Assessing the Long-Term Role of Vaccination against HPV after Loop Electrosurgical Excision Procedure (LEEP): A Propensity-Score Matched Comparison

 , , , , , , , , , ,
, , , , , , , , , ,  , , ,
, , ,  , add
Show full author list
, add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
Statistical Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Burger, E.A.; Portnoy, A.; Campos, N.G.; Sy, S.; Regan, C.; Kim, J.J. Choosing the optimal HPV vaccine: The health impact and economic value of the nonavalent and bivalent HPV vaccines in 48 Gavi-eligible countries. Int. J. Cancer 2020. [Google Scholar] [CrossRef] [PubMed]
- Olsson, S.-E.; Restrepo, J.A.; Reina, J.C.; Pitisuttithum, P.; Ulied, A.; Varman, M.; Van Damme, P.; Moreira, E.D.; Ferris, D.; Block, S.; et al. Long-term immunogenicity, effectiveness, and safety of nine-valent human papillomavirus vaccine in girls and boys 9 to 15 years of age: Interim analysis after 8 years of follow-up. Papillomavirus Res. 2020, 10, 100203. [Google Scholar] [CrossRef] [PubMed]
- Saslow, D.; Ba, K.S.A.; Manassaram-Baptiste, D.; Smith, R.A.; Fontham MPH on behalf of the American Cancer Society Guideline Development Group. Human papillomavirus vaccination 2020 guideline update: American Cancer Society guideline adaptation. CA Cancer J. Clin. 2020, 70, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Baussano, I.; Lazzarato, F.; Ronco, G.; Franceschi, S. Impacts of human papillomavirus vaccination for different populations: A modeling study. Int. J. Cancer 2018, 143, 1086–1092. [Google Scholar] [CrossRef] [PubMed]
- Kulasingam, S.L.; Connelly, L.B.; Conway, E.; Hocking, J.S.; Myers, E.; Regan, D.G.; Roder, D.; Ross, J.; Wain, G. A cost-effectiveness analysis of adding a human papillomavirus vaccine to the Australian National Cervical Cancer Screening Program. Sex. Heal. 2007, 4, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Kang, W.D.; Choi, H.S.; Kim, S.M. Is vaccination with quadrivalent HPV vaccine after loop electrosurgical excision procedure effective in preventing recurrence in patients with high-grade cervical intraepithelial neoplasia (CIN2–3)? Gynecol. Oncol. 2013, 130, 264–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghelardi, A.; Parazzini, F.; Martella, F.; Pieralli, A.; Bay, P.; Tonetti, A.; Svelato, A.; Bertacca, G.; Lombardi, S.; Joura, E.A. SPERANZA project: HPV vaccination after treatment for CIN2+. Gynecol. Oncol. 2018, 151, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Petrillo, M.; Dessole, M.; Tinacci, E.; Saderi, L.; Muresu, N.; Capobianco, G.; Cossu, A.; Dessole, S.; Sotgiu, G.; Piana, A.F. Efficacy of HPV Vaccination in Women Receiving LEEP for Cervical Dysplasia: A Single Institution’s Experience. Vaccines 2020, 8, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sand, F.L.; Kjaer, S.K.; Frederiksen, K.; Dehlendorff, C. Risk of cervical intraepithelial neoplasia grade 2 or worse after conization in relation to HPV vaccination status. Int. J. Cancer 2020, 147, 641–647. [Google Scholar] [CrossRef]
- Paavonen, J.; Naud, P.; Salmerón, J.; Wheeler, C.M.; Chow, S.-N.; Apter, D.; Kitchener, H.; Castellsague, X.; Teixeira, J.C.; Skinner, S.R.; et al. Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by oncogenic HPV types (PATRICIA): Final analysis of a double-blind, randomised study in young women. Lancet 2009, 374, 301–314. [Google Scholar] [CrossRef]
- Bogani, G.; Di Donato, V.; Sopracordevole, F.; Ciavattini, A.; Ghelardi, A.; Lopez, S.; Simoncini, T.; Plotti, F.; Casarin, J.; Serati, M.; et al. Recurrence rate after loop electrosurgical excision procedure (LEEP) and laser Conization: A 5-year follow-up study. Gynecol. Oncol. 2020. [Google Scholar] [CrossRef]
- Bogani, G.; Tagliabue, E.; Ferla, S.; Martinelli, F.; Ditto, A.; Chiappa, V.; Maggiore, U.L.R.; Taverna, F.; Lombardo, C.; Lorusso, D.; et al. Nomogram-based prediction of cervical dysplasia persistence/recurrence. Eur. J. Cancer Prev. 2019, 28, 435–440. [Google Scholar] [CrossRef]
- Bogani, G.; Ditto, A.; Martinelli, F.; Signorelli, M.; Chiappa, V.; Maggiore, U.L.R.; Taverna, F.; Lombardo, C.; Borghi, C.; Scaffa, C.; et al. Artificial intelligence estimates the impact of human papillomavirus types in influencing the risk of cervical dysplasia recurrence. Eur. J. Cancer Prev. 2019, 28, 81–86. [Google Scholar] [CrossRef]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Human Papillomaviruses; International Agency for Research on Cancer: Lyon, France, 2007; Volume 90, pp. 1–636. [Google Scholar]
- Scheller, N.M.; Pasternak, B.; Mølgaard-Nielsen, D.; Svanström, H.; Hviid, A. Quadrivalent HPV Vaccination and the Risk of Adverse Pregnancy Outcomes. N. Engl. J. Med. 2017, 376, 1223–1233. [Google Scholar] [CrossRef] [PubMed]
- Del Pino, M.; Martí, C.; Torras, I.; Henere, C.; Munmany, M.; Marimon, L.; Saco, A.; Torné, A.; Ordi, J. HPV Vaccination as Adjuvant to Conization in Women with Cervical Intraepithelial Neoplasia: A Study under Real-Life Conditions. Vaccines 2020, 8, 245. [Google Scholar] [CrossRef]
- Villa, L.L.; Perez, G.; Kjaer, S.K.; Paavonen, J.; Lehtinen, M.; Munoz, N.; Sigurdsson, K.; Hernandez-Avila, M.; Skjeldestad, F.E.; Thoresen, S.; et al. Quadrivalent Vaccine against Human Papillomavirus to Prevent High-Grade Cervical Lesions. N. Engl. J. Med. 2007, 356, 1915–1927. [Google Scholar] [CrossRef]
- Lehtinen, M.; Paavonen, J.; Wheeler, C.M.; Jaisamrarn, U.; Garland, S.M.; Castellsagué, X.; Skinner, S.R.; Apter, D.; Naud, P.; Salmerón, J.; et al. Overall efficacy of HPV-16/18 AS04-adjuvanted vaccine against grade 3 or greater cervical intraepithelial neoplasia: 4-year end-of-study analysis of the randomised, double-blind PATRICIA trial. Lancet Oncol. 2012, 13, 89–99. [Google Scholar] [CrossRef]
- GISCi. Gruppo Italiano Screening del Cervicocarcinoma. Available online: http://www.gisci.it/ (accessed on 8 June 2020).




{kind=link}
{kind=link}
{kind=link}
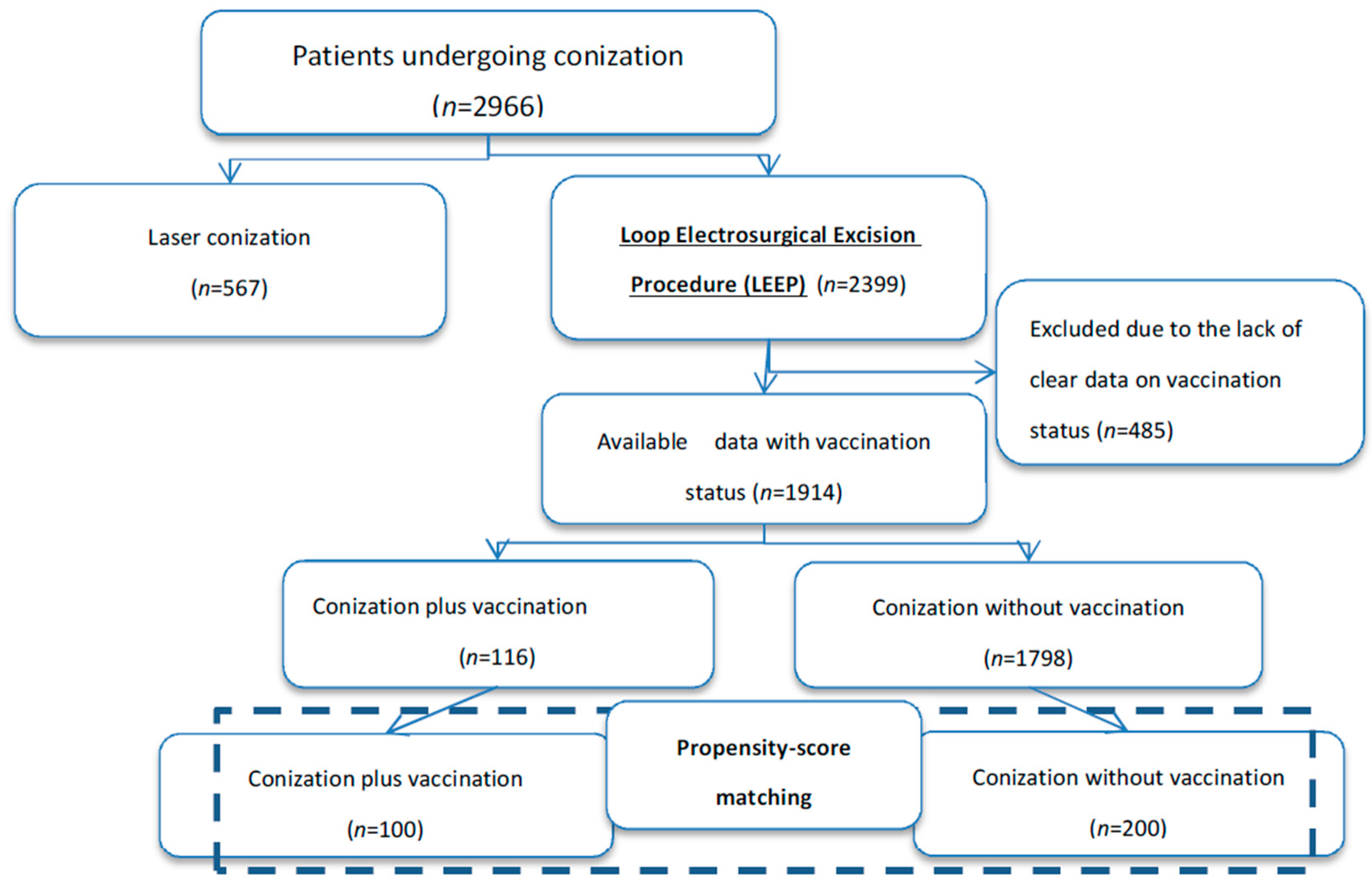
| Characteristics | Whole Study Population (n = 1914) | Conization Plus Vaccination (n = 116) | Conization Alone (n = 1798) | p Value (Vaccinated vs. Not Vaccinated) |
|---|---|---|---|---|
| Age, years | 39 (17–89) | 35 (24–45) | 39 (17–89) | <0.001 |
| Body mass index | 22.85 (14.4–44) | 21 (17–33) | 23 (14.4–44) | <0.001 |
| Menopause | ||||
| No | 1545 (80.7%) | 116 (100%) | 1429 (79.5%) | <0.001 |
| Yes | 369 (19.3%) | // | 369 (20.5%) | |
| Reason for conization | 0.066 | |||
| CIN2 | 827 (43.2%) | 60 (51.7%) | 767 (42.7%) | |
| CIN3 | 1087 (56.8%) | 56 (48.3%) | 1031 (57.3%) | |
| High-risk HPV involved * | <0.001 | |||
| No | 1026 (53.6%) | 41 (35.3%) | 985 (54.8%) | |
| Yes | 888 (46.4%) | 75 (64.7%) | 813 (45.2%) | |
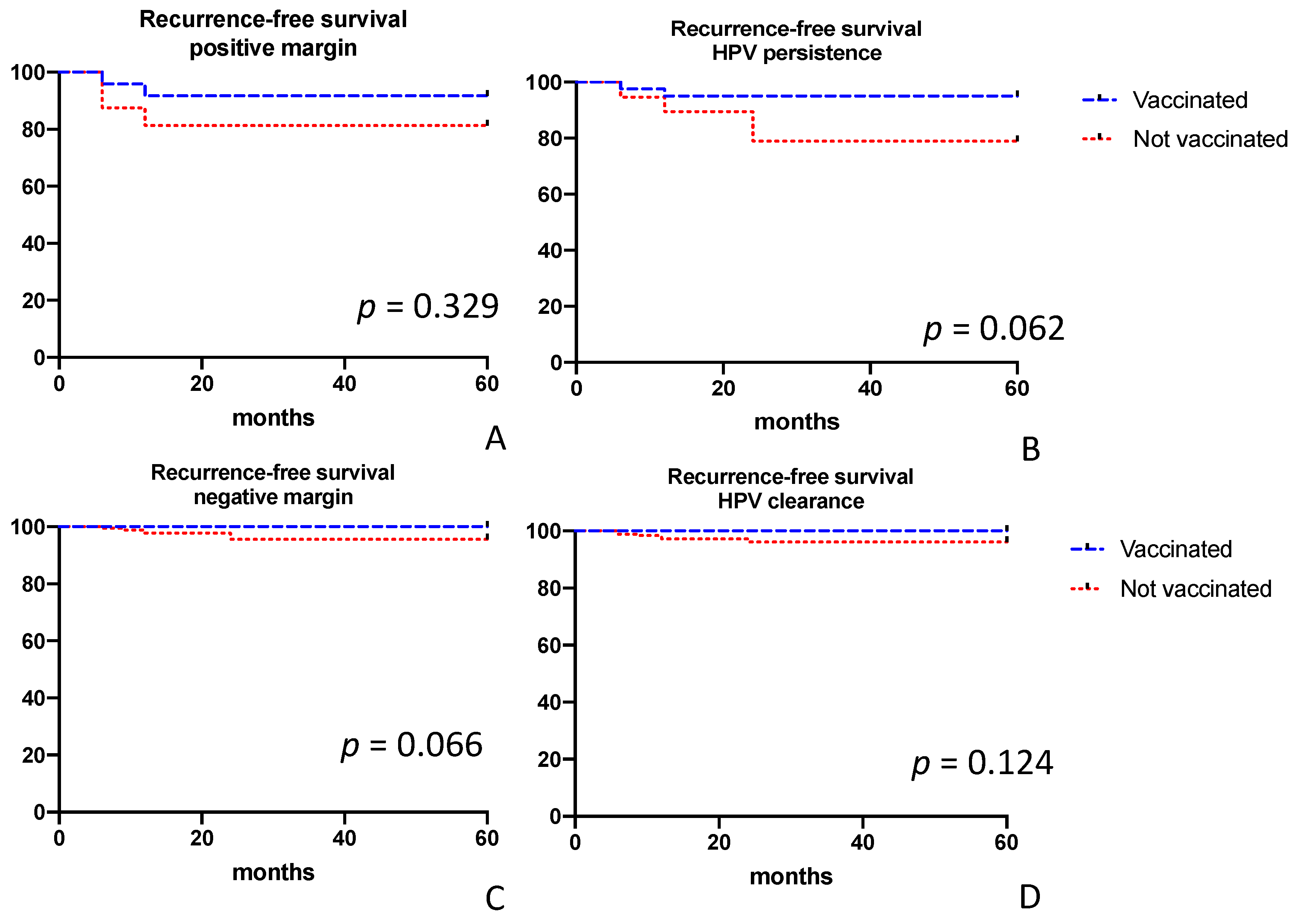
| Positive margins | 189 (9.9%) | 25 (21.5%) | 164 (9.1%) | <0.001 |
| Endocervical | 135 (7%) | 19 (16.4%) | 116 (6.4%) | <0.001 |
| Esocervical | 55 (2.9%) | 6 (5.2%) | 49 (2.7%) | 0.142 |
| HPV persistence ** | ||||
| No | 1053 (55%) | 60 (51.7%) | 993 (55.2%) | 0.501 |
| Yes | 335 (17.5%) | 51 (44%) | 284 (15.8%) | <0.001 |
| Unknown | 526 (27.5%) | 5 (4.3%) | 521(29%) | <0.001 |
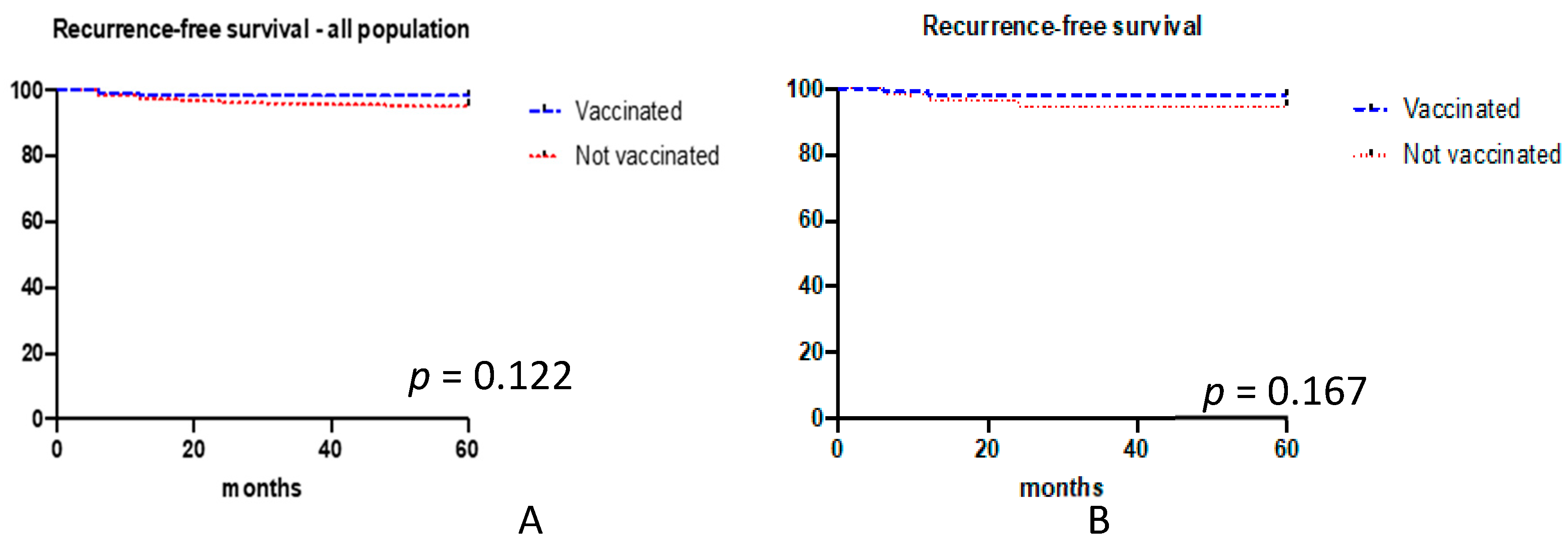
| Recurrence | 104 (5.4%) | 2 (1.7%) | 102 (5.7%) | 0.068 |
| Characteristics | Conization Plus Vaccination (n = 100) | Conization Alone (n = 200) | p Value |
|---|---|---|---|
| Age, years | 33.5 (24–43) | 33.3 (24–44) | 0.895 |
| BMI, kg/mq | 21 (17–33) | 21.1 (17–32.8) | 0.867 |
| Menopause | 1.00 | ||
| No | 100 (100%) | 200 (100%) | |
| Yes | 0 | 0 | |
| HR-HPV detected | 0.895 | ||
| No/Unknown | 31 (31%) | 64 (32%) | |
| Yes | 69 (69%) | 136 (68%) | |
| Not tested | |||
| Type of cervical dysplasia | 0.902 | ||
| CIN2 | 54 (54%) | 106 (53%) | |
| CIN3 | 46 (46%) | 94 (47%) | |
| Positive margins | 1.00 | ||
| No | 76 (76%) | 151 (75.5%) | |
| Yes | 24 (24%) | 49 (24.5%) ** | |
| Type of involved margins | |||
| Endocervical | 18 (18%) | 37 (18.5%) | 1.00 |
| Esocervical | 6 (6%) | 13 (6.5%) | 1.00 |
| HPV persistence * | 0.707 | ||
| No/Unknown | 62 (62%) | 118 (59%) | |
| Yes | 38 (38%) | 82 (41%) | |
| Recurrence/Persistence | |||
| No | 98 (98%) | 189 (94.5%) | 0.231 (yes vs. no) |
| Yes, persistence | 2 (2%) | 2 (1%) | 0.603 (persistence vs no) |
| Yes, recurrence | 0 | 9 (4.5%) | 0.031 (recurrence vs. no) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bogani, G.; Raspagliesi, F.; Sopracordevole, F.; Ciavattini, A.; Ghelardi, A.; Simoncini, T.; Petrillo, M.; Plotti, F.; Lopez, S.; Casarin, J.; et al. Assessing the Long-Term Role of Vaccination against HPV after Loop Electrosurgical Excision Procedure (LEEP): A Propensity-Score Matched Comparison. Vaccines 2020, 8, 717. https://doi.org/10.3390/vaccines8040717
Bogani G, Raspagliesi F, Sopracordevole F, Ciavattini A, Ghelardi A, Simoncini T, Petrillo M, Plotti F, Lopez S, Casarin J, et al. Assessing the Long-Term Role of Vaccination against HPV after Loop Electrosurgical Excision Procedure (LEEP): A Propensity-Score Matched Comparison. Vaccines. 2020; 8(4):717. https://doi.org/10.3390/vaccines8040717
Chicago/Turabian StyleBogani, Giorgio, Francesco Raspagliesi, Francesco Sopracordevole, Andrea Ciavattini, Alessandro Ghelardi, Tommaso Simoncini, Marco Petrillo, Francesco Plotti, Salvatore Lopez, Jvan Casarin, and et al. 2020. "Assessing the Long-Term Role of Vaccination against HPV after Loop Electrosurgical Excision Procedure (LEEP): A Propensity-Score Matched Comparison" Vaccines 8, no. 4: 717. https://doi.org/10.3390/vaccines8040717