
Assessment of Anti-SARS-CoV-2 Antibodies Post-Coronavac Vaccination in the Amazon Region of Brazil

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Studied Samples
2.2. Ethical Aspects
2.3. Antibody Analysis
2.4. Statistical Analysis
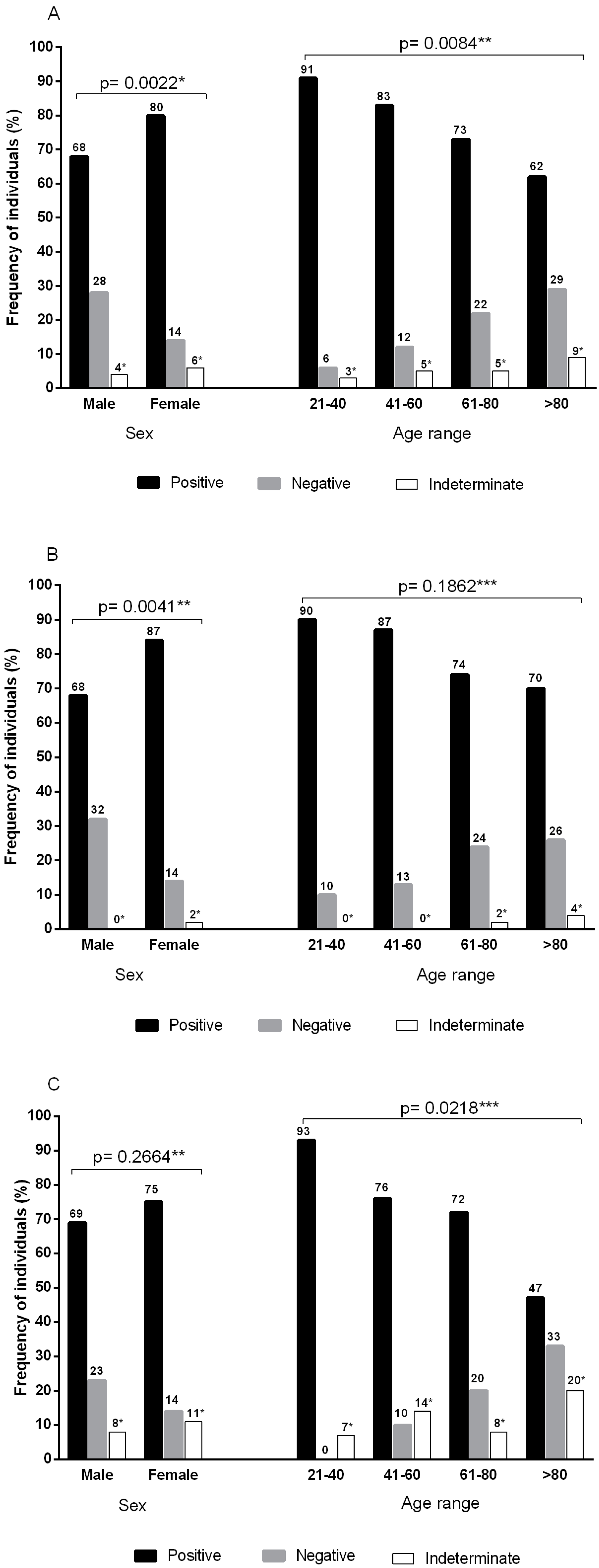
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-2019) Situation Reports. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 27 March 2020).
- Cheng, C.; Wang, H.Y.; Chan, L. Multiple forms of mass anxiety in coronavirus disease-2019 pandemic. J. Affect. Disord. 2021, 291, 338–343. [Google Scholar] [CrossRef]
- Rubin, R. COVID-19 Vaccines vs. Variants-Determining How Much Immunity Is Enough. JAMA 2021, 325, 1241–1243. [Google Scholar] [CrossRef]
- Corey, L.; Mascola, J.R.; Fauci, A.S.; Collins, F.S. A strategic approach to COVID-19 vaccine R&D. Science 2020, 368, 948–950. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Lee, H.K. Delivery Routes for COVID-19 Vaccines. Vaccines 2021, 9, 524. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Gao, Y.; Xiao, M.; Huang, X.; Wu, X. Synthesis and immunological evaluation of synthetic peptide based anti-SARS-CoV-2 vaccine candidates. Chem. Commun. 2021, 57, 1474–1477. [Google Scholar] [CrossRef]
- World Health Organization (WHO). COVID-19 Vaccine Tracker and Landscape. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 7 June 2021).
- Fedele, F.; Aria, M.; Esposito, V.; Micillo, M.; Cecere, G.; Spano, M.; De Marco, G. COVID-19 vaccine hesitancy: A survey in a population highly compliant to common vaccinations. Hum. Vaccin. Immunother. 2021, 7, 1–7. [Google Scholar] [CrossRef]
- Blumental, S.; Debré, P. Challenges and Issues of Anti-SARS-CoV-2 Vaccines. Front. Med. 2021, 8, 664179. [Google Scholar] [CrossRef]
- Zhang, J.; He, Q.; An, C.; Mao, Q.; Gao, F.; Bian, L.; Wu, X.; Wang, Q.; Liu, P.; Song, L.; et al. Boosting with heterologous vaccines effectively improves protective immune responses of the inactivated SARS-CoV-2 vaccine. Emerg. Microbes Infect. 2021, 10, 1598–1608. [Google Scholar] [CrossRef]
- Cerqueira-Silva, T.; de Araújo Oliveira, V.; Pescarini, J.; Bertoldo Júnior, J.; Mota Machado, T.; Flores-Ortiz, R.; Penna, G.; Ichihara, M.Y.; Barros, J.V.; Boaventura, V.S.; et al. Influence of age on the effectiveness and duration of protection in Vaxzevria and CoronaVac vaccines. medRxiv 2021. [Google Scholar] [CrossRef]
- ANVISA. Agencia Nacional de Vigilância Sanitárias. Vacinas—COVID-19. Available online: https://www.gov.br/anvisa/pt-br/assuntos/paf/coronavirus/vacinas (accessed on 7 June 2021).
- Ulhaq, Z.S.; Soraya, G.V.; Zambrano, L.E.A.; Garcia, C.P. Sexual dimorphism in SARS-COV-2 infection. Acta Endocrinol. 2020, 16, 522–523. [Google Scholar] [CrossRef]
- Ciarambino, T.; Para, O.; Giordano, M. Immune system and COVID-19 by sex differences and age. Women’s Health 2021, 17, 17455065211022262. [Google Scholar] [CrossRef]
- Edara, V.V.; Hudson, W.H.; Xie, X.; Ahmed, R.; Suthar, M.S. Neutralizing Antibodies against SARS-CoV-2 Variants after Infection and Vaccination. JAMA 2021, 325, 1896–1898. [Google Scholar] [CrossRef]
- McDonald, J.H. G-test of goodness-of-fit. In Handbook of Biological Statistics, 3rd ed.; Sparky House Publishing: Baltimore, MD, USA, 2014; pp. 53–58. [Google Scholar]
- Instituto Butantan. Vacina Adsorvida COVID-19 (Inativada). Available online: https://vacinacovid.butantan.gov.br/bulas (accessed on 8 June 2020).
- Rogliani, P.; Chetta, A.; Cazzola, M.; Calzetta, L. SARS-CoV-2 Neutralizing Antibodies: A Network Meta-Analysis across Vaccines. Vaccines 2021, 9, 227. [Google Scholar] [CrossRef]
- Tanriover, M.D.; Doğanay, H.L.; Akovam, M.; Güner, H.R.; Azap, A.; Akhan, S.; Köse, Ş.; Erdinç, F.Ş.; Akalın, E.H.; Tabak, Ö.F.; et al. Efficacy and safety of an inactivated whole-virion SARS-CoV-2 vaccine (CoronaVac): Interim results of a double-blind, randomised, placebo-controlled, phase 3 trial in Turkey. Lancet 2021, 398, 213–222. [Google Scholar] [CrossRef]
- Cao, Y.; Yisimayi, A.; Bai, Y.; Huang, W.; Li, X.; Zhang, Z.; Yuan, T.; An, R.; Wang, J.; Xiao, T.; et al. Humoral immune response to circulating SARS-CoV-2 variants elicited by inactivated and RBD-subunit vaccines. Cell Res. 2021, 31, 732–741. [Google Scholar] [CrossRef]
- Wu, Z.; Hu, Y.; Xu, M.; Chen, Z.; Yang, W.; Jiang, Z.; Li, M.; Jin, H.; Cui, G.; Chen, P.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (CoronaVac) in healthy adults aged 60 years and older: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 803–812. [Google Scholar] [CrossRef]
- Omer, S.B.; Yildirim, I.; Forman, H.P. Herd Immunity and Implications for SARS-CoV-2 Control. JAMA 2020, 324, 2095–2096. [Google Scholar] [CrossRef] [PubMed]
- Widge, A.T.; Rouphael, N.G.; Jackson, L.A.; Anderson, E.J.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Durability of Responses after SARS-CoV-2 mRNA-1273 Vaccination. N. Engl. J. Med. 2021, 384, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Jin, S.; An, H.; Zhou, T.; Li, T.; Xie, M.; Chen, S.; Chen, C.; Ying, B.; Xu, Z.; Li, X.; et al. Sex- and age-specific clinical and immunological features of coronavirus disease 2019. PLoS Pathog. 2021, 17, e1009420. [Google Scholar] [CrossRef] [PubMed]
- Grifoni, A.; Weiskopf, D.; Ramirez, S.I.; Mateus, J.; Dan, J.M.; Moderbacher, C.R.; Rawlings, S.A.; Sutherland, A.; Premkumar, L.; Jadi, R.S.; et al. Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals. Cell 2020, 181, 1489–1501.e15. [Google Scholar] [CrossRef] [PubMed]
- Gallais, F.; Velay, A.; Nazon, C.; Wendling, M.J.; Partisani, M.; Sibilia, J.; Candon, S.; Fafi-Kremer, S. Intrafamilial Exposure to SARS-CoV-2 Associated with Cellular Immune Response without Seroconversion, France. Emerg. Infect. Dis. 2021, 27, 113–121. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sample | Vaccine | Test | N | Male | Female | Age (mean/SD) | Reagent (%) | Indeterminate (%) | Negative (%) |
|---|---|---|---|---|---|---|---|---|---|
| Group 1 | Coronavac | Total antibodies | 205 | 77 | 128 | 65.5/14.8 | 159 (77.6%) | 03 (1.5%) | 43 (20.9%) |
| Group 2 | Coronavac | Neutralizing antibodies | 153 | 61 | 93 | 65.4/14.6 | 111 (72.6%) | 15 (9.8%) | 27 (17.6%) |
| Groups 1 and 2 | Coronavac | Total and neutralizing antibodies | 358 | 138 | 220 | 65.4/14.7 | 270 (75.4%) | 18 (5.0%) | 70 (19.6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bichara, C.D.A.; Queiroz, M.A.F.; da Silva Graça Amoras, E.; Vaz, G.L.; Vallinoto, I.M.V.C.; Bichara, C.N.C.; Amaral, I.P.C.d.; Ishak, R.; Vallinoto, A.C.R. Assessment of Anti-SARS-CoV-2 Antibodies Post-Coronavac Vaccination in the Amazon Region of Brazil. Vaccines 2021, 9, 1169. https://doi.org/10.3390/vaccines9101169
Bichara CDA, Queiroz MAF, da Silva Graça Amoras E, Vaz GL, Vallinoto IMVC, Bichara CNC, Amaral IPCd, Ishak R, Vallinoto ACR. Assessment of Anti-SARS-CoV-2 Antibodies Post-Coronavac Vaccination in the Amazon Region of Brazil. Vaccines. 2021; 9(10):1169. https://doi.org/10.3390/vaccines9101169
Chicago/Turabian StyleBichara, Carlos David Araújo, Maria Alice Freitas Queiroz, Ednelza da Silva Graça Amoras, Gergiane Lopes Vaz, Izaura Maria Vieira Cayres Vallinoto, Cléa Nazaré Carneiro Bichara, Isabella Pinheiro Costa do Amaral, Ricardo Ishak, and Antonio Carlos Rosário Vallinoto. 2021. "Assessment of Anti-SARS-CoV-2 Antibodies Post-Coronavac Vaccination in the Amazon Region of Brazil" Vaccines 9, no. 10: 1169. https://doi.org/10.3390/vaccines9101169