
Cross-Sectional Study of Varicella Zoster Virus Immunity in Healthy Korean Children Assessed by Glycoprotein Enzyme-Linked Immunosorbent Assay and Fluorescent Antibody to Membrane Antigen Test


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Glycoprotein Enzyme-Linked Immunoassay (gpEIA)
2.3. Fluorescent Antibody to Membrane Antigen (FAMA) Test
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Enrolled Children
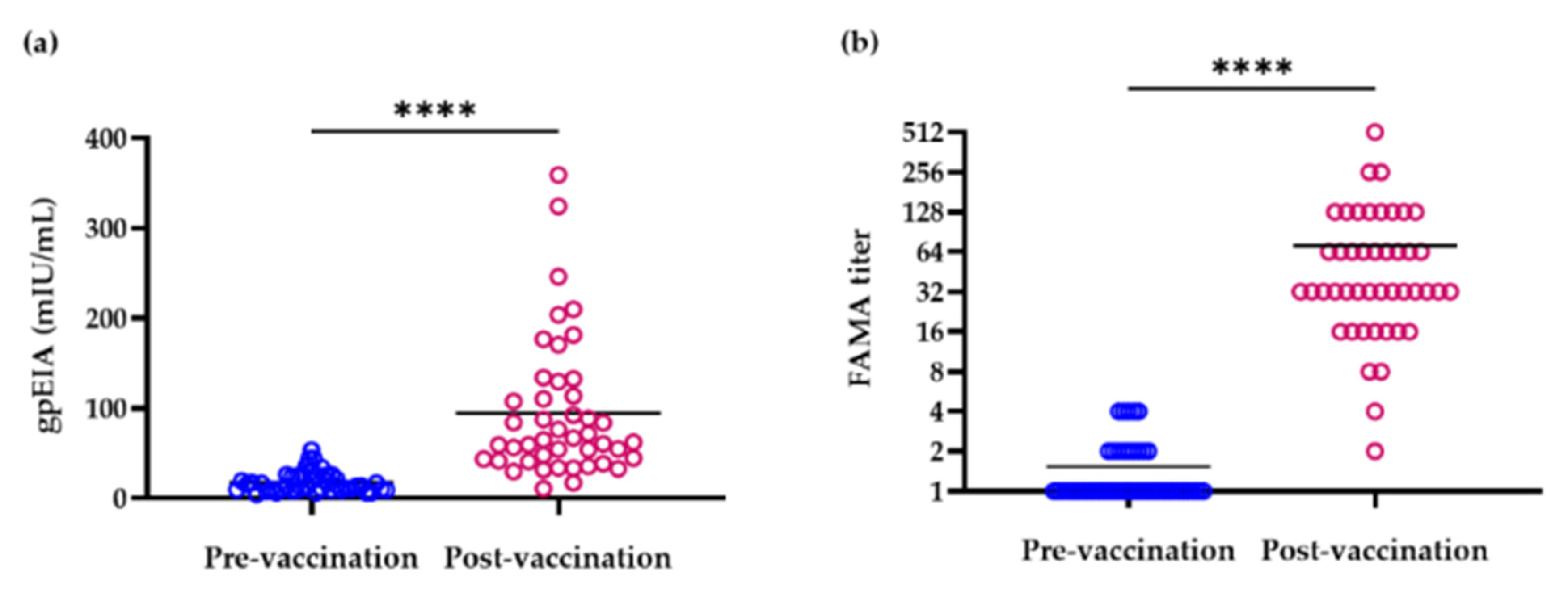
3.2. gpEIA Titer and FAMA Seroprevalence of Pre- and Post-Vaccination Sera
3.3. gpEIA GMT of 2- to 6-Year-Old Children
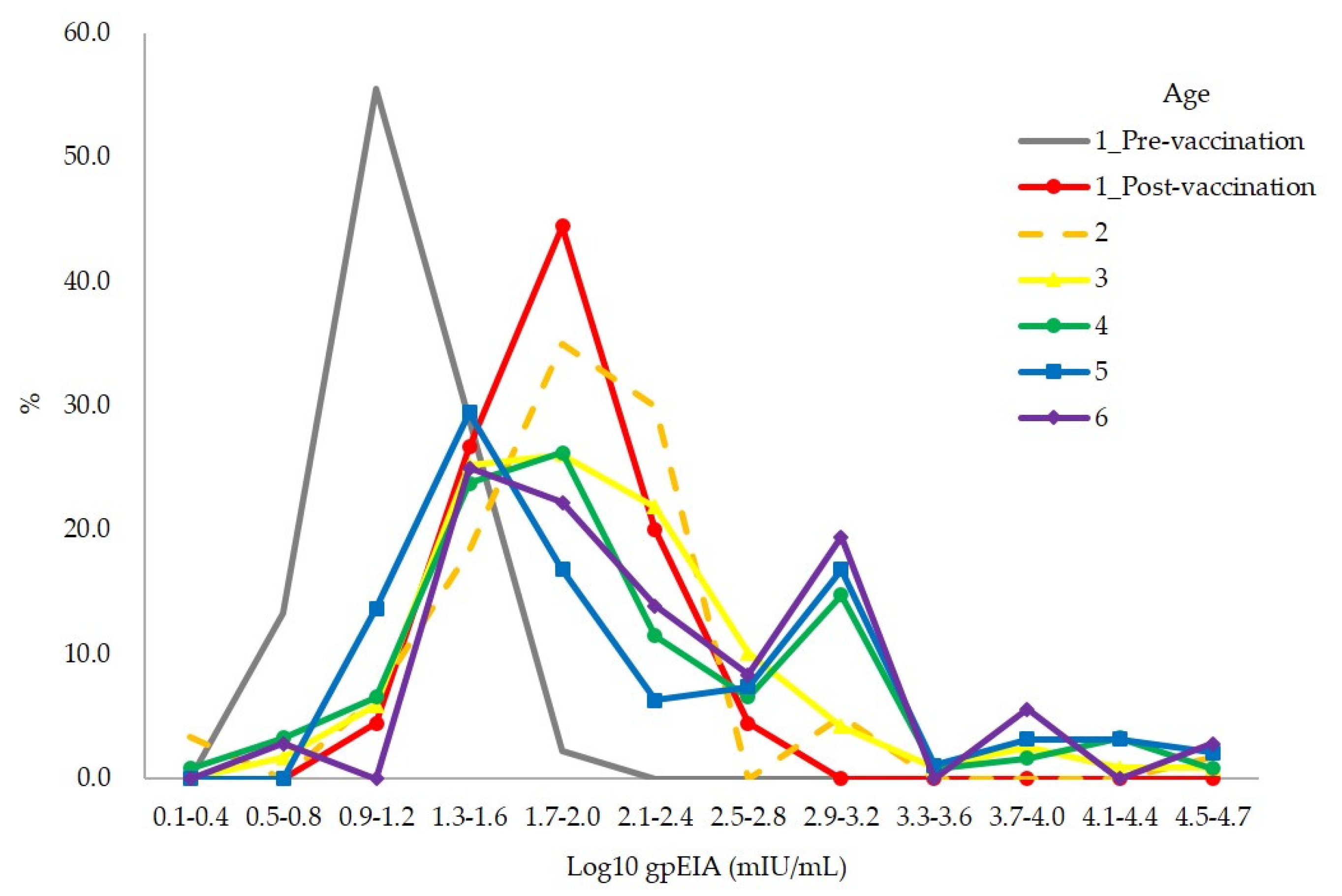
3.4. Distribution of gpEIA Antibody Titer among Vaccinees without Varicella History
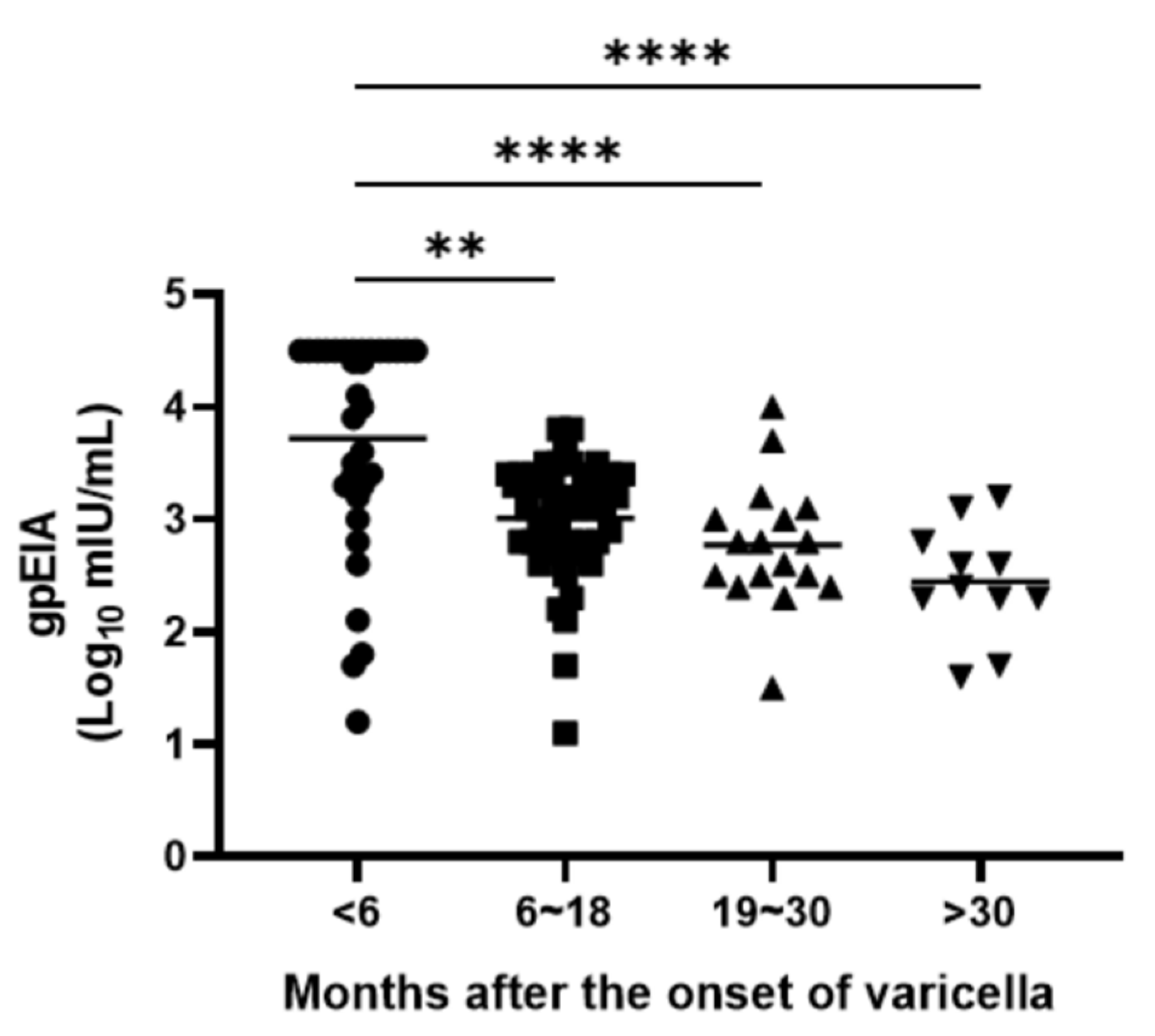
3.5. Waning of Immunity among Vaccinees with Varicella History
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hope-Simpson, R.E. The Nature of Herpes Zoster: A Long-Term Study and a New Hypothesis. Proc. R. Soc. Med. 1965, 58, 9–20. [Google Scholar] [CrossRef] [Green Version]
- Galil, K.; Brown, C.; Lin, F.; Seward, J. Hospitalizations for varicella in the United States, 1988 to 1999. Pediatr. Infect. Dis. J. 2002, 21, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Meyer, P.A.; Seward, J.F.; Jumaan, A.O.; Wharton, M. Varicella mortality: Trends before vaccine licensure in the United States, 1970–1994. J. Infect. Dis. 2000, 182, 383–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H. Survey on Efficacy and Safety of Varicella Vaccine as a Regular Vaccine in Korea. 2005, Volume 139. Available online: https://scienceon.kisti.re.kr/srch/selectPORSrchReport.do?cn=TRKO201300000675 (accessed on 5 April 2021).
- Kim, K.Y.; Jeon, S.Y.; Jeon, M.J.; Lee, K.H.; Lee, S.G.; Kim, D.; Kang, E.; Bae, S.G.; Kim, J. Health impact assessment of free immunization program in Jinju City, Korea. J. Prev. Med. Public Health 2012, 45, 267–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.K.; Kim, S.H.; Chun, B.C.; Kim, K.H.; Lee, H.J. Vaccination coverage in Korean children of six years old and younger. In Proceedings of the 57th Annual Fall Meeting of the Korean Pediatric Society, Seoul, Korea, 19–20 October 2007; p. 90. [Google Scholar]
- Park, B.; Lee, Y.K.; Cho, L.Y.; Go, U.Y.; Yang, J.J.; Ma, S.H.; Choi, B.Y.; Lee, M.S.; Lee, J.S.; Choi, E.H.; et al. Estimation of nationwide vaccination coverage and comparison of interview and telephone survey methodology for estimating vaccination status. J. Korean Med. Sci. 2011, 26, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Statistics for Inoculation Rate in Varicella Vaccine. Korean Statistical Information Service. Available online: https://kosis.kr/statHtml/statHtml.do?orgId=177&tblId=DT_11793N_171&conn_path=I3 (accessed on 6 April 2021).
- Infectious Disease Surveillance Annual Report 2005–2019. Korea Disease Control and Prevention Agency, Infectious Disease Portal. Available online: http://www.kdca.go.kr/npt/biz/npp/ist/bass/bassSexdstnAgeStatsMain.do# (accessed on 6 April 2021).
- Kang, J.H.; Kim, J.H.; Hur, J.K.; Woo, K. Tow-Year Follow-up Study for Clinical Feature and Immunity of The Children, Vaccinated by 47 Passaged Oka Strain Live Attenuated Varicella Vaccine. Korean J. Pediatr. Infect. Dis. 2000, 7, 129–135. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.H.; Hwang, J.Y.; Shim, H.M.; Lee, E.; Park, S.; Park, H. Evaluation of a commercial glycoprotein enzyme-linked immunosorbent assay for measuring vaccine immunity to varicella. Yonsei Med. J. 2014, 55, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Williams, V.; Gershon, A.; Brunell, P.A. Serologic response to varicella-zoster membrane antigens measured by direct immunofluorescence. J. Infect. Dis. 1974, 130, 669–672. [Google Scholar] [CrossRef]
- Arnedo-Pena, A.; Puig-Barbera, J.; Aznar-Orenga, M.A.; Ballester-Albiol, M.; Pardo-Serrano, F.; Bellido-Blasco, J.B.; Romeu-Garcia, M.A. Varicella vaccine effectiveness during an outbreak in a partially vaccinated population in Spain. Pediatr. Infect. Dis. J. 2006, 25, 774–778. [Google Scholar] [CrossRef]
- Gershon, A.A.; Krugman, S. Seroepidemiologic survey of varicella: Value of specific fluorescent antibody test. Pediatrics 1975, 56, 1005–1008. [Google Scholar] [PubMed]
- Kurugol, Z.; Halicioglu, O.; Koc, F.; Koturoglu, G.; Aksit, S. Varicella rates among unvaccinated and one-dose vaccinated healthy children in Izmir, Turkey. Int. J. Infect. Dis. 2011, 15, e475–e480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spackova, M.; Wiese-Posselt, M.; Dehnert, M.; Matysiak-Klose, D.; Heininger, U.; Siedler, A. Comparative varicella vaccine effectiveness during outbreaks in day-care centres. Vaccine 2010, 28, 686–691. [Google Scholar] [CrossRef] [PubMed]
- Tafuri, S.; Martinelli, D.; De Palma, M.; Germinario, C.; Prato, R. Report of varicella outbreak in a low vaccination coverage group of otherwise healthy children in Italy: The role of breakthrough and the need of a second dose of vaccine. Vaccine 2010, 28, 1594–1597. [Google Scholar] [CrossRef]
- Tafuri, S.; Martinelli, D.; Prato, R.; Germinario, C. Vaccine effectiveness evaluation during a varicella outbreak among children of primary schools and day-care centers in a region which adopted UMV. Hum. Vaccines Immunother. 2013, 9, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Vazquez, M.; LaRussa, P.S.; Gershon, A.A.; Steinberg, S.P.; Freudigman, K.; Shapiro, E.D. The effectiveness of the varicella vaccine in clinical practice. N. Engl. J. Med. 2001, 344, 955–960. [Google Scholar] [CrossRef]
- Michalik, D.E.; Steinberg, S.P.; Larussa, P.S.; Edwards, K.M.; Wright, P.F.; Arvin, A.M.; Gans, H.A.; Gershon, A.A. Primary vaccine failure after 1 dose of varicella vaccine in healthy children. J. Infect. Dis. 2008, 197, 944–949. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, S.A.; Orenstein, W.A.; Offit, P.A. Vaccines, 6th ed.; Elsevier Saunders: Philadelphia, PA, USA, 2013. [Google Scholar]
- Oh, S.H.; Choi, E.H.; Shin, S.H.; Kim, Y.K.; Chang, J.K.; Choi, K.M.; Hur, J.K.; Kim, K.H.; Kim, J.Y.; Chung, E.H.; et al. Varicella and varicella vaccination in South Korea. Clin. Vaccine Immunol. 2014, 21, 762–768. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Cho, H.K.; Kim, K.H. Seroepidemiology of varicella-zoster virus in Korea. J. Korean Med. Sci. 2013, 28, 195–199. [Google Scholar] [CrossRef] [Green Version]
- Choi, U.Y.; Huh, D.H.; Kim, J.H.; Kang, J.H. Seropositivity of Varicella zoster virus in vaccinated Korean children and MAV vaccine group. Hum. Vaccines Immunother. 2016, 12, 2560–2564. [Google Scholar] [CrossRef] [Green Version]
- Ndumbe, P.M.; Cradock-Watson, J.; Levinsky, R.J. Natural and artificial immunity to varicella zoster virus. J. Med. Virol. 1988, 25, 171–178. [Google Scholar] [CrossRef]
- Jeon, J.S.; Won, Y.H.; Kim, I.K.; Ahn, J.H.; Shin, O.S.; Kim, J.H.; Lee, C.H. Analysis of single nucleotide polymorphism among Varicella-Zoster Virus and identification of vaccine-specific sites. Virology 2016, 496, 277–286. [Google Scholar] [CrossRef]
- MMWR Recommendations and Reports; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2006; pp. 1–48. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5515a1.htm (accessed on 6 April 2021).
- Garcia Cenoz, M.; Castilla, J.; Chamorro, J.; Martinez-Baz, I.; Martinez-Artola, V.; Irisarri, F.; Arriazu, M.; Ezpeleta, C.; Barricarte, A. Impact of universal two-dose vaccination on varicella epidemiology in Navarre, Spain, 2006 to 2012. Eurosurveillance 2013, 18, 20552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozaki, T. Varicella vaccination in Japan: Necessity of implementing a routine vaccination program. J. Infect. Chemother. 2013, 19, 188–195. [Google Scholar] [CrossRef]
- Pozza, F.; Piovesan, C.; Russo, F.; Bella, A.; Pezzotti, P.; Emberti Gialloreti, L. Impact of universal vaccination on the epidemiology of varicella in Veneto, Italy. Vaccine 2011, 29, 9480–9487. [Google Scholar] [CrossRef] [PubMed]
- Siedler, A.; Arndt, U. Impact of the routine varicella vaccination programme on varicella epidemiology in Germany. Eurosurveillance 2010, 15, 19530. [Google Scholar] [CrossRef]
- NCIRS Fact Sheet: Varicella-Zoster (Chickenpox) Vaccines For Australian Children: Information For Immunisation Providers. 2015. Available online: https://www.ncirs.org.au/sites/default/files/2018-12/varicella-fact-sheet.pdf (accessed on 6 April 2021).
- Jung, J.; Ko, Y.J.; Kim, Y.E.; Huh, K.; Park, B.J.; Yoon, S.J. Epidemiological Impact of the Korean National Immunization Program on Varicella Incidence. J. Korean Med. Sci. 2019, 34, e53. [Google Scholar] [CrossRef]
- Lee, Y.H.; Choe, Y.J.; Cho, S.I.; Kang, C.R.; Bang, J.H.; Oh, M.D.; Lee, J.K. Effectiveness of Varicella Vaccination Program in Preventing Laboratory-Confirmed Cases in Children in Seoul, Korea. J. Korean Med. Sci. 2016, 31, 1897–1901. [Google Scholar] [CrossRef]
- Shapiro, E.D.; Vazquez, M.; Esposito, D.; Holabird, N.; Steinberg, S.P.; Dziura, J.; LaRussa, P.S.; Gershon, A.A. Effectiveness of 2 doses of varicella vaccine in children. J. Infect. Dis. 2011, 203, 312–315. [Google Scholar] [CrossRef] [Green Version]
- Chan, Y.D.; Edmunds, W.J.; Chan, H.L.; Wong, M.L.; Au, K.A.; Chuang, S.K.; van Hoek, A.J.; Flasche, S. Varicella vaccine dose depended effectiveness and waning among preschool children in Hong Kong. Hum. Vaccines Immunother. 2020, 16, 499–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Age (yr) | Vaccinated (n = 541) | Unvaccinated (n = 18) | ||
|---|---|---|---|---|
| Varicella Hx | Varicella Hx | |||
| − | + | − | + | |
| 2 | 60 | 6 | 0 | 0 |
| 3 | 119 | 11 | 0 | 3 |
| 4 | 122 | 31 | 0 | 5 |
| 5 | 95 | 47 | 3 | 4 |
| 6 | 36 | 14 | 2 | 1 |
| Subtotal (%) | 432 (79.9) | 109 (20.1) | 5 (27.8) | 13 (72.2) |
| Age (yr) | Total (n = 604) | |
|---|---|---|
| Male | Female | |
| 1 | 20 | 25 |
| 2 | 29 | 37 |
| 3 | 66 | 67 |
| 4 | 81 | 77 |
| 5 | 92 | 57 |
| 6 | 24 | 29 |
| Subtotal (%) | 312 (51.7) | 292 (48.3) |
| Measurements | Pre-Vaccination (n = 45) | Post-Vaccination (n = 45) |
|---|---|---|
| gpEIA GMT (mIU/mL) | 14.7 | 72.0 **** |
| gpEIA titer range (mIU/mL) | 4.4–53.4 | 10.7–359.1 |
| FAMA positive rate (%) | 0 | 91.1 |
| FAMA GMT | 1.3 | 41.6 **** |
| Subject No. | FAMA | gpEIA (mIU/mL) | ||
|---|---|---|---|---|
| Pre-Vaccination | Post-Vaccination | Pre-Vaccination | Post-Vaccination | |
| 28 | <2 | 4 | 6.42 | 16.96 |
| 34 | <2 | 2 | 8.70 | 10.65 |
| 37 | 4 | 8 | 53.43 | 59.53 |
| 42 | 2 | 8 | 9.53 | 29.62 |
| Age (yr) | Total (mIU/mL) * | Vaccinated (mIU/mL) | Unvaccinated (mIU/mL) | ||
|---|---|---|---|---|---|
| Varicella | Varicella | ||||
| − | + | − | + | ||
| 2 | 104.1 | 85.3 | 762.7 | NA | NA |
| 3 | 133.8 | 114.0 | 571.5 | NA | 378.2 |
| 4 | 223.5 | 133.0 | 1439.3 | NA | 682.2 |
| 5 | 365.1 | 167.1 | 1692.9 | 9.4 | 1987.2 |
| 6 | 352.9 | 220.4 | 2076.2 | 7.2 | 330.0 |
| Total | 215.1 | 131.4 | 1423.4 | 8.4 | 782.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Hwang, J.-Y.; Lee, K.-M.; Lee, E.; Park, H. Cross-Sectional Study of Varicella Zoster Virus Immunity in Healthy Korean Children Assessed by Glycoprotein Enzyme-Linked Immunosorbent Assay and Fluorescent Antibody to Membrane Antigen Test. Vaccines 2021, 9, 492. https://doi.org/10.3390/vaccines9050492
Kim Y, Hwang J-Y, Lee K-M, Lee E, Park H. Cross-Sectional Study of Varicella Zoster Virus Immunity in Healthy Korean Children Assessed by Glycoprotein Enzyme-Linked Immunosorbent Assay and Fluorescent Antibody to Membrane Antigen Test. Vaccines. 2021; 9(5):492. https://doi.org/10.3390/vaccines9050492
Chicago/Turabian StyleKim, Yunhwa, Ji-Young Hwang, Kyung-Min Lee, Eunsil Lee, and Hosun Park. 2021. "Cross-Sectional Study of Varicella Zoster Virus Immunity in Healthy Korean Children Assessed by Glycoprotein Enzyme-Linked Immunosorbent Assay and Fluorescent Antibody to Membrane Antigen Test" Vaccines 9, no. 5: 492. https://doi.org/10.3390/vaccines9050492