
Challenges and Opportunities of Mass Vaccination Centers in COVID-19 Times: A Rapid Review of Literature

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Data Sources
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Data Extraction
3. Results
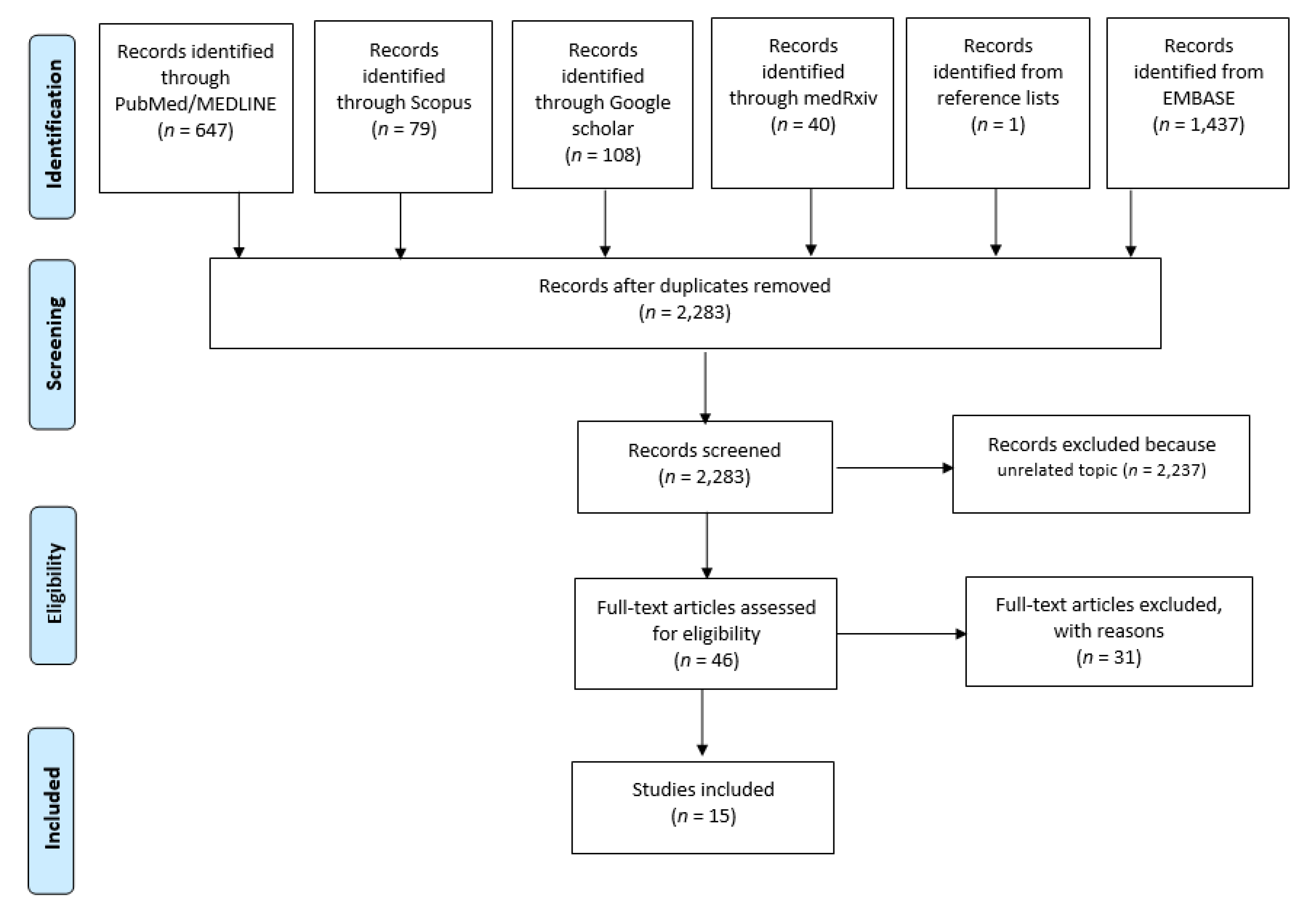
3.1. Literature Search
3.2. Characteristics of Included Studies
3.3. Preparation Needs
3.4. Layout
3.5. Dimensions of Mass Vaccination Center
3.6. Pharmacy Room
3.7. Restrooms
3.8. Staffing and Medical Procedures
3.9. Timing and Performance
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Signorelli, C.; Odone, A.; Gianfredi, V.; Bossi, E.; Bucci, D.; Oradini-Alacreu, A.; Frascella, B.; Capravo, M.; Chiappa, F.; Blandi, L.; et al. The spread of COVID-19 in six western metropolitan regions: A false myth on the excess of mortality in Lombardy and the defense of the city of Milan. Acta Biomed. 2020, 91, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Signorelli, C.; Odone, A.; Gianfredi, V.; Bossi, E.; Bucci, D.; Oradini-Alacreu, A.; Frascella, B.; Capraro, M.; Chiappa, F.; Blandi, L.; et al. COVID-19 mortality rate in nine high-income metropolitan regions. Acta Biomed. 2020, 91, 7–18. [Google Scholar] [PubMed]
- Paciullo, F.; Giannandrea, D.; Gianfredi, V.; Borgognoni, F.; Verdecchia, P.; L’Angiocola, P.D.; Monti, M. Epidemiology of emergency calls for time-dependent acute illnesses during COVID-19 outbreak in Umbria region (Italy). Ann Ig. 2020, 33, 198–200. [Google Scholar] [PubMed]
- Odone, A.; Delmonte, D.; Scognamiglio, T.; Signorelli, C. COVID-19 deaths in Lombardy, Italy: Data in context. Lancet Public Health 2020, 5, e310. [Google Scholar] [CrossRef]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19 11 March World Health Organization, Geneve. 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 6 April 2021).
- Bull, S.; Jamrozik, E.; Binik, A.; Parker, M.J. SARS-CoV-2 challenge studies: Ethics and risk minimisation. J. Med. Ethic 2020. [Google Scholar] [CrossRef]
- Signorelli, C.; Scognamiglio, T.; Odone, A. COVID-19 in Italy: Impact of containment measures and prevalence estimates of infection in the general population. Acta Biomed. 2020, 91, 175–179. [Google Scholar]
- Chung, J.Y.; Thone, M.N.; Kwon, Y.J. COVID-19 vaccines: The status and perspectives in delivery points of view. Adv. Drug Deliv. Rev. 2021, 170, 1–25. [Google Scholar] [CrossRef]
- World Health Organization. Special Feature: Immunization and COVID-19. Second Pulse Poll Offers a more Detailed Understanding of Disruptions to Vaccination Caused by COVID-19 and How to Respond; World Health Organization: Geneve, Switzerland, 2021; Available online: https://www.who.int/immunization/monitoring_surveillance/immunization-and-covid-19/en/ (accessed on 11 April 2021).
- Fontanet, A.; Cauchemez, S. COVID-19 herd immunity: Where are we? Nat. Rev. Immunol. 2020, 20, 583–584. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Guidelines for Large Scale Novel H1N1 Influenza Vaccination Clinics. 2009. Available online: https://www.cdc.gov/h1n1flu/vaccination/pdf/D_Wortley_H1N1_guidelines_pandemic.pdf (accessed on 8 April 2021).
- Direction Générale de Santé Publique. Organisation des Centres de Vaccination de Masse Contre La COVID-19; Direction Générale de Santé Publique: Quebec, QC, Canada, 2021; Available online: https://ciusssmcq.ca/Content/Client/Librairie/Documents/COVID-19/Vaccination_COVID_employes/Organisation-centre-vaccination-de-masse-12mars2021.pdf (accessed on 28 May 2021).
- France24. Disneyland Paris to Host Mass Covid Vaccination Site. 2021. Available online: https://www.france24.com/en/live-news/20210421-disneyland-paris-to-host-mass-covid-vaccination-site (accessed on 26 May 2021).
- Azienda Unità Sanitaria Locale di Parma. Vaccinazioni Anti-Covid 19: Bollettino del 26/05/2021. Available online: https://www.ausl.pr.it/comunicazione_stampa/archivio_3/vaccinazioni_anti_covid_bollettino_2021_37.aspx (accessed on 26 May 2021).
- Signorelli, C.; Odone, A.; Gianfredi, V.; Capraro, C.; Kacerik, E.; Chiecca, G.; Scardoni, A.; Minerva, M.; Mantecca, R.; Musarò, P.; et al. Application of the “immunization islands” model to improve quality, efficiency and safety of a COVID-19 mass vaccination site. Ann Ig. 2021, 5. [Google Scholar] [CrossRef]
- Tricco, A.C.; Langlois, E.V.; Straus, S.E. Rapid Reviews to Strengthen Health Policy and Systems: A Practical Guide; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Fontanesi, J.; Hill, L.; Olson, R.; Bennett, N.M.; Kopald, D. Mass vaccination clinics versus appointments. J. Med. Pract. Manag. 2006, 21, 288–294. [Google Scholar]
- Nolan, P. The Rhode Island meningitis vaccine experience—Mass vaccination campaigns, politics and health policy. Med. Health Rhode Isl. 2004, 87, 65–67. [Google Scholar]
- Jarrett, S.W. Smallpox eradication: Selected management issues. Assign. Child. 1985, 72, 243–261. [Google Scholar]
- Schindler, J.V.; Mraz, T. Agent-based modeling for real-time decision-support for point-of-distribution managers during influenza mass vaccination. AMIA Annu. Symp. Proc. 2008, 2008, 1124. [Google Scholar]
- Dervaux, B.; Leleu, H.; Valdmanis, V.; Walker, D. Parameters of control when facing stochastic demand: A DEA approach applied to Bangladeshi vaccination sites. Int. J. Health Care Financ. Econ. 2003, 3, 287–299. [Google Scholar] [CrossRef]
- Goralnick, E.; Kaufmann, C.; Gawande, A.A. Mass-Vaccination Sites—An Essential Innovation to Curb the Covid-19 Pandemic. N. Engl. J. Med. 2021, 384, e67. [Google Scholar] [CrossRef]
- Ha, E.C.; McCoy, M.D.A.; Taylor, C.B.; Kirk, K.D.; Fry, C.R.S.; Modi, J.R. Using Lean Six Sigma Methodology to Improve a Mass Immunizations Process at the United States Naval Academy. Mil. Med. 2016, 181, 582–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iacobucci, G. Covid vaccine: GPs need more clarity on logistics and planning, say leaders. BMJ 2020, 371, m4555. [Google Scholar] [CrossRef] [PubMed]
- Olmsted, S.S.; Grabenstein, J.D.; Jain, A.K.; Lurie, N. Patient experience with, and use of, an electronic monitoring system to assess vaccination responses. Health Expect. 2006, 9, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Savitz, S.; Stewart, J. Lessons Learned from Smallpox Vaccination of U.S. Navy Forces before Operation Iraqi Freedom. Mil. Med. 2007, 172, 353–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sim, F. Early Covid-19 vaccination rollout: A commentary from England. Isr. J. Health Policy Res. 2021, 10, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Sutter, R.W.; Maher, C. Mass vaccination campaigns for polio eradication: An essential strategy for success. Curr. Top. Microbiol. Immunol. 2006, 304, 195–220. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Iwane, M.K.; Humiston, S.E.; Schaffer, S.; McInerny, T.; Shone, L.; Jennings, J.; Washington, M.L.; Schwartz, B. Time Spent by Primary Care Practices on Pediatric Influenza Vaccination Visits. Arch. Pediatrics Adolesc. Med. 2003, 157, 191–195. [Google Scholar] [CrossRef] [Green Version]
- Kuehnert, P. Now More than Ever: Building and Sustaining Capacity for School-Located Vaccination Initiatives. J. Sch. Nurs. 2010, 26, 27S–29S. [Google Scholar] [CrossRef]
- Lee, T.H.; Chen, A.H. Last-Mile Logistics of Covid Vaccination—The Role of Health Care Organizations. N. Engl. J. Med. 2021, 384, 685–687. [Google Scholar] [CrossRef] [PubMed]
- Meyer, D.; Shearer, M.P.; Chih, Y.-C.; Hsu, Y.-C.; Lin, Y.-C.; Nuzzo, J.B. Taiwan’s Annual Seasonal Influenza Mass Vaccination Program—Lessons for Pandemic Planning. Am. J. Public Health 2018, 108, S188–S193. [Google Scholar] [CrossRef]
- Velimirovic, B. Mass vaccination programs administrative provisions and possibilities. La Ric. Clin. Lab. 1981, 2, 73–80. [Google Scholar]
- Gerber, R.; Murtagh, L.; Wolbert, C.J.; Tinkey, N.M.; Gobeille, B. Recent Developments in Health Law. J. Law Med. Ethic 2007, 35, 495–506. [Google Scholar] [CrossRef] [PubMed]
- Giot, J.L.; Loneux, J.C.; Mardaga, J.; Surleraux, C. Vaccination for viral hepatitis in industrial health. Acta Gastro Enterol. Belg. 2003, 66, 241–246. [Google Scholar]
- Arthur, B.C.; Fisher, A.K.; Shoemaker, S.J.; Pozniak, A.; Stokley, S. Business Models, Vaccination Services, and Public Health Relationships of Retail Clinics: A Qualitative Study. J. Health 2015, 60, 429–440. [Google Scholar] [CrossRef]
- Cho, B.-H.; Hicks, K.A.; Honeycutt, A.A.; Hupert, N.; Khavjou, O.; Messonnier, M.; Washington, M.L. A Tool for the Economic Analysis of Mass Prophylaxis Operations with an Application to H1N1 Influenza Vaccination Clinics. J. Public Health Manag. Pr. 2011, 17, E22–E28. [Google Scholar] [CrossRef] [PubMed]
- Garske, T.; Van Kerkhove, M.D.; Yactayo, S.; Ronveaux, O.; Lewis, R.F.; Staples, J.E.; Perea, W.; Ferguson, N.M. For the Yellow Fever Expert Committee Yellow Fever in Africa: Estimating the Burden of Disease and Impact of Mass Vaccination from Outbreak and Serological Data. PLoS Med. 2014, 11, e1001638. [Google Scholar] [CrossRef] [Green Version]
- Porco, T.C.; Holbrook, K.E.; Fernyak, S.; Portnoy, D.L.; Reiter, R.; Aragón, T.J. Logistics of community smallpox control through contact tracing and ring vaccination: A stochastic network model. BMC Public Health 2004, 4, 34. [Google Scholar] [CrossRef] [Green Version]
- Matteson, L.M. Using Seasonal Influenza Clinics for Public Health Preparedness Exercises. AJN Am. J. Nurs. 2006, 106, 28–29. [Google Scholar] [CrossRef]
- Nicoll, A. Pandemic Risk Prevention in European Countries: Role of the ECDC in Preparing for Pandemics; Springer: Berlin/Heidelberg, Germany, 2010; pp. 1267–1276. [Google Scholar] [CrossRef]
- Rambhia, K.J.K.J.; Watson, M.; Sell, T.K.; Waldhorn, R.; Toner, E. Mass Vaccination for the 2009 H1N1 Pandemic: Approaches, Challenges, and Recommendations. Biosecur. Bioterror. Biodef. Strategy Pract. Sci. 2010, 8, 321–330. [Google Scholar] [CrossRef]
- Rebmann, T.; Loux, T.M.; Zink, T.K.; Swick, Z.; Wakefield, M. Infection prevention and mass vaccination training for U.S. point of dispensing staff and volunteers: A national study. Am. J. Infect. Control 2015, 43, 222–227. [Google Scholar] [CrossRef]
- Rebmann, T.; Loux, T.M.T.M.; Swick, Z.; Dolgin, H.; Reddick, D.; Wakefield, M. Are US Jurisdictions Prepared to Dispense Medical Countermeasures Through Open Points of Dispensing? Findings from a National Study. Health Secur. 2015, 13, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Privor-Dumm, L.; Vasudevan, P.; Kobayashi, K.; Gupta, J. Archetype analysis of older adult immunization decision-making and implementation in 34 countries. Vaccine 2020, 38, 4170–4182. [Google Scholar] [CrossRef] [PubMed]
- Sarma, H.; Budden, A.; Luies, S.K.; Lim, S.S.; Shamsuzzaman, M.; Sultana, T.; Rajaratnam, J.K.; Craw, L.; Banwell, C.; Ali, W.; et al. Implementation of the World’s largest measles-rubella mass vaccination campaign in Bangladesh: A process evaluation. BMC Public Health 2019, 19, 1–10. [Google Scholar] [CrossRef]
- Schwartz, B.; Wortley, P. Mass vaccination for annual and pandemic influenza. In Current Topics in Microbiology and Immunology; Springer: Berlin/Heidelberg, Germany, 2006; pp. 131–152. [Google Scholar]
- Aaby, K.; Herrmann, J.W.; Jordan, C.; Treadwell, M.; Wood, K. Improving Mass Vaccination Clinic Operations. In Proceedings of the International Conference on Health Sciences Simulation, New Orleans, LA, USA, 23–27 January 2005. [Google Scholar]
- Andress, K. A postevent smallpox mass vaccination clinic exercise. Disaster Manag. Response 2003, 1, 54–58. [Google Scholar] [CrossRef]
- Asllani, A.; Dileepan, P.; Ettkin, L. A methodology for using simulation to optimize emergency mass vaccination parameters. J. Med. Syst. 2007, 31, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Asllani, A.; Dileepan, P.; Ettkin, L. Developing an Emergency Preparedness Plan: A Case for Simulation. Acad. Health Care Manag. J. 2007, 3, 51–63. [Google Scholar]
- Caum, J.; Alles, S. Ready or Not: Analysis of a No-Notice Mass Vaccination Field Response in Philadelphia. Biosecurity Bioterrorism: Biodefense Strat. Pract. Sci. 2013, 11, 262–270. [Google Scholar] [CrossRef]
- Gupta, A.; Evans, G.W.; Heragu, S.S. Simulation and optimization modeling for drive-through mass vaccination—A generalized approach. Simul. Model. Pract. Theory 2013, 37, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Ha, C.; Taylor, C.; Modi, J.R. Mass Vaccinations at the United States Naval Academy. Health Secur. 2016, 14, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Jenlink, C.H.; Kuehnert, P.; Mazyck, D. Key Components of a School-Located Vaccination Clinic: Lessons Learned from Fall 2009. J. Sch. Nurs. 2010, 26, 14S–26S. [Google Scholar] [CrossRef] [PubMed]
- Jenlink, C.H.; Kuehnert, P.; Mazyck, D. Influenza Vaccinations, Fall 2009: Model School-Located Vaccination Clinics. J. Sch. Nurs. 2010, 26, 7S–13S. [Google Scholar] [CrossRef] [PubMed]
- Kar, S.K.; Sah, B.; Patnaik, B.; Kim, Y.H.; Kerketta, A.S.; Shin, S.; Rath, S.B.; Ali, M.; Mogasale, V.; Khuntia, H.K.; et al. Mass Vaccination with a New, Less Expensive Oral Cholera Vaccine Using Public Health Infrastructure in India: The Odisha Model. PLoS Negl. Trop. Dis. 2014, 8, e2629. [Google Scholar] [CrossRef] [PubMed]
- Phillips, F.B.; Williamson, J.P. Local Health Department Applies Incident Management System for Successful Mass Influenza Clinics. J. Public Health Manag. Pract. 2005, 11, 269–273. [Google Scholar] [CrossRef]
- Porter, D.; Hall, M.; Hartl, B.; Raevsky, C.; Peacock, R.; Kraker, D.; Walls, S.; Brink, G. Local Health Department 2009 H1N1 Influenza Vaccination Clinics—CDC Staffing Model Comparison and Other Best Practices. J. Public Health Manag. Pract. 2011, 17, 530–533. [Google Scholar] [CrossRef]
- Swift, M.D.; Aliyu, M.H.; Byrne, D.W.; Qian, K.; McGown, P.; Kinman, P.O.; Hanson, K.L.; Culpepper, D.; Cooley, T.J.; Yarbrough, M.I. Emergency Preparedness in the Workplace: The Flulapalooza Model for Mass Vaccination. Am. J. Public Health 2017, 107, S168–S176. [Google Scholar] [CrossRef] [Green Version]
- COVID-19 Vaccines Begin at Disneyland Parking Lot, Orange County’s First Super Site. Available online: https://www.ocregister.com/2021/01/13/covid-19-vaccine-shots-begin-at-disneyland-parking-lot-orange-countys-first-super-site/ (accessed on 27 May 2021).
- Yang, J.; Acosta, C.J.; Si, G.-A.; Zeng, J.; Li, C.-Y.; Liang, D.-B.; Ochiai, R.L.; Page, A.-L.; Danovaro-Holliday, M.C.; Zhang, J.; et al. A mass vaccination campaign targeting adults and children to prevent typhoid fever in Hechi; Expanding the use of Vi polysaccharide vaccine in Southeast China: A cluster-randomized trial. BMC Public Health 2005, 5, 49. [Google Scholar] [CrossRef] [Green Version]
- Bundesanstalt für Arbeitsschutz und Arbeitsmedizin. Empfehlung des Ausschusses für Biologische Arbeitsstoffe (ABAS) zu “Arbeitsschutzmaßnahmen bei der Durchführung von Impfungen gegen SARS-CoV-2 in Impfzentren”. Berlin; January 2021 Contract No.: Beschluss 21/2020. Available online: https://www.baua.de/DE/Aufgaben/Geschaeftsfuehrung-von-Ausschuessen/ABAS/Empfehlungen.html (accessed on 27 May 2021).
- National Health Service. COVID-19 Vaccination Centres: Operating Framework. Information and Guidance on Operating Vaccination Centres. 20 January 2021 Contract No.: 001559. Available online: https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2021/01/C1034-operating-framework-information-and-guidance-on-operating-vaccination-centres-v1.1-20-january-21.pdf (accessed on 27 May 2021).
- Gianfredi, V.; Dallagiacoma, G.; Provenzano, S.; Santangelo, O.E. Factors predicting health science students’ willingness to be vaccinated against seasonal flu during the next campaign. Ann Ist Super Sanita 2019, 55, 209–216. [Google Scholar] [PubMed]
- Riccò, M.; Vezzosi, L.; Gualerzi, G.; Signorelli, C. Knowledge, attitudes and practices (KAP) towards vaccinations in the school settings: An explorative survey. J. Prev. Med. Hyg. 2017, 58, E266–E278. [Google Scholar] [PubMed]
- Ricco, M.; Vezzosi, L.; Gualerzi, G.; Balzarini, F.; Mezzoiuso, A.G.; Odone, A.; Signorelli, C. Measles vaccine in the school settings: A cross-sectional study about knowledge, personal beliefs, attitudes and practices of school teachers in northern Italy. Minerva Pediatrica 2018. [Google Scholar] [CrossRef]
- Wallace, M.; Woodworth, K.R.; Gargano, J.W.; Scobie, H.M.; Blain, A.E.; Moulia, D.; Chamberland, M.; Reisman, N.; Hadler, S.C.; MacNeil, J.R.; et al. The Advisory Committee on Immunization Practices’ Interim Recommendation for Use of Pfizer-BioNTech COVID-19 Vaccine in Adolescents Aged 12–15 Years—United States, May 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 749–752. [Google Scholar] [CrossRef]
- Ricco, M.; De Nard, F.; Peruzzi, S. Mosaic vaccination schedule: An unexpected card to play against SARS-CoV-2? Infect. Dis. Now 2021, 51, 402–405. [Google Scholar] [CrossRef]
- Cella, P.; Voglino, G.; Barberis, I.; Alagna, E.; Alessandroni, C.; Cuda, A.; D’Aloisio, F.; Dallagiacoma, G.; De Nitto, S.; Di Gaspare, F.; et al. Resources for assessing parents’ vaccine hesitancy: A systematic review of the literature. J Prev. Med. Hyg. 2020, 61, E340–E373. [Google Scholar]
- Gianfredi, V.; Grisci, C.; Nucci, D.; Parisi, V.; Moretti, M. Communication in health. Recenti Prog Med. 2018, 109, 374–383. [Google Scholar] [CrossRef]
- Razai, M.S.; Chaudhry, U.A.R.; Doerholt, K.; Bauld, L.; Majeed, A. Covid-19 vaccination hesitancy. BMJ 2021, 373. [Google Scholar] [CrossRef]
- Bass, S.B.; Wilson-Genderson, M.; Garcia, D.T.; Akinkugbe, A.A.; Mosavel, M. SARS-CoV-2 Vaccine Hesitancy in a Sample of US Adults: Role of Perceived Satisfaction with Health, Access to Healthcare, and Attention to COVID-19 News. Front. Public Health 2021, 9, 665724. [Google Scholar] [CrossRef] [PubMed]
- Coustasse, A.; Kimble, C.; Maxik, K. COVID-19 and Vaccine Hesitancy. J. Ambul. Care Manag. 2021, 44, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Odone, A.; Bucci, D.; Croci, R.; Riccò, M.; Affanni, P.; Signorelli, C. Vaccine hesitancy in COVID-19 times. An update from Italy before flu season starts. Acta Biomed. 2020, 91, e2020031. [Google Scholar]
- Gianfredi, V.; Monarca, S.; Moretti, M.; Villarini, M. Health education, what is the role for pharmacist? Results from a cross sectional study in Umbria, Italy. Recenti Progress. Med. 2017, 108, 433–441. [Google Scholar]
- Gianfredi, V.; Odone, A.; Fiacchini, D.; Rosselu, R.; Battista, T.; Signorelli, C. Trust and reputation management, branding, social media management nelle organizzazioni sanitarie: Sfide e opportunity per la comunita igienistica italiana. J. Prev. Med. Hyg. 2019, 60, E108–E109. [Google Scholar]
- Government of Canada. Planning Guidance for Immunization Clinics for COVID-19 Vaccines. 2021. Available online: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/guidance-documents/planning-immunization-clinics-covid-19-vaccines.html#a2.2 (accessed on 20 May 2021).
- Gianfredi, V.; Moretti, M.; Lopalco, P.L. Countering vaccine hesitancy through immunization information systems, a narrative review. Hum. Vaccines Immunother. 2019, 15, 2508–2526. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Balzarini, F.; Gola, M.; Mangano, S.; Carpagnano, L.F.; Colucci, M.E.; Gentile, L.; Piscitelli, A.; Quattrone, F.; Scuri, S.; et al. Leadership in Public Health: Opportunities for Young Generations Within Scientific Associations and the Experience of the “Academy of Young Leaders”. Front. Public Health 2019, 7, 378. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Author | Year | Country | Vaccine | Preparation Needs | Layout | Dimension * | Location |
|---|---|---|---|---|---|---|---|
| Aaby et al. [49] | 2004 | USA | Smallpox | Not available | Triage station outside the center where linear flow split in two lines according to medical history, registration station, waiting rooms with educational videos, screening station, consultation station (only for people with comorbidities), vaccination station, exit | Not available | School |
| Andress, et al. [50] | 2003 | USA | Smallpox | Strategy meetings; visit the potential sites; training involved personnel, staff distinctive vest for personnel | Vaccine storage, triage, screening, education, isolation, vaccination, computer entry, with signs identifying the stations | 105,000 square foot | Shopping mall |
| Asllani et al. [51] | 2007 | USA | Influenza | Trained personnel, transportation, equipment, retrieve available guidelines, vaccines, visits to the potential sites and investigate the layout | Registration immediately after entrance, waiting rooms with educational videos, medical evaluation rooms, vaccination station, and exit | Not applicable | Computer simulation |
| Asllani et al. [52] | 2007 | USA | Influenza | transportation vehicles, medical and assistant equipment such as wheelchairs | Entrance, registration area, waiting rooms with educational videos, vaccination room or medical evaluation area for those with comorbidities, waiting room and exit | Not applicable | Computer simulation |
| Caum et al. [53] | 2013 | USA | Influenza | Estimate number of doses needed, ensure that stocks arrived, evaluate which vaccine formulation to offer, understand characteristics of target population (if any special needs), training personnel also in electronic data entry | The vaccinator sat between the 2 seated patients to facilitate rapid access to patients. Drawer was on the other side of the room ensuring a setady supply of vaccine. For each patient’s seat there was a data collector | Not available | School |
| Gupta et al. [54] | 2009 | USA | Influenza | Not available | Arrival, consent hand out lane, consent form filled in lane, vaccination at the point of dispense, detour and depart | Vehicle gap length 12 feet, length of the consent form lane 950 feet, length of vaccination lane 50 feet | Drive-through clinic at a stadium |
| Ha et al. [55] | 2014 | USA | Influenza | Standardized training for personnel, meeting, staff distinctive vest for personnel | Linear flow split in two lines according to medical history; with signs identifying the stations | Not available | Auditorium |
| Jenlink et al. [56] | 2009 | USA | Influenza for children | Promotional campaign to the population only when sure about vaccine supply. One lot per day for each center in order to print the lot number on all the form and save time. Determine target population for the vaccine. Secure supply | Unidirectional linear flow from gathering area, multiple stations for eligiblity, screening, completition and review form, and perform vaccination; and 1 post-vaccination area | Not available | School |
| Jenlink et al. [57] | 2009 | USA | Influenza for adults | Preparation meeting during the summer in order to know the vaccination plan and flu update | Not available | Not available | Clinics with school nurses |
| Kar et al. [58] | 2011 | India | Cholera | Training for staff | Screening, verbal consent, vaccination station, registration station, waiting room, issued vaccination cards, collected remaining vaccine vials and waste at the end of each session, and brought waste back to the designated health facility | Not available | School and local clubs |
| Phillips et al. [59] | 2004 | USA | Influenza | Staff meeting one week before to ensure availability of administrative and clinical supplies, distribute staffing schedules, and order staff refreshments. A mandatory meeting for all staff involved was planned the day before the mass vaccination day | Incident Command Center, staff accommodations, restrooms, entrance and exits, parking and proposed traffic flow with signs and marking corridors | Not available | School |
| Porter et al. [60] | 2009 | USA | Influenza | A good reservation system in plan, scanner, personnel | Not available | Not available | Health department location |
| Swift et al. [61] | 2011–2015 | USA | Influenza | Staff meetings to identify challenges and opportunities. Training for staff | Entrance in the midway along the long side of the tent, 4 lines with traffic flow personnel who directed to 18 horizontal vaccination stations. Vaccination station, documentation stations and exit. The vaccination tent also contained the incident command center. Next to the vaccination tent there was an emergency medical tent | 40 × 120 feet | Outdoor tent clinic outside the hospital |
| Wheeler et al. [62] | 2021 | USA | COVID-19 | A phone app and web-site appointment systems | Parking, check-in station, waiting area, recovery and observational tent | Not available | Disneyland parking |
| Yang et al. [62] | 2003 | China | Typhoid fever and meningitis A | Promotional campaign, training for staff, simulation with a sub sample | Multiple vaccination centers (107), one for each cluster | Not available | School, health facility, factory or locations such as intersections and squares |
| Author | Pharmacy Room | Restrooms | Waiting Room Capacity and Management | Staffing | Medical Procedures | Timing/Performance | Others | Map |
|---|---|---|---|---|---|---|---|---|
| Aaby et al. [49] | Vaccines stored at the logistic hub at Hechi CDC: a 3 × 12 m2 room equipped with 8 refrigerators and 1 freezer | Not available | Not available | Staff number needed for each stage: triage: 5; registration:8; education: 8; screening: 9; consultation: 6; vaccination: 16 | Injection performed by nurses. Medical history collectors not available | Time for each stage: triage: 2:18; registration: 2:43; education: 31:23; screening: 16:77; vaccination: 8:87; total in system 60:02 Working time: 2:30 p.m.–3 p.m. | Not available | No |
| Andress, et al. [50] | Forecasted without details | Large enough in order to guarantee accessibility for all | Not forecasted | 140 in total, including human resources manager, translators, security and nurses | Medical history collection and vaccine injection performed by medical staff (nurses and physicians) | 104 vaccinations in 2 h (it was a 2-h exercise) | Not available | No |
| Asllani et al. [51] | Not available | Not available | Not available | Not available | Not available | 50,000 vaccinations in 3 days | Creation of a network among the mass vaccination centers in order to share resources dynamically | Yes |
| Asllani et al. [52] | Not available | Not available | Not available | Not available | Not available | 700 vaccinations per hour; vaccination session lasted 24 h. Time for each stage for person: registration 30–90 s, registration form 2 min, video watch 3–5 min, medical evaluation 2–10 min, vaccine administration 2–4 min | Not available | Yes |
| Caum et al. [53] | Not available | Not available | Stores of emergency medical materials; capacity not available | 1 vaccinator, 1 drawer, 1 data collector with a range of vaccination stations up to 14. Presence of a human resources manager to supervise the tasks of each staff ensuring that everyone understood their role | Data collectors interviewed the students. Injection performed by vaccinator (not otherwise specified) | 32–45 people for each vaccination station per hour; vaccination session lasted 1:30 (1:05–2:35 p.m.). In total 52 people in 54 min | Preference of electronic data entry | Yes |
| Gupta et al. [54] | Not available | Not available | Not available | Not available | Consent form workers who distributed and received the filled-out consent forms. Injection performed by medical workers | 7732 vaccinations in a 12 h (7 a.m.–7 p.m.); 12,613 served via 10 drive-through lanes after two days. Time for each person: 27.4+/−0.8 min | Not available | No |
| Ha et al. [55] | Store vaccines in standardized boxes, placed where trained staff exactly know. Vaccination stations placed closer together and near the supply box | Not available | Not available | 40 in total | Medical history collected by nurses or healthcare providers. Injectors not available | 4500 vaccinations in 6 h (time for each vaccination session). Working days: 3 | Not available | Yes |
| Jenlink et al. [56] | Strict regulation of thermometers. Attention to the refrigerated transportation | Not available | 15 min of observation; capacity not available | Nurses paid and on a voluntary basis (nursing students). For each vaccinator 4 nonmedical staff useful as greeters, traffic direction, form review, and supply runners. School staff to obtain consent for vaccination | 1 to 10 rooms each with 5 to 6 nurses for screening and checking the form and vaccinate | 2500 s doses in 3 h (time for vaccination session). Time for each person: 30 min | School was a good location for child vaccination because guardians/parents did not need to take time off from work | No |
| Jenlink et al. [57] | Not available | Not available | 15 min of observation; capacity not available | School staff to obtain consent for vaccination. Nurses to check the consent form | Not available | 11,200 vaccinations in 5 h for the 9 clinics. 100 appointments for every 5–8 min settled by the call center dedicated. Working days: 3 weeks, during the evening or on Saturday | Not available | No |
| Kar et al. [58] | Not available | Not available | Not available | 395 health workers/volunteers organized in team | Not available | Working time: 7:00 a.m.–5:00 p.m. for 3 consecutive days in each round from 5 May to 4 June 2011 (in total 15 working days) | The walk-in cooler temperature was monitored and maintained between +2 to +8C | No |
| Phillips et al. [59] | Not available | Not available | Not available | 36 nurses, 10 personals to record electronically data, 2 persons to greet at the entrance, 5 traffic flow personnel, 15 persons to screen for vaccine eligibility, 2 persons to maintain real time hourly vaccine counts | Not available | 640 vaccinations per hour; each vaccination session lasted 8 h (8:20 a.m.–5 p.m.). Working days: 2 consecutive Saturdays | The fire department provided a basic life support ambulance on sire, and voluntary companies provided refreshments from a fully equipped service vehicle | No |
| Porter et al. [60] | Not available | Breaks and lunches coordinated by area supervisors | Not available | 1 vaccine preparator for 4 vaccinators, 133 physicians, 43 vaccinators, 11 vaccine preparer, 77 administrative staff | Medical history collected by staff. Injection performed by nurses | 7889 vaccinations in 9.5 h (time for each vaccination session). Time for each person: 15 min | Not available | No |
| Swift et al. [61] | Not available | A staff break room stocked with snacks and beverages | Tent located adjacent to the vaccination clinic; capacity not available | Leaders from occupational health, nurses, pharmacists, student health, supply management, human resources, safety and event officers | Injection performed by nurses or pharmacists or nursing or pharmacy students certified to administer intramuscular injections. Medical history collectors not available | 12,850 with 37.1 vaccines per vaccinator/hour. Each vaccination session lasted 8 h (10 a.m.–4 p.m.). Working days: 1–2 days/year per 5 years in total | Each vaccination station was supplied with a flag system allowing vaccinators to raise color-coded flags Job action sheet were provided to the staff. Prefer one location in order to facilitate staff management, supply and avoid surplus or shortages in one of the centers | Yes |
| Wheeler et al. [62] | Not available | Not available | Tent with medical staff; capacity not available | Not available | Not available | 7500–8000 vaccinations for each vaccination session. Time for each person: 30 min | Not available | No |
| Yang et al. [62] | Not available | Not available | 15 min of observation monitored by physicians; capacity not available | 30 physicians, 43 nurses, 24 other health workers and 9 nonhealth workers to record data, 78 community helpers to facilitate the process. Each cluster was provided by a team based on one physician, one nurse, one recorder and one community helper | Injection performed by nurses. Medical history collectors not available | 200 vaccinations for each cluster per day. Working days: 31, from 8 April to 12 May 2003 | Each vaccination center administered only one vaccine | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gianfredi, V.; Pennisi, F.; Lume, A.; Ricciardi, G.E.; Minerva, M.; Riccò, M.; Odone, A.; Signorelli, C. Challenges and Opportunities of Mass Vaccination Centers in COVID-19 Times: A Rapid Review of Literature. Vaccines 2021, 9, 574. https://doi.org/10.3390/vaccines9060574
Gianfredi V, Pennisi F, Lume A, Ricciardi GE, Minerva M, Riccò M, Odone A, Signorelli C. Challenges and Opportunities of Mass Vaccination Centers in COVID-19 Times: A Rapid Review of Literature. Vaccines. 2021; 9(6):574. https://doi.org/10.3390/vaccines9060574
Chicago/Turabian StyleGianfredi, Vincenza, Flavia Pennisi, Alessandra Lume, Giovanni Emanuele Ricciardi, Massimo Minerva, Matteo Riccò, Anna Odone, and Carlo Signorelli. 2021. "Challenges and Opportunities of Mass Vaccination Centers in COVID-19 Times: A Rapid Review of Literature" Vaccines 9, no. 6: 574. https://doi.org/10.3390/vaccines9060574