Impact of Influenza Vaccination on All-Cause Mortality and Hospitalization for Pneumonia in Adults and the Elderly with Diabetes: A Meta-Analysis of Observational Studies

 ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Study Search and Selection
2.4. Data Retrieval
2.5. Statistical Analyses
2.6. Role of the Funding Source
3. Results
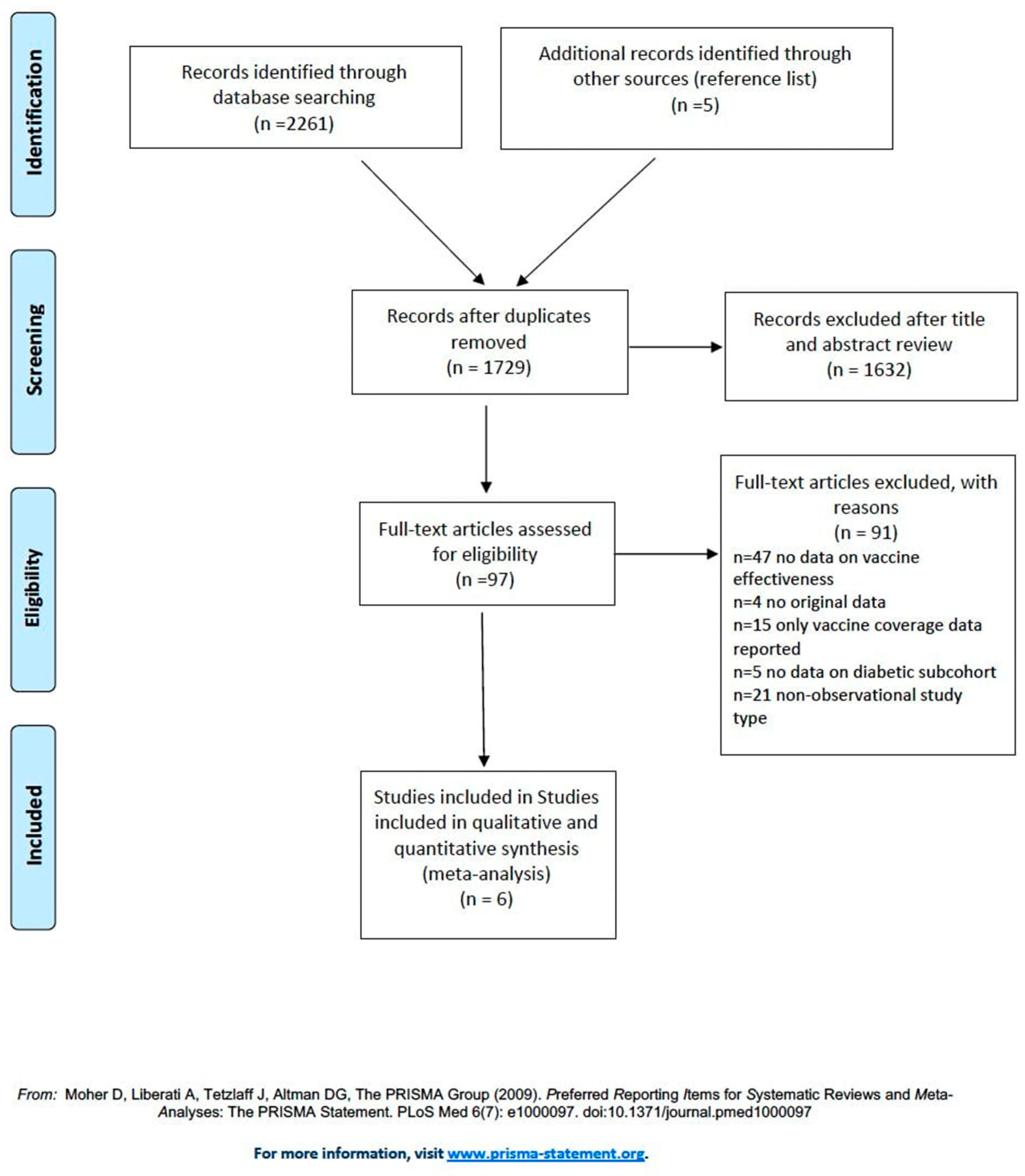
3.1. Studies Selection
3.2. All Cause-Mortality
3.3. Hospitalization for Pneumonia
3.4. Quality of Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Nicholson, K.G.; Wood, J.M.; Zambon, M. Influenza. Lancet 2003, 362, 1733–1745. [Google Scholar] [CrossRef]
- Smeeth, L.; Cook, C.; Thomas, S.; Hall, A.J.; Hubbard, R.; Vallance, P. Risk of deep vein thrombosis and pulmonary embolism after acute infection in a community setting. Lancet 2006, 367, 1075–1079. [Google Scholar] [CrossRef]
- Mertz, D.; Kim, T.H.; Johnstone, J.; Lam, P.P.; Kuster, S.P.; Fadel, S.A.; Tran, D.; Fernandez, E.; Bhatnagar, N.; Loeb, M. Populations at risk for severe or complicated influenza illness: Systematic review and meta-analysis. BMJ 2013, 347, f5061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Background Paper on Influenza Vaccines and Immunization. SAGE Working Group. Available online: https://www.who.int/immunization/sage/meetings/2012/april/1_Background_Paper_Mar26_v13_cleaned.pdf (accessed on 25 January 2020).
- American Diabetes Association. 4. Comprehensive Medical Evaluation and Assessment of Comorbidities: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42 (Suppl. S1), S34–S45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Handelsman, Y.; Bloomgarden, Z.T.; Grunberger, G.; Umpierrez, G.; Zimmerman, R.S.; Bailey, T.S.; Blonde, L.; Bray, G.A.; Cohen, A.J.; Dagogo-Jack, S.; et al. American association of clinical endocrinologists and american college of endocrinology—Clinical practice guidelines for developing a diabetes mellitus comprehensive care plan—2015. Endocr. Pract. 2015, 21 (Suppl. S1), 1–87. [Google Scholar] [CrossRef] [Green Version]
- Italian Standards for Diabetes Mellitus. Available online: https://aemmedi.it/wp-content/uploads/2009/06/AMD-Standard-unico1.pdf (accessed on 8 January 2020).
- Muller, L.M.; Gorter, K.J.; Hak, E.; Goudzwaard, W.L.; Schellevis, F.G.; Hoepelman, A.I.; Rutten, G.E. Increased risk of common infections in patients with type 1 and type 2 diabetes mellitus. Clin. Infect. Dis. 2005, 41, 281–288. [Google Scholar] [CrossRef] [Green Version]
- Calvet, H.M.; Yoshikawa, T.T. Infections in diabetes. Infect. Dis. Clin. North. Am. 2001, 15, 407–421. [Google Scholar] [CrossRef]
- Emerging Risk Factors Collaboration. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N. Engl. J. Med. 2011, 364, 829–841. [Google Scholar] [CrossRef] [Green Version]
- Diepersloot, R.J.; Bouter, K.P.; Beyer, W.E.; Hoekstra, J.B.; Masurel, N. Humoral immune response and delayed type hypersensitivity to influenza vaccine in patients with diabetes mellitus. Diabetologia 1987, 30, 397–401. [Google Scholar] [CrossRef] [Green Version]
- Muszkat, M.; Friedman, G.; Dannenberg, H.D.; Greenbaum, E.; Lipo, M.; Heymann, Y.; Zakay-Rones, Z.; Ben-Yehuda, A. Response to influenza vaccination in community and in nursing home residing elderly: Relation to clinical factors. Exp. Gerontol. 2003, 38, 1199–1203. [Google Scholar] [CrossRef]
- Pozzilli, P.; Gale, E.A.; Visalli, N.; Baroni, M.; Crovari, P.; Frighi, V.; Cavallo, M.G.; Andreani, D. The immune response to influenza vaccination in diabetic patients. Diabetologia 1986, 29, 850–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Madhun, A.S.; Cox, R.J.; Seime, A.; Søvik, O.; Haaheim, L.R. Systemic and local immune responses after parenteral influenza vaccination in juvenile diabetic patients and healthy controls: Results from a pilot study. Vaccine 1998, 16, 156–160. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.; Shea, B.; O’Connel, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. 2013. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 20 February 2020).
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Horsley, T.; Dingwall, O.; Sampson, M. Checking reference lists to find additional studies for systematic reviews. Cochrane Database Syst. Rev. 2011, MR000026. [Google Scholar] [CrossRef]
- Heymann, A.D.; Shapiro, Y.; Chodick, G.; Shalev, V.; Kokia, E.; Kramer, E.; Shemer, J. Reduced hospitalizations and death associated with influenza vaccination among patients with and without diabetes. Diabetes Care 2004, 27, 2581–2584. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Blanco, T.; Vila-Corcoles, A.; de Diego, C.; Ochoa-Gondar, O.; Valdivieso, E.; Bobe, F.; Morro, A.; Herńndez, N.; Martin, A.; Calamote, F.; et al. Relationship between annual influenza vaccination and winter mortality in diabetic people over 65 years. Hum. Vaccines Immunother. 2012, 8, 363–370. [Google Scholar] [CrossRef] [Green Version]
- Schade, C.P.; McCombs, M.A. Influenza immunization and mortality among diabetic Medicare beneficiaries in West Virginia. W. V. Med. J. 2000, 96, 444–448. [Google Scholar]
- Vamos, E.P.; Pape, U.J.; Curcin, V.; Harris, M.J.; Valabhji, J.; Majeed, A.; Millett, C. Effectiveness of the influenza vaccine in preventing admission to hospital and death in people with type 2 diabetes. CMAJ 2016, 188, E342–E351. [Google Scholar] [CrossRef] [Green Version]
- Looijmans-Van den Akker, I.; Verheij, T.J.; Buskens, E.; Nichol, K.L.; Rutten, G.E.; Hak, E. Clinical effectiveness of first and repeat influenza vaccination in adult and elderly diabetic patients. Diabetes Care 2006, 29, 1771–1776. [Google Scholar] [CrossRef] [Green Version]
- Wang, I.K.; Lin, C.L.; Chang, Y.C.; Lin, P.C.; Liang, C.C.; Liu, Y.L.; Chang, C.T.; Yen, T.H.; Huang, C.C.; Sung, F.C. Effectiveness of influenza vaccination in elderly diabetic patients: A retrospective cohort study. Vaccine 2013, 31, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Remschmidt, C.; Wichmann, O.; Harder, T. Vaccines for the prevention of seasonal influenza in patients with diabetes: Systematic review and meta-analysis. BMC Med. 2015, 13, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasparini, R.; Amicizia, D.; Lai, P.L.; Rossi, S.; Panatto, D. Effectiveness of adjuvanted seasonal influenza vaccines (Inflexal V® and Fluad®) in preventing hospitalization for influenza and pneumonia in the elderly: A matched case-control study. Hum. Vaccines Immunother. 2013, 9, 144–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selvais, P.L.; Hermans, M.P.; Donckier, J.E.; Buysschaert, M. Reported rates, incentives, and effectiveness of major vaccinations in 501 attendees at two diabetes clinics. Diabetes Care 1997, 20, 1212–1213. [Google Scholar] [CrossRef] [PubMed]
- Hak, E.; Nordin, J.; Wei, F.; Mullooly, J.; Poblete, S.; Strikas, R.; Nichol, K.L. Influence of high-risk medical conditions on the effectiveness of influenza vaccination among elderly members of 3 large managed-care organizations. Clin. Infect. Dis. 2002, 35, 370–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colquhoun, A.J.; Nicholson, K.G.; Botha, J.L.; Raymond, N.T. Effectiveness of influenza vaccine in reducing hospital admissions in people with diabetes. Epidemiol. Infect. 1997, 119, 335–341. [Google Scholar] [CrossRef]
- Lau, D.; Eurich, D.T.; Majumdar, S.R.; Katz, A.; Johnson, J.A. Effectiveness of influenza vaccination in working-age adults with diabetes: A population-based cohort study. Thorax 2013, 68, 658–663. [Google Scholar] [CrossRef] [Green Version]
- Isotani, H. Use of influenza vaccine in patients with diabetes, particularly those with complications of cardiac or renal disease. Intern. Med. 2000, 39, 862. [Google Scholar] [CrossRef] [Green Version]
- Jefferson, T.; Rivetti, D.; Rivetti, A.; Rudin, M.; Di Pietrantonj, C.; Demicheli, V. Efficacy and effectiveness of influenza vaccines in elderly people: A systematic review. Lancet 2005, 366, 1165–1174. [Google Scholar] [CrossRef]
- Clar, C.; Oseni, Z.; Flowers, N.; Keshtkar-Jahromi, M.; Rees, K. Influenza vaccines for preventing cardiovascular disease. Cochrane Database Syst. Rev. 2015, 5, CD005050. [Google Scholar] [CrossRef] [Green Version]
- Hulme, K.D.; Gallo, L.A.; Short, K.R. Influenza Virus and Glycemic Variability in Diabetes: A Killer Combination? Front. Microbiol. 2017, 8, 861. [Google Scholar] [CrossRef] [PubMed]
- Bechini, A.; Lorini, C.; Zanobini, P.; Mandò Tacconi, F.; Boccalini, S.; Grazzini, M.; Bonanni, P.; Bonaccorsi, G. Utility of Healthcare System-Based Interventions in Improving the Uptake of Influenza Vaccination in Healthcare Workers at Long-Term Care Facilities: A Systematic Review. Vaccines 2020, 8, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonanni, P.; Boccalini, S.; Zanobini, P.; Dakka, N.; Lorini, C.; Santomauro, F.; Bechini, A. The appropriateness of the use of influenza vaccines: Recommendations from the latest seasons in Italy. Hum. Vaccines Immunother. 2018, 14, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Sarría-Santamera, A.; Timoner, J. Influenza vaccination in old adults in Spain. Eur. J. Public Health 2003, 13, 133–137. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-García, R.; Mayo-Montero, E.; Hernández-Barrera, V.; Garrido, P.C.; Martinez-Hernandez, D.; de Miguel, A.G. Influenza vaccination among diabetic adults: Related factors and trend from 1993 to 2001 in Spain. Diabetes Care 2005, 28, 2031–2033. [Google Scholar] [CrossRef] [Green Version]
- Mereckiene, J.; Cotter, S.; Nicoll, A.; Lopalco, P.; Noori, T.; VENICE project gatekeepers group. Seasonal influenza immunisation in Europe. Overview of recommendations and vaccination coverage for three seasons: Pre-pandemic (2008/09), pandemic (2009/10) and post-pandemic (2010/11). Eurosurveillance 2014, 19, 20780. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention (CDC). Influenza and pneumococcal vaccination levels among adults aged > or = 65 years—United States, 1997. MMWR Morb. Mortal. Wkly. Rep. 1998, 47, 797–802. [Google Scholar]
- Kaufman, Z.; Green, M.S. Compliance with influenza and pneumococcal vaccinations in Israel, 1999–2002. Public Health Rev. 2003, 31, 71–79. [Google Scholar]
- Li, Y.C. Absence of influenza vaccination among high-risk older adults in Taiwan. BMC Public Health 2010, 10, 603. [Google Scholar] [CrossRef] [Green Version]
- Casanova, L.; Cortaredona, S.; Gaudart, J.; Launay, O.; Vanhems, P.; Villani, P.; Verger, P. Effectiveness of seasonal influenza vaccination in patients with diabetes: Protocol for a nested case-control study. BMJ Open 2017, 7, e016023. [Google Scholar] [CrossRef] [Green Version]
- Mann, J.I.; De Leeuw, I.; Hermansen, K.; Karamanos, B.; Karlström, B.; Katsilambros, N.; Diabetes and Nutrition Study Group (DNSG) of the European Association. Evidence-based nutritional approaches to the treatment and prevention of diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2004, 14, 373–394. [Google Scholar] [CrossRef]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; American Diabetes Association (ADA); European Association for the Study of Diabetes (EASD). Management of hyperglycemia in type 2 diabetes: A patient-centered approach: Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2012, 35, 1364–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rydén, L.; Grant, P.J.; Anker, S.D.; Berne, C.; Cosentino, F.; Danchin, N. ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD: The Task Force on diabetes, pre-diabetes, and cardiovascular diseases of the European Society of Cardiology (ESC) and developed in collaboration with the European Association for the Study of Diabetes (EASD). Eur. Heart J. 2013, 34, 3035–3087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerra, N.; Pestal, K.; Juarez, T.; Beck, J.; Tkach, K.; Wang, L.; Raulet, D.H. A selective role of NKG2D in inflammatory and autoimmune diseases. Clin. Immunol. 2013, 149, 432–439. [Google Scholar] [CrossRef] [Green Version]
- Macroepidemiology of Influenza Vaccination (MIV) Study Group. The macro-epidemiology of influenza vaccination in 56 countries, 1997–2003. Vaccine 2005, 23, 5133–5143. [Google Scholar] [CrossRef]


{kind=link}
| Author | Study Design and Period | Country | Age in Years (Mean/Range) | Male (%) | Identification of Diabetic Patient and Data Source | Circulating Influenza (Sub)Strains | Study Size (n) |
|---|---|---|---|---|---|---|---|
| Cohort studies | |||||||
| Heymann, 2004 [19] | Retrospective, 2000/2001 | Israel | Vacc 1., 72.8 Non vacc., 73.1 | Vacc. 51.8 Non vacc 42.1 | International Classification of Diseases (ICD)-9 codes, diabetes register of healthcare service | Not reported | 16,383 |
| Rodriguez-Blanco, 2012 [20] | Retrospective, 2002–2005 | Spain | Vacc., 75.2 Non Vacc 73.1 | Vacc., 39.8 Non vacc., 42.2 | ICD-9 codes, clinical records | A(H3N2) | 2650 |
| Shade, 2000 [21] | Retrospective, 1996–1998 | US | 65 to 114 years | Not reported | ICD-9 codes, hospital discharge | Not reported | 26,443 in 96/97 23,839 in 97/98 |
| Vamos, 2016 [22] | Retrospective 2003–2010 | England | Vacc., 66.0 Non vacc., 56.2 | Vacc., 53.9 Non vacc., 54.2 | ICD-10 codes, hospital admissions | A(H1N1) pdm09 | 124,503 |
| Case-control studies | |||||||
| Looijmans, 2006 [23] | Nested, 1999/2000 | Netherlands | Cases, 68.1 Controls 69.8 | Cases 51.6 Controls 38.3 | International Classification of Primary Care (ICPC) codes, GPs | A(H3N2) | 1753 (192 cases, 1561 controls) |
| Wang, 2013 [24] | Nested, 2001–2009 | Taiwan | Vacc., 73.1 Non vacc. 73.2 | Vacc., 50.0 Non vacc., 49.5 | ICD-9 codes, NHRI-database | Not reported | 9025, (4571 vacc., 4454 non vacc.) |
| Cohort Study | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Author, Year | Selection | Comparability | Outcome | Total Quality Score | ||||||
| Representativeness of the Exposed Cohort | Selection of the Non-Exposed Cohort | Ascertainment of Exposure | Demonstration that Outcome of Interest Was not Present at Start of Study | Main Factor | Additional Factor | Assessment of Outcome with Independency | Adequacy of Follow up Length (to Asses Outcome) | Loss to Follow up Acceptable (Less than 10% and Reported) | ||
| Heymann, 2004 [19] | * | * | * | * | * | * | 6/9 | |||
| Rodriguez-Blanco, 2012 [20] | * | * | * | * | * | * | * | * | * | 9/9 |
| Shade, 2000 [21] | * | * | * | * | 4/9 | |||||
| Vamos, 2016 [22] | * | * | * | * | * | * | * | * | * | 9/9 |
| Case-Control Study | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Author, Year | Selection | Comparability | Exposure | Total Quality Score | ||||||
| The Case Definition Adequate | Representative Series of Cases | Selection of Controls | Definition of Controls | Main Factor | Additional Factor | Ascertainment of Exposure Using Secure Records | Ascertainment of Exposure Using the Same Method for Cases and Controls | Ascertainment of Exposure with Non-Response Rate for Both Groups | ||
| Looijmans, 2006 [23] | * | * | * | * | * | * | * | * | * | 9/9 |
| Wang, 2013 [24] | * | * | * | * | * | * | * | * | * | 9/9 |
| Study Name | Statistics for Each Study | Rate Ratio and 95% IC | ||||
| Rate Ratio | Lower Limit | Upper Limit | Z-Value | p-Value |  Favors Vaccination Favors Non-Vaccination | |
| Heymann, 2004 [19] | 0.33 | 0.25 | 0.43 | −8.41 | 0.00 | |
| Looijmans, 2006 [23] | 0.56 | 0.32 | 0.97 | −2.06 | 0.04 | |
| Rodriguez-Blanco, 2012 [20] | 0.78 | 0.53 | 1.15 | −1.24 | 0.21 | |
| Shade, 2000 [21] | 0.54 | 0.50 | 0.58 | −16.08 | 0.00 | |
| Vamos, 2016 [22] | 0.85 | 0.80 | 0.90 | −5.13 | 0.00 | |
| Wang, 2013 [24] | 0.39 | 0.32 | 0.48 | −9.10 | 0.00 | |
| Overall | 0.54 | 0.40 | 0.74 | −3.84 | 0.00 | |
| Study Name | Statistics for Each Study | Rate Ratio and 95% IC | ||||
| Rate Ratio | Lower Limit | Upper Limit | Z-Value | p-Value |  Favors Vaccination Favors Non-Vaccination | |
| Heymann, 2004 [19] | 0.83 | 0.75 | 0.92 | −3.34 | 0.01 | |
| Looijmans, 2006 [23] | 0.70 | 0.47 | 1.03 | −0.80 | 0.072 | |
| Vamos, 2016 [22] | 0.97 | 0.91 | 1.04 | −0.77 | 0.00 | |
| Wang, 2013 [24] | 0.88 | 0.78 | 0.99 | −2.20 | 0.00 | |
| Overall | 0.89 | 0.80 | 0.98 | −2.36 | 0.00 | |
| Certainty Assessment | N° of Patients | Effect | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Influenza Vaccine | No Vaccine | Relative (95% CI) | Absolute (95% CI) | ||
| All-cause mortality | ||||||||||||
| 6 | Observational studies | Serious a | Very serious b | Not serious | Not serious | Strong association all plausible residual confounding would reduce the demonstrated effect | 3545/108241 (3.3%) | 5195/88837 (5.8%) | OR 0.54 (0.40 to 0.74) | 26 fewer per 1.000 (from 34 fewer to 15 fewer) |  MODERATE | CRITICAL |
| Hospitalization for pneumonia | ||||||||||||
| 4 | Observational studies | Serious a | Very serious b | Not serious | Not serious | Strong association all plausible residual confounding would reduce the demonstrated effect | 3203/83990 (3.8%) | 2702/57038 (4.7%) | OR 0.89 (0.80 to 0.98) | 5 fewer per 1.000 (from 9 fewer to 1 fewer) | MODERATE | IMPORTANT |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bechini, A.; Ninci, A.; Del Riccio, M.; Biondi, I.; Bianchi, J.; Bonanni, P.; Mannucci, E.; Monami, M. Impact of Influenza Vaccination on All-Cause Mortality and Hospitalization for Pneumonia in Adults and the Elderly with Diabetes: A Meta-Analysis of Observational Studies. Vaccines 2020, 8, 263. https://doi.org/10.3390/vaccines8020263
Bechini A, Ninci A, Del Riccio M, Biondi I, Bianchi J, Bonanni P, Mannucci E, Monami M. Impact of Influenza Vaccination on All-Cause Mortality and Hospitalization for Pneumonia in Adults and the Elderly with Diabetes: A Meta-Analysis of Observational Studies. Vaccines. 2020; 8(2):263. https://doi.org/10.3390/vaccines8020263
Chicago/Turabian StyleBechini, Angela, Alessandra Ninci, Marco Del Riccio, Ilaria Biondi, Jacopo Bianchi, Paolo Bonanni, Edoardo Mannucci, and Matteo Monami. 2020. "Impact of Influenza Vaccination on All-Cause Mortality and Hospitalization for Pneumonia in Adults and the Elderly with Diabetes: A Meta-Analysis of Observational Studies" Vaccines 8, no. 2: 263. https://doi.org/10.3390/vaccines8020263