
COVID-19 Vaccine Booster Hesitancy (VBH) of Healthcare Workers in Czechia: National Cross-Sectional Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Instrument
2.4. Ethics
2.5. Statistics
3. Results
3.1. Demographic Characteristics
3.2. COVID-19-Related Anamnesis
3.3. COVID-19 Vaccine-Related Anamnesis
3.4. COVID-19 Vaccine BD-Related Attitudes
3.5. Psychosocial Drivers of BD-Related Attitudes
3.6. Determinants of BD-Related Attitudes
3.7. Analysis of COVID-19 Vaccine BD Hesitancy vs. Acceptance
4. Discussion
4.1. Strengths
4.2. Limitations
4.3. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention (CDC) COVID-19 Vaccine Booster Shots. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/booster-shot.html (accessed on 16 November 2021).
- Ministerstvo Zdravotnictví (MZCR) Posilovací a Dodatečná Dávka (Booster and Extra Doses). Available online: https://covid.gov.cz/situace/registrace-na-ockovani/posilovaci-dodatecna-davka (accessed on 16 November 2021).
- Atwell, J.E.; Salmon, D.A. Pertussis Resurgence and Vaccine Uptake: Implications for Reducing Vaccine Hesitancy. Pediatrics 2014, 134, 602–604. [Google Scholar] [CrossRef] [Green Version]
- Dasgupta, P.; Bhattacherjee, S.; Mukherjee, A.; Dasgupta, S. Vaccine hesitancy for childhood vaccinations in slum areas of Siliguri, India. Indian J. Public Health 2018, 62, 253. [Google Scholar] [CrossRef]
- Facciola, A.; Visalli, G.; Orlando, A.; Bertuccio, M.P.; Spataro, P.; Squeri, R.; Picerno, I.; Di Pietro, A. Vaccine hesitancy: An overview on parents’ opinions about vaccination and possible reasons of vaccine refusal. J. Public Health Res. 2019, 8, 13–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Azman, A.S.; Lu, W.; Sun, R.; Zheng, N.; Ge, S.; Deng, X.; Yang, J.; Leung, D.T.; Yu, H. Prediction of vaccine efficacy of the Delta variant. medRxiv 2021. [Google Scholar] [CrossRef]
- Lange, B.; Gerigk, M.; Tenenbaum, T. Breakthrough Infections in BNT162b2-Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1145–1146. [Google Scholar] [CrossRef]
- Mizrahi, B.; Lotan, R.; Kalkstein, N.; Peretz, A.; Perez, G.; Ma, M.N.; Ben-Tov, A.; Chodick, G.; Gazit, S.; Patalon, T. Correlation of SARS-CoV-2 Breakthrough Infections to Time-from-vaccine; Preliminary Study. medRxiv 2021. [Google Scholar] [CrossRef]
- Nasreen, S.; Chung, H.; He, S.; Brown, K.A.; Gubbay, J.B.; Buchan, S.A.; Fell, D.B.; Austin, P.C.; Schwartz, K.L.; Sundaram, M.E.; et al. Effectiveness of COVID-19 vaccines against variants of concern in Ontario, Canada. medRxiv 2021. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning immunity of the BNT162b2 vaccine: A nationwide study from Israel. medRxiv 2021. [Google Scholar] [CrossRef]
- Wall, E.C.; Wu, M.; Harvey, R.; Kelly, G.; Warchal, S.; Sawyer, C.; Daniels, R.; Hobson, P.; Hatipoglu, E.; Ngai, Y.; et al. Neutralising antibody activity against SARS-CoV-2 VOCs B.1.617.2 and B.1.351 by BNT162b2 vaccination. Lancet 2021, 397, 2331–2333. [Google Scholar] [CrossRef]
- Coronavirus (COVID-19) Update: FDA Authorizes Additional Vaccine Dose for Certain Immunocompromised Individuals | FDA. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-additional-vaccine-dose-certain-immunocompromised (accessed on 16 November 2021).
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, risk of hospital admission, and vaccine effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S.; et al. Six-Month Effectiveness of BNT162B2 mRNA COVID-19 Vaccine in a Large US Integrated Health System: A Retrospective Cohort Study. SSRN Electron. J. 2021. [Google Scholar] [CrossRef]
- Tang, P.; Hasan, M.R.; Chemaitelly, H.; Yassine, H.M.; Benslimane, F.M.; Khatib, H.A.A.; AlMukdad, S.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. BNT162b2 and mRNA-1273 COVID-19 vaccine effectiveness against the Delta (B.1.617.2) variant in Qatar. medRxiv 2021. [Google Scholar] [CrossRef]
- Bernal, J.L.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 vaccines against the B.1.617.2 variant. medRxiv 2021. [Google Scholar] [CrossRef]
- Fowlkes, A.; Gaglani, M.; Groover, K.; Thiese, M.S.; Tyner, H.; Ellingson, K. Effectiveness of COVID-19 Vaccines in Preventing SARS-CoV-2 Infection Among Frontline Workers Before and During B.1.617.2 (Delta) Variant Predominance—Eight U.S. Locations, December 2020-August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1167–1169. [Google Scholar] [CrossRef] [PubMed]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. BNT162b2 vaccine booster dose protection: A nationwide study from Israel. medRxiv 2021. [Google Scholar] [CrossRef]
- Silva-Cayetano, A.; Foster, W.S.; Innocentin, S.; Belij-Rammerstorfer, S.; Spencer, A.J.; Burton, O.T.; Fra-Bidó, S.; Le Lee, J.; Thakur, N.; Conceicao, C.; et al. A booster dose enhances immunogenicity of the COVID-19 vaccine candidate ChAdOx1 nCoV-19 in aged mice. Med 2021, 2, 243–262.e8. [Google Scholar] [CrossRef]
- Williams, J.L.; Christensen, C.J.; McMahon, B.J.; Bulkow, L.R.; Cagle, H.H.; Mayers, J.S.; Zanis, C.L.; Parkinson, A.J.; Margolis, H.S. Evaluation of the response to a booster dose of hepatitis B vaccine in previously immunized healthcare workers. Vaccine 2001, 19, 4081–4085. [Google Scholar] [CrossRef]
- Jayasundara, D.; Sheridan, S.; Randall, D.; Campbell, P.; Edmond, K.; Liu, B.; McIntyre, P.B.; Gidding, H.F.; Wood, J.G. 472Long-term effectiveness of 3-dose primary course and 4-year booster dose of pertussis vaccine in Australia. Int. J. Epidemiol. 2021, 50. [Google Scholar] [CrossRef]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Rzymski, P.; Poniedziałek, B.; Fal, A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines 2021, 9, 1286. [Google Scholar] [CrossRef] [PubMed]
- Klugar, M.; Riad, A.; Mekhemar, M.; Conrad, J.; Buchbender, M.; Howaldt, H.-P.; Attia, S. Side Effects of mRNA-Based and Viral Vector-Based COVID-19 Vaccines among German Healthcare Workers. Biology 2021, 10, 752. [Google Scholar] [CrossRef] [PubMed]
- Surgo Ventures. Six Ways to Better Understand COVID-19 Vaccine Hesitancy. Available online: https://surgoventures.medium.com/six-ways-to-better-understand-covid-19-vaccine-hesitancy-3689dfd65b86 (accessed on 17 November 2021).
- Berg, S. Which COVID-19 Vaccine Should I Get? What to Tell Your Patients. Available online: https://www.ama-assn.org/delivering-care/public-health/which-covid-19-vaccine-should-i-get-what-tell-your-patients (accessed on 17 November 2021).
- World Economic Forum (WEF). Would You Get a COVID-19 Booster Shot if Offered? Available online: https://www.weforum.org/agenda/2021/09/covid-19-booster-shot-if-offered/ (accessed on 16 November 2021).
- Díaz Crescitelli, M.E.; Ghirotto, L.; Sisson, H.; Sarli, L.; Artioli, G.; Bassi, M.C.; Appicciutoli, G.; Hayter, M. A Meta-Synthesis Study of the Key Elements Involved in Childhood Vaccine Hesitancy; Public Health: London, UK, 2020; Volume 180, pp. 38–45. [Google Scholar]
- Butler, R.; MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; et al. Diagnosing the determinants of vaccine hesitancy in specific subgroups: The Guide to Tailoring Immunization Programmes (TIP). Vaccine 2015, 33, 4176–4179. [Google Scholar] [CrossRef] [PubMed]
- Strategic Advisory Group of Experts on Immunization (SAGE). Report of the Sage Working Group on Vaccine Hesitancy; SAGE: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Lane, S.; MacDonald, N.E.; Marti, M.; Dumolard, L. Vaccine hesitancy around the globe: Analysis of three years of WHO/UNICEF Joint Reporting Form data-2015–2017. Vaccine 2018, 36, 3861–3867. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Vaccine Adverse Event Reporting System (VAERS). Available online: https://vaers.hhs.gov/ (accessed on 17 November 2021).
- Government of Canada (Canada.ca). Canadian Adverse Events Following Immunization Surveillance System (CAEFISS). Available online: https://www.canada.ca/en/public-health/services/immunization/canadian-adverse-events-following-immunization-surveillance-system-caefiss.html (accessed on 17 November 2021).
- Medicines and Healthcare Products Regulatory Agency (MHRA). Coronavirus (COVID-19) Vaccines Adverse Reactions. Available online: https://www.gov.uk/government/publications/coronavirus-covid-19-vaccine-adverse-reactions (accessed on 17 November 2021).
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- Jęśkowiak, I.; Wiatrak, B.; Grosman-Dziewiszek, P.; Szeląg, A. The Incidence and Severity of Post-Vaccination Reactions after Vaccination against COVID-19. Vaccines 2021, 9, 502. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Schünemann, H.; Attia, S.; Peričić, T.P.; Žuljević, M.F.; Jürisson, M.; Kalda, R.; Lang, K.; Morankar, S.; Yesuf, E.A.; et al. COVID-19 Vaccines Safety Tracking (CoVaST): Protocol of a Multi-Center Prospective Cohort Study for Active Surveillance of COVID-19 Vaccines’ Side Effects. Int. J. Environ. Res. Public Health 2021, 18, 7859. [Google Scholar] [CrossRef]
- Klugar, M.; Riad, A. COVID-19 Vaccines Safety Tracking (CoVaST). Available online: https://clinicaltrials.gov/ct2/show/NCT04834869 (accessed on 15 July 2021).
- Berg, S. What Doctors Wish Patients Knew about COVID-19 Caccine Boosters. 2021. Available online: https://www.ama-assn.org/delivering-care/public-health/what-doctors-wish-patients-knew-about-covid-19-vaccine-boosters (accessed on 17 November 2021).
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against COVID-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef]
- Dziedzic, A.; Riad, A.; Attia, S.; Klugar, M.; Tanasiewicz, M. Self-Reported Adverse Events of COVID-19 Vaccines in Polish Healthcare Workers and Medical Students. Cross-Sectional Study and Pooled Analysis of CoVaST Project Results in Central Europe. J. Clin. Med. 2021, 10, 5338. [Google Scholar] [CrossRef]
- Riad, A.; Pokorná, A.; Attia, S.; Klugarová, J.; Koščík, M.; Klugar, M. Prevalence of COVID-19 Vaccine Side Effects among Healthcare Workers in the Czech Republic. J. Clin. Med. 2021, 10, 1428. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Sağıroğlu, D.; Üstün, B.; Pokorná, A.; Klugarová, J.; Attia, S.; Klugar, M. Prevalence and Risk Factors of CoronaVac Side Effects: An Independent Cross-Sectional Study among Healthcare Workers in Turkey. J. Clin. Med. 2021, 10, 2629. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Hocková, B.; Kantorová, L.; Slávik, R.; Spurná, L.; Stebel, A.; Havriľak, M.; Klugar, M. Side Effects of mRNA-Based COVID-19 Vaccine: Nationwide Phase IV Study among Healthcare Workers in Slovakia. Pharmaceuticals 2021, 14, 873. [Google Scholar] [CrossRef]
- Alhazmi, A.; Alamer, E.; Daws, D.; Hakami, M.; Darraj, M.; Abdelwahab, S.; Maghfuri, A.; Algaissi, A. Evaluation of Side Effects Associated with COVID-19 Vaccines in Saudi Arabia. Vaccines 2021, 9, 674. [Google Scholar] [CrossRef]
- Riad, A.; Pokorná, A.; Klugarová, J.; Antalová, N.; Kantorová, L.; Koščík, M.; Klugar, M. Side Effects of mRNA-Based COVID-19 Vaccines among Young Adults (18–30 Years Old): An Independent Post-Marketing Study. Pharmaceuticals 2021, 14, 1049. [Google Scholar] [CrossRef]
- Almufty, H.B.; Mohammed, S.A.; Abdullah, A.M.; Merza, M.A. Potential adverse effects of COVID19 vaccines among Iraqi population; a comparison between the three available vaccines in Iraq; a retrospective cross-sectional study. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102207. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Pokorná, A.; Mekhemar, M.; Conrad, J.; Klugarová, J.; Koščík, M.; Klugar, M.; Attia, S. Safety of ChAdOx1 nCoV-19 Vaccine: Independent Evidence from Two EU States. Vaccines 2021, 9, 673. [Google Scholar] [CrossRef] [PubMed]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef]
- Marion, O.; Del Bello, A.; Abravanel, F.; Couat, C.; Faguer, S.; Esposito, L.; Hebral, A.L.; Izopet, J.; Kamar, N. Safety and Immunogenicity of Anti-SARS-CoV-2 Messenger RNA Vaccines in Recipients of Solid Organ Transplants. Ann. Intern. Med. 2021, 174, 1336–1338. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA Covid-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef] [PubMed]
- Monin, L.; Laing, A.G.; Muñoz-Ruiz, M.; McKenzie, D.R.; del Molino del Barrio, I.; Alaguthurai, T.; Domingo-Vila, C.; Hayday, T.S.; Graham, C.; Seow, J.; et al. Safety and immunogenicity of one versus two doses of the COVID-19 vaccine BNT162b2 for patients with cancer: Interim analysis of a prospective observational study. Lancet Oncol. 2021, 22, 765–778. [Google Scholar] [CrossRef]
- KoBoToolbox.org. KoBoToolbox. Available online: https://support.kobotoolbox.org/welcome.html (accessed on 15 August 2020).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. UroToday Int. J. 2007, 335, 806–808. [Google Scholar] [CrossRef] [Green Version]
- Česká Lékařská Společnost Jana Evangelisty Purkyně (CzMA) Společnosti ČLS JEP, z.s. (Member Societies of the Czech Medical Association). Available online: https://www.cls.cz/spolecnosti-cls-jep (accessed on 15 November 2021).
- CZECRIN. Czech Clinical Research Infrastructure Network. Available online: https://czecrin.cz/en/home/ (accessed on 2 March 2021).
- Ústav Zdravotnických Informací a Statistiky České Republiky (ÚZIS ČR). Systém Hlášení Nežádoucích Událostí (SHNU). Available online: https://shnu.uzis.cz/ (accessed on 8 March 2021).
- Česká Asociace Sester (CNNA). Postoje Zdravotnických Pracovníků ke Třetím (Posilovacím) Dávkám Očkování Proti COVID-19. Available online: https://www.cnna.cz/ (accessed on 15 November 2021).
- Nás|UNIFY ČR. Available online: http://www.unify-cr.cz/o-nas (accessed on 17 November 2021).
- ČKPA—Česká Komora Porodních Asistentek, z.s. Available online: https://www.ckpa.cz/ (accessed on 17 November 2021).
- SVVS—Kdo Jsme. Available online: https://www.svvs.cz/ (accessed on 17 November 2021).
- Avvnzp. Available online: https://avvnzp.webnode.cz/ (accessed on 17 November 2021).
- Dokumenty APSS ČR—Asociace|Asociace Poskytovatelů Sociálních Služeb České Republiky. Available online: https://www.apsscr.cz/cz/asociace/dokumenty-apss-cr (accessed on 17 November 2021).
- Ministerstvo zdravotnictví České republiky (MZČR). Dotazníkový Průzkum: Postoje Zdravotnických Pracovníků ke Třetím (Posilovacím) Dávkám Očkování Proti COVID-19. Available online: https://www.mzcr.cz/dotaznik-postoje-zdravotnickych-pracovniku-treti-davka-ockovani-covid-19/ (accessed on 15 November 2021).
- Centers for Disease Control and Prevention (CDC). Epi Info™ for Windows. Available online: https://www.cdc.gov/epiinfo/pc.html (accessed on 25 December 2020).
- Centers for Disease Control and Prevention (CDC). Population Survey or Descriptive Study. Available online: https://www.cdc.gov/epiinfo/user-guide/statcalc/samplesize.html (accessed on 19 May 2021).
- Institute of Health Information and Statistics of the Czech Republic (UZIS). Health Yearbook of the Czech Republic 2017. Available online: https://www.uzis.cz/index-en.php?pg=record&id=8166 (accessed on 3 March 2021).
- Riad, A.; Abdulqader, H.; Morgado, M.; Domnori, S.; Koščík, M.; Mendes, J.J.; Klugar, M.; Kateeb, E. Global Prevalence and Drivers of Dental Students’ COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 566. [Google Scholar] [CrossRef]
- Riad, A.; Huang, Y.; Abdulqader, H.; Morgado, M.; Domnori, S.; Koščík, M.; Mendes, J.J.; Klugar, M.; Kateeb, E. IADS-SCORE Universal Predictors of Dental Students’ Attitudes towards COVID-19 Vaccination: Machine Learning-Based Approach. Vaccines 2021, 9, 1158. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Pokorná, A.; Antalová, N.; Krobot, M.; Zviadadze, N.; Serdiuk, I.; Koščík, M.; Klugar, M. Prevalence and Drivers of COVID-19 Vaccine Hesitancy among Czech University Students: National Cross-Sectional Study. Vaccines 2021, 9, 948. [Google Scholar] [CrossRef]
- Kateeb, E.; Danadneh, M.; Pokorná, A.; Klugarová, J.; Abdulqader, H.; Klugar, M.; Riad, A. Predictors of Willingness to Receive COVID-19 Vaccine: Cross-Sectional Study of Palestinian Dental Students. Vaccines 2021, 9, 954. [Google Scholar] [CrossRef]
- Štěpánek, L.; Janošíková, M.; Nakládalová, M.; Štěpánek, L.; Boriková, A.; Vildová, H. Motivation to COVID-19 Vaccination and Reasons for Hesitancy in Employees of a Czech Tertiary Care Hospital: A Cross-Sectional Survey. Vaccines 2021, 9, 863. [Google Scholar] [CrossRef] [PubMed]
- Trent, M.; Seale, H.; Chughtai, A.; Salmon, D.; MacIntyre, C. Trust in government, intention to vaccinate and COVID-19 vaccine hesitancy: A comparative survey of five large cities in the United States, United Kingdom, and Australia. Vaccine 2021, in press. [Google Scholar] [CrossRef]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Salerno, L.; Craxì, L.; Amodio, E.; Lo Coco, G. Factors Affecting Hesitancy to mRNA and Viral Vector COVID-19 Vaccines among College Students in Italy. Vaccines 2021, 9, 927. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- (WMA), W.M.A. World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Proton Technologies AG General Data Protection Regulation (GDPR). Compliance Guidelines. Available online: https://gdpr.eu/ (accessed on 1 May 2020).
- SPSS Inc. IBM SPSS Statistics 28. Available online: https://www.ibm.com/support/pages/ibm-spss-statistics-28-documentation (accessed on 14 March 2021).
- AION-CS 95/2004 Sb. Zákon o Podmínkách Získávání a Uznávání Způsobilosti k Výkonu Povolání Lékařů a Farmaceutů. Available online: https://www.zakonyprolidi.cz/cs/2004-95 (accessed on 15 November 2021).
- AION-CS 96/2004 Sb. Zákon o Nelékařských Zdravotnických Povoláních. Available online: https://www.zakonyprolidi.cz/cs/2004-96 (accessed on 15 November 2021).
- Ústav Zdravotnických Informací a Statistiky ČR (ÚZIS). Rozlišení Lékařských a Nelékařských Zdravotnických Povolání: Lékař, Sestra a Další Nelékařská Povolání. Available online: https://www.nzip.cz/clanek/479-lekarska-vs-nelekarska-zdravotnicka-povolani (accessed on 15 November 2021).
- AION-CS 129/2000 Sb. Zákon o Krajích. Available online: https://www.zakonyprolidi.cz/cs/2000-129 (accessed on 15 November 2021).
- NHMRC, N.H.; M.R.C. Australian Guidelines for the Clinical Care of People with COVID-19. Available online: https://www.clinicalguidelines.gov.au/register/australian-guidelines-clinical-care-people-covid-19 (accessed on 17 September 2020).
- Sugawara, N.; Yasui-Furukori, N.; Fukushima, A.; Shimoda, K.; Diclemente, J. Attitudes of Medical Students toward COVID-19 Vaccination: Who Is Willing to Receive a Third Dose of the Vaccine? Vaccines 2021, 9, 1295. [Google Scholar] [CrossRef] [PubMed]
- Czech Statistical Office (CZSO). Zaostřeno na Ženy a Muže 2018 (Focus on Women and Men 2018). Available online: https://www.czso.cz/documents/10180/60622084/30000218.pdf (accessed on 17 November 2021).
- Czech Statistical Office (CZSO). Odměňování Zdravotnických Pracovníků (Remuneration of Healthcare Staff). Available online: https://www.czso.cz/documents/10180/112643651/260024-19.pdf (accessed on 17 November 2021).
- Worldmeter Coronavirus Update (Live). Available online: https://www.worldometers.info/coronavirus/ (accessed on 17 November 2021).
- Jarkovsky, J.; Benesova, K.; Cerny, V.; Razova, J.; Kala, P.; Dolina, J.; Majek, O.; Sebestova, S.; Bezdekova, M.; Melicharova, H.; et al. Covidogram as a simple tool for predicting severe course of COVID-19: Population-based study. BMJ Open 2021, 11, e045442. [Google Scholar] [CrossRef] [PubMed]
- Komenda, M.; Bulhart, V.; Karolyi, M.; Jarkovský, J.; Mužík, J.; Májek, O.; Šnajdrová, L.; Růžičková, P.; Rážová, J.; Prymula, R.; et al. Complex reporting of the COVID-19 epidemic in the czech republic: Use of an interactive web-based app in practice. J. Med. Internet Res. 2020, 22, e19367. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 v ČR: Otevřené Datové Sady a Sady ke Stažení | Onemocnění Aktuálně od MZČR. Available online: https://onemocneni-aktualne.mzcr.cz/api/v2/covid-19 (accessed on 17 November 2021).
- Shatnawi, N.J.; Mesmar, Z.; Al-Omari, G.A.; AL-Sheyab, W.; AlZoubi, N.A.; AL-Ghazo, M.; Hamouri, S.; AL-Faori, I.; Bani-Essa, A.; Matalka, I.; et al. Compliance with safety measures and risk of COVID-19 transmission among healthcare workers. Future Sci. OA 2021. [Google Scholar] [CrossRef]
- Lai, X.; Wang, X.; Yang, Q.; Xu, X.; Tang, Y.; Liu, C.; Tan, L.; Lai, R.; Wang, H.; Zhang, X.; et al. Will healthcare workers improve infection prevention and control behaviors as COVID-19 risk emerges and increases, in China? Antimicrob. Resist. Infect. Control 2020, 9, 83. [Google Scholar] [CrossRef]
- Ashinyo, M.E.; Dubik, S.D.; Duti, V.; Amegah, K.E.; Ashinyo, A.; Asare, B.A.; Ackon, A.A.; Akoriyea, S.K.; Kuma-Aboagye, P. Infection prevention and control compliance among exposed healthcare workers in COVID-19 treatment centers in Ghana: A descriptive cross-sectional study. PLoS ONE 2021, 16, e0248282. [Google Scholar] [CrossRef]
- Keehner, J.; Horton, L.E.; Pfeffer, M.A.; Longhurst, C.A.; Schooley, R.T.; Currier, J.S.; Abeles, S.R.; Torriani, F.J. SARS-CoV-2 Infection after Vaccination in Health Care Workers in California. N. Engl. J. Med. 2021, 384, 1774–1775. [Google Scholar] [CrossRef]
- Gohil, S.K.; Olenslager, K.; Quan, K.A.; Dastur, C.K.; Afsar, N.; Chang, W.; Huang, S.S. Asymptomatic and Symptomatic COVID-19 Infections Among Health Care Personnel Before and After Vaccination. JAMA Netw. Open 2021, 4, e2115980. [Google Scholar] [CrossRef]
- Gilboa, M.; Tal, I.; Levin, E.G.; Segal, S.; Belkin, A.; Zilberman-Daniels, T.; Biber, A.; Rubin, C.; Rahav, G.; Regev-Yochay, G. Coronavirus disease 2019 (COVID-19) vaccination uptake among healthcare workers. Infect. Control Hosp. Epidemiol. 2021, 1–6. [Google Scholar] [CrossRef]
- Lee, J.T.; Althomsons, S.P.; Wu, H.; Budnitz, D.S.; Kalayil, E.J.; Lindley, M.C.; Pingali, C.; Bridges, C.B.; Geller, A.I.; Fiebelkorn, A.P.; et al. Disparities in COVID-19 Vaccination Coverage Among Health Care Personnel Working in Long-Term Care Facilities, by Job Category, National Healthcare Safety Network—United States, March 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1036–1039. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. Covid-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef]
- Ministerstvo Zdravotnictví ČR (MZČR). COVID-19: Přehled Vykázaných Očkování v ČR. Available online: https://onemocneni-aktualne.mzcr.cz/vakcinace-cr (accessed on 10 November 2021).
- Finney Rutten, L.J.; Zhu, X.; Leppin, A.L.; Ridgeway, J.L.; Swift, M.D.; Griffin, J.M.; St. Sauver, J.L.; Virk, A.; Jacobson, R.M. Evidence-Based Strategies for Clinical Organizations to Address COVID-19 Vaccine Hesitancy. Mayo Clin. Proc. 2021, 96, 699–707. [Google Scholar] [CrossRef]
- Kuter, B.J.; Browne, S.; Momplaisir, F.M.; Feemster, K.A.; Shen, A.K.; Green-McKenzie, J.; Faig, W.; Offit, P.A. Perspectives on the receipt of a COVID-19 vaccine: A survey of employees in two large hospitals in Philadelphia. Vaccine 2021, 39, 1693–1700. [Google Scholar] [CrossRef] [PubMed]
- Schernhammer, E.; Weitzer, J.; Laubichler, M.D.; Birmann, B.M.; Bertau, M.; Zenk, L.; Caniglia, G.; Jäger, C.C.; Steiner, G. Correlates of COVID-19 vaccine hesitancy in Austria: Trust and the government. J. Public Health 2021, fdab122. [Google Scholar] [CrossRef]
- Gur-Arie, R.; Jamrozik, E.; Kingori, P. No Jab, No Job? Ethical Issues in Mandatory COVID-19 Vaccination of Healthcare Personnel. BMJ Glob. Health 2021, 6, e004877. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Cohen, C.; Hernán, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef]
- Flanagan, K.L.; Fink, A.L.; Plebanski, M.; Klein, S.L. Sex and Gender Differences in the Outcomes of Vaccination over the Life Course. Annu. Rev. Cell Dev. Biol. 2017, 33, 577–599. [Google Scholar] [CrossRef]
- Klein, S.L.; Jedlicka, A.; Pekosz, A. The Xs and Y of immune responses to viral vaccines. Lancet Infect. Dis. 2010, 10, 338–349. [Google Scholar] [CrossRef]
- Gadoth, A.; Halbrook, M.; Martin-Blais, R.; Gray, A.; Tobin, N.H.; Ferbas, K.G.; Aldrovandi, G.M.; Rimoin, A.W. Cross-sectional Assessment of COVID-19 Vaccine Acceptance Among Health Care Workers in Los Angeles. Ann. Intern. Med. 2021, 174, 882–885. [Google Scholar] [CrossRef]
- Keske, Ş.; Mutters, N.T.; Tsioutis, C.; Ergönül, Ö. Influenza vaccination among infection control teams: A EUCIC survey prior to COVID-19 pandemic. Vaccine 2020, 38, 8357–8361. [Google Scholar] [CrossRef] [PubMed]
- Hollmeyer, H.G.; Hayden, F.; Poland, G.; Buchholz, U. Influenza vaccination of health care workers in hospitals--a review of studies on attitudes and predictors. Vaccine 2009, 27, 3935–3944. [Google Scholar] [CrossRef] [PubMed]
- Pless, A.; McLennan, S.R.; Nicca, D.; Shaw, D.M.; Elger, B.S. Reasons why nurses decline influenza vaccination: A qualitative study. BMC Nurs. 2017, 16, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Media Briefing on COVID-19. Available online: https://www.youtube.com/watch?v=L3fNLTJT4GU&t=3s&ab_channel=WorldHealthOrganization%28WHO%29 (accessed on 17 November 2021).
- Hotez, P.J.; Batista, C.; Amor, Y.B.; Ergonul, O.; Figueroa, J.P.; Gilbert, S.; Gursel, M.; Hassanain, M.; Kang, G.; Kaslow, D.C.; et al. Global public health security and justice for vaccines and therapeutics in the COVID-19 pandemic. EClinicalMedicine 2021, 39, 101053. [Google Scholar] [CrossRef]
- WHO-SAGE. Interim Statement on Booster Doses for COVID-19 Vaccination. Available online: https://www.who.int/news/item/04-10-2021-interim-statement-on-booster-doses-for-covid-19-vaccination (accessed on 17 November 2021).
- Parente, D.J.; Ojo, A.; Gurley, T.; Le Master, J.W.; Meyer, M.; Wild, D.M.; Mustafa, R.A. Acceptance of COVID-19 Vaccination Among Health System Personnel. J. Am. Board Fam. Med. 2021, 34, 498–508. [Google Scholar] [CrossRef]
- Rey, D.; Fressard, L.; Cortaredona, S.; Bocquier, A.; Gautier, A.; Peretti-Watel, P.; Verger, P. Vaccine hesitancy in the French population in 2016, and its association with vaccine uptake and perceived vaccine risk–benefit balance. Eurosurveillance 2018, 23, 17-00816. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
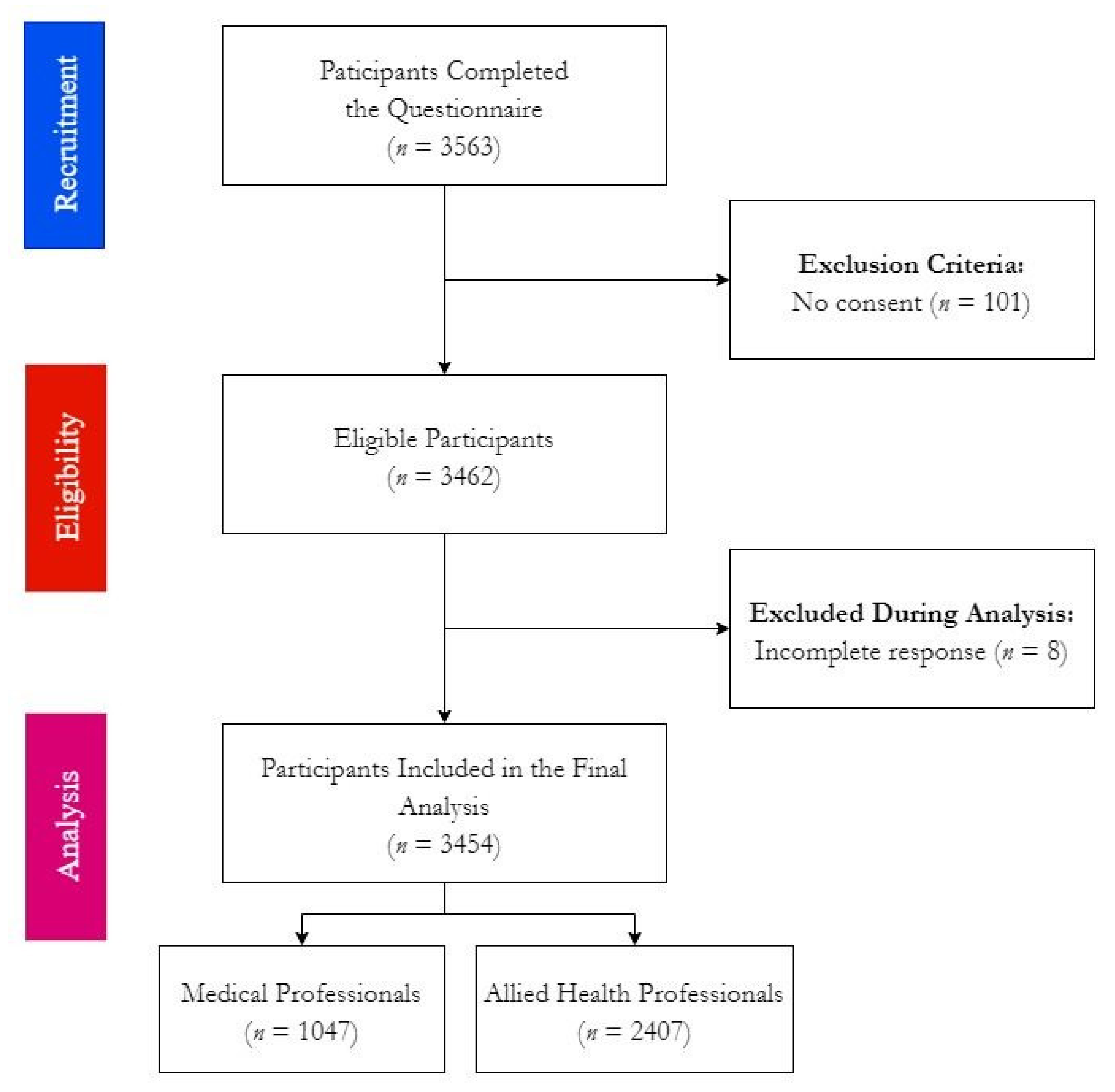
| Variable | Outcome | Frequency (n) | Percentage (%) |
|---|---|---|---|
| Gender | Female † | 2796 | 80.9% |
| Male | 643 | 18.6% | |
| LGBTQ+ | 15 | 0.4% | |
| † Pregnancy | Yes ‡ | 25 | 0.9% |
| No | 2771 | 99.1% | |
| ‡ Trimester | 1st Trimester | 9 | 36% |
| 2nd Trimester | 10 | 40% | |
| 3rd Trimester | 6 | 24% | |
| Age | ≤47 years-old | 1744 | 50.5% |
| >47 years-old | 1710 | 49.5% | |
| Profession | Medical Professionals (MP) | 1047 | 30.3% |
| Allied Health Professionals (AHP) | 2407 | 69.7% |
| Variable | Outcome | Medical Professionals (n = 1047) | Allied Health Professionals (n = 2407) | Sig. | Female (n = 2796) | Male (n = 643) | Sig. | ≤47 Years (n = 1744) | >47 Years (n = 1710) | Sig. | Total (n = 3454) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Infection | Yes † | 297 (28.4%) | 809 (33.6%) | 0.002 | 908 (32.5%) | 195 (30.3%) | 0.293 | 602 (34.5%) | 504 (29.5%) | 0.001 | 1106 (32.0%) |
| No | 750 (71.6%) | 1598 (66.4%) | 1888 (67.5%) | 448 (69.7%) | 1142 (65.5%) | 1206 (70.5%) | 2348 (68.0%) | ||||
| † Onset | Before 1st Dose | 257 (86.5%) | 714 (88.3%) | 0.437 | 793 (87.3%) | 175 (89.7%) | 0.352 | 527 (87.5%) | 444 (88.1%) | 0.779 | 971 (87.8%) |
| Between Doses | 22 (7.4%) | 47 (5.8%) | 0.330 | 57 (6.3%) | 12 (6.2%) | 0.948 | 41 (6.8%) | 28 (5.6%) | 0.390 | 69 (6.2%) | |
| After 2nd Dose | 18 (6.1%) | 48 (5.9%) | 0.937 | 58 (6.4%) | 8 (4.1%) | 0.222 | 34 (5.6%) | 32 (6.3%) | 0.624 | 66 (6.0%) | |
| † Severity | Asymptomatic | 17 (5.7%) | 62 (7.7%) | 0.267 | 61 (6.7%) | 18 (9.2%) | 0.217 | 39 (6.5%) | 40 (7.9%) | 0.348 | 79 (7.1%) |
| Mild | 188 (63.3%) | 470 (58.1%) | 0.118 | 542 (59.7%) | 114 (58.5%) | 0.751 | 392 (65.1%) | 266 (52.8%) | <0.001 | 658 (59.5%) | |
| Moderate | 84 (28.3%) | 263 (32.5%) | 0.179 | 290 (31.9%) | 56 (28.7%) | 0.379 | 164 (27.2%) | 183 (36.3%) | 0.001 | 347 (31.4%) | |
| Severe | 5 (1.7%) | 13 (1.6%) | 1.000 * | 13 (1.4%) | 5 (2.6%) | 0.344 * | 6 (1.0%) | 12 (2.4%) | 0.070 | 18 (1.6%) | |
| Critic | 3 (1.0%) | 1 (0.1%) | 0.062 * | 2 (0.2%) | 2 (0.1%) | 0.146 * | 1 (0.2%) | 3 (0.6%) | 0.336 * | 4 (0.4%) | |
| † Sign & Symptoms | Fever | 185 (62.3%) | 439 (54.3%) | 0.017 | 502 (55.3%) | 119 (61.0%) | 0.143 | 331 (55.0%) | 293 (58.1%) | 0.292 | 624 (56.4%) |
| Cough | 149 (50.2%) | 403 (49.8%) | 0.917 | 461 (50.8%) | 90 (46.2%) | 0.242 | 293 (48.7%) | 259 (51.4%) | 0.368 | 552 (49.9%) | |
| Dyspnea | 55 (18.5%) | 265 (32.8%) | <0.001 | 278 (30.6%) | 41 (21.0%) | 0.007 | 160 (26.6%) | 160 (31.7%) | 0.059 | 320 (28.9%) | |
| Fatigue | 229 (77.1%) | 624 (77.1%) | 0.992 | 705 (77.6%) | 145 (74.4%) | 0.322 | 458 (76.1%) | 395 (78.4%) | 0.366 | 853 (77.1%) | |
| Myalgia | 194 (65.3%) | 538 (66.5%) | 0.713 | 601 (66.2%) | 128 (65.6%) | 0.883 | 406 (67.4%) | 326 (64.7%) | 0.334 | 732 (66.2%) | |
| Headache | 167 (56.2%) | 533 (65.9%) | 0.003 | 601 (66.2%) | 97 (49.7%) | <0.001 | 394 (65.4%) | 306 (60.7%) | 0.104 | 700 (63.3%) | |
| Anosmia | 163 (54.9%) | 500 (61.8%) | 0.037 | 574 (63.2%) | 87 (44.6%) | <0.001 | 398 (66.1%) | 265 (52.6%) | <0.001 | 663 (59.9%) | |
| Dysgeusia | 115 (38.7%) | 396 (48.9%) | 0.002 | 444 (48.9%) | 65 (33.3%) | <0.001 | 296 (49.2%) | 215 (42.7%) | 0.031 | 511 (46.2%) | |
| Pharyngitis | 54 (18.2%) | 148 (18.3%) | 0.966 | 177 (19.5%) | 25 (12.8%) | 0.029 | 110 (18.3%) | 92 (18.3%) | 0.994 | 202 (18.3%) | |
| Congestion | 104 (35.0%) | 261 (32.3%) | 0.388 | 319 (35.1%) | 46 (23.6%) | 0.002 | 228 (37.9%) | 137 (27.2%) | <0.001 | 365 (33.0%) | |
| Rhinitis | 100 (33.7%) | 256 (31.6%) | 0.523 | 301 (33.1%) | 55 (28.2%) | 0.180 | 208 (34.6%) | 148 (29.4%) | 0.066 | 356 (32.2%) | |
| Nausea | 29 (9.8%) | 128 (15.8%) | 0.011 | 142 (15.6%) | 14 (7.2%) | 0.002 | 74 (12.3%) | 83 (16.5%) | 0.048 | 157 (14.2%) | |
| Vomiting | 6 (2.0%) | 49 (6.1%) | 0.006 | 49 (5.4%) | 6 (3.1%) | 0.177 | 29 (4.8%) | 26 (5.2%) | 0.795 | 55 (5.0%) | |
| Diarrhea | 46 (15.5%) | 159 (19.7%) | 0.114 | 173 (19.1%) | 31 (15.9%) | 0.303 | 96 (15.9%) | 109 (21.6%) | 0.015 | 205 (18.5%) |
| Variable | Outcome | Medical Professionals (n = 1047) | Allied Health Professionals (n = 2407) | Sig. | Female (n = 2796) | Male (n = 643) | Sig. | ≤47 Years (n = 1744) | >47 Years (n = 1710) | Sig. | Total (n = 3454) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Vaccinated | Yes † | 1012 (96.7%) | 2275 (94.5%) | 0.007 | 2651 (94.8%) | 625 (97.2%) | 0.010 | 1637 (93.9%) | 1650 (96.5%) | <0.001 | 3287 (95.2%) |
| No | 35 (3.3%) | 132 (5.5%) | 145 (5.2%) | 18 (2.8%) | 107 (6.1%) | 60 (3.5%) | 167 (4.8%) | ||||
| † Vaccine Type | BTN162b2 | 962 (95.1%) | 2018 (88.7%) | <0.001 | 2390 (90.2%) | 580 (92.8%) | 0.041 | 1481 (90.5%) | 1499 (90.8%) | 0.710 | 2980 (90.7%) |
| mRNA-1273 | 19 (1.9%) | 156 (6.9%) | <0.001 | 155 (5.8%) | 20 (3.2%) | 0.008 | 100 (6.1%) | 75 (4.5%) | 0.046 | 175 (5.3%) | |
| AZD1222 | 20 (2.0%) | 68 (3.0%) | 0.097 | 70 (2.6%) | 17 (2.7%) | 0.911 | 36 (2.2%) | 52 (3.2%) | 0.091 | 88 (2.7%) | |
| Ad26.COV2.S | 11 (1.1%) | 33 (1.5%) | 0.402 | 36 (1.4%) | 8 (1.3%) | 0.879 | 20 (1.2%) | 24 (1.5%) | 0.561 | 44 (1.3%) | |
| † Doses Number | One | 16 (1.6%) | 43 (1.9%) | 0.539 | 50 (1.5%) | 9 (1.4%) | 0.451 | 29 (1.8%) | 30 (1.8%) | 0.918 | 59 (1.8%) |
| Two | 387 (38.2%) | 1246 (54.7%) | <0.001 | 1388 (52.4%) | 237 (37.9%) | <0.001 | 907 (55.4%) | 726 (44.0%) | <0.001 | 1633 (49.7%) | |
| Three | 609 (60.2%) | 986 (43.3%) | <0.001 | 1213 (45.8%) | 379 (60.6%) | <0.001 | 701 (42.8%) | 894 (54.2%) | <0.001 | 1595 (48.5%) | |
| † Medical Care | Yes | 23 (2.3%) | 90 (4.0%) | 0.014 | 98 (3.7%) | 13 (2.1%) | 0.044 | 64 (3.9%) | 49 (3.0%) | 0.139 | 113 (3.4%) |
| No | 989 (97.7%) | 2185 (96.0%) | 2553 (96.3%) | 612 (97.9%) | 1573 (96.1%) | 1601 (97.0%) | 3174 (96.6%) |
| Variable | Outcome | Medical Professionals (n = 1047) | Allied Health Professionals (n = 2407) | Sig. | Female (n = 2796) | Male (n = 643) | Sig. | ≤47 Years (n = 1744) | >47 Years (n = 1710) | Sig. | Total (n = 3454) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Attitudes | Rejection | 154 (14.7%) | 416 (17.3%) | 0.061 | 468 (16.7%) | 93 (14.5%) | 0.159 | 344 (19.7%) | 226 (13.2%) | <0.001 | 570 (16.5%) |
| Hesitancy | 80 (7.6%) | 340 (14.1%) | <0.001 | 379 (13.6%) | 40 (6.2%) | <0.001 | 244 (14.0%) | 176 (10.3%) | <0.001 | 420 (12.2%) | |
| Acceptance † | 813 (77.7%) | 1651 (68.6%) | <0.001 | 1949 (69.7%) | 510 (79.3%) | <0.001 | 1156 (66.3%) | 1308 (76.5%) | <0.001 | 2464 (71.3%) | |
| † Promoter | Self-protection | 773 (95.1%) | 1511 (91.5%) | 0.001 | 1806 (92.7%) | 473 (92.7%) | 0.949 | 1068 (92.4%) | 1216 (93.0%) | 0.582 | 2284 (82.7%) |
| Patient Prot. | 608 (74.8%) | 1126 (68.2%) | <0.001 | 1376 (70.6%) | 354 (69.4%) | 0.601 | 817 (70.7%) | 917 (70.1%) | 0.758 | 1734 (70.4%) | |
| Family Prot. | 690 (84.9%) | 1354 (82.0%) | 0.076 | 1626 (83.4%) | 414 (81.2%) | 0.229 | 996 (86.2%) | 1048 (80.1%) | <0.001 | 2044 (83.0%) | |
| Community Prot. | 618 (76.0%) | 1018 (61.7%) | <0.001 | 1256 (64.4%) | 376 (73.7%) | <0.001 | 788 (68.2%) | 848 (64.8%) | 0.080 | 1636 (66.4%) | |
| Avoid Testing | 238 (29.3%) | 482 (29.2%) | 0.967 | 561 (28.8%) | 158 (31.0%) | 0.332 | 344 (29.8%) | 376 (28.7%) | 0.582 | 720 (29.2%) | |
| Easier Mobility | 419 (51.5%) | 809 (49.0%) | 0.236 | 959 (49.2%) | 267 (52.4%) | 0.206 | 603 (52.2%) | 625 (47.8%) | 0.030 | 1128 (49.8%) | |
| Employer | 26 (3.2%) | 58 (3.5%) | 0.685 | 61 (3.1%) | 23 (4.5%) | 0.127 | 38 (3.3%) | 46 (3.5%) | 0.754 | 84 (3.4%) |
| Variable | Outcome | Frequency (n) | Percentage (%) |
|---|---|---|---|
| [Severe Illness] I think the currently available BD (third shots) can protect me from severe COVID-19 infection. | Disagreement | 309 | 8.9% |
| Not Sure | 373 | 10.8% | |
| Agreement | 2772 | 80.3% | |
| [Symptomatic Infection] I think the currently available BD (third shots) can protect me from symptomatic COVID-19 infection. | Disagreement | 663 | 19.2% |
| Not Sure | 793 | 23.0% | |
| Agreement | 1998 | 57.8% | |
| [Community Transmission] I think the currently available BD (third shots) can prevent community transmission of SARS-CoV-2 and its variants. | Disagreement | 645 | 18.7% |
| Not Sure | 709 | 20.5% | |
| Agreement | 2100 | 60.8% | |
| [Mutations Control] I will not take the third shoot (BD) until I find reliable evidence confirming their ability to tackle the new circulating variants of SARS-CoV-2. | Disagreement | 589 | 17.1% |
| Not Sure | 618 | 17.9% | |
| Agreement | 2247 | 65.1% | |
| [Equal Safety] I think the currently available BD (third shots) are as safe as the previous doses of COVID-19 vaccines. | Disagreement | 241 | 7.0% |
| Not Sure | 570 | 16.5% | |
| Agreement | 2643 | 76.5% | |
| [Non-inferior Safety] I think that the currently available BD (third shots) are as safe as the previous doses of COVID-19 vaccines. | Disagreement | 1929 | 55.8% |
| Not Sure | 1094 | 31.7% | |
| Agreement | 431 | 12.5% | |
| [Risk-benefit Ratio] I believe that the benefits of BD (third shots) outweigh their risks. | Disagreement | 331 | 9.6% |
| Not Sure | 426 | 12.3% | |
| Agreement | 2697 | 78.1% | |
| [Self-prioritization] I agree to be prioritized to receive the currently available BD (third shorts). | Disagreement | 625 | 18.1% |
| Not Sure | 509 | 14.7% | |
| Agreement | 2320 | 67.2% | |
| [Global Vaccine Justice] I agree to receive the BD (third shot) of the COVID-19 vaccine even after learning that administering third shots in developed economies may deprive masses in the third world from getting even the first dose. | Disagreement | 1052 | 30.5% |
| Not Sure | 1255 | 36.3% | |
| Agreement | 1147 | 33.2% | |
| [National Vaccine Justice] I agree to receive the BD (third shot) of the COVID-19 vaccine even after learning that this may affect the accessibility of some population groups to the vaccine. | Disagreement | 1297 | 37.6% |
| Not Sure | 1153 | 33.4% | |
| Agreement | 1004 | 29.1% | |
| [Vaccine Satisfaction] I think I should receive a different vaccine type/brand for the BD from the previous doses. | Disagreement | 1405 | 40.7% |
| Not Sure | 1680 | 48.6% | |
| Agreement † | 369 | 10.7% | |
| [Vaccine Selectivity] I think the government should purchase a particular vaccine type/brand for the BD. | Disagreement | 1071 | 31.0% |
| Not Sure | 1644 | 47.6% | |
| Agreement † | 739 | 21.4% | |
| † [Preferred Vaccine] Which vaccine type should be promoted for BD? | BTN162b2 | 611 | 69.3% |
| mRNA-1273 | 193 | 21.9% | |
| AZD1222 | 21 | 2.4% | |
| Ad26.COV2.S | 57 | 6.5% |
| Variable | Outcome | Medical Professionals (n = 1047) | Allied Health Professionals (n = 2407) | Sig. | Female (n = 2796) | Male (n = 643) | Sig. | ≤47 Years (n = 1744) | >47 Years (n = 1710) | Sig. |
|---|---|---|---|---|---|---|---|---|---|---|
| Severe Illness | Disagree | 78 (7.4%) | 231 (9.6%) | 0.042 | 261 (9.3%) | 43 (6.7%) | 0.033 | 194 (11.1%) | 115 (6.7%) | <0.001 |
| Not Sure | 72 (6.9%) | 301 (12.5%) | <0.001 | 329 (11.8%) | 42 (6.5%) | <0.001 | 210 (12.0%) | 163 (9.5%) | 0.018 | |
| Agree | 897 (85.7%) | 1875 (77.9%) | <0.001 | 2206 (78.9%) | 558 (86.8%) | <0.001 | 1340 (76.8%) | 1432 (83.7%) | <0.001 | |
| Symptomatic Infection | Disagree | 196 (18.7%) | 467 (19.4%) | 0.640 | 548 (19.6%) | 106 (16.5%) | 0.070 | 397 (22.8%) | 266 (15.6%) | <0.001 |
| Not Sure | 184 (17.6%) | 609 (25.3%) | <0.001 | 675 (24.1%) | 114 (17.7%) | <0.001 | 415 (23.8%) | 378 (22.1%) | 0.238 | |
| Agree | 667 (63.7%) | 1331 (55.3%) | <0.001 | 1573 (56.3%) | 423 (65.8%) | <0.001 | 932 (53.4%) | 1066 (62.3%) | <0.001 | |
| Community Transmission | Disagree | 178 (17.0%) | 467 (19.4%) | 0.096 | 521 (18.6%) | 116 (18.0%) | 0.727 | 400 (22.9%) | 245 (14.3%) | <0.001 |
| Not Sure | 169 (16.1%) | 540 (22.4%) | <0.001 | 599 (21.4%) | 108 (16.8%) | 0.009 | 366 (21.0%) | 343 (20.1%) | 0.500 | |
| Agree | 700 (66.9%) | 1400 (58.2%) | <0.001 | 1676 (59.9%) | 419 (65.2%) | 0.014 | 978 (56.1%) | 1122 (65.6%) | <0.001 | |
| Mutations Control | Disagree | 217 (20.7%) | 372 (15.5%) | <0.001 | 443 (15.8%) | 144 (22.4%) | <0.001 | 329 (18.9%) | 260 (15.2%) | 0.004 |
| Not Sure | 152 (14.5%) | 466 (19.4%) | <0.001 | 515 (18.4%) | 100 (15.6%) | 0.087 | 320 (18.3%) | 298 (17.4%) | 0.480 | |
| Agree | 678 (64.8%) | 1569 (65.2%) | 0.808 | 1838 (65.7%) | 399 (62.1%) | 0.077 | 1095 (62.8%) | 1152 (67.4%) | 0.005 | |
| Equal Safety | Disagree | 68 (6.5%) | 173 (7.2%) | 0.463 | 203 (7.3%) | 33 (5.1%) | 0.054 | 145 (8.3%) | 96 (5.6%) | 0.002 |
| Not Sure | 94 (9.0%) | 476 (19.8%) | <0.001 | 508 (18.2%) | 58 (9.0%) | <0.001 | 311 (17.8%) | 259 (15.1%) | 0.033 | |
| Agree | 885 (84.5%) | 1758 (73.0%) | <0.001 | 2085 (74.6%) | 552 (85.8%) | <0.001 | 1288 (73.9%) | 1355 (79.2%) | <0.001 | |
| Non-inferior Safety | Disagree | 689 (65.8%) | 1240 (51.5%) | <0.001 | 1467 (52.5%) | 453 (70.5%) | <0.001 | 956 (54.8%) | 973 (56.9%) | 0.217 |
| Not Sure | 242 (23.1%) | 852 (35.4%) | <0.001 | 955 (34.2%) | 134 (20.8%) | <0.001 | 555 (31.8%) | 539 (31.5%) | 0.848 | |
| Agree | 116 (11.1%) | 315 (13.1%) | 0.101 | 374 (13.4%) | 56 (8.7%) | 0.001 | 233 (13.4%) | 198 (11.6%) | 0.113 | |
| Risk-benefit Ratio | Disagree | 86 (8.2%) | 245 (10.2%) | 0.071 | 272 (9.7%) | 52 (8.1%) | 0.199 | 198 (11.4%) | 133 (7.8%) | <0.001 |
| Not Sure | 80 (7.6%) | 346 (14.4%) | <0.001 | 383 (13.7%) | 42 (6.5%) | <0.001 | 248 (14.2%) | 178 (10.4%) | <0.001 | |
| Agree | 881 (84.1%) | 1816 (75.4%) | <0.001 | 2141 (76.6%) | 549 (85.4%) | <0.001 | 1298 (74.4%) | 1399 (81.8%) | <0.001 | |
| Self-prioritization | Disagree | 142 (13.6%) | 483 (20.1%) | <0.001 | 537 (19.2%) | 83 (12.9%) | <0.001 | 387 (22.2%) | 238 (13.9%) | <0.001 |
| Not Sure | 145 (13.8%) | 364 (15.1%) | 0.332 | 414 (14.8%) | 92 (14.3%) | 0.747 | 291 (16.7%) | 218 (12.7%) | 0.001 | |
| Agree | 760 (72.6%) | 1560 (64.8%) | <0.001 | 1845 (66.0%) | 468 (72.8%) | <0.001 | 1066 (61.1%) | 1254 (73.3%) | <0.001 | |
| Global Vaccine Justice | Disagree | 244 (23.3%) | 808 (33.6%) | <0.001 | 896 (32.0%) | 149 (23.2%) | <0.001 | 629 (36.1%) | 423 (24.7%) | <0.001 |
| Not Sure | 362 (34.6%) | 893 (37.1%) | 0.156 | 1058 (37.8%) | 193 (30.0%) | <0.001 | 596 (34.2%) | 659 (38.5%) | 0.008 | |
| Agree | 441 (42.1%) | 706 (29.3%) | <0.001 | 842 (30.1%) | 301 (46.8%) | <0.001 | 519 (29.8%) | 628 (36.7%) | <0.001 | |
| National Vaccine Justice | Disagree | 330 (31.5%) | 967 (40.2%) | <0.001 | 1099 (39.3%) | 191 (29.7%) | <0.001 | 766 (43.9%) | 531 (31.1%) | <0.001 |
| Not Sure | 323 (30.9%) | 830 (34.5%) | 0.037 | 961 (34.4%) | 188 (29.2%) | 0.013 | 513 (29.4%) | 640 (37.4%) | <0.001 | |
| Agree | 394 (37.6%) | 610 (25.3%) | <0.001 | 736 (26.3%) | 264 (41.1%) | <0.001 | 465 (26.7%) | 539 (31.5%) | 0.002 | |
| Vaccine Satisfaction | Disagree | 393 (37.5%) | 1012 (42.0%) | 0.013 | 1151 (41.2%) | 248 (38.6%) | 0.227 | 764 (43.8%) | 641 (37.5%) | <0.001 |
| Not Sure | 531 (50.7%) | 1149 (47.7%) | 0.107 | 1370 (49.0%) | 303 (47.1%) | 0.391 | 786 (45.1%) | 894 (52.3%) | <0.001 | |
| Agree | 123 (11.7%) | 246 (10.2%) | 0.182 | 275 (9.8%) | 92 (14.3%) | <0.001 | 194 (11.1%) | 175 (10.2%) | 0.397 | |
| Vaccine Selectivity | Disagree | 304 (29.0%) | 767 (31.9%) | 0.098 | 875 (31.3%) | 190 (29.5%) | 0.388 | 629 (36.1%) | 442 (25.8%) | <0.001 |
| Not Sure | 504 (48.1%) | 1140 (47.4%) | 0.675 | 1346 (48.1%) | 292 (45.4%) | 0.212 | 790 (45.3%) | 854 (49.9%) | 0.006 | |
| Agree | 239 (22.8%) | 500 (20.8%) | 0.176 | 575 (20.6%) | 161 (25.0%) | 0.013 | 325 (18.6%) | 414 (24.2%) | <0.001 | |
| Preferred Vaccine | BTN162b2 | 189 (66.3%) | 422 (70.7%) | 0.188 | 476 (70.0%) | 132 (66.7%) | 0.371 | 257 (63.9%) | 354 (73.8%) | 0.002 |
| mRNA-1273 | 68 (23.9%) | 125 (20.9%) | 0.326 | 147 (21.6%) | 45 (22.7%) | 0.740 | 105 (26.1%) | 88 (18.3%) | 0.005 | |
| AZD1222 | 11 (3.9%) | 10 (1.7%) | 0.047 | 11 (1.6%) | 10 (5.1%) | 0.013 * | 9 (2.2%) | 12 (2.5%) | 0.800 | |
| Ad26.COV2.S | 17 (6.0%) | 40 (6.7%) | 0.678 | 46 (6.8%) | 11 (5.6%) | 0.543 | 31 (7.7%) | 26 (5.4%) | 0.167 |
| Variable | Outcome | Rejection (n = 570; 16.5%) | Sig. | Hesitancy (n = 420; 12.2%) | Sig. | Acceptance (n = 2464; 71.3%) | Sig. | |
|---|---|---|---|---|---|---|---|---|
| Demographic | Gender | Female † | 468 (16.7%) | 0.159 | 379 (13.6%) | <0.001 | 1949 (69.7%) | <0.001 |
| Male | 93 (14.5%) | 40 (6.2%) | 510 (79.3%) | |||||
| † Pregnancy | Yes | 12 (48.0%) | <0.001 | 4 (16.0%) | 0.720 | 9 (36.0%) | <0.001 | |
| No | 456 (16.5%) | 375 (13.5%) | 1940 (70.0%) | |||||
| Age Group | ≤47 years-old | 344 (19.7%) | <0.001 | 244 (14.0%) | <0.001 | 1156 (66.3%) | <0.001 | |
| >47 years-old | 226 (13.2%) | 176 (10.3%) | 1308 (76.5%) | |||||
| Profession | Medical Professionals | 154 (14.7%) | 0.061 | 80 (7.6%) | <0.001 | 813 (77.7%) | <0.001 | |
| Allied Health Professionals | 416 (17.3%) | 340 (14.1%) | 1651 (68.6%) | |||||
| COVID-19-related Anamnesis | Infection | Yes ‡ | 268 (24.2%) | <0.001 | 180 (16.3%) | <0.001 | 658 (59.5%) | <0.001 |
| No | 302 (12.9%) | 240 (10.2%) | 1806 (76.9%) | |||||
| ‡ Onset | Before 1st Dose | 247 (25.4%) | 0.012 | 155 (16.0%) | 0.451 | 569 (58.6%) | 0.104 | |
| Between Doses | 9 (13.0%) | 0.025 | 16 (23.2%) | 0.108 | 44 (63.8%) | 0.455 | ||
| After 2nd Dose | 12 (18.2%) | 0.237 | 9 (13.6%) | 0.549 | 45 (68.2%) | 0.138 | ||
| ‡ Severity | Asymptomatic | 19 (24.1%) | 0.969 | 9 (11.4%) | 0.222 | 51 (64.6%) | 0.341 | |
| Mild | 163 (24.8%) | 0.611 | 106 (16.1%) | 0.857 | 389 (59.1%) | 0.758 | ||
| Moderate | 81 (23.3%) | 0.641 | 63 (18.2%) | 0.252 | 203 (58.5%) | 0.649 | ||
| Severe | 3 (16.7%) | 0.586 * | 2 (11.1%) | 0.753 * | 13 (72.2%) | 0.267 | ||
| Critical | 2 (50.0%) | 0.249 * | 0 (0%) | 1.000 * | 2 (50.0%) | 1.000 * | ||
| ‡ Signs & Symptoms | Fever | 153 (24.5%) | 0.799 | 94 (15.1%) | 0.215 | 377 (60.4%) | 0.477 | |
| Cough | 133 (24.1%) | 0.915 | 96 (17.4%) | 0.315 | 323 (58.5%) | 0.508 | ||
| Dyspnea | 73 (22.8%) | 0.482 | 53 (16.6%) | 0.869 | 194 (60.6%) | 0.625 | ||
| Fatigue | 210 (24.6%) | 0.581 | 155 (18.2%) | 0.002 | 488 (57.2%) | 0.004 | ||
| Myalgia | 175 (23.9%) | 0.725 | 127 (17.3%) | 0.175 | 430 (58.7%) | 0.477 | ||
| Headache | 176 (25.1%) | 0.353 | 128 (18.3%) | 0.017 | 396 (56.6%) | 0.009 | ||
| Anosmia | 170 (25.6%) | 0.181 | 120 (18.1%) | 0.044 | 373 (56.3%) | 0.007 | ||
| Dysgeusia | 129 (25.2%) | 0.466 | 97 (19.0%) | 0.024 | 285 (55.8%) | 0.019 | ||
| Pharyngitis | 56 (27.7%) | 0.200 | 33 (16.3%) | 0.979 | 113 (55.9%) | 0.255 | ||
| Congestion | 99 (27.1%) | 0.115 | 73 (20.0%) | 0.019 | 193 (52.9%) | 0.002 | ||
| Rhinitis | 102 (28.7%) | 0.018 | 67 (18.8%) | 0.114 | 187 (52.5%) | 0.001 | ||
| Nausea | 36 (22.9%) | 0.681 | 26 (16.6%) | 0.917 | 95 (60.5%) | 0.780 | ||
| Vomiting | 10 (18.2%) | 0.283 | 13 (23.6%) | 0.129 | 32 (58.2%) | 0.839 | ||
| Diarrhea | 43 (21.0%) | 0.228 | 41 (20.0%) | 0.109 | 121 (59.0%) | 0.879 | ||
| Vaccine-related Anamnesis | Vaccinated | Yes Ψ | 422 (12.8%) | <0.001 | 408 (12.4%) | 0.044 | 2457 (74.7%) | <0.001 |
| No | 148 (88.6%) | 12 (7.2%) | 7 (4.2%) | |||||
| Ψ Vaccine Type | BTN162b2 | 349 (11.7%) | <0.001 | 349 (11.7%) | <0.001 | 2282 (76.6%) | <0.001 | |
| mRNA-1273 | 35 (20.0%) | 0.004 | 44 (25.1%) | <0.001 | 96 (54.9%) | <0.001 | ||
| AZD1222 | 11 (12.5%) | 0.923 | 10 (11.4%) | 0.762 | 67 (76.1%) | 0.761 | ||
| Ad26.COV2.S | 27 (61.4%) | <0.001 | 5 (11.4%) | 0.823 | 12 (27.3%) | <0.001 | ||
| Ψ Doses Number | One | 29 (49.2%) | <0.001 | 13 (22.0%) | 0.024 | 17 (28.8%) | <0.001 | |
| Two | 291 (17.8%) | <0.001 | 366 (22.4%) | <0.001 | 976 (59.8%) | <0.001 | ||
| Three | 102 (6.4%) | <0.001 | 29 (1.8%) | <0.001 | 1464 (91.8%) | <0.001 | ||
| Ψ Medical Care | Yes | 48 (42.5%) | <0.001 | 22 (19.5%) | 0.021 | 43 (38.1%) | <0.001 | |
| No | 374 (11.8%) | 386 (12.2%) | 2414 (76.1%) | |||||
| Psychosocial Drivers of COVID-19 Vaccine BD-related Attitudes | Severe Illness | Disagree | 246 (79.6%) | <0.001 | 29 (9.4%) | 0.118 | 34 (11.0%) | <0.001 |
| Not Sure | 111 (29.8%) | <0.001 | 193 (51.7%) | <0.001 | 69 (18.5%) | <0.001 | ||
| Agree | 213 (7.7%) | <0.001 | 198 (7.1%) | <0.001 | 2361 (85.2%) | <0.001 | ||
| Symptomatic Infection | Disagree | 302 (45.6%) | <0.001 | 101 (15.2%) | 0.007 | 260 (39.2%) | <0.001 | |
| Not Sure | 129 (16.3%) | 0.839 | 213 (26.9%) | <0.001 | 451 (56.9%) | <0.001 | ||
| Agree | 139 (7.0%) | <0.001 | 106 (5.3%) | <0.001 | 1753 (87.7%) | <0.001 | ||
| Community Transmission | Disagree | 330 (51.2%) | <0.001 | 124 (19.2%) | <0.001 | 191 (29.6%) | <0.001 | |
| Not Sure | 102 (14.4%) | 0.089 | 190 (26.8%) | <0.001 | 417 (58.8%) | <0.001 | ||
| Agree | 138 (6.6%) | <0.001 | 106 (5.0%) | <0.001 | 1856 (88.4%) | <0.001 | ||
| Mutations Control | Disagree | 111 (18.8%) | 0.093 | 37 (6.3%) | <0.001 | 441 (74.9%) | 0.037 | |
| Not Sure | 77 (12.5%) | 0.003 | 87 (14.1%) | 0.107 | 454 (73.5%) | 0.197 | ||
| Agree | 382 (17.0%) | 0.282 | 296 (13.2%) | 0.013 | 1569 (69.8%) | 0.007 | ||
| Equal Safety | Disagree | 179 (74.3%) | <0.001 | 25 (10.4%) | 0.379 | 37 (15.4%) | <0.001 | |
| Not Sure | 166 (29.1%) | <0.001 | 175 (30.7%) | <0.001 | 229 (40.2%) | <0.001 | ||
| Agree | 225 (8.5%) | <0.001 | 220 (8.3%) | <0.001 | 2198 (83.2%) | <0.001 | ||
| Non-inferior Safety | Disagree | 184 (9.5%) | <0.001 | 118 (6.1%) | <0.001 | 1627 (84.3%) | <0.001 | |
| Not Sure | 232 (21.2%) | <0.001 | 233 (21.3%) | <0.001 | 629 (57.5%) | <0.001 | ||
| Agree | 154 (35.7%) | <0.001 | 69 (16.0%) | 0.009 | 208 (48.3%) | <0.001 | ||
| Risk-benefit Ratio | Disagree | 251 (75.8%) | <0.001 | 27 (8.2%) | 0.019 | 53 (16.0%) | <0.001 | |
| Not Sure | 130 (30.5%) | <0.001 | 206 (48.4%) | <0.001 | 90 (21.1%) | <0.001 | ||
| Agree | 189 (7.0%) | <0.001 | 187 (6.9%) | <0.001 | 2321 (86.1%) | <0.001 | ||
| Self-prioritization | Disagree | 298 (47.7%) | <0.001 | 119 (19.0%) | <0.001 | 208 (33.3%) | <0.001 | |
| Not Sure | 99 (19.4%) | 0.052 | 146 (28.7%) | <0.001 | 264 (51.9%) | <0.001 | ||
| Agree | 173 (7.5%) | <0.001 | 155 (6.7%) | <0.001 | 1992 (85.9%) | <0.001 | ||
| Global Vaccine Justice | Disagree | 360 (34.2%) | <0.001 | 209 (19.9%) | <0.001 | 483 (45.9%) | <0.001 | |
| Not Sure | 123 (9.8%) | <0.001 | 157 (12.5%) | 0.634 | 975 (77.7%) | <0.001 | ||
| Agree | 87 (7.6%) | <0.001 | 54 (4.7%) | <0.001 | 1006 (87.7%) | <0.001 | ||
| National Vaccine Justice | Disagree | 374 (28.8%) | <0.001 | 232 (17.9%) | <0.001 | 691 (53.3%) | <0.001 | |
| Not Sure | 124 (10.8%) | <0.001 | 136 (11.8%) | 0.643 | 893 (77.5%) | <0.001 | ||
| Agree | 72 (7.2%) | <0.001 | 52 (5.2%) | <0.001 | 880 (87.6%) | <0.001 | ||
| Vaccine Satisfaction | Disagree | 227 (16.2%) | 0.650 | 158 (11.2%) | 0.173 | 1020 (72.6%) | 0.175 | |
| Not Sure | 278 (16.5%) | 0.945 | 212 (12.6%) | 0.422 | 1190 (70.8%) | 0.524 | ||
| Agree | 65 (17.6%) | 0.542 | 50 (13.6%) | 0.387 | 254 (68.8%) | 0.261 | ||
| Vaccine Selectivity | Disagree | 220 (20.5%) | <0.001 | 130 (12.1%) | 0.979 | 721 (67.3%) | <0.001 | |
| Not Sure | 255 (15.5%) | 0.135 | 203 (12.3%) | 0.747 | 1186 (72.1%) | 0.320 | ||
| Agree | 95 (12.9%) | 0.003 | 87 (11.8%) | 0.716 | 557 (75.4%) | 0.006 | ||
| Preferred Vaccine | BTN162b2 | 69 (11.3%) | <0.001 | 65 (10.6%) | 0.255 | 477 (78.1%) | <0.001 | |
| mRNA-1273 | 22 (11.4%) | 0.248 | 24 (12.4%) | 0.627 | 147 (76.2%) | 0.573 | ||
| AZD1222 | 5 (23.8%) | 0.187 | 2 (9.5%) | 0.779 | 14 (66.7%) | 0.398 | ||
| Ad26.COV2.S | 27 (47.4%) | <0.001 | 10 (17.5%) | 0.135 | 20 (35.1%) | <0.001 |
| Hesitancy | Acceptance | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Predictor | B (SE) | Wald | OR (CI 95%) | Sig. | Predictor | B (SE) | Wald | OR (CI 95%) | Sig. |
| Female (vs. Male) | 0.86 (0.17) | 24.91 | 2.36 (1.69–3.31) | <0.001 | Male (vs. Female) | 0.51 (0.11) | 23.34 | 1.67 (1.36–2.05) | <0.001 |
| Pregnancy: Yes (vs. No) | 0.20 (0.55) | 0.13 | 1.22 (0.42–3.57) | 0.720 | Pregnancy: No (vs. Yes) | 1.42 (0.42) | 11.55 | 4.15 (1.83–9.43) | <0.001 |
| ≤47 yo (vs. >47 yo) | 0.35 (0.11) | 10.98 | 1.42 (1.15–1.74) | <0.001 | >47 yo (vs. ≤47 yo) | 0.50 (0.08) | 43.63 | 1.66 (1.43–1.92) | <0.001 |
| AHP (vs. Medical) | 0.69 (0.13) | 27.85 | 1.99 (1.54–2.57) | <0.001 | Medical (vs. AHP) | 0.46 (0.09) | 29.01 | 1.59 (1.34–1.88) | <0.001 |
| Infection: Yes (vs. No) | 0.54 (0.11) | 25.38 | 1.71 (1.39–2.10) | <0.001 | Infection: No (vs. Yes) | 0.82 (0.08) | 109.11 | 2.27 (1.95–2.65) | <0.001 |
| Vaccinated: No (vs. Yes) | 0.61 (0.30) | 3.95 | 1.83 (1.01–3.32) | 0.047 | Vaccinated: Yes (vs. No) | 4.22 (0.39) | 228.85 | 67.66 (31.62–144.81) | <0.001 |
| Care: Yes (vs. No) | 0.56 (0.24) | 5.23 | 1.75 (1.08–2.82) | 0.022 | Care: No (vs. Yes) | 1.64 (0.20) | 68.74 | 5.17 (3.51–7.63) | <0.001 |
| Predictor | B (SE) | Wald | AOR (CI 95%) | Sig. |
|---|---|---|---|---|
| Severe Illness: Agree | 3.24 (0.14) | 542.23 | 25.55 (19.45–33.57) | <0.001 |
| Symptomatic Infection: Agree | 1.76 (0.10) | 310.51 | 5.81 (4.78–7.07) | <0.001 |
| Community Transmission: Agree | 2.07 (0.10) | 410.49 | 7.90 (6.47–9.65) | <0.001 |
| Mutations Control: Disagree | 0.27 (0.13) | 4.21 | 1.31 (1.01–1.69) | 0.040 |
| Equal Safety: Agree | 1.99 (0.11) | 350.53 | 7.32 (5.94–9.01) | <0.001 |
| Non-inferior Safety: Disagree | 1.38 (0.10) | 198.93 | 3.97 (3.28–4.81) | <0.001 |
| Risk-benefit Ratio: Agree | 2.97 (0.13) | 565.22 | 19.42 (15.20–24.80) | <0.001 |
| Self-prioritization: Agree | 1.96 (0.10) | 383.86 | 7.10 (5.83–8.63) | <0.001 |
| Global Vaccine Justice: Disagree | −1.46 (0.10) | 226.91 | 0.23 (0.19–0.28) | <0.001 |
| National Vaccine Justice: Disagree | −1.14 (0.09) | 146.96 | 0.32 (0.27–0.39) | <0.001 |
| Vaccine Satisfaction: Agree | 0.06 (0.16) | 0.16 | 1.06 (0.78–1.44) | 0.689 |
| Vaccine Selectivity: Agree | 0.14 (0.11) | 1.49 | 1.15 (0.92–1.44) | 0.223 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klugar, M.; Riad, A.; Mohanan, L.; Pokorná, A. COVID-19 Vaccine Booster Hesitancy (VBH) of Healthcare Workers in Czechia: National Cross-Sectional Study. Vaccines 2021, 9, 1437. https://doi.org/10.3390/vaccines9121437
Klugar M, Riad A, Mohanan L, Pokorná A. COVID-19 Vaccine Booster Hesitancy (VBH) of Healthcare Workers in Czechia: National Cross-Sectional Study. Vaccines. 2021; 9(12):1437. https://doi.org/10.3390/vaccines9121437
Chicago/Turabian StyleKlugar, Miloslav, Abanoub Riad, Lekshmi Mohanan, and Andrea Pokorná. 2021. "COVID-19 Vaccine Booster Hesitancy (VBH) of Healthcare Workers in Czechia: National Cross-Sectional Study" Vaccines 9, no. 12: 1437. https://doi.org/10.3390/vaccines9121437