiss Med. Wkly. 2005, 135, 192–199. [Google Scholar] [PubMed]
- Hobeika, E.; Usta, I.M.; Helou, R.; Jabak, S.; El Kak, F.; Nassar, A.H. Practice and Attitudes towards Immunization among Lebanese Obstetricians and Gynecologists. Hum. Vaccines Immunother. 2018, 14, 1501–1508. [Google Scholar] [CrossRef] [PubMed]
- Pelullo, C.P.; Della Polla, G.; Napolitano, F.; Di Giuseppe, G.; Angelillo, I.F. Healthcare Workers’ Knowledge, Attitudes, and Practices about Vaccinations: A Cross-Sectional Study in Italy. Vaccines 2020, 8, 148. [Google Scholar] [CrossRef] [Green Version]
- Almughais, E.S.; Alfarhan, A.; Salam, M. Awareness of Primary Health Care Physicians about Human Papilloma Virus Infection and Its Vaccination: A Cross-Sectional Survey from Multiple Clinics in Saudi Arabia. Infect. Drug Resist. 2018, 11, 2257–2267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Power, M.L.; Leddy, M.A.; Anderson, B.L.; Gall, S.A.; Gonik, B.; Schulkin, J. Obstetrician–Gynecologists’ Practices and Perceived Knowledge Regarding Immunization. Am. J. Prev. Med. 2009, 37, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Daley, M.F.; Liddon, N.; Crane, L.A.; Beaty, B.L.; Barrow, J.; Babbel, C.; Markowitz, L.E.; Dunne, E.F.; Stokley, S.; Dickinson, L.M.; et al. A National Survey of Pediatrician Knowledge and Attitudes Regarding Human Papillomavirus Vaccination. Pediatrics 2006, 118, 2280–2289. [Google Scholar] [CrossRef]
- Wong, L.P.; Edib, Z.; Alias, H.; Mohamad Shakir, S.M.; Raja Muhammad Yusoff, R.N.A.; Sam, I.-C.; Zimet, G.D. A Study of Physicians’ Experiences with Recommending HPV Vaccines to Adolescent Boys. J. Obstet. Gynaecol. 2017, 37, 937–943. [Google Scholar] [CrossRef]
- Abi Jaoude, J.; Khair, D.; Dagher, H.; Saad, H.; Cherfan, P.; Kaafarani, M.A.; Jamaluddine, Z.; Ghattas, H. Factors Associated with Human Papilloma Virus (HPV) Vaccine Recommendation by Physicians in Lebanon, a Cross-Sectional Study. Vaccine 2018, 36, 7562–7567. [Google Scholar] [CrossRef]
- Collange, F.; Verger, P.; Launay, O.; Pulcini, C. Knowledge, Attitudes, Beliefs and Behaviors of General Practitioners/Family Physicians toward Their Own Vaccination: A Systematic Review. Hum. Vaccines Immunother. 2016, 12, 1282–1292. [Google Scholar] [CrossRef] [PubMed]
- Hofstetter, A.M.; Lappetito, L.; Stockwell, M.S.; Rosenthal, S.L. Human Papillomavirus Vaccination of Adolescents with Chronic Medical Conditions: A National Survey of Pediatric Subspecialists. J. Pediatr. Adolesc. Gynecol. 2017, 30, 88–95. [Google Scholar] [CrossRef] [Green Version]
- Kempe, A.; Allison, M.A.; MacNeil, J.R.; O’Leary, S.T.; Crane, L.A.; Beaty, B.L.; Hurley, L.P.; Brtnikova, M.; Lindley, M.C.; Albert, A.P. Adoption of Serogroup B Meningococcal Vaccine Recommendations. Pediatrics 2018, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Maréchal, M.; Fressard, L.; Raude, J.; Verger, P.; Pulcini, C. General Practitioners and Vaccination of Children Presenting with a Benign Infection. Med. Mal. Infect. 2018, 48, 44–52. [Google Scholar] [CrossRef] [Green Version]
- Neufeind, J.; Betsch, C.; Habersaat, K.B.; Eckardt, M.; Schmid, P.; Wichmann, O. Barriers and Drivers to Adult Vaccination among Family Physicians–Insights for Tailoring the Immunization Program in Germany. Vaccine 2020, 38, 4252–4262. [Google Scholar] [CrossRef] [PubMed]
- Shibli, R.; Rishpon, S.; Cohen-Dar, M.; Kandlik, Y. What Affects Pediatric Healthcare Providers to Encourage Receipt of Routine Childhood Vaccinations? Results from the Northern District of Israel, 2016. Vaccine 2019, 37, 524–529. [Google Scholar] [CrossRef]
- Stefanoff, P.; Sobierajski, T.; Bulinska-Stangrecka, H.; Augustynowicz, E. Exploring Factors Improving Support for Vaccinations among Polish Primary Care Physicians. PLoS ONE 2020, 15, e0232722. [Google Scholar] [CrossRef]
- Vadaparampil, S.T.; Staras, S.A.S.; Malo, T.L.; Eddleton, K.Z.; Christie, J.; Rodriguez, M.; Giuliano, A.R.; Shenkman, E.A. Provider Factors Associated with Disparities in Human Papillomavirus Vaccination among Low-Income 9- to 17-Year-Old Girls. Cancer 2013, 119, 621–628. [Google Scholar] [CrossRef]
- Verger, P.; Collange, F.; Fressard, L.; Bocquier, A.; Gautier, A.; Pulcini, C.; Raude, J.; Peretti-Watel, P. Prevalence and Correlates of Vaccine Hesitancy among General Practitioners: A Cross-Sectional Telephone Survey in France, April to July 2014. Eurosurveillance 2016, 21. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Biringer, A.; Ofner-Agostini, M.; Upshur, R.; McGeer, A. A Cross-Sectional Study of Maternity Care Providers’ and Women’s Knowledge, Attitudes, and Behaviours Towards Influenza Vaccination during Pregnancy. J. Obstet. Gynaecol. Can. 2008, 30, 404–410. [Google Scholar] [CrossRef]
- Inoue, Y.; Matsui, K. Physicians’ Recommendations to Their Patients Concerning a Novel Pandemic Vaccine: A Cross-Sectional Survey of the 2009 Influenza A/H1N1 Pandemic in Japan. Environ. Health Prev. Med. 2011, 16, 320–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shibli, R.; Shemer, R.; Lerner-Geva, L.; Rishpon, S. Knowledge and Recommendation Regarding Routine Childhood Vaccinations among Pediatric Healthcare Providers in Israel. Vaccine 2017, 35, 633–638. [Google Scholar] [CrossRef]
- Krishnaswamy, S.; Wallace, E.M.; Buttery, J.; Giles, M.L. A Study Comparing the Practice of Australian Maternity Care Providers in Relation to Maternal Immunisation. Aust. N. Z. J. Obstet. Gynaecol. 2019, 59, 408–415. [Google Scholar] [CrossRef]
- Wilcox, C.R.; Little, P.; Jones, C.E. Current Practice and Attitudes towards Vaccination during Pregnancy: A Survey of GPs across England. Br. J. Gen. Pract. 2020, 70, e179–e185. [Google Scholar] [CrossRef]
- Fagnan, L.J.; Shipman, S.A.; Gaudino, J.A.; Mahler, J.; Sussman, A.L.; Holub, J. To Give or Not to Give: Approaches to Early Childhood Immunization Delivery in Oregon Rural Primary Care Practices: Rural Oregon Immunization Initiative. J. Rural Health 2011, 27, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Dombkowski, K.J.; Leung, S.W.; Clark, S.J. Physician Perspectives Regarding Annual Influenza Vaccination among Children with Asthma. Ambul. Pediatr. 2008, 8, 294–299. [Google Scholar] [CrossRef]
- Barnack, J.L.; Reddy, D.M.; Swain, C. Predictors of Parents’ Willingness to Vaccinate for Human Papillomavirus and Physicians’ Intentions to Recommend the Vaccine. Womens Health Issues 2010, 20, 28–34. [Google Scholar] [CrossRef]
- Arnell, T.L.; York, C.; Nadeau, A.; Donnelly, M.L.; Till, L.; Zargari, P.; Davis, W.; Finley, C.; Delaney, T.; Carney, J. The Role of the Dental Community in Oropharyngeal Cancer Prevention Through HPV Vaccine Advocacy. J. Cancer Educ. 2019. [Google Scholar] [CrossRef]
- Hoque, M.E. Factors Influencing the Recommendation of the Human Papillomavirus Vaccine by South African Doctors Working in a Tertiary Hospital. Afr. Health Sci. 2016, 16, 567–575. [Google Scholar] [CrossRef]
- Noh, J.Y.; Seo, Y.B.; Song, J.Y.; Choi, W.S.; Lee, J.; Jung, E.; Kang, S.; Choi, M.J.; Jun, J.; Yoon, J.G.; et al. Perception and Attitudes of Korean Obstetricians about Maternal Influenza Vaccination. J. Korean Med. Sci. 2016, 31, 1063. [Google Scholar] [CrossRef] [Green Version]
- Kao, C.-C.; Huang, S.-Y.; Cheng, P.-J.; Shaw, S.-W.; Chueh, H.-Y.; Chang, S.-D.; Hsu, T.-Y.; Kung, F.-T.; Hsieh, T.-T. Factors Associated with the Intention to Recommend Pertussis Vaccination for Postpartum Women: A Survey in Taiwan of Obstetrician–Gynecologists’ Knowledge, Beliefs, and Attitudes-ClinicalKey. Available online: https://www-clinicalkey-com.proxy.lib.duke.edu/#!/content/playContent/1-s2.0-S1028455912000666?returnurl=https:%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS1028455912000666%3Fshowall%3Dtrue&referrer= (accessed on 22 February 2021).
- Rutten, L.J.F.; St Sauver, J.L.; Beebe, T.J.; Wilson, P.M.; Jacobson, D.J.; Fan, C.; Breitkopf, C.R.; Vadaparampil, S.T.; Jacobson, R.M. Clinician Knowledge, Clinician Barriers, and Perceived Parental Barriers Regarding Human Papillomavirus Vaccination: Association with Initiation and Completion Rates. Vaccine 2017, 35, 164–169. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, T.G.; Wood, N.J.; West, R.M.; Darling, J.C. UK Health Professionals’ Attitudes and Knowledge Regarding Human Papillomavirus (HPV) Vaccination: A West Yorkshire Study. J. Paediatr. Child Health 2009, 45, 652–655. [Google Scholar] [CrossRef]
- Pavia, M.; Rita Foresta, M.; Carbone, V.; Angelillo, I.F. Influenza and Pneumococcal Immunization in the Elderly: Knowledge, Attitudes, and Practices among General Practitioners in Italy. Public Health 2003, 117, 202–207. [Google Scholar] [CrossRef]
- Betsch, C.; Wicker, S. Personal Attitudes and Misconceptions, Not Official Recommendations Guide Occupational Physicians’ Vaccination Decisions. Vaccine 2014, 32, 4478–4484. [Google Scholar] [CrossRef]
- Soon, R.; Dela Cruz, M.R.I.; Tsark, J.U.; Chen, J.J.; Braun, K.L. A Survey of Physicians’ Attitudes and Practices about the Human Papillomavirus (HPV) Vaccine in Hawai‘i. Hawaii J. Med. Public Health 2015, 74, 234–241. [Google Scholar]
- Vilca, L.M.; Martínez, C.; Burballa, M.; Campins, M. Maternal Care Providers’ Barriers Regarding Influenza and Pertussis Vaccination during Pregnancy in Catalonia, Spain. Matern. Child Health J. 2018, 22, 1016–1024. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, E.; Kennedy, A.; Soud, F.; Burns, A. Physicians Who Do and Do Not Recommend Children Get All Vaccinations. J. Health Commun. 2008, 13, 573–582. [Google Scholar] [CrossRef]
- Topuridze, M.; Butsashvili, M.; Kamkamidze, G.; Kajaia, M.; Morse, D.; McNutt, L.A. Barriers to Hepatitis B Vaccine Coverage among Healthcare Workers in the Republic of Georgia: An International Perspective. Infect. Control Hosp. Epidemiol. 2010, 31, 158–164. [Google Scholar] [CrossRef]
- Wagner, A.; Kundi, M.; Zwiauer, K.; Wiedermann, U. Paediatricians Require More Information before They Routinely Co-Administer the Meningococcal B Vaccine with Routine Infant Vaccines. Acta Paediatr. 2015, 104, e439–e447. [Google Scholar] [CrossRef]
- Canon, C.; Effoe, V.; Shetty, V.; Shetty, A.K. Knowledge and Attitudes Towards Human Papillomavirus (HPV) Among Academic and Community Physicians in Mangalore, India. J. Cancer Educ. 2017, 32, 382–391. [Google Scholar] [CrossRef]
- Wilson, R.; Scronias, D.; Zaytseva, A.; Ferry, M.-A.; Chamboredon, P.; Dubé, E.; Verger, P. Seasonal Influenza Self-Vaccination Behaviours and Attitudes among Nurses in Southeastern France. Hum. Vaccines Immunother. 2019, 15, 2423–2433. [Google Scholar] [CrossRef] [PubMed]
- Çiftci, F.; Şen, E.; Demir, N.; Çiftci, O.; Erol, S.; Kayacan, O. Beliefs, Attitudes, and Activities of Healthcare Personnel about Influenza and Pneumococcal Vaccines. Hum. Vaccines Immunother. 2018, 14, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding Vaccine Hesitancy around Vaccines and Vaccination from a Global Perspective: A Systematic Review of Published Literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are Healthcare Workers’ Intentions to Vaccinate Related to Their Knowledge, Beliefs and Attitudes? A Systematic Review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef] [Green Version]
- Schmittdiel, J.; Grumbach, K.; Selby, J.V.; Quesenberry, C.P. Effect of Physician and Patient Gender Concordance on Patient Satisfaction and Preventive Care Practices. J. Gen. Intern. Med. 2000, 15, 761–769. [Google Scholar] [CrossRef] [Green Version]
- Takeshita, J.; Wang, S.; Loren, A.W.; Mitra, N.; Shults, J.; Shin, D.B.; Sawinski, D.L. Association of Racial/Ethnic and Gender Concordance between Patients and Physicians with Patient Experience Ratings. JAMA Netw. Open 2020, 3, e2024583. [Google Scholar] [CrossRef] [PubMed]
- Meghani, S.H.; Brooks, J.M.; Gipson-Jones, T.; Waite, R.; Whitfield-Harris, L.; Deatrick, J.A. Patient–Provider Race-Concordance: Does It Matter in Improving Minority Patients’ Health Outcomes? Ethn. Health 2009, 14, 107–130. [Google Scholar] [CrossRef]
- Killian, M.; Detoc, M.; Berthelot, P.; Charles, R.; Gagneux-Brunon, A.; Lucht, F.; Pulcini, C.; Barbois, S.; Botelho-Nevers, E. Vaccine Hesitancy among General Practitioners: Evaluation and Comparison of Their Immunisation Practice for Themselves, Their Patients and Their Children. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1837–1843. [Google Scholar] [CrossRef] [PubMed]
- Nutman, A.; Yoeli, N. Influenza Vaccination Motivators among Healthcare Personnel in a Large Acute Care Hospital in Israel. Isr. J. Health Policy Res. 2016, 5, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levi, M.; Bonanni, P.; Biffino, M.; Conversano, M.; Corongiu, M.; Morato, P.; Maio, T. Influenza Vaccination 2014–2015: Results of a Survey Conducted among General Practitioners in Italy. Hum. Vaccines Immunother. 2018, 14, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Ciardi, F.; Menon, V.; Jensen, J.L.; Shariff, M.A.; Pillai, A.; Venugopal, U.; Kasubhai, M.; Dimitrov, V.; Kanna, B.; Poole, B.D. Knowledge, Attitudes and Perceptions of COVID-19 Vaccination among Healthcare Workers of an Inner-City Hospital in New York. Vaccines 2021, 9, 516. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Gagnon, D.; MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Strategies Intended to Address Vaccine Hesitancy: Review of Published Reviews. Vaccine 2015, 33, 4191–4203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foss, H.S.; Oldervoll, A.; Fretheim, A.; Glenton, C.; Lewin, S. Communication around HPV Vaccination for Adolescents in Low- and Middle-Income Countries: A Systematic Scoping Overview of Systematic Reviews. Syst. Rev. 2019, 8. [Google Scholar] [CrossRef]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors Associated With US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open 2020, 3. [Google Scholar] [CrossRef]
- Miller, K.; COVID-19 Vaccine Booster Doses May Soon Be a Reality. Here’s What Experts Know So Far. Available online: https://www.prevention.com/health/a35644466/covid-19-vaccine-booster-shot/ (accessed on 17 April 2021).
- Grumbach, K.; Judson, T.; Desai, M.; Jain, V.; Lindan, C.; Doernberg, S.B.; Holubar, M. Association of Race/Ethnicity with Likeliness of COVID-19 Vaccine Uptake among Health Workers and the General Population in the San Francisco Bay Area. JAMA Intern. Med. 2021. [Google Scholar] [CrossRef]
- Konstantinou, P.; Georgiou, K.; Kumar, N.; Kyprianidou, M.; Nicolaides, C.; Karekla, M.; Kassianos, A.P. Transmission of Vaccination Attitudes and Uptake Based on Social Contagion Theory: A Scoping Review. Vaccines 2021, 9, 607. [Google Scholar] [CrossRef]


{kind=link}
| Relevant Factors | More Likely to Recommend * | Less Likely to Recommend † | Non-Significant ‡ |
|---|---|---|---|
| Vaccine and Disease Attributes | |||
| Weighting vaccine benefit vs. risk | perceived more benefit [35,50,52] | perceived more risk [53,54,55] | |
| Vaccine safety and side effect | believed safe [42,55,56,57,58,59], fewer side effect concerns [60] | with safety concern [42,52,55,61,62]; viewed safety a barrier [63]; believed vaccine could cause side effects [64,65] | safety [45,66,67,68,69,70,71], adverse events [48] |
| Vaccine efficacy | (likely to adopt) [60,65,68,72]; (intent to recommend) [45,56,61,63,66,68,69,73,74,75,76,77,78,79] | perceived low or unclear efficacy [45,61,63,69,77,80,81,82], waning immunity [83,84] | [69,70,71,85] |
| Disease severity and prevalence | [8,40,42,73,75,86]; believed vaccines reduce negative health outcomes [87] | perceived low severity [88,89] | [67] |
| Risk of infection | risk for patients [65,68,85,90,91,92,93]; believing they are at risk of getting/transmitting disease [73] | [65] | |
| Vaccine utility/ necessity or importance | [7,8,15,29,40,57,87,88,94] | doubt utility/necessity [54,64,85,95]; beliefs in natural immunity [84] | [96] |
| HCP Characteristics | |||
| Gender | female [50,60,97,98] | males more likely to be nonadopters [99] | [37,42,52,62,63,65,68,70,72,79,83,90,100,101,102,103,104,105,106,107,108,109,110] |
| Race and ethnicity | Indian doctors in Malaysia [100] | [52,66,86,109] | |
| Age and experience | older or more experienced [49,73,81,111] | older [65] | Age [42,63,72,90,97,100,101,104,105,106,108,109,112]; experience [54,63,87,113,114] |
| Number of years practicing | greater number [65,72,100,115]; recent graduates [46] | year of graduation [47]; time practicing [56,71,82,116] | |
| History treating the disease | [45,54,67,70,87,110,112] | ||
| Number of patients seen | greater number [49,117] | [72] | |
| Specialty | pediatricians [39,50,54,57,58,59,101,118], FP [66], hematology/oncology or rheumatology [103], PCP [98], doctor (vs. Nurse) [56,73], dentist (vs. Hygienist) [119], pediatric resident [81], Vaccines for Children doctors [52] | FP [88], obstetrician [111], physicians w/out a specialty [94] | [47,68,71,85,97,115,116] |
| Level of training | training on disease [65]; adopting new technology [45,77] | inadequate training [82]; insufficient info to counsel [81] | [69,70] |
| Information | adequate/reliable [38,42,55,70,96,120,121] | lack information [30,44,55,82,85,98] | needing more info [72]; felt poorly informed [78] |
| Believing vaccination was their responsibility | (recommending) [71,81], (discussing) [115] | ||
| Knowledge of vaccine and/or disease | [41,50,86,91,93,101,111,122,123]; confidence in vaccine study [42] | aware Guillain–Barre disease related to influenza vaccine [112] | [56,78,97,99,103,108,109,124] |
| Knowledge of guidelines | [65,68,86,93,105,114,125] | [126] | |
| Confidence in knowledge | [51,55,64,106,114,115] | confidence in general [127] | |
| Attitudes towards vaccines | positive attitudes [55,75,93,111,126]; perceive vaccine acceptance by others [39,57,74,92]; believing vaccines reduce parents losing work time [87] | ||
| Own uptake of a vaccine | [39,44,56,67,71,91,95,106,111,128] | not vaccinating own child [54,58,102] | [67,112,129] |
| Perceived norm or expectation | peer pressure [36,108]; having vaccinated colleagues [73,130] | ||
| Patient Characteristics | |||
| Demographics | age [66,75,104]; older [85]; seeing more Black patients [60] | low socioeconomic status [70]; seeing mostly non-Hispanic white [66] | age [101]; race [103] |
| Political Views | non-conservative [101] | ||
| Patient/parent behavior, views, or related factors | HCP not believing parents would reject [46], anticipating concerns [77], expecting compliance [120]; patients not understanding disease severity [59]; parents not believing in efficacy [78] | expressed refusal or concerns [32,40,42,73,74,82,107]; believing patients/parents lack adequate info [78], would not complete future screening [45]; HCP placing emphasis on parental request [84] | |
| Patient condition | older, with comorbidities [75]; children with asthma [117]; immunocompromised [60]; upper respiratory tract infection [46]; chronic medical conditions [103]; attending day care [60]; pregnant patients [55] | patient allergic to something in vaccine [94] | |
| System Factors | |||
| Recommendations and guidelines | having guidelines [50,84]; following guidelines [49,55,68,80,92,105,114] | lacking guidelines [63,95,100,131] | |
| Trust in authorities or information sources | trust [56,62,64] | lack of trust [53] | [58] |
| Sources of information | official sources [87]; | media [89]; internet, magazines, pharmaceutical companies [129] | [89,108,125] |
| Barriers to recommendation | lack of time [63,67,78,82,83,94] logistical difficulties [45,48,63,67,68,95,116] failure to discuss vaccine [117] | (not having) time to discuss [127] | |
| Place of practice | private [104,109]; larger [60,129]; solo practice [72]; preventative [107]; urban [76,100,116]; metro [71] | neighborhood or community health centers [87]; secondary/tertiary hospital [65]; practices where alternative medicine used [110] | location [42,63,82,83,100,103,104,105,131]; practice type [65,68,79,103,105,114,131]; private practice [128] |
| Cost | cost of disease [39,65,74,92,94]; free vaccine [132]; having privately purchased vaccines [117] | cost of vaccine [27,40,76]; patient ability to pay or financial burden [61,85]; high cost or non-funded [70] | vaccine cost [66,70,78,85,127]; reimbursed [42,66]; patient payment [132]; affordability [67]; too costly to store [87] |
| Patient insurance | seeing fewer uninsured patients [90]; more Medicaid patients [60] | number of Medicaid patients [104,117]; insurance status [103] | |
| HPV Specific | |||
| Patient demographics | older [50,76,83,99]; female [50,99,101] | infrequent visits [76,90] | |
| Factors regarding sexual health or sexuality | discussed sexuality & sexual health [76,81,103,124,127]; comfortable discussing [64]; discussion prior to sexual activity [81]; having more sexually active patients [49] | feeling uncomfortable discussing [50,66,99,103]; aware patient not sexually active [83]; believing discussion would increase sexual activity [66,69] | discussing sex [52]; believing discussion would increase sexual activity [78,132]; comfortable discussing sexuality & sexual health [99,129] |
| Believing HPV is a public safety issue | [97] | ||
| Resulting diseases | believing vaccine prevents cervical cancer and warts [81,95] | uncertain if HPV results in cancer [132] | |
| Patient and parental attitudes | to patient accompanied by mother to appointment [101] | believing they will be less receptive [90,99], refuse [83], not vaccinate their sons [76] | [77,78] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.; Mullen, J.; Smith, D.; Kotarba, M.; Kaplan, S.J.; Tu, P. Healthcare Providers’ Vaccine Perceptions, Hesitancy, and Recommendation to Patients: A Systematic Review. Vaccines 2021, 9, 713. https://doi.org/10.3390/vaccines9070713
Lin C, Mullen J, Smith D, Kotarba M, Kaplan SJ, Tu P. Healthcare Providers’ Vaccine Perceptions, Hesitancy, and Recommendation to Patients: A Systematic Review. Vaccines. 2021; 9(7):713. https://doi.org/10.3390/vaccines9070713
Chicago/Turabian StyleLin, Cheryl, Jewel Mullen, Danielle Smith, Michaela Kotarba, Samantha J. Kaplan, and Pikuei Tu. 2021. "Healthcare Providers’ Vaccine Perceptions, Hesitancy, and Recommendation to Patients: A Systematic Review" Vaccines 9, no. 7: 713. https://doi.org/10.3390/vaccines9070713