
The COVID-19 Vaccine Is Here—Now Who Is Willing to Get It?


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Recruitment
2.3. Materials
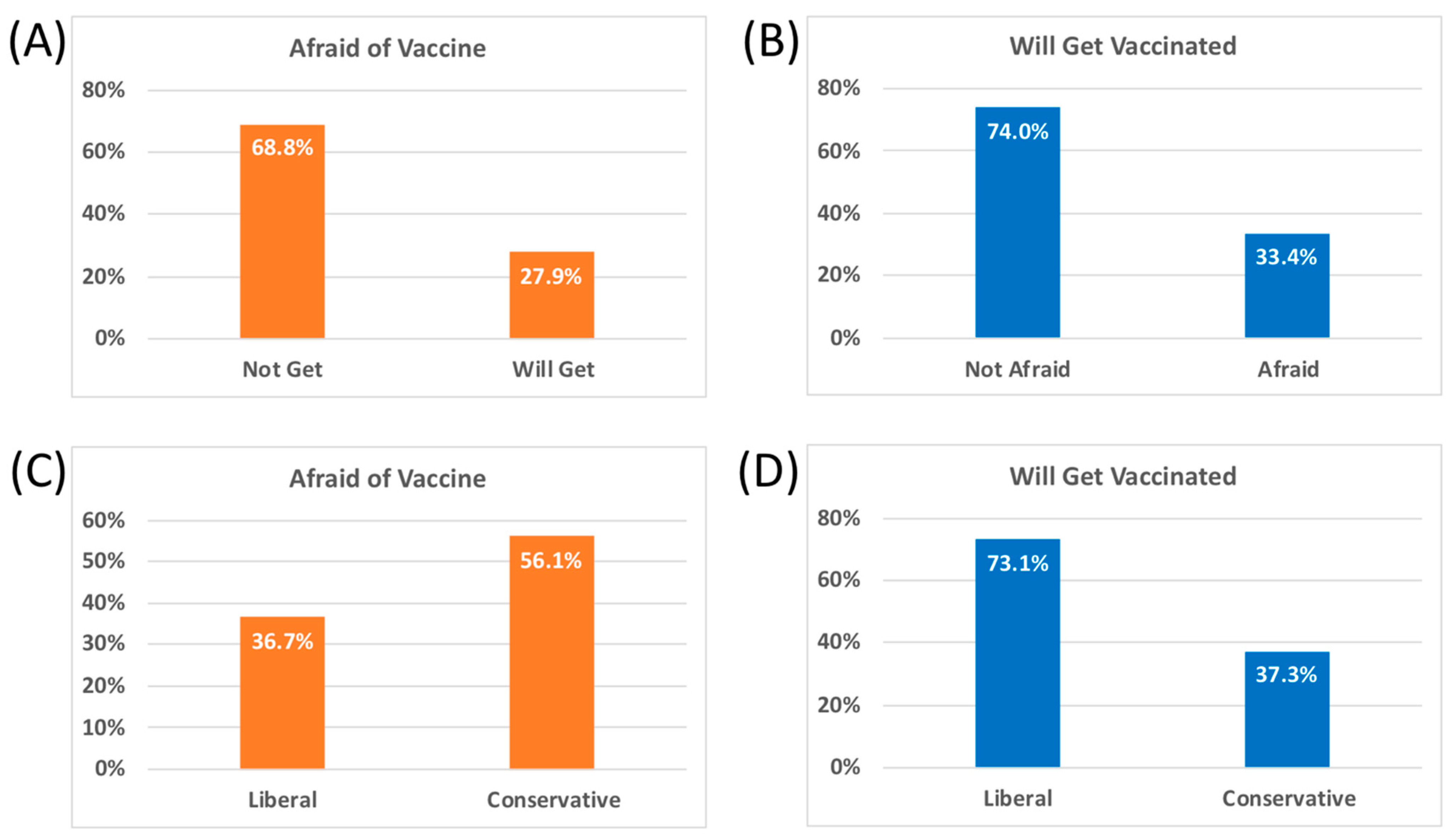
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bloom, B.R.; Nowak, G.J.; Orenstein, W. “When will we have a vaccine?”—Understanding questions and answers about Covid-19 vaccination. N. Engl. J. Med. 2020, 383, 2202–2204. [Google Scholar] [CrossRef]
- Vergara, R.J.D.; Sarmiento, P.J.D.; Lagman, J.D.N. Building public trust: A response to COVID-19 vaccine hesitancy predicament. J. Public Health 2021, fdaa282. [Google Scholar] [CrossRef] [PubMed]
- Bunch, L. A Tale of two crises: Addressing covid-19 vaccine hesitancy as promoting racial justice. HEC Forum 2021, 1–12. [Google Scholar] [CrossRef]
- Chou, W.-Y.S.; Budenz, A. Considering emotion in COVID-19 vaccine communication: Addressing vaccine hesitancy and fostering vaccine confidence. Health Commun. 2020, 35, 1718–1722. [Google Scholar] [CrossRef]
- Litman, L.; Robinson, J.; Abberbock, T. TurkPrime.com: A versatile crowdsourcing data acquisition platform for the behavioral sciences. Behav. Res. Methods 2016, 49, 433–442. [Google Scholar] [CrossRef] [Green Version]
- Robinson, J.; Rosenzweig, C.; Moss, A.J.; Litman, L. Tapped out or barely tapped? Recommendations for how to harness the vast and largely unused potential of the Mechanical Turk participant pool. PLoS ONE 2019, 14, e0226394. [Google Scholar] [CrossRef] [Green Version]
- Thomas, K.A.; Clifford, S. Validity and Mechanical Turk: An assessment of exclusion methods and interactive experiments. Comput. Hum. Behav. 2017, 77, 184–197. [Google Scholar] [CrossRef]
- Hauser, D.J.; Schwarz, N. Attentive Turkers: MTurk participants perform better on online attention checks than do subject pool participants. Behav. Res. Methods 2015, 48, 400–407. [Google Scholar] [CrossRef]
- Walters, K.; Christakis, D.A.; Wright, D.R. Are Mechanical Turk worker samples representative of health status and health behaviors in the U.S.? PLoS ONE 2018, 13, e0198835. [Google Scholar] [CrossRef] [Green Version]
- Mortensen, K.; Alcalá, M.G.; French, M.T.; Hu, T. Self-reported health status differs for Amazon’s Mechanical Turk respondents compared with nationally representative surveys. Med. Care 2018, 56, 211–215. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Prins, A.; Ouimette, P.; Kimerling, R.; Camerond, R.P.; Hugelshofer, D.S.; Shaw-Hegwer, J.; Thrailkill, A.; Gusman, F.D.; Sheikh, J.I. The primary care PTSD screen (PC–PTSD): Development and operating characteristics. Prim. Care Psychiatry 2004, 9, 9–14. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2020, 384, 403–416. [Google Scholar] [CrossRef]
- Attwell, K.; Lake, J.; Sneddon, J.; Gerrans, P.; Blyth, C.; Lee, J. Converting the maybes: Crucial for a successful COVID-19 vaccination strategy. PLoS ONE 2021, 16, e0245907. [Google Scholar] [CrossRef]
- Daly, M.; Robinson, E. Willingness to vaccinate against COVID-19 in the US: Longitudinal evidence from a nationally representative sample of adults from April–October 2020. medRxiv 2020. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and receptivity for COVID-19 vaccines: A rapid systematic review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef]
- Ruiz, J.B.; Bell, R.A. Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine 2021, 39, 1080–1086. [Google Scholar] [CrossRef]
- LeDoux, J.E.; Gorman, J.M. A call to action: Overcoming anxiety through active coping. Am. J. Psychiatry 2001, 158, 1953–1955. [Google Scholar] [CrossRef] [PubMed]
- Ruiter, R.A.C.; Kessels, L.T.E.; Peters, G.Y.; Kok, G. Sixty years of fear appeal research: Current state of the evidence. Int. J. Psychol. 2014, 49, 63–70. [Google Scholar] [CrossRef]
- Lyons, B.A.; Hasell, A.; Tallapragada, M.; Jamieson, K.H. Conversion messages and attitude change: Strong arguments, not costly signals. Public Underst. Sci. 2019, 28, 320–338. [Google Scholar] [CrossRef]
- Heffner, J.; Vives, M.-L.; FeldmanHall, O. Emotional responses to prosocial messages increase willingness to self-isolate during the COVID-19 pandemic. Pers. Individ. Dif. 2020, 170, 110420. [Google Scholar] [CrossRef]
- Albarracin, D.; Shavitt, S. Attitudes and attitude change. Annu. Rev. Psychol. 2018, 69, 299–327. [Google Scholar] [CrossRef] [PubMed]
- Momplaisir, F.; Haynes, N.; Nkwihoreze, H.; Nelson, M.; Werner, R.M.; Jemmott, J. Understanding Drivers of COVID-19 Vaccine Hesitancy Among Blacks. Clin. Infect. Dis. 2021, ciab102. [Google Scholar] [CrossRef] [PubMed]
- Lahijani, A.Y.; King, A.R.; Gullatte, M.M.; Hennink, M.; Bednarczyk, R.A. HPV Vaccine Promotion: The church as an agent of change. Soc. Sci. Med. 2021, 268, 113375. [Google Scholar] [CrossRef]
- Bajaj, S.S.; Stanford, F.C. Beyond tuskegee—Vaccine distrust and everyday racism. N. Engl. J. Med. 2021, 384, e12. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, K.; Hughes, T.L. Comparing Amazon’s Mechanical Turk platform to conventional data collection methods in the health and medical research literature. J. Gen. Intern. Med. 2018, 33, 533–538. [Google Scholar] [CrossRef] [Green Version]
- Bartneck, C.; Duenser, A.; Moltchanova, E.; Zawieska, K. Comparing the similarity of responses received from studies in amazon’s mechanical Turk to studies conducted online and with direct recruitment. PLoS ONE 2015, 10, e0121595. [Google Scholar] [CrossRef] [PubMed]
- Redmiles, E.M.; Kross, S.; Mazurek, M.L. How Well Do My Results Generalize? Comparing Security and Privacy Survey Results from MTurk, Web, and Telephone Samples. In Proceedings of the 2019 IEEE Symposium on Security and Privacy (SP), New York, NY, USA, 23 May 2019; pp. 1326–1343. [Google Scholar]
- Killgore, W.D.; Cloonan, S.A.; Taylor, E.C.; Dailey, N.S. Loneliness: A signature mental health concern in the era of COVID-19. Psychiatry Res. 2020, 290, 113117. [Google Scholar] [CrossRef]
- Killgore, W.D.; Cloonan, S.A.; Taylor, E.C.; Fernandez, F.; Grandner, M.A.; Dailey, N.S. Suicidal ideation during the COVID-19 pandemic: The role of insomnia. Psychiatry Res. 2020, 290, 113134. [Google Scholar] [CrossRef]
- Killgore, W.D.; Taylor, E.C.; Cloonan, S.A.; Dailey, N.S. Psychological resilience during the COVID-19 lockdown. Psychiatry Res. 2020, 291, 113216. [Google Scholar] [CrossRef]
- Killgore, W.D.; Cloonan, S.A.; Taylor, E.C.; Miller, M.A.; Dailey, N.S. Three months of loneliness during the COVID-19 lockdown. Psychiatry Res. 2020, 293, 113392. [Google Scholar] [CrossRef]
- Killgore, W.D.; Cloonan, S.A.; Taylor, E.C.; Allbright, M.C.; Dailey, N.S. Trends in suicidal ideation over the first three months of COVID-19 lockdowns. Psychiatry Res. 2020, 293, 113390. [Google Scholar] [CrossRef]
- Killgore, W.D.; Cloonan, S.A.; Taylor, E.C.; Lucas, D.A.; Dailey, N.S. Loneliness during the first half-year of COVID-19 Lockdowns. Psychiatry Res. 2020, 294, 113551. [Google Scholar] [CrossRef]
- Clifford, S.; Jewell, R.M.; Waggoner, P.D. Are samples drawn from Mechanical Turk valid for research on political ideology? Res. Politics 2015, 2, 1–9. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristic | Total Sample (N = 1017) |
|---|---|
| Age—years | 37.0 ± 12.2 |
| Female sex—number (%) | 594 (58.4) |
| Please Education—years | 15.1 ± 2.2 |
| Ethnicity—number (%) | |
| White | 770 (75.7) |
| Black/African American | 113 (11.1) |
| Hispanic/Latino | 47 (4.7) |
| Asian | 55 (5.4) |
| Native American/American Indian/Alaska Native | 7 (0.7) |
| Native Hawaiian/Pacific Islander | 3 (0.3) |
| Other | 22 (2.2) |
| Prefer not to answer | 0 (0.0) |
| Income—number (%) | |
| ≤USD 10,000 | 63 (6.2) |
| USD 10,001–USD 25,000 | 126 (12.4) |
| USD 25,001–USD 50,000 | 275 (27.0) |
| USD 50,001–USD 75,000 | 196 (19.3) |
| USD 75,001–USD 100,000 | 156 (15.3) |
| USD 100,001–USD 150,000 | 126 (12.4) |
| USD 150,001–USD 200,000 | 42 (4.1) |
| ≥USD 200,001 | 33 (3.2) |
| Political Ideology (1 = strongly liberal; 7 = strongly conservative) | 3.43 ± 1.90 |
| “Have you been formally diagnosed with COVID-19?” (yes)—number (%) | 60 (5.9) |
| “Are you considered to be in a “high-risk” group for COVID-19” (yes)—number (%) | 317 (31.2) |
| “I am gravely afraid of catching the COVID-19 virus” (1 = totally disagree; 7 = totally agree) | 4.27 ± 1.88 |
| “I’m afraid to get the new COVID-19 vaccine” (1 = totally disagree; 7 = totally agree) | 3.89 ± 1.96 |
| “I will get the new COVID-19 vaccine as soon as it is offered to me (1 = totally disagree; 7 = totally agree) | 4.49 ± 1.18 |
| GAD-7 (Generalized Anxiety Disorder scale-7) | 7.27 ± 6.03 |
| PHQ-9 (Patient Health Questionnaire-9) | 8.59 ± 6.70 |
| PC-PTSD (Primary Care Posttraumatic Stress Disorder) | 1.12 ± 1.48 |
| CD-RISC (Connor-Davidson Resilience Scale) | 64.25 ± 17.45 |
| Predictor Variables | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dependent Variable | Political Ideology (Conservative) | Sex (Female) | Annual Income | Race/Ethnicity (White) | GAD-7 Anxiety | PHQ-9 Depression | PHQ-9 PTSD | I Am Gravely Afraid of Catching the COVID-19 Virus | CD-RISC | Dx with COVID-19 (Yes) | High Risk for COVID-19 (Yes) | Age | Education |
| “I’m afraid to get the new COVID-19 vaccine” | 0.283 * | 0.218 * | −0.162 * | −0.07 | 0.113 * | 0.119 * | 0.098 * | −0.038 | 0.029 | 0.018 | 0.06 | −0.03 | −0.182 * |
| “I will get the new COVID-19 vaccine as soon as it is offered to me” | −0.448 * | −0.114 * | 0.10 * | 0.019 | 0.076 | 0.048 | 0.060 | 0.414 * | −0.136 * | 0.047 | 0.024 | 0.032 | 0.227 * |
| Vaccine Outcome Variable | R | Adjusted R2 | F | p-Value | Predictor Variables | β | t | p-Value | Partial r |
|---|---|---|---|---|---|---|---|---|---|
| “I’m afraid to get the new COVID-19 vaccine” | 0.434 | 0.184 | 39.08 | 7.62−43 | Political Ideology (conservative) | 0.317 | 10.836 | 5.83−26 | 0.323 |
| Sex (Female) | 0.197 | 6.785 | 1.97−11 | 0.209 | |||||
| Race/Ethnicity (White) | −0.121 | −4.226 | 0.0000 | −0.132 | |||||
| GAD-7 Generalized Anxiety | 0.112 | 3.769 | 0.0002 | 0.118 | |||||
| Annual Income | −0.105 | −3.389 | 0.0010 | −0.106 | |||||
| Education (years) | −0.087 | −2.84 | 0.0050 | −0.089 | |||||
| “I will get the new COVID-19 vaccine as soon as it is offered to me” | 0.596 | 0.349 | 61.52 | 1.04−89 | Political Ideology (conservative) | −0.343 | −12.028 | 3.11−31 | −0.354 |
| “I’m gravely afraid of catching the COVID-19 virus” (yes) | 0.308 | 10.985 | 1.36−26 | 0.327 | |||||
| Education (years) | 0.126 | 4.595 | 0.000005 | 0.143 | |||||
| Sex (Female) | −0.145 | −5.582 | 3.06−8 | −0.173 | |||||
| Annual Income | 0.102 | 3.69 | 0.0002 | 0.116 | |||||
| CD-RISC | −0.091 | −3.464 | 0.001 | −0.109 | |||||
| Age | 0.081 | 3.037 | 0.002 | 0.095 | |||||
| Race/Ethnicity (White) | 0.068 | 2.622 | 0.009 | 0.082 | |||||
| Dx with COVID-19 (yes) | 0.053 | 2.047 | 0.041 | 0.064 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Killgore, W.D.S.; Cloonan, S.A.; Taylor, E.C.; Dailey, N.S. The COVID-19 Vaccine Is Here—Now Who Is Willing to Get It? Vaccines 2021, 9, 339. https://doi.org/10.3390/vaccines9040339
Killgore WDS, Cloonan SA, Taylor EC, Dailey NS. The COVID-19 Vaccine Is Here—Now Who Is Willing to Get It? Vaccines. 2021; 9(4):339. https://doi.org/10.3390/vaccines9040339
Chicago/Turabian StyleKillgore, William D. S., Sara A. Cloonan, Emily C. Taylor, and Natalie S. Dailey. 2021. "The COVID-19 Vaccine Is Here—Now Who Is Willing to Get It?" Vaccines 9, no. 4: 339. https://doi.org/10.3390/vaccines9040339