
Transmission of Vaccination Attitudes and Uptake Based on Social Contagion Theory: A Scoping Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
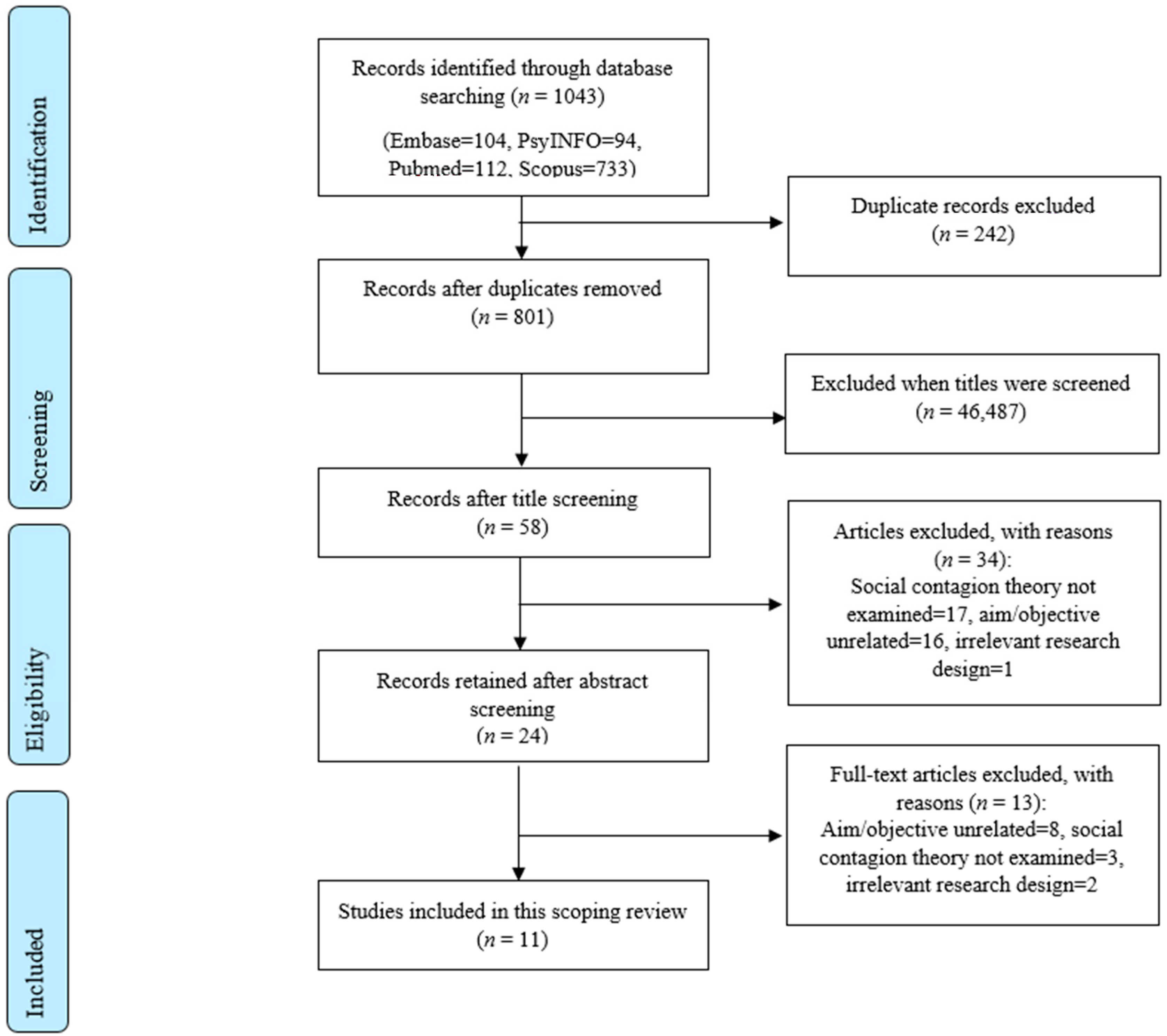
2.2. Search Strategy and Study Selection
2.3. Data Extraction and Synthesis
3. Results
3.1. Study Characteristics
3.2. Description of Methodology and Analytical Approach
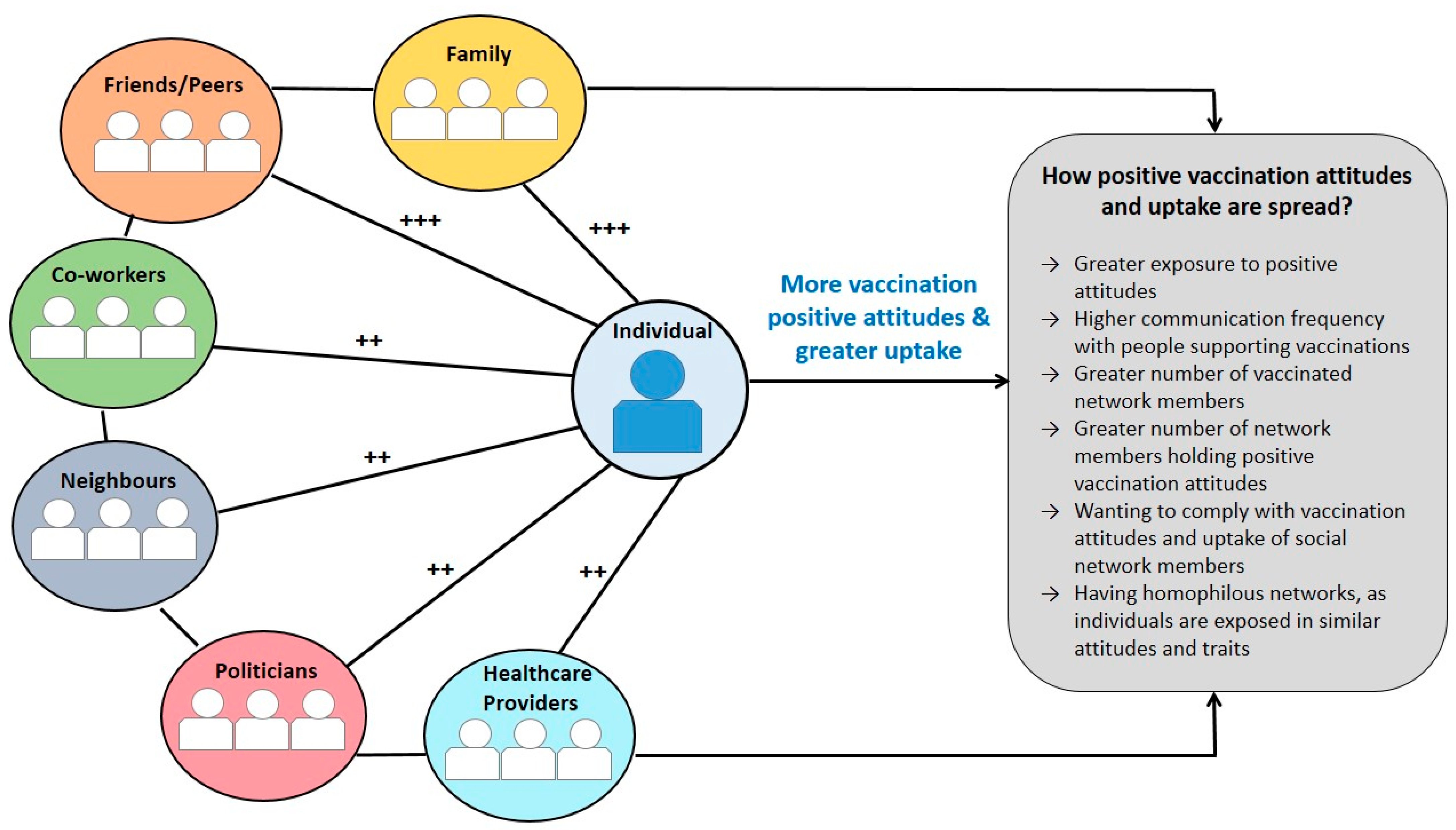
3.3. Transmission of Vaccination Attitudes and Uptake within Social Networks
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Glossary
| Centrality | The position of an individual in the centre of a social network |
| Clustering | Co-occurrence of a trait of interest in connected individuals in a social network |
| Egocentric network | An individual’s network is mapped based on information provided on his or her ties |
| Homophily | The tendency of people to relate with people who have similar characteristics |
| Social ties | The relationship between individuals such as family ties |
| Sociocentric network | A network of all members of a community or group is mapped with interactions between each provided |
| Spread | The mechanism underlying how attitudes and behaviours are transmitted from one person to another |
Appendix A
Search Strategy
- Pubmed
- PsycInfo
- Embase
- Scopus
Appendix B
Information Extracted by Each Study
- Characteristics of the study: publication year, country of the study, research design, and aim;
- Characteristics of the population: sample size, age, gender, education, population type, and vaccine type;
- Analytical approach: how the data were analysed such as social network analysis or multiple regression;
- Description of type of network: egocentric (i.e., a network mapped asking an individual to identify their social contacts) or sociocentric (i.e., a network mapped identifying all members of a specific network);
- Main findings:
- Centrality: the position of an individual in the centre of a network.
- Clustering: co-occurrence of a trait of interest in connected individuals in a network (e.g., vaccination acceptance in individuals working together in a company).
- Homophily: the tendency of individuals to relate with people who have similar attributes.
- Social ties: the relationship between individuals such as friendship, spouse and family ties.
- Spread: the mechanism underlying how vaccination attitudes and uptake are transmitted from one person to another.
- Other findings: description of social networks and other mechanisms underlying how vaccination attitudes and uptake are transmitted within networks.
References
- Christakis, N.A.; Fowler, J.H. Social network sensors for early detection of contagious outbreaks. PLoS ONE 2010, 5, e12948. [Google Scholar] [CrossRef] [Green Version]
- Christakis, N.A.; Fowler, J.H. Social contagion theory: Examining dynamic social networks and human behavior. Stat. Med. 2013, 32, 556–577. [Google Scholar] [CrossRef] [Green Version]
- Scherer, C.W.; Cho, H. A social network contagion theory of risk perception. Risk Anal. 2003, 23, 261–267. [Google Scholar] [CrossRef]
- Aral, S.; Nicolaides, C. Exercise contagion in a global social network. Nat. Commun. 2017, 8, 14753. [Google Scholar] [CrossRef] [Green Version]
- Pachucki, M.A.; Jacques, P.F.; Christakis, N.A. Social network concordance in food choice among spouses, friends, and siblings. Am. J. Public Health 2011, 101, 2170–2177. [Google Scholar] [CrossRef]
- Christakis, N.A.; Fowler, J.H. The Spread of Obesity in a Large Social Network over 32 Years. N. Engl. J. Med. 2007, 357, 370–379. [Google Scholar] [CrossRef] [Green Version]
- Smith, K.P.; Christakis, N.A. Social networks and health. Annu. Rev. Sociol. 2008, 34, 405–429. [Google Scholar] [CrossRef] [Green Version]
- Rosenquist, J.N.; Fowler, J.H.; Christakis, N.A. Social network determinants of depression. Mol. Psychiatry 2011, 16, 273–281. [Google Scholar] [CrossRef] [Green Version]
- Mednick, S.C.; Christakis, N.A.; Fowler, J.H. The spread of sleep loss influences drug use in adolescent social networks. PLoS ONE 2010, 5. [Google Scholar] [CrossRef]
- Mcpherson, M.; Lovin, L.S.; Cook, J.M. Birds of a Feather: Homophily in Social Networks. Annu. Rev. Sociol. 2001, 27, 415–444. [Google Scholar] [CrossRef] [Green Version]
- Fowler, J.H.; Christakis, N.A. Dynamic spread of happiness in a large social network: Longitudinal analysis over 20 years in the Framingham Heart Study. BMJ 2009, 338, 23–26. [Google Scholar] [CrossRef] [Green Version]
- Christakis, N.A.; Fowler, J.H. The Collective Dynamics of Smoking in a Large Social Network. N. Engl. J. Med. 2008, 358, 2249–2258. [Google Scholar] [CrossRef] [Green Version]
- Rosenquist, J.N.; Murabito, J.; Fowler, J.H.; Christakis, N.A. The spread of alcohol consumption behavior in a large social network. Ann. Intern. Med. 2010, 152, 426–433. [Google Scholar] [CrossRef] [Green Version]
- Holtz, D.; Zhao, M.; Benzell, S.G.; Cao, C.Y.; Rahimian, M.A.; Yang, J.; Allen, J.; Collis, A.; Moehring, A.; Sowrirajan, T.; et al. Interdependence and the cost of uncoordinated responses to COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 19837–19843. [Google Scholar] [CrossRef]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J.A. Vaccine hesitancy: An overview. Hum. Vaccin. Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Salmon, D.A.; Dudley, M.Z.; Glanz, J.M.; Omer, S.B. Vaccine hesitancy: Causes, consequences, and a call to action. Vaccine 2015, 33, D66–D71. [Google Scholar] [CrossRef]
- World Health Organization. Report of the SAGE Working Group on Vaccine Hesitancy; World Health Organization: Geneva, Switzerland, 2014; Available online: http://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed on 1 January 2021).
- Tricco, A.C.; Lillie, E.; Zarin, W.; Brien, K.K.O.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Ma, Q.; Horsley, T.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club 1995, 123, A12–A13. [Google Scholar] [CrossRef]
- Pontius, R.G.; Millones, M. Death to Kappa: Birth of quantity disagreement and allocation disagreement for accuracy assessment. Int. J. Remote Sens. 2011, 32, 4407–4429. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Bujold, M.; Wassef, M. Convergent and sequential synthesis designs: Implications for conducting and reporting systematic reviews of qualitative and quantitative evidence. Syst. Rev. 2017, 6, 61. [Google Scholar] [CrossRef] [Green Version]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A Product from the ESRC Methods Programme. ESRC Methods Program 2006, 1, b921. [Google Scholar] [CrossRef]
- Brunson, E.K. The impact of social networks on parents’ vaccination decisions. Pediatrics 2013, 131, e1397–e1404. [Google Scholar] [CrossRef] [Green Version]
- Casillas, A.; Singhal, R.; Tsui, J.; Glenn, B.A.; Bastani, R.; Mangione, C.M. The Impact of Social Communication on Perceived HPV vaccine effectiveness in a low-income, minority population. Ethn. Dis. 2011, 21, 495–501. [Google Scholar]
- Edge, R.; Heath, J.; Rowlingson, B.; Keegan, T.J.; Isba, R. Seasonal influenza vaccination amongst medical students: A social network analysis based on a cross-sectional study. PLoS ONE 2015, 10, e0140085. [Google Scholar] [CrossRef]
- Edge, R.; Keegan, T.; Isba, R.; Diggle, P. Observational study to assess the effects of social networks on the seasonal influenza vaccine uptake by early career doctors. BMJ Open 2019, 9, e026997. [Google Scholar] [CrossRef] [Green Version]
- Frank, L.B. Contagious: Social Norms about Health in Work Group Networks; University of Southern California: Los Angeles, CA, USA, 2011. [Google Scholar]
- Fu, L.Y.; Zimet, G.D.; Latkin, C.A.; Joseph, J.G. Social Networks for Human Papillomavirus Vaccine Advice among African American Parents. J. Adolesc. Health 2019, 65, 124–129. [Google Scholar] [CrossRef]
- Goldberg, A.B. Norms within Networks: Opinion Leader and Peer Network Influences on Mothers/Caregivers’ Childhood Immunization Decisions in Rural Northern Nigeria. Ph.D. Thesis, Columbia University, New York, NY, USA, 2014. [Google Scholar]
- Hernandez, E.M.; Pullen, E.; Brauer, J. Social networks and the emergence of health inequalities following a medical advance: Examining prenatal H1N1 vaccination decisions. Soc. Netw. 2019, 58, 156–167. [Google Scholar] [CrossRef]
- Mascia, D.; Iacopino, V.; Frisicale, E.M.; Iacovelli, A.; Boccia, S.; Poscia, A. The impact of school and after-school friendship networks on adolescent vaccination behavior. Vaccines 2020, 8, 55. [Google Scholar] [CrossRef] [Green Version]
- Nyhan, B.; Reifler, J.; Richey, S. The role of social networks in influenza vaccine attitudes and intentions among college students in the southeastern united states. J. Adolesc. Health 2012, 51, 302–304. [Google Scholar] [CrossRef]
- Ruiz, J.B. Immunizing against Vaccine Hesitancy: An Assessment of Online Communication and Social Network Factors Impacting Vaccine Adoption; Unversity of California: Oakland, CA, USA, 2015. [Google Scholar]
- Rulison, K.L.; Feinberg, M.; Gest, S.D.; Osgood, D.W. Diffusion of intervention effects: The impact of a family-based substance use prevention program on friends of participants. J. Adolesc. Health 2015, 57, 433–440. [Google Scholar] [CrossRef] [Green Version]
- Christakis, N.A. Social networks and collateral health effects. BMJ 2004, 329, 184–185. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Icek, A. The Theory of Planned Behavior Organizational Behavior and Human Decision Processes. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar]
- Jacob, M.; Bradley, J.; Barone, M.A. Human papillomavirus vaccines: What does the future hold for preventing cervical cancer in resource-poor settings through immunization programs? Sex. Transm. Dis. 2005, 32, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Oraby, T.; Thampi, V.; Bauch, C.T. The influence of social norms on the dynamics of vaccinating behaviour for paediatric infectious diseases. Proc. R. Soc. B Biol. Sci. 2014, 281. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, S.; Agerström, J. Do Social Norms Influence Young People’s Willingness to Take the COVID-19 Vaccine? PsyArXiv 2021. [Google Scholar] [CrossRef]
- Moehring, A.; Collis, A.; Garimella, K.; Rahimian, M.A.; Aral, S.; Eckles, D. Surfacing Norms to Increase Vaccine Acceptance. SSRN 2021, 1–33. [Google Scholar] [CrossRef]
- Malchodi, C.S.; Oncken, C.; Dornelas, E.A.; Caramanica, L.; Gregonis, E.; Curry, S.L. The effects of peer counseling on smoking cessation and reduction. Obstet. Gynecol. 2003, 101, 504–510. [Google Scholar] [CrossRef]
- Karimi, F.; Génois, M.; Wagner, C.; Singer, P.; Strohmaier, M. Homophily infuences ranking of minorities in social networks. Sci. Rep. 2018, 8, 11077. [Google Scholar] [CrossRef]
- Centola, D.; Gonzalez-Avella, J.C.; Eguíluz, V.M.; San Miguel, M. Homophily, Cultural Drift, and the Co-Evolution of Cultural Groups. J. Confl. Resolut. 2007, 51, 905–929. [Google Scholar] [CrossRef] [Green Version]
- Beck, C.; McSweeney, J.C.; Richards, K.C.; Roberson, P.K.; Tsai, P.F.; Souder, E. Challenges in tailored intervention research. Nurs. Outlook 2010, 58, 104–110. [Google Scholar] [CrossRef] [Green Version]
- Lawes-Wickwar, S.; Ghio, D.; Tang, M.Y.; Keyworth, C.; Stanescu, S.; Westbrook, J.; Jenkinson, E.; Kassianos, A.P.; Scanlan, D.; Garnett, N.; et al. A rapid systematic review of public responses to health messages encouraging vaccination against infectious diseases in a pandemic or epidemic. Vaccines 2021, 9, 72. [Google Scholar] [CrossRef]
- Ghio, D.; Lawes-Wickwar, S.; Tang, M.Y.; Epton, T.; Howlett, N.; Jekinson, E.; Stanescu, S.; Westbrook, J.; Kassianos, A.P.; Watson, D.; et al. What influences people’s responses to public health messages for managing risks and preventing infectious diseases? A rapid systematic review of the evidence and recommendations. PsyArXiv 2020. [CrossRef]
- Wrzus, C.; Hänel, M.; Wagner, J.; Neyer, F.J. Social network changes and life events across the life span: A meta-analysis. Psychol. Bull. 2013, 139, 53–80. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study 1 | Country | Aim | Population | Sample Size | % Females | Age 2 (M, SD) | Education 3 | Vaccination Type |
|---|---|---|---|---|---|---|---|---|
| Brunson (2013) [23] | USA | To examine the effect of parent, people and source networks on parents’ vaccination decisions. | First-time parents with children aged ≤18 months | 196 | 92.3% | 31.3 (4.7) | Bachelor’s degree: 46.4% | Childhood vaccinations (type not specified) |
| Casillas et al. (2011) [24] | USA | To examine the influence of hearing or discussing the vaccine with family/friends on perceived HPV vaccine effectiveness. | Low-income, minority women aged 18–65 | 294 | 100% | 43.9 (0.3) | Highest education—high school: 40.2% | HPV |
| Edge et al. (2015) [25] | UK | To examine the effects of social networks on influenza vaccination decision. | Primary undergraduate medical students at Lancaster Medical School | 217 | NR | NR | Primary undergraduate medical degree: 100% | Seasonal flu |
| Edge et al. (2019) [26] | UK | To evaluate the effect of social network on seasonal influenza vaccination uptake by healthcare workers. | Early career doctors working at the Pennine Acute Hospitals NHS Trust | 138 | 49.3% | NR | Early career doctors at year 1: 72.4% | Seasonal flu |
| Frank (2011) [27] | USA | To explore how social norms about health are understood in adults working together in organizational settings. | Adults who work together for the same organization in the same physical location | 152 | 57.0% | 30–49: 49.0% | 4-year college degree: 41.0% | H1N1 |
| Fu et al. (2019) [28] | USA | To examine the influence of social networks for HPV vaccine among African American parents. | African American parents of children aged 10–12 years | 353 | 94.1% | Median: 37 (NR) | ≤High school graduate: 45.3% Some college/technical school: 41.9% | HPV |
| Goldberg (2014) [29] | Nigeria | To examine the influence of social networks and social norms in mothers/caregivers immunization decisions and behaviours. | Mothers living in the Health and Demographic Surveillance System in Bungudu | 550 | 100% | 25–34: 42.4% | Qu’ranic school: 93.3% | All routine childhood vaccinations, e.g., Hepatitis B, Measles |
| Hernandez, Pullen & Brauer (2019) [30] | USA | To examine the role of social networks in decision making of H1N1 vaccination decisions during pregnancy. | Pregnant with first child | 223 | 100% | 29.9 (5.3) | Bachelor’s degree: 38.8% | H1N1 |
| Mascia et al. (2020) [31] | Italy | To explore the relationship between students’ vaccination behaviour and their friendship social networks. | Children up to 12 years | 49 | 45.0% | NR | Children in Class 1: 37% | All routine childhood vaccinations, e.g., Hepatitis B |
| Nyhan et al. (2012) [32] | USA | To examine the effects of social networks on perceptions and vaccination behaviour. | Undergraduate university students | 1018 | 64.0% | NR | Undergraduate university students: 100% | H1N1, seasonal flu |
| Ruiz (2015) [33] | USA | To assess HPV vaccination sources of information, knowledge, adoption and social networks among young adults. | Undergraduate university students | 346 | 66.2% | 20.22 (3.5) | Senior students: 40% Junior students: 39% | HPV |
| Study | Analytical Approach | Social Contagion Results | Impact of Social Networks on Vaccinations | Other Findings | ||
|---|---|---|---|---|---|---|
| Clustering 1 | Centrality 2 | Homophily 3 | ||||
| Childhood vaccinations (n = 4) | ||||||
| Brunson (2013) [23] | SNA:
| NR | NR | NR | Non-vaccination increased when having more non-conformers 4 in network (OR = 30.57, CI: 5.75–162.65). | Non-conformers 4 were more likely to have higher education (i.e., graduate degree; OR = 5.34, CI: 1.05–27.08) |
| Fu et al. (2019) [28] | LR:
| NR | NR | Participants tended to have similar social networks to themselves:
|
| The vaccine advice networks were small, dense, family centric, and homophilous. |
| Goldberg (2014) [29] | SNA:
| NR | Centrality did not predict vaccination uptake | Participants tend to have similar peers in networks:
|
|
|
| Mascia et al. (2020) [31] | SNA:
| NR | NR | Vaccination uptake was more similar in students with the same ethnicity (OR = 5.39–6.13), different gender (OR = 0.84–0.87) and belonging to the same class (OR = 1.68–1.82). | Students were more likely to report similar vaccination uptake with friendship ties occurring after school rather than those established during school (OR = 1.47). | - |
| Self-vaccination (n = 7) | ||||||
| Casillas et al. (2011) [24] | LR:
| NR | NR | NR | Participants were more likely to perceive the vaccine as effective:
| Having high school education as the highest education level decreased the odds of perceived vaccine effectiveness compared to no school and college levels (OR = 0.47, 95% CI: 0.23–0.96) |
| Edge et al. (2015) [25] | SNA:
| No clustering observed between vaccinated and non-vaccinated individuals | NR | NR | Participants were more likely to get vaccinated if they perceived their peers as being vaccinated (no statistical information reported). | - |
| Edge et al. (2019) [26] | SNA:
| NR | NR | No homophily observed (Assortativity = −0.03, 95% CI: −0.12–0.10) | Participants were more likely to get vaccinated if they had a higher proportion of vaccinated neighbors in their social network (OR = 2.63, 95% CI: 1.28 −5.38). | - |
| Frank (2011) [27] | SNA:
| People in the same working group in the company | NR | NR |
| - |
| Hernandez, Pullen and Brauer (2019) [30] | SNA:
| NR | NR | Well-educated women tend to have well-educated networks who support vaccination uptake |
| - |
| Nyhan et al. (2012) [32] | LR:
| NR | NR | NR |
| - |
| Ruiz (2015) [33] | LR:
| NR | NR | NR | Higher vaccination uptake, compared to non-vaccination, was associated with:
| Vaccinated participants were more likely to trust family members (75%) for information about vaccines compared to non-vaccinated (60%) (p < 0.05). |
| Type of Social Network | Vaccination Type | Studies | Vaccination Attitude | Further Research |
|---|---|---|---|---|
| General | All self and childhood | - | Positive Negative |
|
| Family/spouses/partners | H1N1 (Self) HPV (Self and Childhood) Seasonal flu (Self) | Casillas et al. (2011) [24] Fu et al. (2019) [28] Hernandez et al. (2019) [30] Nyhan et al. (2012) [32] Ruiz (2015) [33] | Positive | Mechanisms underlying why:
|
| All routine childhood H1N1 (Self) HPV (Childhood) Seasonal flu (Self) | Brunson et al. (2013) [23] Fu et al. (2019) [28] Hernandez et al. (2019) [30] Nyhan et al. (2012) [32] Ruiz (2015) [33] | Negative | ||
| Friends/Peers | All routine childhood H1N1 (Self) HPV (Self and Childhood) Seasonal flu (Self) | Casillas et al. (2011) [24] Edge et al. (2015) [25] Fu et al. (2019) [28] Goldberg (2014) [29] Hernandez et al. (2019) [30] Mascia et al. (2020) [31] Nyhan et al. (2012) [32] | Positive | |
| All routine childhood H1N1 (Self) HPV (Childhood) Seasonal flu (Self) | Brunson et al. (2013) [23] Fu et al. (2019) [28] Goldberg (2014) [29] Hernandez et al. (2019) [30] Nyhan et al. (2012) [32] | Negative | ||
| Health Care Providers | All routine childhood H1N1 (Self) HPV (Self) Seasonal flu (Self) | Casillas et al. (2011) [24] Goldberg (2014) [29] Hernandez et al. (2019) [30] Nyhan et al. (2012) [32] | Positive |
|
| All routine childhood H1N1 (Self) Seasonal flu (Self) | Brunson et al. (2013) [23] Goldberg (2014) [29] Hernandez et al. (2019) [30] Nyhan et al. (2012) [32] | Negative | ||
| Co-workers | H1N1 (Self) | Frank (2011) [27] | Positive | Mechanisms underlying why:
|
| All routine childhood H1N1 (Self) | Brunson et al. (2013) [23] Frank (2011) [27] | Negative | ||
| Politicians | All routine childhood | Goldberg (2014) [29] | Positive |
|
| - | - | Negative | ||
| Neighbours | Seasonal flu (Self) | Edge et al. (2019) [26] | Positive |
|
| - | - | Negative |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konstantinou, P.; Georgiou, K.; Kumar, N.; Kyprianidou, M.; Nicolaides, C.; Karekla, M.; Kassianos, A.P. Transmission of Vaccination Attitudes and Uptake Based on Social Contagion Theory: A Scoping Review. Vaccines 2021, 9, 607. https://doi.org/10.3390/vaccines9060607
Konstantinou P, Georgiou K, Kumar N, Kyprianidou M, Nicolaides C, Karekla M, Kassianos AP. Transmission of Vaccination Attitudes and Uptake Based on Social Contagion Theory: A Scoping Review. Vaccines. 2021; 9(6):607. https://doi.org/10.3390/vaccines9060607
Chicago/Turabian StyleKonstantinou, Pinelopi, Katerina Georgiou, Navin Kumar, Maria Kyprianidou, Christos Nicolaides, Maria Karekla, and Angelos P. Kassianos. 2021. "Transmission of Vaccination Attitudes and Uptake Based on Social Contagion Theory: A Scoping Review" Vaccines 9, no. 6: 607. https://doi.org/10.3390/vaccines9060607