
COVID-19 Vaccination Behavior of People Living with HIV: The Mediating Role of Perceived Risk and Vaccination Intention


Abstract
:1. Introduction
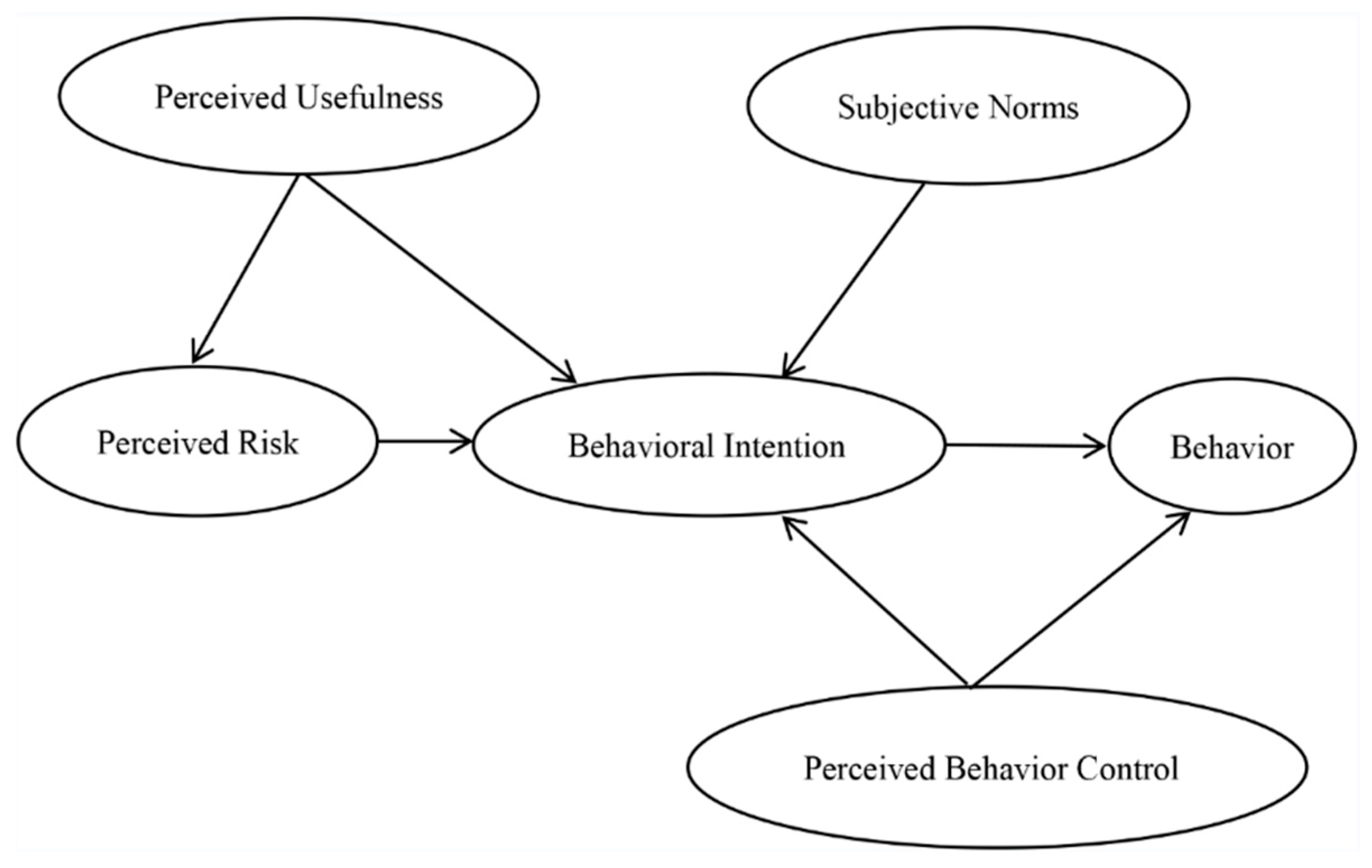
2. Literature Review and Research Hypotheses
3. Methods
3.1. Study Design
3.2. Questionnaire
3.3. Variables and Measurements
3.4. Reliability of the Questionnaire
3.5. Statistical Analysis
3.6. Ethical Considerations
4. Results
4.1. Intention to Get Vaccinated, Vaccination Status, and Participant Characteristics
4.2. The SEM Fitting Index Results
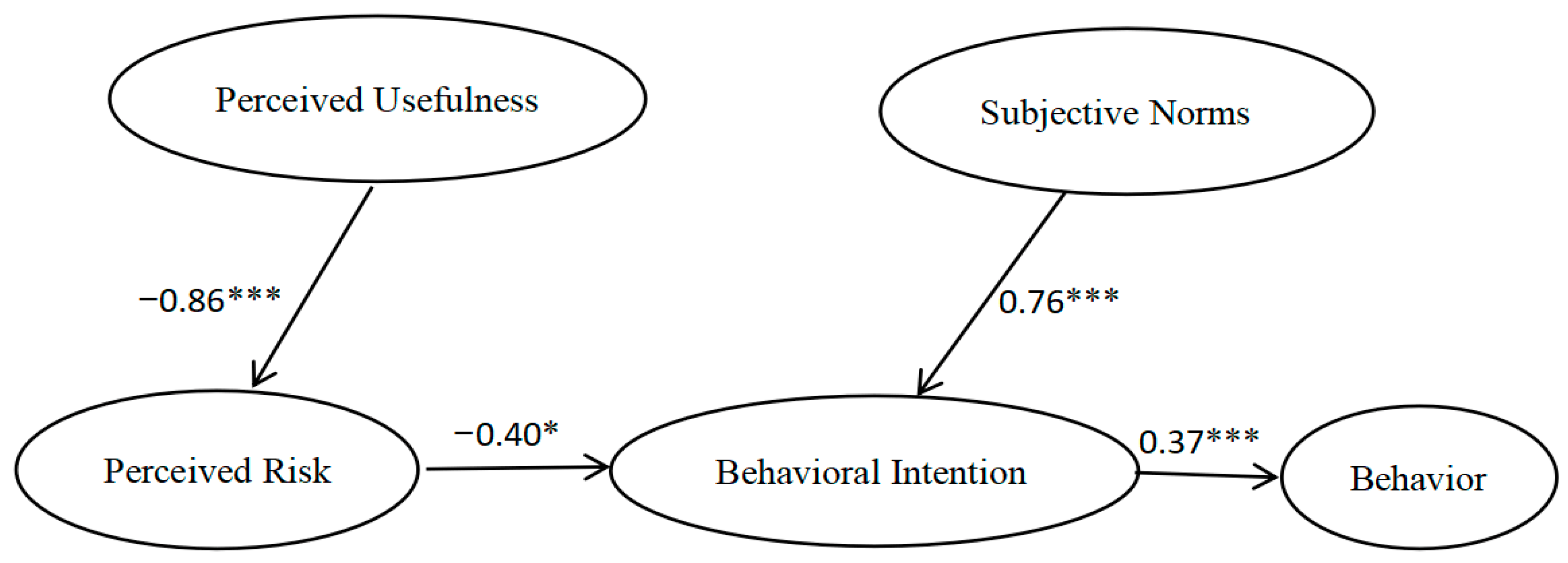
4.3. Model Analysis Results
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PLWH | people living with HIV |
| B | behavior |
| PU | perceived usefulness |
| PR | perceived risk |
| SNs | subjective norms |
| PBC | perceived behavior control |
| BI | behavior intention |
References
- Jin, Y.-M.; Wu, W.-X.; Xiang, W.; Wu, B.; Fu, Z.-W.; Wang, H.-M.; Wu, W.-X.; Su, Q.-J.; Wang, W.-L.; Feng, Y.-G.; et al. Strategy on coping with COVID-19 vaccine hesitancy. China Trop. Med. 2021, 21, 365–369. [Google Scholar]
- Dil, S.; Dil, N.; Maken, Z.H. COVID-19 Trends and Forecast in the Eastern Mediterranean Region with a Particular Focus on Pakistan. Cureus 2020, 12, e8582. [Google Scholar]
- Lobo, A.P.; Cardoso-Dos-Santos, A.C.; Rocha, M.S.; Pinheiro, R.S.; Bremm, J.M.; Macário, E.M.; Oliveira, W.K.; França, G.V.A. COVID-19 epidemic in Brazil: Where are we at? Int. J. Infect. Dis. 2020, 97, 382–385. [Google Scholar] [CrossRef]
- Utamura, M.; Koizumi, M.; Kirikami, S. An epidemiological model considering isolation to predict COVID-19 trends in Tokyo, Japan: Numerical analysis. JMIR Public Health Surveill. 2020, 6, e23624. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease 2019 (COVID-19). Numbers at a Glance. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 9 July 2021).
- Moore, S.; Hill, E.M.; Dyson, L.; Tildesley, M.J.; Keeling, M.J. Modelling optimal vaccination strategy for SARS-CoV-2 in the UK. PLoS Comput. Biol. 2021, 17, e1008849. [Google Scholar] [CrossRef]
- Robertson, E.; Reeve, K.S.; Niedzwiedz, C.L.; Moore, J.; Blake, M.; Green, M.; Katikireddi, S.V.; Benzeval, M.J. Predictors of COVID-19 vaccine hesitancy in the UK household longitudinal study. Brain Behav. Immun. 2021, 4, 41–50. [Google Scholar] [CrossRef]
- Wang, Z.-W.; Li, Z.; Huang, H.-M.; Yang, Z.-C.; Lv, J.-C. Investigation on residents’ awareness of COVID-19 vaccines and vaccination willingness in Guangzhou. Mod. Prev. Med. 2021, 48, 732–737. [Google Scholar]
- Hursh, S.R.; Strickland, J.C.; Schwartz, L.P.; Reed, D.D. Quantifying the impact of public perceptions on vaccine acceptance using behavioral economics. Front. Public Health 2020, 8, 608852. [Google Scholar] [CrossRef]
- Chung, J.Y.; Thone, M.N.; Kwon, Y.J. COVID-19 vaccines: The status and perspectives in delivery points of view. Adv. Drug Deliv. Rev. 2021, 170, 1–25. [Google Scholar] [CrossRef]
- Stern, P.L. The changing face of vaccines and vaccination. Vaccine 2016, 34, 6653–6654. [Google Scholar] [CrossRef] [Green Version]
- Storlie, C.B.; Pollock, B.D.; Rojas, R.L.; Demuth, G.O.; Johnson, P.W.; Wilson, P.M.; Heinzen, E.P.; Liu, H.; Carter, R.E.; Habermann, E.B.; et al. Quantifying the importance of COVID-19 vaccination to our future outlook. Mayo Clin. Proc. 2021, 96, 1890–1895. [Google Scholar] [CrossRef] [PubMed]
- Bureau of Disease Control and Prevention of National Health Commission of the People’s Republic of China. Technical vaccination recommendations for COVID-19 vaccines in China. JOL Chin. Viral Dis. 2021, 11, 161–162. [Google Scholar]
- World Health Organization. HIV/AIDS Fact Sheet; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/news-room/fact-sheets/detail/hiv-aids (accessed on 18 January 2021).
- Mellor, M.M.; Bast, A.C.; Jones, N.R.; Roberts, N.W.; Ordóñez-Mena, J.M.; Reith, A.J.M.; Butler, C.C.; Matthews, P.C.; Dorward, J. Risk of adverse coronavirus disease 2019 outcomes for people living with HIV. AIDS 2021, 35, F1–F10. [Google Scholar] [CrossRef] [PubMed]
- Vallée, A.; Fourn, E.; Majerholc, C.; Touche, P.; Zucman, D. COVID-19 vaccine hesitancy among french people living with HIV. Vaccines 2021, 9, 302. [Google Scholar] [CrossRef]
- Rahimi, B.; Nadri, H.; Lotfnezhad, A.H.; Timpka, T. A systematic review of the technology acceptance model in health informatics. Appl. Clin. Inform. 2018, 9, 604–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mailizar, M.; Burg, D.; Maulina, S. Examining university students’ behavioural intention to use e-learning during the COVID-19 pandemic: An extended TAM model. Educ. Inf. Technol. 2021, 8, 1–21. [Google Scholar]
- Jaspal, R.; Breakwell, G.M. Social support, perceived risk and the likelihood of COVID-19 testing and vaccination: Cross-sectional data from the United Kingdom. Curr. Psychol. 2021, 8, 1–13. [Google Scholar]
- Germani, A.; Buratta, L.; Delvecchio, E.; Gizzi, G.; Mazzeschi, C. Anxiety severity, perceived risk of COVID-19 and individual functioning in emerging adults facing the pandemic. Front. Psychol. 2020, 11, 567505. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- La Barbera, F.; Ajzen, I. Control interactions in the theory of planned behavior: Rethinking the role of subjective norm. Eur. J. Psychol. 2020, 16, 401–417. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.Y.; Kim, G.M.; Kim, E.J. Predictors of entrepreneurial intention of nursing students based on theory of planned behavior. J. Multidiscip. Healthc. 2021, 14, 533–543. [Google Scholar] [CrossRef]
- MacCallum, R.C.; Browne, M.W.; Sugawara, H.M. Power analysis and determination of sample size for covariance structure modeling. Psychol. Methods 1996, 1, 130–149. [Google Scholar] [CrossRef]
- Browne, M.W.; MacCallum, R.C.; Kim, C.T.; Andersen, B.L.; Glaser, R. When fit indices and residuals are incompatible. Psychol. Methods 2002, 7, 403–421. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Bentler, P.M. Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychol. Methods 1998, 3, 424–453. [Google Scholar] [CrossRef]
- Wu, G.-W.; Deng, T.; Zhang, M.-Q.; Li, Z.-N.; Pu, W.-D.; Wang, J.-X. A survey on the attitudes towards COVID-19 vaccination and its’sociological and psychological influencing factors. Chin. J. Clin. Psychol. 2021, 29, 622–625. [Google Scholar]
- Akarsu, B.; Canbay, Ö.D.; Ayhan, B.D.; Aksoy, H.; Fidancı, İ.; Cankurtaran, M. While studies on COVID-19 vaccine is ongoing, the public’s thoughts and attitudes to the future COVID-19 vaccine. Int. J. Clin. Pract. 2021, 75, e13891. [Google Scholar] [CrossRef] [PubMed]
- Ward, J.K.; Alleaume, C.; Patrick, P.W.; The COCONEL Group. The French public’s attitudes to a future COVID-19 vaccine: The politicization of a public health issue. Soc. Sci. Med. 2020, 265, 113414. [Google Scholar] [CrossRef]
- Sun, S.; Lin, D.; Operario, D. Interest in COVID-19 vaccine trials participation among young adults in China: Willingness, reasons for hesitancy, and demographic and psychosocial determinants. Prev. Med. Rep. 2021, 22, 101350. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes toward a potential SARS-CoV-2 vaccine: A survey of U.S. Adults Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Shmueli, L. Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behavior model. BMC Public Health 2021, 21, 804. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, R.; Huang, R.; Cao, Y.; Wang, J.; Feng, D. Influencing factors and their relationships of risk perception and decision-making behaviour of polypharmacy in patients with chronic diseases: A qualitative descriptive study. BMJ Open 2021, 11, e043557. [Google Scholar] [CrossRef]
- Ferrer, R.; Klein, W.M. Risk perceptions and health behavior. Curr. Opin. Psychol. 2015, 5, 85–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, J.A.; Upshur, R.E.G. The granting of emergency use designation to COVID-19 candidate vaccines: Implications for COVID-19 vaccine trials. Lancet Infect. Dis. 2021, 21, e103–e109. [Google Scholar] [CrossRef]
- Wentzell, E.; Racila, A.M. The social experience of participation in a COVID-19 vaccine trial: Subjects' motivations, others' concerns, and insights for vaccine promotion. Vaccine 2021, 39, 2445–2451. [Google Scholar] [CrossRef] [PubMed]
- Byrne, K.A.; Six, S.G.; Anaraky, R.G.; Harris, M.W.; Winterlind, E.L. Risk-taking unmasked: Using risky choice and temporal discounting to explain COVID-19 preventative behaviors. PLoS ONE 2021, 16, e0251073. [Google Scholar] [CrossRef] [PubMed]
- Wouters, O.J.; Shadlen, K.C.; Salcher-Konrad, M.; Pollard, A.J.; Larson, H.J.; Teerawattananon, Y.; Jit, M. Challenges in ensuring global access to COVID-19 vaccines: Production, affordability, allocation, and deployment. Lancet 2021, 397, 1023–1034. [Google Scholar] [CrossRef]
- Guoming, Y.; Ya, Y.; Xuejiao, C. Cognition, willingness and influencing factors of vaccination among residents in China from the perspective of platform. J. Mass Commun. Mon. 2021, 7, 64–72. [Google Scholar]



{kind=link}
{kind=link}
| Research Constructs | Measurement Items |
|---|---|
| PU | 1. You think the COVID-19 vaccine can prevent COVID-19. 2. You think it’s easier to get COVID-19 without vaccination. 3. You think vaccination can benefit you. 4. You think vaccination can benefit others. |
| PR | 1. You think the COVID-19 vaccine is safe. 2. You think the COVID-19 vaccine will have side effects. 3. You think you can be infected with COVID-19, even if you have been vaccinated. 4. You think not vaccinating will have an impact on the people around you. |
| SN | 1. The people around you have been vaccinated. 2. Your family supports your vaccination. 3. You accept your family’s advice regarding the COVID-19 vaccination. 4. You accept your friends’ advice regarding the COVID-19 vaccination. 5. You accept medical workers’ advice regarding the COVID-19 vaccination. 6. You accept the government’s advice regarding the COVID-19 vaccination. 7. You accept the suggestions of media publicity regarding the COVID-19 vaccination. 8. You will get vaccinated after a lot of people have been vaccinated. |
| PBC | 1. You can decide for yourself to get vaccinated. 2. You can choose your own type of vaccine. 3. You can choose your own time for the vaccine. 4. You can choose your own place for the vaccine. |
| BI | 1. You would like to be vaccinated. 2. You support the application of vaccines in PLWH. 3. You will recommend vaccinations to others. |
| All Subjects (n = 350) N(%) | Intention to Get Vaccinated Against COVID-19 | COVID-19 Vaccination Behavior | |||||
|---|---|---|---|---|---|---|---|
| Intend to Get Vaccinated (n = 280) N(%) | Do Not Intend to Get Vaccinated (n = 70) N(%) | p-Value | Vaccinated (n = 153) N(%) | Do Not Vaccinate (n = 197) N(%) | p-Value | ||
| Sociodemographic | |||||||
| Gender | 0.741 | 0.174 | |||||
| Male | 335(95.7) | 269(80.3) | 66(19.7) | 149(44.5) | 186(55.5) | ||
| Female | 15(4.3) | 11(73.3) | 4(26.7) | 4(26.7) | 11(73.3) | ||
| Age group | 0.648 | 0.198 | |||||
| 18–20 | 4(1.1) | 4(100.0) | 0(0.0) | 3(75.0) | 1(25.0) | ||
| 21–30 | 110(31.5) | 88(80.0) | 22(20.0) | 48(43.6) | 62(56.4) | ||
| 31–40 | 141(40.3) | 108(76.6) | 33(23.4) | 60(42.6) | 81(57.4) | ||
| 41–50 | 64(18.3) | 55(85.9) | 9(14.1) | 33(51.6) | 31(48.4) | ||
| 51–60 | 27(7.7) | 22(81.5) | 5(18.5) | 9(33.3) | 18(66.7) | ||
| 61+ | 4(1.1) | 3(75.0) | 1(25.0) | 0(0.0) | 4(100.0) | ||
| Religious belief | 0.454 | 0.718 | |||||
| Religious belief | 41(11.7) | 31(75.6) | 10(24.4) | 19(46.3) | 22(53.7) | ||
| No religious belief | 309(88.3) | 249(80.6) | 60(19.4) | 134(43.4) | 175(56.6) | ||
| Marital status | 0.900 | 0.328 | |||||
| Single | 268(76.6) | 214(79.9) | 54(20.1) | 121(45.1) | 147(54.9) | ||
| Married | 82(23.4) | 66(80.5) | 16(19.5) | 32(39.0) | 50(61.0) | ||
| Income | 0.852 | 0.610 | |||||
| ≤3000 | 141(40.3) | 111(78.7) | 30(21.3) | 57(40.4) | 84(59.6) | ||
| 3001–5000 | 107(30.6) | 85(79.4) | 22(20.6) | 46(43.0) | 61(57.0) | ||
| 5001–10,000 | 74(21.1) | 60(81.1) | 14(18.9) | 36(48.6) | 38(51.4) | ||
| >10,000 | 28(8.0) | 24(85.7) | 4(14.3) | 14(50.0) | 14(50.0) | ||
| Educational level | 0.439 | 0.944 | |||||
| Junior high school and below | 87(24.9) | 70(80.5) | 17(19.5) | 36(41.4) | 51(58.6) | ||
| High school or polytechnic school | 61(17.4) | 46(75.4) | 15(24.6) | 26(42.6) | 35(57.4) | ||
| College or bachelor degree | 186(53.1) | 149(80.1) | 37(19.9) | 84(45.2) | 102(54.8) | ||
| Master degree or above | 16(4.6) | 15(93.8) | 1(6.3) | 7(43.8) | 9(56.3) | ||
| Occupation | 0.130 | 0.742 | |||||
| Medical-related majors | 21(6.0) | 15(71.4) | 6(28.6) | 10(47.6) | 11(52.4) | ||
| Staff of relevant government departments or teacher | 50(14.3) | 45(90.0) | 5(10.0) | 26(52.0) | 24(48.0) | ||
| Worker | 55(15.7) | 45(81.8) | 10(18.2) | 24(43.6) | 31(56.4) | ||
| Farmer | 31(8.9) | 21(67.7) | 10(32.3) | 13(41.9) | 18(58.1) | ||
| Service trades staff | 193(55.1) | 154(79.8) | 39(20.2) | 80(41.5) | 113(58.5) | ||
| HIV related characteristics | |||||||
| Duration of diagnosis | 0.126 | 0.857 | |||||
| ≤5 years | 224(64.0) | 185(82.6) | 39(17.4) | 100(44.6) | 124(55.4) | ||
| 6–10 years | 98(28.0) | 74(75.5) | 24(24.5) | 41(41.8) | 57(58.2) | ||
| 11–15 years | 19(5.4) | 13(68.4) | 6(31.6) | 9(47.4) | 10(52.6) | ||
| 16–20 years | 7(2.0) | 7(100.0) | 0(0.0) | 3(42.9) | 4(57.1) | ||
| >20 years | 2(0.6) | 1(50.0) | 1(50.0) | 0(0.0) | 2(100.0) | ||
| Chronic Disease | 0.418 | 0.119 | |||||
| Chronic disease | 68(19.4) | 52(76.5) | 16(23.5) | 24(35.3) | 44(64.7) | ||
| No chronic disease | 282(80.6) | 228(80.9) | 54(19.1) | 129(45.7) | 153(54.3) | ||
| The side effect of anti-retroviral drugs | 0.201 | 0.091 | |||||
| No side effects | 21(6.0) | 19(90.5) | 2(9.5) | 14(66.7) | 7(33.3) | ||
| Mild side effects | 282(80.6) | 227(80.5) | 55(19.5) | 119(42.2) | 163(57.8) | ||
| Moderate side effects | 47(13.4) | 34(72.3) | 13(27.7) | 20(42.6) | 27(57.4) | ||
| Viral Load | All Subjects (n = 189) N(%) | Intention to Get Vaccinated against COVID-19 | COVID-19 Vaccination Behavior | ||||
|---|---|---|---|---|---|---|---|
| Intend to Get Vaccinated (n = 136) N(%) | Do Not Intend to Get Vaccinated (n = 53) N(%) | p-Value | Vaccinated (n = 77) N(%) | Do Not Vaccinate (n = 112) N(%) | p-Value | ||
| Not detected | 180(95.2) | 131(72.8) | 49(27.2) | 0.458 | 74(41.1) | 106(58.9) | 0.908 |
| detected | 9(4.8) | 5(55.6) | 4(44.4) | 3(33.3) | 6(66.7) | ||
| Hypothesis | Path between | Nonstandard Coefficient | Standardization Coefficient | S.E. | C.R. | p |
|---|---|---|---|---|---|---|
| H1 | PU→PR | −1.049 | −0.857 | 0.147 | −7.137 | *** |
| H2 | PU→BI | 0.074 | 0.055 | 0.306 | 0.242 | 0.809 |
| H3 | PR→BI | −0.448 | −0.404 | 0.085 | −2.025 | 0.043 * |
| H4 | SN→BI | 0.731 | 0.760 | 0.055 | 13.378 | *** |
| H5 | PBC→BI | 0.063 | 0.090 | 0.033 | 1.878 | 0.060 |
| H6 | PBC→B | 0.004 | 0.010 | 0.021 | 0.191 | 0.848 |
| H7 | BI→B | 0.224 | 0.370 | 0.032 | 7.018 | *** |
| Mediation Path | Mediating Effect | Mediating Effect | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| IV | M | DV | Effect Value | SE | Bias-Corrected 95% CI | Percentile 95% CI | |||||
| Lower | Upper | p | Lower | Upper | p | ||||||
| PU | PR | BI | 0.405 | 0.099 | 0.225 | 0.612 | 0.001 | 0.226 | 0.613 | 0.001 | Full |
| PR | BI | B | −0.177 | 0.044 | −0.271 | −0.100 | 0.001 | −0.264 | −0.095 | 0.001 | Full |
| SN | BI | B | 0.287 | 0.061 | 0.161 | 0.396 | 0.001 | 0.155 | 0.394 | 0.001 | Full |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qi, L.; Yang, L.; Ge, J.; Yu, L.; Li, X. COVID-19 Vaccination Behavior of People Living with HIV: The Mediating Role of Perceived Risk and Vaccination Intention. Vaccines 2021, 9, 1288. https://doi.org/10.3390/vaccines9111288
Qi L, Yang L, Ge J, Yu L, Li X. COVID-19 Vaccination Behavior of People Living with HIV: The Mediating Role of Perceived Risk and Vaccination Intention. Vaccines. 2021; 9(11):1288. https://doi.org/10.3390/vaccines9111288
Chicago/Turabian StyleQi, Li, Li Yang, Jie Ge, Lan Yu, and Xiaomei Li. 2021. "COVID-19 Vaccination Behavior of People Living with HIV: The Mediating Role of Perceived Risk and Vaccination Intention" Vaccines 9, no. 11: 1288. https://doi.org/10.3390/vaccines9111288