
Does Influenza Vaccination during Pregnancy Have Effects on Non-Influenza Infectious Morbidity? A Systematic Review and Meta-Analysis of Randomised Controlled Trials

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
- –
- RCTs assessing the effect of an IIV vs. either placebo or another non-influenza vaccine administered during pregnancy;
- –
- RCTs that contained information about one or more of the following outcomes: miscarriage, stillbirth, maternal death, infant death, maternal non-influenza infectious adverse events, and child non-influenza infectious adverse events.
2.3. Data Extraction
- (1)
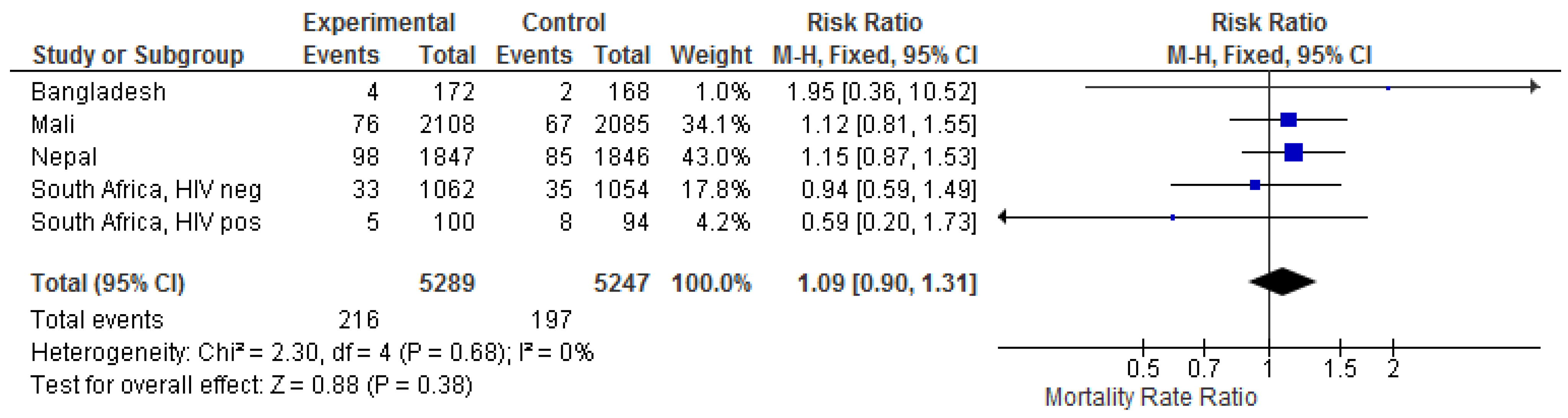
- Maternal all-cause mortality (excluding accidents and suicide). One trial reported no maternal deaths [24]. From the other trials, deaths were either presented in the text [25,26] or in the appendix [21,27]. We excluded one death due to suicide [25] as well as two deaths due to electrocution and ‘cervical fracture, post-trauma’ [26].
- (2)
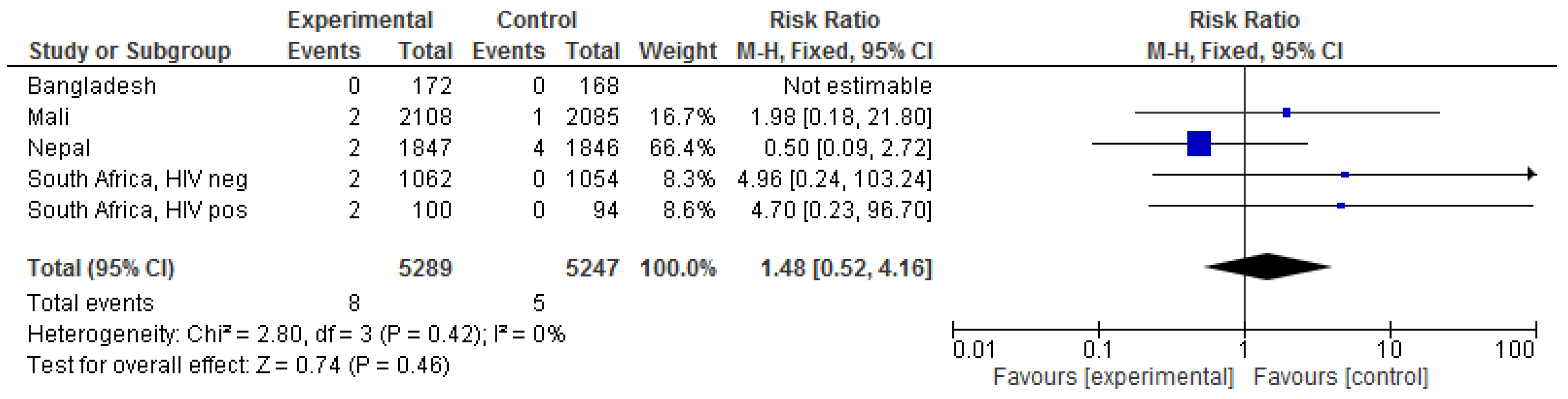
- Maternal mortality from presumed infectious causes. Causes of death were either presented in the text [25,26] or in the appendix [27]. We excluded deaths related to haemorrhage, cancers, cardiovascular events, and TB (presumably acquired prior to trial vaccination) but included death due to infection after caesarean section [27].
- (3)
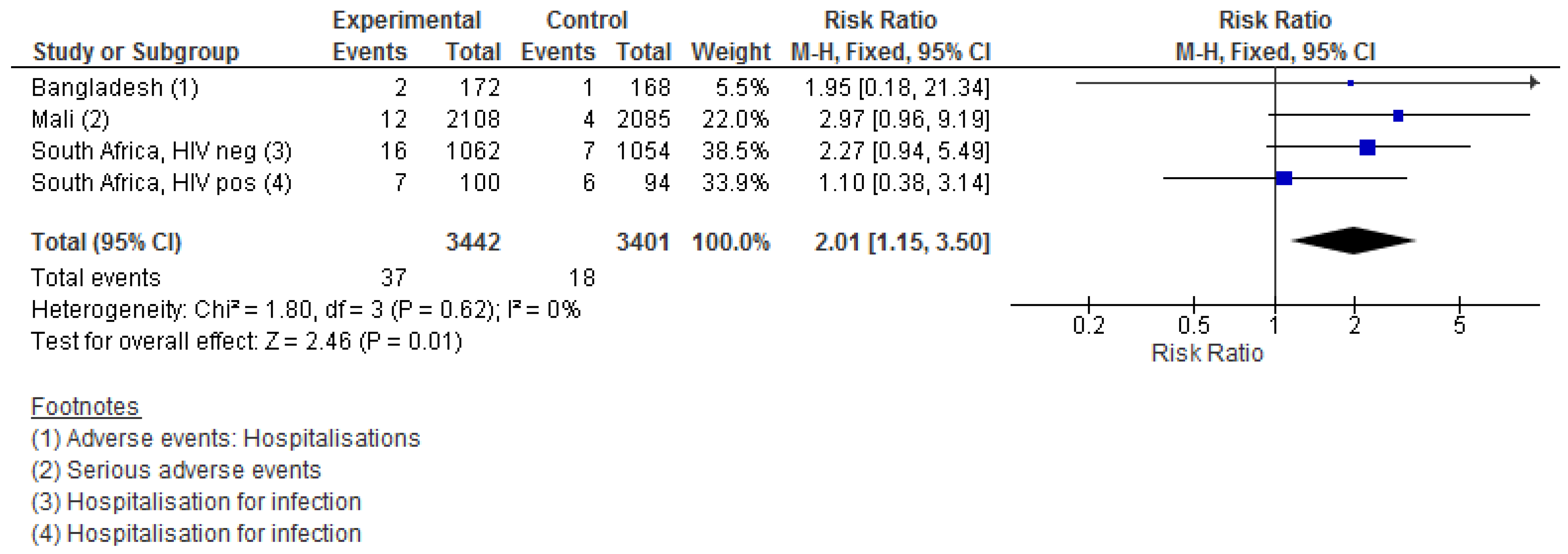
- Maternal non-influenza infectious adverse events. This outcome was recorded as hospital admission in the South African trial [27], as serious adverse events in the Bangladesh and Mali trials [24,26]; the Nepal trial did not report this outcome [25]. We did not include TB and HIV, as we assumed that these were acquired before enrolment. Both the South African and Mali trials reported categories of non-mutually exclusive outcomes, so one individual could account for several outcomes, but based on the reported data from South Africa, the number of outcomes was not much larger than the number of individuals (316 all-cause hospitalisations in 304 women; 313 all-cause hospitalisations in 289 infants).
- (4)
- (5)
- (6)
- (7)
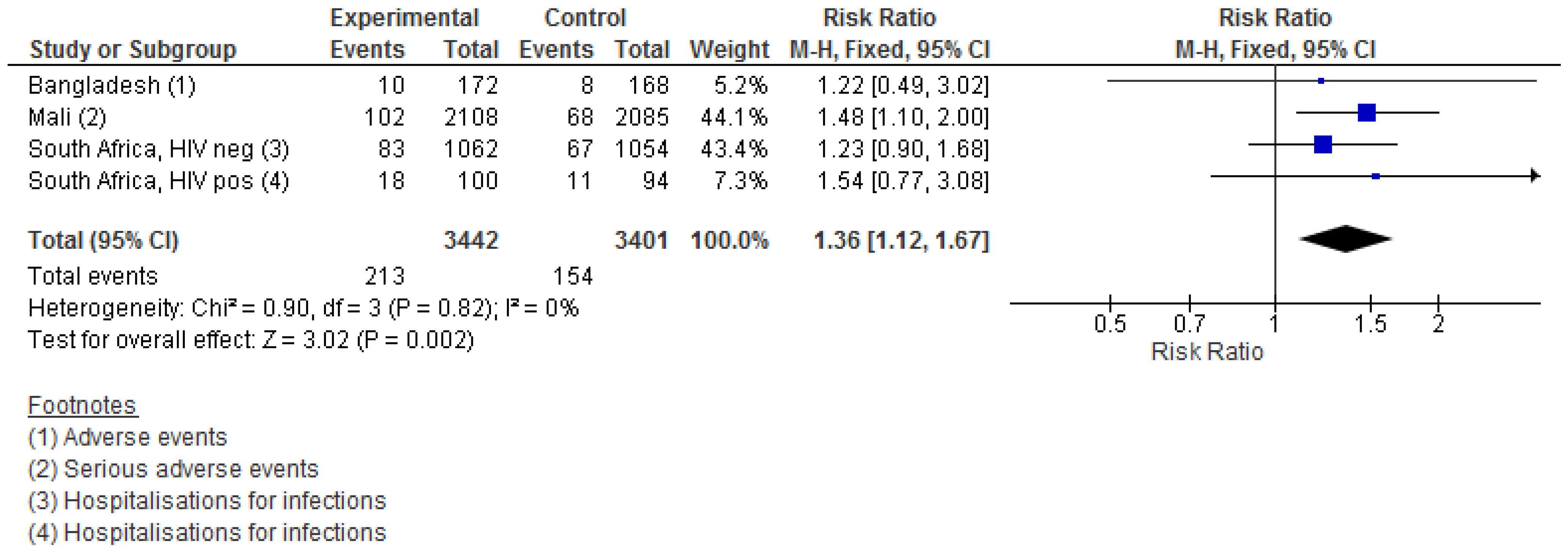
- Infant non-influenza infectious adverse events. The outcome was extracted from the tables [27] and appendices [24,26]. Both South African and Mali trials reported categories of non-mutually exclusive outcomes, but the number of individuals with several events was limited. We excluded ‘neonatal sepsis, within 3 days of birth’, which we interpreted as included in ‘neonatal sepsis, within 28 days of birth’; otherwise, we counted each event as one event.
2.4. Statistical Analyses
3. Results
3.1. Maternal Outcomes
3.2. Child Outcomes
4. Discussion
4.1. Strengths and Weaknesses
4.2. Interpretation
4.3. Immunological Mechanisms
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neuzil, K.M.; Mellen, B.G.; Wright, P.F.; Mitchel, E.F.; Griffin, M.R., Jr. The effect of influenza on hospitalizations, outpatient visits, and courses of antibiotics in children. N. Engl. J. Med. 2000, 342, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Edwards, K.M. Maternal antibodies and infant immune responses to vaccines. Vaccine 2015, 33, 6469–6472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Vaccines against influenza WHO position paper-November 2012. Wkly. Epidemiol. Rec. Relev. Épidémiologique Hebd. 2012, 87, 461–476. [Google Scholar]
- Nunes, M.C.; Madhi, S.A. Influenza vaccination during pregnancy for prevention of influenza confirmed illness in the infants: A systematic review and meta-analysis. Hum. Vaccines Immunother. 2018, 14, 758–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunes, M.C.; Aqil, A.R.; Omer, S.B.; Madhi, S.A. The Effects of Influenza Vaccination during Pregnancy on Birth Outcomes: A Systematic Review and Meta-Analysis. Am. J. Perinatol. 2016, 33, 1104–1114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bratton, K.N.; Wardle, M.T.; Orenstein, W.A.; Omer, S.B. Maternal influenza immunization and birth outcomes of stillbirth and spontaneous abortion: A systematic review and meta-analysis. Clin. Infect. Dis. 2015, 60, e11–e19. [Google Scholar] [CrossRef]
- McMillan, M.; Porritt, K.; Kralik, D.; Costi, L.; Marshall, H. Influenza vaccination during pregnancy: A systematic review of fetal death, spontaneous abortion, and congenital malformation safety outcomes. Vaccine 2015, 33, 2108–2117. [Google Scholar] [CrossRef] [PubMed]
- Omer, S.B.; Clark, D.R.; Madhi, S.A.; Tapia, M.D.; Nunes, M.C.; Cutland, C.L.; Simoes, E.A.F.; Aqil, A.R.; Kata, J.; Tielsch, J.M.; et al. Efficacy, duration of protection, birth outcomes, and infant growth associated with influenza vaccination in pregnancy: A pooled analysis of three randomised controlled trials. Lancet Respir. Med. 2020, 8, 597–608. [Google Scholar] [CrossRef]
- Benn, C.S.; Netea, M.G.; Selin, L.K.; Aaby, P. A small jab-a big effect: Nonspecific immunomodulation by vaccines. Trends Immunol. 2013, 34, 431–439. [Google Scholar] [CrossRef]
- Pollard, A.J.; Bijker, E.M. A guide to vaccinology: From basic principles to new developments. Nat. Rev. Immunol. 2021, 21, 83–100. [Google Scholar] [CrossRef]
- WHO. Meeting of the Strategic advisory group of experts on immunization, april 2014–conclusions and recommendations. Wkly. Epidemiol. Rec. 2014, 89, 221–236. [Google Scholar]
- Higgins, J.P.; Soares-Weiser, K.; Lopez-Lopez, J.A.; Kakourou, A.; Chaplin, K.; Christensen, H.; Martin, N.K.; Sterne, J.A.C.; Reingold, A.L. Association of BCG, DTP, and measles containing vaccines with childhood mortality: Systematic review. BMJ 2016, 355, i5170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benn, C.S.; Fisker, A.B.; Rieckmann, A.; Sørup, S.; Aaby, P. Vaccinology: Time to change the paradigm? Lancet Infect. Dis. 2020, 20, e274–e283. [Google Scholar] [CrossRef]
- Aaby, P.; Ravn, H.; Fisker, A.B.; Rodrigues, A.; Benn, C.S. Is diphtheria-tetanus-pertussis (DTP) associated with increased female mortality? A meta-analysis testing the hypotheses of sex-differential non-specific effects of DTP vaccine. Trans. R. Soc. Trop. Med. Hyg. 2016, 110, 570–581. [Google Scholar]
- Garly, M.L.; Jensen, H.; Martins, C.L.; Balé, C.; Baldé, M.A.; Lisse, I.M.; Aaby, P. Hepatitis B vaccination associated with higher female than male mortality in Guinea-bissau: An observational study. Pediatric Infect. Dis. J. 2004, 23, 1086–1092. [Google Scholar]
- Aaby, P.; Garly, M.L.; Nielsen, J.; Ravn, H.; Martins, C.; Balé, C.; Rodrigues, A.; Benn, C.S.; Lisse, I.M. Increased female-male mortality ratio associated with inactivated polio and diphtheria-tetanus-pertussis vaccines: Observations from vaccination trials in Guinea-Bissau. Pediatric Infect. Dis. J. 2007, 26, 247–252. [Google Scholar] [CrossRef]
- Fisker, A.B.; Biering-Sorensen, S.; Lund, N.; Djana, Q.; Rodrigues, A.; Martins, C.L.; Benn, C.S. Contrasting female-male mortality ratios after routine vaccinations with pentavalent vaccine versus measles and yellow fever vaccine. A cohort study from urban Guinea-Bissau. Vaccine 2016, 34, 4551–4557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cowling, B.J.; Fang, V.J.; Nishiura, H.; Chan, K.-H.; Ng, S.; Ip, D.K.M.; Chiu, S.S.S.; Leung, G.; Peiris, J.S.M. Increased Risk of Noninfluenza Respiratory Virus Infections Associated with Receipt of Inactivated Influenza Vaccine. Clin. Infect. Dis. 2012, 54, 1778–1783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, A.; Fisker, A.; Rodrigues, A.; Martins, C.; Ravn, H.; Lund, N.; Biering-Sørensen, S.; Benn, C.S.; Aaby, P. National Immunization Campaigns with Oral Polio Vaccine Reduce All-Cause Mortality: A Natural Experiment within Seven Randomized Trials. Front. Public Health 2018, 6, 13. [Google Scholar] [CrossRef]
- Hansen, O.B.; Rodrigues, A.; Martins, C.; Rieckmann, A.; Benn, C.S.; Aaby, P.; Fisker, A.B. Impact of H1N1 Influenza Vaccination on Child Morbidity in Guinea-Bissau. J. Trop. Pediatr. 2018, 65, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Andersen, A.; Fisker, A.B.; Nielsen, S.; Rodrigues, A.; Benn, C.S.; Aaby, P. National Immunization Campaigns with Oral Polio Vaccine May Reduce All-cause Mortality: An Analysis of 13 Years of Demographic Surveillance Data from an Urban African Area. Clin. Infect. Dis. 2021, 72, e596–e603. [Google Scholar] [CrossRef] [PubMed]
- Donzelli, A. Influenza vaccination for all pregnant women? So far the less biased evidence does not favour it. Hum. Vaccines Immunother. 2019, 15, 2159–2164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, D.R.; Omer, S.B.; Tapia, M.D.; Nunes, M.C.; Cutland, C.L.; Tielsch, J.M.; Wairagkar, N.; Madhi, S.A. Influenza or Meningococcal Immunization During Pregnancy and Mortality in Women and Infants: A Pooled Analysis of Randomized Controlled Trials. Pediatric Infect. Dis. J. 2020, 39, 641. [Google Scholar] [CrossRef]
- Zaman, K.; Roy, E.; Arifeen, S.E.; Rahman, M.; Raqib, R.; Wilson, E.; Omer, S.B.; Shahid, N.S.; Breiman, R.F.; Steinhoff, M.C. Effectiveness of Maternal Influenza Immunization in Mothers and Infants. N. Engl. J. Med. 2008, 359, 1555–1564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinhoff, M.C.; Katz, J.; Englund, J.A.; Khatry, S.K.; Shrestha, L.; Kuypers, J.; Stewart, L.; Mullany, L.C.; Chu, H.Y.; LeClerq, S.C.; et al. Year-round influenza immunisation during pregnancy in Nepal: A phase 4, randomised, placebo-controlled trial. Lancet Infect. Dis. 2017, 17, 981–989. [Google Scholar] [CrossRef] [Green Version]
- Tapia, M.D.; Sow, S.O.; Tamboura, B.; Tégueté, I.; Pasetti, M.F.; Kodio, M.; Onwuchekwa, U.; Tennant, S.M.; Blackwelder, W.C.; Coulibaly, F.; et al. Maternal immunisation with trivalent inactivated influenza vaccine for prevention of influenza in infants in Mali: A prospective, active-controlled, observer-blind, randomised phase 4 trial. Lancet Infect. Dis. 2016, 16, 1026–1035. [Google Scholar] [CrossRef] [Green Version]
- Madhi, S.A.; Cutland, C.L.; Kuwanda, L.; Weinberg, A.; Hugo, A.; Jones, S.; Adrian, P.V.; Van Niekerk, N.; Treurnicht, F.; Ortiz, J.R.; et al. Influenza Vaccination of Pregnant Women and Protection of Their Infants. N. Engl. J. Med. 2014, 371, 918–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byberg, S.; Benn, C.S. Placebo use in vaccine trials: Caution when using active vaccines as placebo. Vaccine 2017, 35, 1211. [Google Scholar] [CrossRef]
- Cutts, F.; Zaman, S.; Enwere, G.; Jaffar, S.; Levine, O.; Okoko, J.; Oluwalana, C.; Vaughan, A.; Obaro, S.; Leach, A.; et al. Efficacy of nine-valent pneumococcal conjugate vaccine against pneumonia and invasive pneumococcal disease in The Gambia: Randomised, double-blind, placebo-controlled trial. Lancet 2005, 365, 1139–1146. [Google Scholar] [CrossRef]
- Krammer, F.; Smith, G.J.D.; Fouchier, R.A.M.; Peiris, M.; Kedzierska, K.; Doherty, P.C.; Palese, P.; Shaw, M.L.; Treanor, J.; Webster, R.G.; et al. Influenza. Nat. Rev. Dis Primers 2018, 4, 3. [Google Scholar] [CrossRef] [PubMed]
- Beumer, M.; Koch, R.; van Beuningen, D.; OudeLashof, A.; van de Veerdonk, F.; Kolwijck, E.; van der Hoeven, J.; Bergmans, D.; Hoedemaekers, C. Influenza virus and factors that are associated with ICU admission, pulmonary co-infections and ICU mortality. J. Crit. Care 2019, 50, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Nunes, M.C.; Cutland, C.L.; Jones, S.; Downs, S.; Weinberg, A.; Ortiz, J.R.; Neuzil, K.M.; Simões, E.A.F.; Klugman, K.P.; Madhi, S.A. Efficacy of Maternal Influenza Vaccination Against All-Cause Lower Respiratory Tract Infection Hospitalizations in Young Infants: Results from a Randomized Controlled Trial. Clin. Infect. Dis. 2017, 65, 1066–1071. [Google Scholar] [CrossRef]
- Omer, S.B.; Clark, D.R.; Aqil, A.R.; Tapia, M.D.; Nunes, M.C.; Kozuki, N.; Steinhoff, M.C.; Madhi, S.A.; Wairagkar, N. Maternal Influenza Immunization and Prevention of Severe Clinical Pneumonia in Young Infants: Analysis of Randomized Controlled Trials Conducted in Nepal, Mali and South Africa. Pediatric Infect. Dis. J. 2018, 37, 436–440. [Google Scholar] [CrossRef]
- Steinhoff, M.C.; Omer, S.B.; Roy, E.; El Arifeen, S.; Raqib, R.; Dodd, C.; Breiman, R.F.; Zaman, K. Neonatal outcomes after influenza immunization during pregnancy: A randomized controlled trial. Can. Med. Assoc. J. 2012, 184, 645–653. [Google Scholar] [CrossRef] [Green Version]
- Klein, S.L.; Shann, F.; Moss, W.J.; Benn, C.S.; Aaby, P. RTS,S Malaria Vaccine and Increased Mortality in Girls. MBio 2016, 7, e00514–e00516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aaby, P.; Rodrigues, A.; Kofoed, P.E.; Benn, C.S. RTS,S/AS01 malaria vaccine and child mortality. Lancet 2015, 386, 1735–1736. [Google Scholar] [CrossRef] [Green Version]
- Kleinnijenhuis, J.; Quintin, J.; Preijers, F.; Joosten, L.A.B.; Ifrim, D.C.; Saeed, S.; Jacobs, C.; van Loenhout, J.; de Jong, D.; Stunnenberg, H.G.; et al. Bacille Calmette-Guerin induces NOD2-dependent nonspecific protection from reinfection via epigenetic reprogramming of monocytes. Proc. Natl. Acad. Sci. USA 2012, 109, 17537–17542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blok, B.A.; de Bree, L.C.J.; Diavatopoulos, D.A.; Langereis, J.D.; Joosten, L.A.B.; Aaby, P.; van Crevel, R.; Benn, C.S.; Netea, M.G. Interacting non-specific immunological effects of BCG and Tdap vaccinations: An explorative randomized trial. Clin. Infect. Dis. 2019, 70, 455–463. [Google Scholar]
- Blok, B.A.; Jensen, K.J.; Aaby, P.; Fomsgaard, A.; Van Crevel, R.; Benn, C.S.; Netea, M.G. Opposite effects of Vaccinia and modified Vaccinia Ankara on trained immunity. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Leentjens, J.; Kox, M.; Stokman, R.; Gerretsen, J.; Diavatopoulos, D.A.; van Crevel, R.; Rimmelzwaan, G.F.; Pickkers, P.; Netea, M.G. BCG Vaccination Enhances the Immunogenicity of Subsequent Influenza Vaccination in Healthy Volunteers: A Randomized, Placebo-Controlled Pilot Study. J. Infect. Dis. 2015, 212, 1930–1938. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Author, Year | Number of Pregnant Women | Influenza Vaccine, Type | Control Group Treatment | Time of Randomisation and Vaccination | Follow-Up | VE against Laboratory-Confirmed Influenza in Women | VE against Laboratory-Confirmed Influenza in Infants | Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|
| Bangladesh | Zaman et al. 2008 [24] | 340 | 3-valent IIV | 23-valent pneumococcal polysaccharide vaccine | 3rd trimester | 24 weeks of age | N/A | 63% (5–85%) | Low: Randomisation, allocation concealment, intention-to-treat analysis, observer blinding. |
| South Africa | Madhi et al. 2014 [27] | HIV neg: 2116HIV pos: 194 | 3-valent IIV | Saline | 2nd + 3rd trimester (weeks 20–36) | 24 weeks of age | HIV neg: 50% (15–71%) HIV pos: 58% (0–82%) | HIV neg: 49% (12–70%) HIV pos: 27%; p = 0.60 | Low: Randomisation, allocation concealment, intention-to-treat analysis, observer blinding. |
| Mali | Tapia et al. 2016 [26] | 4193 | 3-valent IIV | 4-valent meningococcal vaccine | 3rd trimester (≥28 weeks) | 6 months of age | 70% (42–86%) | 33% (4–54%) | Low: Randomisation, allocation concealment, intention-to-treat analysis, observer blinding. |
| Nepal | Steinhoff et al. 2017 [25] | 3693 | 3-valent IIV | Saline | 2nd + 3rd trimester (weeks 17–34) | 6 months of age | 31% (−10–56%) | 30% (5–48%) | Low: Randomisation, allocation concealment, intention-to-treat analysis, observer blinding. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hansen, K.P.; Benn, C.S.; Aamand, T.; Buus, M.; da Silva, I.; Aaby, P.; Fisker, A.B.; Thysen, S.M. Does Influenza Vaccination during Pregnancy Have Effects on Non-Influenza Infectious Morbidity? A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Vaccines 2021, 9, 1452. https://doi.org/10.3390/vaccines9121452
Hansen KP, Benn CS, Aamand T, Buus M, da Silva I, Aaby P, Fisker AB, Thysen SM. Does Influenza Vaccination during Pregnancy Have Effects on Non-Influenza Infectious Morbidity? A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Vaccines. 2021; 9(12):1452. https://doi.org/10.3390/vaccines9121452
Chicago/Turabian StyleHansen, Katrine Pedersbæk, Christine Stabell Benn, Thomas Aamand, Martin Buus, Isaquel da Silva, Peter Aaby, Ane Bærent Fisker, and Sanne Marie Thysen. 2021. "Does Influenza Vaccination during Pregnancy Have Effects on Non-Influenza Infectious Morbidity? A Systematic Review and Meta-Analysis of Randomised Controlled Trials" Vaccines 9, no. 12: 1452. https://doi.org/10.3390/vaccines9121452