
The Bacterial Meningitis Epidemic in Banalia in the Democratic Republic of Congo in 2021
 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Setting
2.2. Meningitis Surveillance
2.3. Laboratory Confirmation
2.4. Public Health Response
2.5. Data Collection and Statistical Analysis
2.6. Ethics Considerations
3. Results
3.1. Outbreak Detection, Investigation, and Spread
3.2. Laboratory Confirmation
3.3. Case Management
3.4. Psychological Support
3.5. Infection Prevention Control
3.6. Reactive Immunization
3.7. Coordination, Monitoring, and Evaluation
3.8. Risk Communication and Community Engagement
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Meningitis. Available online: https://www.who.int/health-topics/meningitis#tab=tab_1 (accessed on 1 March 2023).
- World Health Organization. Meningococcal Meningitis. Available online: https://www.who.int/teams/health-product-policy-and-standards/standards-and-specifications/vaccine-standardization/meningococcal-meningitis#:~:text=N.,particularly%20in%20sub%2DSaharan%20Africa (accessed on 5 March 2023).
- Greenwood, B. Meningococcal meningitis in Africa. Trans. R. Soc. Trop. Med. Hyg. 1999, 93, 341–353. [Google Scholar] [CrossRef] [PubMed]
- Marc LaForce, F.M.; Ravenscroft, N.; Djingarey, M.; Viviani, S. Epidemic meningitis due to Group A Neisseria meningitidis in the African meningitis belt: A persistent problem with an imminent solution. Vaccine 2009, 27 (Suppl. S2), B13–B19. [Google Scholar] [CrossRef]
- Frasch, C.E.; Preziosi, M.P.; LaForce, F.M. Development of a group A meningococcal conjugate vaccine, MenAfriVac(TM). Hum. Vaccin. Immunother. 2012, 8, 715–724. [Google Scholar] [CrossRef]
- Program for Appropriate Technology in Health. The Meningitis Vaccine Project—Frequently Asked Questions. Available online: https://www.path.org/resources/the-meningitis-vaccine-project-frequently-asked-questions/ (accessed on 6 December 2022).
- Centers for Disease Control and Prevention. Bacterial Meningitis. Available online: https://www.cdc.gov/meningitis/lab-manual/chpt01-intro.html (accessed on 8 October 2022).
- Lapeyssonnie, L. Cerebrospinal meningitis in Africa. Bull. World Health Organ. 1963, 28, 1–114. [Google Scholar]
- Global Burden of Disease Collaborative. Network. Glob Burden Dis Study 2019 (GBD 2019). Available online: http://www.healthdata.org/gbd/2019 (accessed on 8 October 2022).
- Trotter, C.L.; Lingani, C.; Fernandez, K.; Cooper, L.V.; Bita, A.; Tevi-Benissan, C.; Ronveaux, O.; Préziosi, M.-P.; Stuart, J.M. Impact of MenAfriVac in nine countries of the African meningitis belt, 2010–2015: An analysis of surveillance data. Lancet Infect. Dis. 2017, 17, 867–872. [Google Scholar] [CrossRef]
- Retchless, A.C.; Hu, F.; Ouédraogo, A.-S.; Diarra, S.; Knipe, K.; Sheth, M.; Rowe, L.A.; Sangaré, L.; Ba, A.K.; Ouangraoua, S.; et al. The establishment and diversification of epidemic-associated serogroup W meningococcus in the African Meningitis Belt, 1994 to 2012. mSphere 2016, 1, e00201-16. [Google Scholar] [CrossRef] [PubMed]
- Mounkoro, D.; Nikiema, C.S.; Maman, I.; Sakandé, S.; Bozio, C.H.; Tall, H.; Sadji, A.Y.; Njanpop-Lafourcade, B.-M.; Sibabe, A.; Landoh, D.E.; et al. Neisseria meningitidis Serogroup W Meningitis Epidemic in Togo, 2016. J. Infect. Dis. 2019, 220 (Suppl. S4), S216–S224. [Google Scholar] [CrossRef] [PubMed]
- Koumaré, B.; Ouedraogo-Traoré, R.; Sanou, I.; Yada, A.A.; Sow, I.; Lusamba, P.-S.; Traoré, E.; Dabal, M.; Santamaria, M.; Hacen, M.-M.; et al. The first large epidemic of meningococcal disease caused by serogroup W135, Burkina Faso, 2002. Vaccine 2007, 25 (Suppl. S1), A37–A41. [Google Scholar] [CrossRef]
- Sidikou, F.; Zaneidou, M.; Alkassoum, I.; Schwartz, S.; Issaka, B.; Obama, R.; Lingani, C.; Tate, A.; Ake, F.; Sakande, S.; et al. Emergence of epidemic Neisseria meningitidis serogroup C in Niger, 2015: An analysis of national surveillance data. Lancet Infect. Dis. 2016, 16, 1288–1294. [Google Scholar] [CrossRef]
- Traore, Y.; Njanpop-Lafourcade, B.; Adjogble, K.; Lourd, M.; Yaro, S.; Nacro, B.; Drabo, A.; du Chatelet, I.P.; Mueller, J.E.; Taha, M.; et al. The rise and fall of epidemic Neisseria meningitidis serogroup W135 meningitis in Burkina Faso, 2002–2005. Clin. Infect. Dis 2006, 43, 817–822. [Google Scholar] [CrossRef]
- Maïnassara, H.B.; Oumarou, G.I.; Issaka, B.; Sidiki, A.; Idi, I.; Pelat, J.M.; Fontanet, A.; Mueller, J.E. Evaluation of response strategies against epidemics due to Neisseria meningitidis C in Niger. Trop. Med. Int. Health 2017, 22, 196–204. [Google Scholar] [CrossRef]
- MacNeil, J.R.; Medah, I.; Koussoubé, D.; Novak, R.T.; Cohn, A.C.; Diomandé, F.V.; Yelbeogo, D.; Kambou, J.L.; Tarbangdo, T.F.; Ouédraogo-Traoré, R.; et al. Neisseria meningitidis serogroup W, Burkina Faso, 2012. Emerg. Infect. Dis. 2014, 20, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Topaz, N.; Caugant, D.A.; Taha, M.-K.; Brynildsrud, O.B.; Debech, N.; Hong, E.; Deghmane, A.-E.; Ouédraogo, R.; Ousmane, S.; Gamougame, K.; et al. Phylogenetic relationships and regional spread of meningococcal strains in the meningitis belt, 2011–2016. EBiomedicine 2019, 41, 488–496. [Google Scholar] [CrossRef]
- Mohammed, I.; Nasidi, A.; Alkali, A.; Garbati, M.; Ajayi-Obe, E.; Audu, K.A.; Usman, A.; Abdullahi, S. A severe epidemic of meningococcal meningitis in Nigeria, 1996. Trans. R. Soc. Trop. Med. Hyg. 2000, 94, 265–270. [Google Scholar] [CrossRef]
- Chow, J.; Uadiale, K.; Bestman, A.; Kamau, C.; Caugant, D.A.; Shehu, A.; Greig, J. Invasive meningococcal meningitis serogroup C outbreak in northwest Nigeria, 2015—Third consecutive outbreak of a new strain. PLoS Curr. 2016, 8. [Google Scholar] [CrossRef]
- World Health Organization Country Office Democratic Republic of Congo. Meningitis Epidemic in DRC in. Democratic Republic of the Congo: Meningitis. 2016. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2021-DON334 (accessed on 20 September 2021).
- World Health Organization. Control of epidemic meningitis in countries in the African meningitis belt, 2021. Wkly. Epidemiol. Rec. 2022, 35, 409–423. [Google Scholar]
- Bwaka, A.; Bita, A.; Lingani, C.; Fernandez, K.; Durupt, A.; Mwenda, J.M.; Mihigo, R.; Djingarey, M.H.; Ronveaux, O.; Preziosi, M.-P. Status of the rollout of the meningococcal serogroup A conjugate vaccine in African meningitis belt countries in 2018. J. Infect. Dis. 2019, 220 (Suppl. S4), S140–S147. [Google Scholar] [CrossRef]
- Arsene Bita Fouda, A.A. Epidemiological status of bacterial meningitis disease following the introduction of the meningococcal A conjugate vaccine in the African meningitis belt. Int. J. Immunol. 2019, 7, 12–22. [Google Scholar] [CrossRef]
- Ministry of Public Health Hygiene and Prevention of Democratic Republic of Congo. Epidemiological Situation Report n° 109; Ministry of Public Health Hygiene and Prevention of Democratic Republic of Congo: Kinshasa, Congo, 2021.
- Ministry of Public Health Hygiene and Prevention of Democratic Republic of Congo. After Action Review Report; Ministry of Public Health Hygiene and Prevention of Democratic Republic of Congo: Kinshasa, Congo, 2022.
- Ministry of Public Health Hygiene and Prevention of Democratic Republic of Congo. End Meningitis Epidemic in Banalia health Zone Report; Public Health Hygiene and Prevention of Democratic Republic of Congo: Kinshasa, Congo, 2022.
- World Health Organization Regional Office. Standard Operating Procedures for Surveillance of Meningitis Preparedness and Response to Epidemics in Africa. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/312141/9789290234241-eng.pdf (accessed on 17 July 2021).
- Lingani, C.; Bergeron-Caron, C.; Stuart, J.M.; Fernandez, K.; Djingarey, M.H.; Ronveaux, O.; Schnitzler, J.C.; Perea, W.A. Meningococcal meningitis surveillance in the African meningitis belt, 2004-2013. Clin. Infect. Dis. 2015, 61 (Suppl. S5), S410–S415. [Google Scholar] [CrossRef]
- World Health Organization. Meningococcal vaccines: WHO position paper. Wkly. Epidemiol. Rec. 2011, 86, 521–539. [Google Scholar]
- Maiden, M.C.; Bygraves, J.A.; Feil, E.; Morelli, G.; Russell, J.E.; Urwin, R.; Zhang, Q.; Zhou, J.; Zurth, K.; Caugant, D.A.; et al. Multilocus sequence typing: A portable approach to the identification of clones within populations of pathogenic microorganisms. Proc. Natl. Acad. Sci. USA 1998, 95, 3140–3145. [Google Scholar] [CrossRef]
- Taha, M.K.; Vázquez, J.A.; Hong, E.; Bennett, D.E.; Bertrand, S.; Bukovski, S.; Cafferkey, M.T.; Carion, F.; Christensen, J.J.; Diggle, M.; et al. Target gene sequencing to characterize the penicillin G susceptibility of Neisseria meningitidis. Antimicrob. Agents Chemother. 2007, 51, 2784–2792. [Google Scholar] [CrossRef]
- Vázquez, J.A.; Arreaza, L.; Block, C.; Ehrhard, I.; Gray, S.J.; Heuberger, S.; Hoffmann, S.; Kriz, P.; Nicolas, P.; Olcen, P.; et al. Interlaboratory comparison of agar dilution and Etest methods for determining the MICs of antibiotics used in management of Neisseria meningitidis infections. Antimicrob. Agents Chemother 2003, 47, 3430–3434. [Google Scholar] [CrossRef]
- Jolley, K.A.; Brehony, C.; Maiden, M.C. Molecular typing of meningococci: Recommendations for target choice and nomenclature. FEMS Microbiol. Rev. 2007, 31, 89–96. [Google Scholar] [CrossRef]
- Taha, M.K. Simultaneous approach for nonculture PCR-based identification and serogroup prediction of Neisseria meningitidis. J. Clin. Microbiol. 2000, 38, 855–857. [Google Scholar] [CrossRef] [PubMed]
- Helena De Oliveira, L.H.; Jauregui, B.; Carvalho, A.F.; Giglio, N. Impact and effectiveness of meningococcal vaccines: A review. Rev. Panam. Salud. Publ. 2017, 41, e158. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Public Health Hygiene and Prevention of Democratic Republic of Congo. Response Campaign against Meningitis, Rural Health Zone of Banalia Report; Public Health Hygiene and Prevention of Democratic Republic of Congo: Kinshasa, Congo, 2021.



{kind=link}
{kind=link}
| Sub-Health Zones | Population | Cumulative Suspected Cases | Cumulative Attack Rate (per 100,000 Inhabitants) | Weeks in Which Epidemic Threshold Was Crossed (Number of Suspected Cases) | Cumulative Deaths | Case Fatality Ratio (%) |
|---|---|---|---|---|---|---|
| Right bank | 79,319 | 1844 | 2326.1 | w21 (13), w22 (8), w24 (10), w25 (20), w26 (16), w27 (18), w28 (17), w30 (14), w31 (10), w33 (13), w34 (34), w35 (25), w36 (61), w37 (217), w38 (223), w39 (258), w40 (312), w41 (253), w42 (125), w43 (108), w44 (56) | 170/2326.1 | 9.2% |
| Left bank | 88,286 | 818 | 926.5 | w35 (14), w36 (32), w37 (81), w38 (136), w39 (150), w40 (116), w41 (118), w42 (90), w43 (26), w44 (17) | 35/926.5 | 4.3% |
| Banalia health zone | 167,605 | 2662 | 1588.9 | W 21–44 | 205/2662 | 7.7% |
| Variables | Number (n1) | Meningitis Suspected Cases (n2/N3) | p-Value |
|---|---|---|---|
| Age group | |||
| 0–59 month | 188/2409 (7.8%) | ||
| 5–14 year | 251/2409 (10.5%) | ||
| 15–29 year | 647/2409 (26.8%) | <0.001 * | |
| 30–49 year | 927/2409 (38.5%) | ||
| 50 year and above | 396/2409 (14.4%) | ||
| Missing data | 253/2662 (9.5%) | ||
| Gender | |||
| Female | 1163/2447 (47.6%) | 0.8 ** | |
| Male | 1284/2447 (52.4%) | ||
| Missing data | 215/2662 (8%) | ||
| Status | |||
| Alive | 2457/2662 (96.3%) | <0.001 * | |
| Death | 205/2662 (7.7%) |
| Pathogens Confirmed | Meningitis Pathogens n1/N2 (%) |
|---|---|
| N. Meningitidis W | 47/57 (82.5%) |
| N. Meningitidis C | 4/57 (7%) |
| S. pneumoniae | 3/57 (5%) |
| Haemophilus influenzae b | 2/57(3,5%) |
| Haemophilus influenzae non-b | 1/57 (2%) |
| Total | 57/57 (100%) |
| Number of Cases | p-Value | Number of Deaths | p-Value | |||
|---|---|---|---|---|---|---|
| Before Reactive Vaccination w 21–40 | After Reactive Vaccination w 41–47 | Before Ceftriaxone Introduction w 21–31 | After Ceftriaxone Introduction w 32–47 | |||
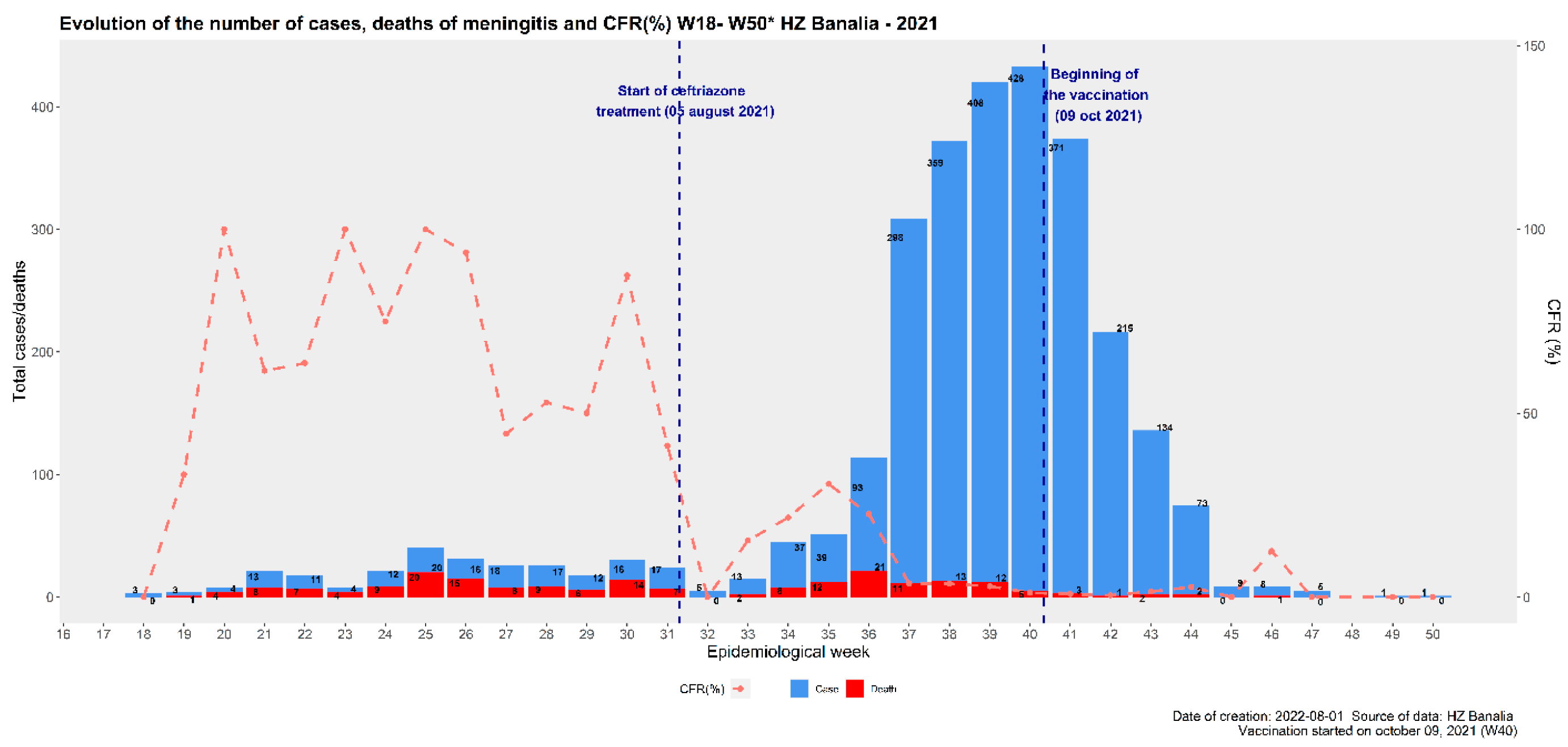
| Cases and deaths before and after interventions | 1745 | 908 | p = 0.001 1 | 111 deaths | 94 deaths | p = 0.001 1 |
| Characteristic | IRR 1 | 95% CI 2 | p-Value |
|---|---|---|---|
| Reactive vaccination campaign | |||
| Before (suspected cases) | — | — | |
| After (suspected cases) | 0.18 | 0.02, 0.80 | 0.041 |
| Ceftriaxone administration | |||
| Before (deaths) | — | — | |
| After (deaths) | 12.5 | 1.48, 114 | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bita Fouda, A.A.; Latt, A.; Sinayoko, A.; Mboussou, F.F.R.; Pezzoli, L.; Fernandez, K.; Lingani, C.; Miwanda, B.; Bulemfu, D.; Baelongandi, F.; et al. The Bacterial Meningitis Epidemic in Banalia in the Democratic Republic of Congo in 2021. Vaccines 2024, 12, 461. https://doi.org/10.3390/vaccines12050461
Bita Fouda AA, Latt A, Sinayoko A, Mboussou FFR, Pezzoli L, Fernandez K, Lingani C, Miwanda B, Bulemfu D, Baelongandi F, et al. The Bacterial Meningitis Epidemic in Banalia in the Democratic Republic of Congo in 2021. Vaccines. 2024; 12(5):461. https://doi.org/10.3390/vaccines12050461
Chicago/Turabian StyleBita Fouda, Andre Arsene, Anderson Latt, Abdoulaye Sinayoko, Franck Fortune Roland Mboussou, Lorenzo Pezzoli, Katya Fernandez, Clement Lingani, Berthe Miwanda, Dorothée Bulemfu, Francis Baelongandi, and et al. 2024. "The Bacterial Meningitis Epidemic in Banalia in the Democratic Republic of Congo in 2021" Vaccines 12, no. 5: 461. https://doi.org/10.3390/vaccines12050461