
Positive Association between Individualism and Vaccination Resistance against COVID-19 Vaccination among Chinese Adults: Mediations via Perceived Personal and Societal Benefits


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Data Collection
2.2. Measurements
2.2.1. Background Information
2.2.2. Vaccination Resistance
2.2.3. PPB of COVID-19 Vaccination
2.2.4. PSB of COVID-19 Vaccination
2.2.5. Individualism
2.3. Data Analysis
3. Results
3.1. Descriptive Statistics
3.2. Factors of Vaccination Resistance
3.3. Correlation Analyses
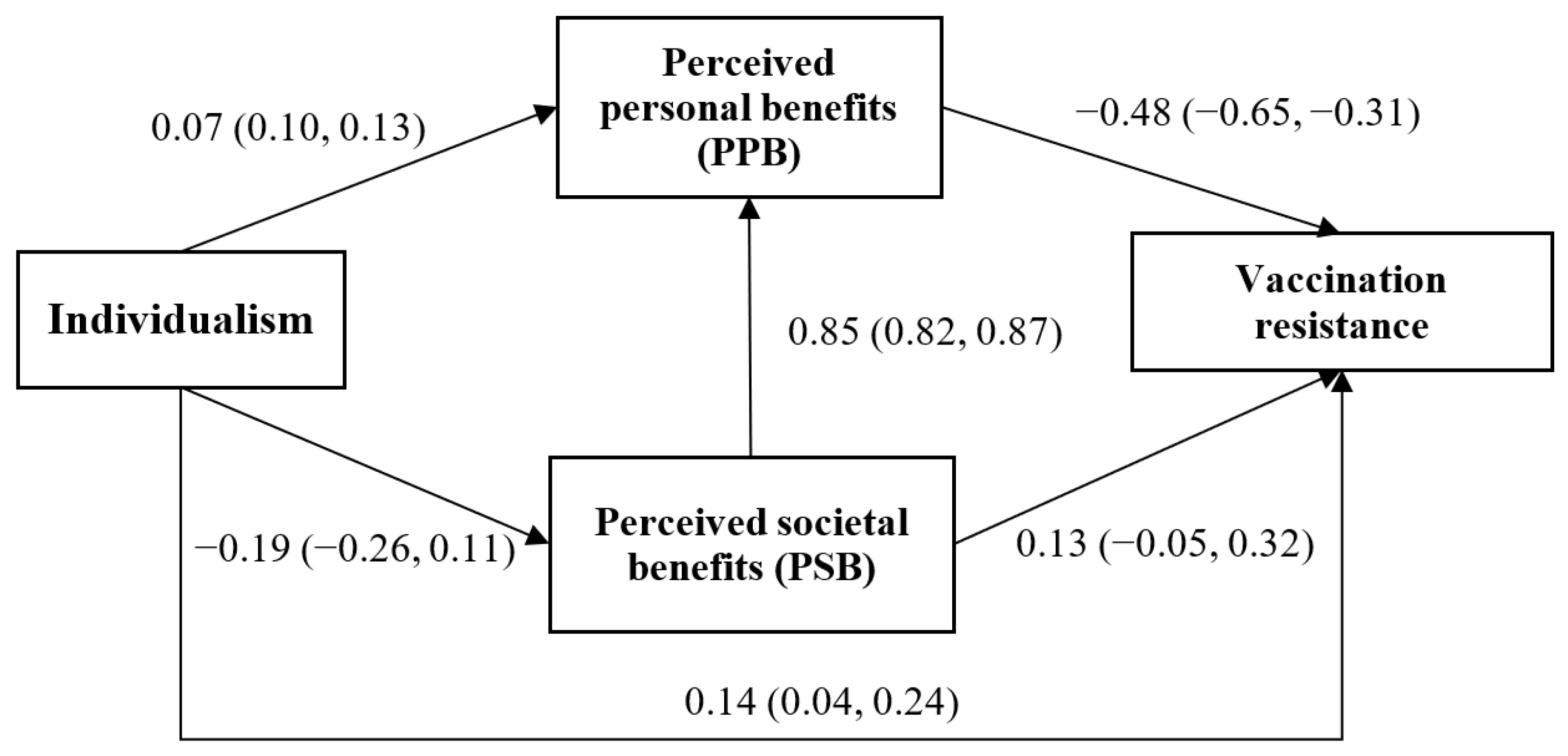
3.4. Path Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cordina, M.; Lauri, M.A.; Lauri, J. Attitudes towards COVID-19 vaccination, vaccine hesitancy and intention to take the vaccine. Pharm. Pract. 2021, 19, 2317. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 1–15. [Google Scholar] [CrossRef]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 vaccination hesitancy in the United States: A rapid national assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 27, 225–228. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; Van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Qunaibi, E.A.; Helmy, M.; Basheti, I.; Sultan, I. A high rate of COVID-19 vaccine hesitancy in a large-scale survey on Arabs. ELife 2021, 10, 68038. [Google Scholar] [CrossRef]
- Bloomberg, Vaccine Tracker. 2021. Available online: https://www.bloomberg.com/graphics/covid-vaccine-tracker-global-distribution/ (accessed on 25 June 2021).
- Yu, Y.; Lau, J.T.; Lau, M.M.; Wong, M.C.; Chan, P.K. Understanding the prevalence and associated factors of behavioral intention of COVID-19 vaccination under specific scenarios combining effectiveness, safety, and cost in the Hong Kong Chinese general population. Int. J. Health Policy Manag. 2021. [Google Scholar] [CrossRef]
- Yu, Y.; Lau, J.T.F.; She, R.; Chen, X.; Li, L.; Li, L.; Chen, X. Prevalence and associated factors of intention of COVID-19 vaccination among healthcare workers in China: Application of the health belief model. Hum. Vaccines Immunother. 2021, 17, 2894–2902. [Google Scholar] [CrossRef]
- Yu, Y.; Lau, M.; Jiang, H.; Lau, J.T. Prevalence and factors of the performed or scheduled COVID-19 vaccination in a Chinese adult general population in Hong Kong. Vaccines 2021, 9, 847. [Google Scholar] [CrossRef]
- Khan, N.; Mahmud, N. Effectiveness of SARS-CoV-2 vaccination in a veterans affairs cohort of inflammatory bowel disease patients with diverse exposure to immunosuppressive medications. Gastroenterology 2021, 161, 827–836. [Google Scholar] [CrossRef]
- Moore, J.; Gilbert, K.; Lively, K.; Laurent, C.; Chawla, R.; Li, C.; Johnson, R.; Petcu, R.; Mehra, M.; Spooner, A.; et al. Correlates of COVID-19 vaccine hesitancy among a community sample of African Americans living in the Southern United States. Vaccines 2021, 9, 879. [Google Scholar] [CrossRef]
- Bono, S.A.; de Moura Villela, E.F.; Siau, C.S.; Chen, W.S.; Pengpid, S.; Hasan, M.T.; Sessou, P.; Ditekemena, J.D.; Amodan, B.O.; Hosseinipour, M.C.; et al. Factors affecting COVID-19 vaccine acceptance: An international survey among low- and middle-income countries. Vaccines 2021, 9, 515. [Google Scholar] [CrossRef] [PubMed]
- Yoda, T.; Katsuyama, H. Willingness to receive COVID-19 vaccination in Japan. Vaccines 2021, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Rieger, M.O. Triggering altruism increases the willingness to get vaccinated against COVID-19. Soc. Health Behav. 2020, 3, 78. [Google Scholar] [CrossRef]
- Yu, Y.; Luo, S.; Mo, P.K.-H.; Wang, S.; Zhao, J.; Zhang, G.; Li, L.; Li, L.; Lau, J.T.-F. Prosociality and social responsibility were associated with intention of COVID-19 vaccination among university students in China. Int. J. Health Policy Manag. 2021. [Google Scholar] [CrossRef]
- Soares, P.; Rocha, J.; Moniz, M.; Gama, A.; Laires, P.; Pedro, A.; Dias, S.; Leite, A.; Nunes, C. Factors associated with COVID-19 vaccine hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef]
- Yigit, M.; Ozkaya-Parlakay, A.; Senel, E. Evaluation of COVID-19 vaccine refusal in parents. Pediatr. Infect. Dis. J. 2021, 40, e134–e136. [Google Scholar] [CrossRef]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 1–15. [Google Scholar] [CrossRef]
- Edwards, B.; Biddle, N.; Gray, M.; Sollis, K. COVID-19 vaccine hesitancy and resistance: Correlates in a nationally representative longitudinal survey of the Australian population. PLoS ONE 2021, 16, e0248892. [Google Scholar] [CrossRef]
- Gul, F.; Pesendorfer, W. Temptation and self-control. Econometrica 2001, 69, 1403–1435. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The health belief model: A decade later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, M.C.S.; Wong, E.L.Y.; Huang, J.; Cheung, A.W.L.; Law, K.; Chong, M.K.C.; Ng, R.W.Y.; Lai, C.K.C.; Boon, S.S.; Lau, J.T.F.; et al. Acceptance of the COVID-19 vaccine based on the health belief model: A population-based survey in Hong Kong. Vaccine 2021, 39, 1148–1156. [Google Scholar] [CrossRef] [PubMed]
- Vayisoglu, S.K.; Zincir, Z. The health action process approach-based program’s effects on Influenza vaccination behavior. J. Nurse Pract. 2019, 15, 517–524. [Google Scholar] [CrossRef]
- She, R.; Chen, X.; Li, L.; Li, L.; Huang, Z.; Lau, J.T. Factors associated with behavioral intention of free and self-paid COVID-19 vaccination based on the social cognitive theory among nurses and doctors in China. Infect. Control. Hosp. Epidemiol. 2021, 1–25. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Ecological Systems Theory; Jessica Kingsley Publishers: London, UK, 1992. [Google Scholar]
- Triandis, H.C. Individualism-collectivism and personality. J. Personal. 2001, 69, 907–924. [Google Scholar] [CrossRef]
- Betsch, C.; Böhm, R. Moral values do not affect prosocial vaccination. Nat. Hum. Behav. 2018, 2, 881–882. [Google Scholar] [CrossRef] [PubMed]
- Mai, Y.; Hu, J.; Yan, Z.; Zhen, S.; Wang, S.; Zhang, W. Structure and function of maladaptive cognitions in Pathological Internet Use among Chinese adolescents. Comput. Hum. Behav. 2012, 28, 2376–2386. [Google Scholar] [CrossRef]
- Biddlestone, M.; Green, R.; Douglas, K.M. Cultural orientation, power, belief in conspiracy theories, and intentions to reduce the spread of COVID-19. Br. J. Soc. Psychol. 2020, 59, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Kwok, K.O.; Li, K.K.; Chan, H.H.H.; Yi, Y.Y.; Tang, A.; Wei, W.I.; Wong, S.Y.S. Community responses during early phase of COVID-19 epidemic, Hong Kong. Emerg. Infect. Dis. 2020, 26, 1575–1579. [Google Scholar] [CrossRef]
- Schneider, C.R.; Dryhurst, S.; Kerr, J.; Freeman, A.L.; Recchia, G.; Spiegelhalter, D.; van der Linden, S. COVID-19 risk perception: A longitudinal analysis of its predictors and associations with health protective behaviours in the United Kingdom. J. Risk Res. 2021, 24, 294–313. [Google Scholar] [CrossRef]
- Castle, C.; Di Guilmi, C.; Stavrunova, O. Individualism and Collectivism as Predictors of Compliance with COVID-19 Public Health Safety Expectations; Working Paper Series; No. 3; Department of Economics: Ultimo, NSW, Australia, 2021. [Google Scholar]
- Yu, Y.; Lau, J.T.F.; Lau, M.M.C. Competing or interactive effect between perceived response efficacy of governmental social distancing behaviors and personal freedom on social distancing behaviors in the Chinese adult general population in Hong Kong. Int. J. Health Policy Manag. 2020. [Google Scholar] [CrossRef] [PubMed]
- Global Protest Tracker. Available online: https://carnegieendowment.org/publications/interactive/protest-tracker (accessed on 15 September 2020).
- S.A.R Government Hong Kong. Together, We Fight the Virus. 2020. Available online: https://www.coronavirus.gov.hk/sim/ (accessed on 27 July 2021).
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Hagger, M.S.; Hankonen, N.; Kangro, E.; Lintunen, T.; Pagaduan, J.; Polet, J.; Ries, F.; Hamilton, K. Trait self-control, social cognition constructs, and intentions: Correlational evidence for mediation and moderation effects in diverse health behaviours. Appl. Psychol. Health Well-Being 2019, 11, 407–437. [Google Scholar] [CrossRef] [Green Version]
- Xia, D.; Li, Y.; He, Y.; Zhang, T.; Wang, Y.; Gu, J. Exploring the role of cultural individualism and collectivism on public acceptance of nuclear energy. Energy Policy 2019, 132, 208–215. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 1–11. [Google Scholar] [CrossRef]
- Suess, C.; Maddock, J.E.; Dogru, T.; Mody, M.; Lee, S. Using the health belief model to examine travelers’ willingness to vaccinate and support for vaccination requirements prior to travel. Tour. Manag. 2022, 88, 104405. [Google Scholar] [CrossRef] [PubMed]
- Guillon, M.; Kergall, P. Factors associated with COVID-19 vaccination intentions and attitudes in France. Public Health 2021, 198, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Triandis, H.C.; Gelfand, M.J. Converging measurement of horizontal and vertical individualism and collectivism. J. Personal. Soc. Psychol. 1998, 74, 118. [Google Scholar] [CrossRef]
- Hsieh, F.Y.; Bloch, D.A.; Larsen, M.D. A simple method of sample size calculation for linear and logistic regression. Stat. Med. 1998, 17, 1623–1634. [Google Scholar] [CrossRef] [Green Version]
- S.A.R Government Hong Kong. Early Vaccination for All, It’s More than a Jab: COVID-19 Vaccination Program. 2021. Available online: https://www.covidvaccine.gov.hk/en/ (accessed on 21 October 2021).
- Wu, C.; Qiao, T.; Qiu, H.; Shi, B.; Bao, Q. Individualism or collectivism: A reinforcement learning mechanism for vaccination decisions. Information 2021, 12, 66. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Norcross, J.C.; DiClemente, C.C. Changing for Good; Avon Books: New York, NY, USA, 1994. [Google Scholar]
- Dietrich, T.; Rundle-Thiele, S.; Kubacki, K. Segmentation in Social Marketing; Springer: Berlin, Germany, 2017; Volume 1. [Google Scholar]
- Luo, S.; Xin, M.; Wang, S.; Zhao, J.; Zhang, G.; Li, L.; Li, L.; Lau, J.T.F. Behavioral intention of receiving COVID-19 vaccination, social media exposures, and peer discussions in China. Epidemiol. Infect. 2021, 149, e158. [Google Scholar] [CrossRef] [PubMed]
- S.A.R Government Hong Kong. Hong Kong Vaccination Dashboard. Available online: https://www.covidvaccine.gov.hk/en/ (accessed on 25 June 2021).


{kind=link}
| n | % | |
|---|---|---|
| Background Factors | ||
| Sex | ||
| Female | 249 | 63.0 |
| Male | 146 | 37.0 |
| Age groups (years) | ||
| 18–50 | 225 | 57.0 |
| 51–75 | 170 | 43.0 |
| Educational attainment | ||
| Below college | 278 | 70.4 |
| College or above | 109 | 27.6 |
| Missing data | 8 | 2.0 |
| Marital status | ||
| Others (single/separated/divorced/w-idowed/cohabited) | 141 | 35.7 |
| Married | 254 | 64.3 |
| Chronic disease status ¶ | ||
| No | 287 | 72.7 |
| Yes | 108 | 27.3 |
| History of influenza vaccination | ||
| No | 303 | 76.7 |
| Yes | 92 | 23.3 |
| Vaccination resistance | ||
| No | 172 | 43.5 |
| Yes | 223 | 56.5 |
| Vaccination Resistance | ||
|---|---|---|
| ORc (95% CI) | ORa (95% CI) | |
| Individualism | 1.04 (1.00, 1.08) * | 1.05 (1.01, 1.09) * |
| Perceived personal benefits (PPB) | 0.51 (0.40, 0.66) *** | 0.40 (0.29, 0.55) *** |
| Perceived societal benefits (PSB) | 0.61 (0.49, 0.75) *** | 0.61 (0.49, 0.76) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, Y.; Lau, M.M.C.; Lau, J.T.-F. Positive Association between Individualism and Vaccination Resistance against COVID-19 Vaccination among Chinese Adults: Mediations via Perceived Personal and Societal Benefits. Vaccines 2021, 9, 1225. https://doi.org/10.3390/vaccines9111225
Yu Y, Lau MMC, Lau JT-F. Positive Association between Individualism and Vaccination Resistance against COVID-19 Vaccination among Chinese Adults: Mediations via Perceived Personal and Societal Benefits. Vaccines. 2021; 9(11):1225. https://doi.org/10.3390/vaccines9111225
Chicago/Turabian StyleYu, Yanqiu, Mason M. C. Lau, and Joseph Tak-Fai Lau. 2021. "Positive Association between Individualism and Vaccination Resistance against COVID-19 Vaccination among Chinese Adults: Mediations via Perceived Personal and Societal Benefits" Vaccines 9, no. 11: 1225. https://doi.org/10.3390/vaccines9111225