
Side Effects of COVID-19 Pfizer-BioNTech mRNA Vaccine in Children Aged 12–18 Years in Saudi Arabia

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Population, and Setting
2.2. Ethical Approval
2.3. Sample Size and Statistical Analysis
3. Results
3.1. Characteristics of the Study Participants
3.2. Side Effects Following Vaccinations
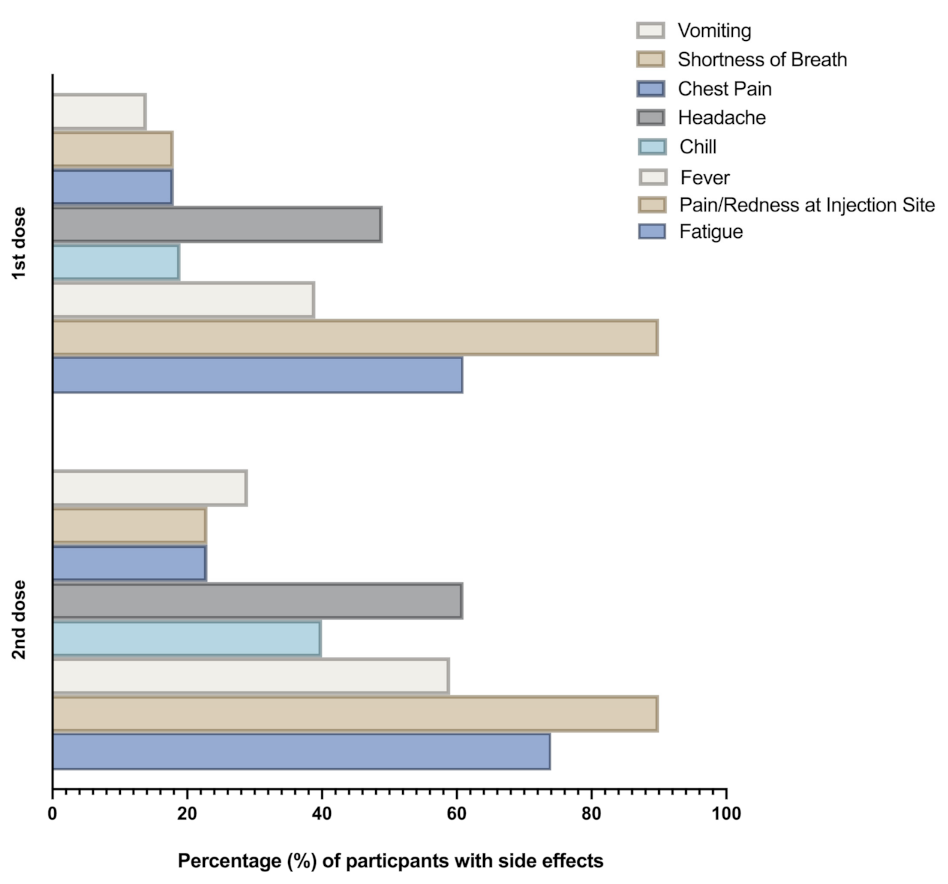
3.3. Comparison of Side Effects Reported Following One- or Two-Dose Vaccinations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- W.H.O. Weekly Epidemiological Update 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---31-august-2021 (accessed on 18 September 2021).
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Tregoning, J.S.; Flight, K.E.; Higham, S.L.; Wang, Z.; Pierce, B.F. Progress of the COVID-19 vaccine effort: Viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat. Rev. Immunol. 2021, 21, 626–636. [Google Scholar] [CrossRef]
- Eurosurveillance Editorial Team. Updated rapid risk assessment from ECDC on the risk related to the spread of new SARS-CoV-2 variants of concern in the EU/EEA—First update. Eurosurveillance 2021, 26, 2101211. [Google Scholar]
- Holmes, E.C.; Goldstein, S.A.; Rasmussen, A.L.; Robertson, D.L.; Crits-Christoph, A.; Wertheim, J.O.; Anthony, S.J.; Barclay, W.S.; Boni, M.F.; Doherty, P.C.; et al. The origins of SARS-CoV-2: A critical review. Cell 2021, 184, 4848–4856. [Google Scholar] [CrossRef] [PubMed]
- De Wit, E.; Van Doremalen, N.; Falzarano, D.; Munster, V.J. SARS and MERS: Recent insights into emerging coronaviruses. Nat. Rev. Genet. 2016, 14, 523–534. [Google Scholar] [CrossRef] [PubMed]
- Masters, P.S. The molecular biology of coronaviruses. Adv. Virus Res. 2006, 66, 193–292. [Google Scholar] [PubMed]
- Fehr, A.R.; Perlman, S. Coronaviruses: An overview of their replication and pathogenesis. Methods Mol. Biol. 2015, 1282, 1–23. [Google Scholar] [PubMed] [Green Version]
- Ashraf, M.; Kim, Y.; Kumar, S.; Seo, D.; Ashraf, M.; Bae, Y.-S. COVID-19 vaccines (revisited) and oral-mucosal vector system as a potential vaccine platform. Vaccines 2021, 9, 171. [Google Scholar] [CrossRef]
- Dai, L.; Gao, G.F. Viral targets for vaccines against COVID-19. Nat. Rev. Immunol. 2020, 21, 73–82. [Google Scholar] [CrossRef]
- Krammer, F. SARS-CoV-2 vaccines in development. Nature 2020, 586, 516–527. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): A review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Our World in Data. Coronavirus (COVID-19) Vaccinations. 2021. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 18 September 2021).
- Assiri, A.; Al-Tawfiq, J.A.; Alkhalifa, M.; Al Duhailan, H.; Al Qahtani, S.; Abu Dawas, R.; El Seoudi, A.A.; Alomran, N.; Abu Omar, O.; Alotaibi, N.; et al. Launching COVID-19 vaccination in Saudi Arabia: Lessons learned, and the way forward. Travel Med. Infect. Dis. 2021, 43, 102119. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health (MOH). MOH Begins Vaccinating 12–18 Age Group with Pfizer Vaccine. 2021. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2021-06-27-008.aspx (accessed on 18 September 2021).
- Saudi Public Health Authority. 2021. Available online: https://covid19.cdc.gov.sa/professionals-health-workers/interim-guidelines-for-the-use-of-sars-cov-2-vaccine/ (accessed on 18 September 2021).
- Tumban, E. Lead SARS-CoV-2 candidate vaccines: Expectations from phase III trials and recommendations post-vaccine approval. Viruses 2020, 13, 54. [Google Scholar] [CrossRef]
- Anand, P.; Stahel, V.P. The safety of Covid-19 mRNA vaccines: A review. Patient Saf. Surg. 2021, 15, 20. [Google Scholar] [CrossRef]
- Mulligan, M.J.; Lyke, K.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Raabe, V.; Bailey, R.; Swanson, K.A.; et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature 2020, 586, 589–593. [Google Scholar] [CrossRef]
- Skowronski, D.M.; De Serres, G. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2021, 384, 1576–1577. [Google Scholar]
- Frenck, R.W., Jr.; Klein, N.P.; Kitchin, N.; Gurtman, A.; Absalon, J.; Lockhart, S.; Perez, J.L.; Walter, E.B.; Senders, S.; Bailey, R.; et al. Safety, immunogenicity, and efficacy of the BNT162b2 Covid-19 vaccine in adolescents. N. Engl. J. Med. 2021, 385, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA Covid-19 vaccine in a nationwide setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef]
- Ossato, A.; Tessari, R.; Trabucchi, C.; Zuppini, T.; Realdon, N.; Marchesini, F. Comparison of medium-term adverse reactions induced by the first and second dose of mRNA BNT162b2 (Comirnaty, Pfizer-BioNTech) vaccine: A post-marketing Italian study conducted between 1 January and 28 February 2021. Eur. J. Hosp. Pharm. 2021. [Google Scholar] [CrossRef]
- Arce, J.S.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.J.; Ansotegui, I.J.; Campbell, D.E.; Cardona, V.; Ebisawa, M.; El-Gamal, Y.; Fineman, S.; Geller, M.; Gonzalez-Estrada, A.; Greenberger, P.A.; et al. COVID-19 vaccine-associated anaphylaxis: A statement of the World Allergy Organization Anaphylaxis Committee. World Allergy Organ. J. 2021, 14, 100517. [Google Scholar] [CrossRef]
- Dal-Ré, R.; Caplan, A.L.; Gluud, C.; Porcher, R. Ethical and scientific considerations regarding the early approval and deployment of a COVID-19 vaccine. Ann. Intern. Med. 2021, 174, 258–260. [Google Scholar] [CrossRef] [PubMed]
- Banerji, A.; Wickner, P.G.; Saff, R.; Stone, C.A.; Robinson, L.B.; Long, A.A.; Wolfson, A.R.; Williams, P.; Khan, D.A.; Phillips, E.; et al. mRNA vaccines to prevent COVID-19 disease and reported allergic reactions: Current evidence and suggested approach. J. Allergy Clin. Immunol. Pract. 2021, 9, 1423–1437. [Google Scholar] [CrossRef] [PubMed]
- Ball, P. The lightning-fast quest for COVID vaccines—And what it means for other diseases. Nature 2021, 589, 16–18. [Google Scholar] [CrossRef]
- Cuschieri, S.; Borg, M.; Agius, S.; Souness, J.; Brincat, A.; Grech, V. Adverse reactions to Pfizer-BioNTech vaccination of healthcare workers at Malta’s state hospital. Int. J. Clin. Pract. 2021, 75, e14605. [Google Scholar] [CrossRef]
- Hagin, D.; Freund, T.; Navon, M.; Halperin, T.; Adir, D.; Marom, R.; Levi, I.; Benor, S.; Freund, N.T. Immunogenicity of Pfizer-BioNTech COVID-19 vaccine in patients with inborn errors of immunity. J. Allergy Clin. Immunol. 2021, 148, 739–749. [Google Scholar] [CrossRef]
- Nittner-Marszalska, M.; Rosiek-Biegus, M.; Kopeć, A.; Pawłowicz, R.; Kosińska, M.; Łata, A.; Szenborn, L. Pfizer-BioNTech COVID-19 vaccine tolerance in allergic versus non-allergic individuals. Vaccines 2021, 9, 553. [Google Scholar] [CrossRef]
- Carli, G.; Nichele, I.; Ruggeri, M.; Barra, S.; Tosetto, A. Deep Vein Thrombosis (DVT) occurring shortly after the second dose of mRNA SARS-CoV-2 vaccine. Intern. Emerg. Med. 2021, 16, 803–804. [Google Scholar] [CrossRef]
- Dionne, A.; Sperotto, F.; Chamberlain, S.; Baker, A.L.; Powell, A.J.; Prakash, A.; Castellanos, D.A.; Saleeb, S.F.; de Ferranti, S.D.; Newburger, J.W.; et al. Association of myocarditis with BNT162b2 messenger RNA COVID-19 Vaccine in a case series of children. JAMA Cardiol. 2021. [Google Scholar] [CrossRef]
- Oliver, S.E.; Gargano, J.W.; Marin, M.; Wallace, M.; Curran, K.G.; Chamberland, M.; McClung, N.; Campos-Outcalt, D.; Morgan, R.L.; Mbaeyi, S. The advisory committee on immunization practices’ interim recommendation for use of Pfizer-BioNTech COVID-19 vaccine—United States, December 2020. MMWR 2020, 69, 1922–1924. [Google Scholar] [PubMed]
- Alhazmi, A.; Alamer, E.; Daws, D.; Hakami, M.; Darraj, M.; Abdelwahab, S.; Maghfuri, A.; Algaissi, A. Evaluation of side effects associated with COVID-19 vaccines in Saudi Arabia. Vaccines 2021, 9, 674. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, K.L.; Fink, A.L.; Plebanski, M.; Klein, S.L. Sex and gender differences in the outcomes of vaccination over the life course. Annu. Rev. Cell Dev. Biol. 2017, 33, 577–599. [Google Scholar] [CrossRef]
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Frieman, M.; Harris, A.D.; Herati, R.S.; Krammer, F.; Mantovani, A.; Rescigno, M.; Sajadi, M.M.; Simon, V. SARS-CoV-2 vaccines for all but a single dose for COVID-19 survivors. EBioMedicine 2021, 68, 103401. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID symptom study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]


{kind=link}
| Manufacturer | Type | Recommended Doses | Targeted Population |
|---|---|---|---|
| Pfizer-BioNTech | mRNA | Two | Adults and children older than 12 years |
| Moderna | mRNA | Two | Adults and children older than 12 years |
| AstraZeneca-Oxford | Viral vector adenovirus | Two | 18 years of age and older |
| Characteristic | Category | Number of Participants n (%) |
|---|---|---|
| Total number of participants | 965 | |
| Gender | Male Female | 460 (48) 505 (52) |
| Age a | 16 ± 2 | |
| Presence of health conditions | Yes No | 97 (10) 868 (90) |
| Diagnosed previously with COVID-19 | Yes | 283 (29) |
| No | 282 (71) | |
| Doses of Pfizer-BioNTech (BNT162b2) vaccine | One Two | 539 (56) 426 (44) |
| Report of at least one side effect after vaccination | Yes No | 571 (60) 394 (40) |
| Variable | Participants with Side Effects, n = 571 (60%) | Participants without Side Effects, n = 394 (40%) | p-Value # |
|---|---|---|---|
| Age, years (Median; SD) | 16;2 | 16;2 | 1 |
| Male, n (%) | 274 (48) | 186 (47) | 0.844 |
| Presence of health conditions, n (%) | 56 (10) | 36 (9) | 0.824 |
| Diagnosed previously with COVID-19, n (%) | 194 (34) | 89 (22) | 0.0001 * |
| Received two doses, n (%) | 273 (48) | 153 (39) | 0.003 * |
| Variable | Participants with Side Effects, n = 571 |
|---|---|
| Timing of side effects | |
| First day | 409 (72%) |
| Second day | 115 (20%) |
| Third day or later | 47 (8%) |
| Duration of the side effects (days) | |
| From 1 to 3 | 369 (65%) |
| From 3 to 5 | 169 (30%) |
| More than 5 | 33 (5%) |
| Taking medication to mitigate side effects | 369 (65%) |
| Visiting a physician due to side effects | 81 (14%) |
| Hospitalization due to side effects | 49 (8%) |
| Variable | Single Dose, n = 298 (52%) | Two Doses, n = 273 (48%) | p-Value # |
|---|---|---|---|
| History of health conditions, n (%) | 28 (9) | 31 (11) | 0.492 |
| History of COVID-19, n (%) | 102 (34) | 92 (34) | 0.930 |
| Male, n (%) | 143 (48) | 131 (48) | 1 |
| Timing of side effects | 0.894 | ||
| First day | 216 | 193 | |
| Second day | 60 | 55 | |
| Third day or later | 22 | 25 | |
| Duration of the side effects (days) | 0.400 | ||
| From 1 to 3 | 200 | 169 | |
| From 3 to 5 | 81 | 88 | |
| More than 5 | 17 | 16 | |
| Fatigue | 181 (61) | 201 (74) | 0.001 * |
| Pain | 269 (90) | 247 (90) | 1 |
| Fever | 116 (39) | 161 (59) | 0.0001 * |
| Chills | 58 (19) | 110 (40) | 0.0001 * |
| Headache | 146 (49) | 168 (61) | 0.003 * |
| Vomiting | 42 (14) | 78 (29) | 0.0001 * |
| Chest pain | 55 (18) | 62 (23) | 0.215 |
| Shortness of breath | 55 (18) | 62 (23) | 0.215 |
| Doctor visit | 35 (12) | 46 (17) | 0.093 |
| Hospitalization | 16 (5) | 33 (12) | 0.004 * |
| Taking medication to mitigate side effects | 166 (56) | 203 (74) | 0.0001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alamer, E.; Alhazmi, A.; Qasir, N.A.; Alamer, R.; Areeshi, H.; Gohal, G.; Qadri, M.; Hashem, A.M.; Algaissi, A. Side Effects of COVID-19 Pfizer-BioNTech mRNA Vaccine in Children Aged 12–18 Years in Saudi Arabia. Vaccines 2021, 9, 1297. https://doi.org/10.3390/vaccines9111297
Alamer E, Alhazmi A, Qasir NA, Alamer R, Areeshi H, Gohal G, Qadri M, Hashem AM, Algaissi A. Side Effects of COVID-19 Pfizer-BioNTech mRNA Vaccine in Children Aged 12–18 Years in Saudi Arabia. Vaccines. 2021; 9(11):1297. https://doi.org/10.3390/vaccines9111297
Chicago/Turabian StyleAlamer, Edrous, Abdulaziz Alhazmi, Naaif A. Qasir, Rahaf Alamer, Halima Areeshi, Gassem Gohal, Marwa Qadri, Anwar M. Hashem, and Abdullah Algaissi. 2021. "Side Effects of COVID-19 Pfizer-BioNTech mRNA Vaccine in Children Aged 12–18 Years in Saudi Arabia" Vaccines 9, no. 11: 1297. https://doi.org/10.3390/vaccines9111297