
Low Measles Vaccination Coverage and Spatial Analysis of High Measles Vaccination Dropout in Ethiopia’s Underprivileged Areas
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Study Participants
2.3. Sample Size Determination
2.4. Sampling Procedure
2.5. Data Collection Procedures and Data Quality Assurance
2.6. Ascertainment of Childhood Vaccination
2.7. Data Management and Statistical Analysis
2.8. Measles Vaccination Coverage
2.9. Measles Vaccination Dropout
2.10. Spatial Autocorrelation
2.11. Hot Spot Analysis (Getis-Ord Gi* Statistics)
2.12. Ethical Approval
3. Results
3.1. Sociodemographic Characteristics
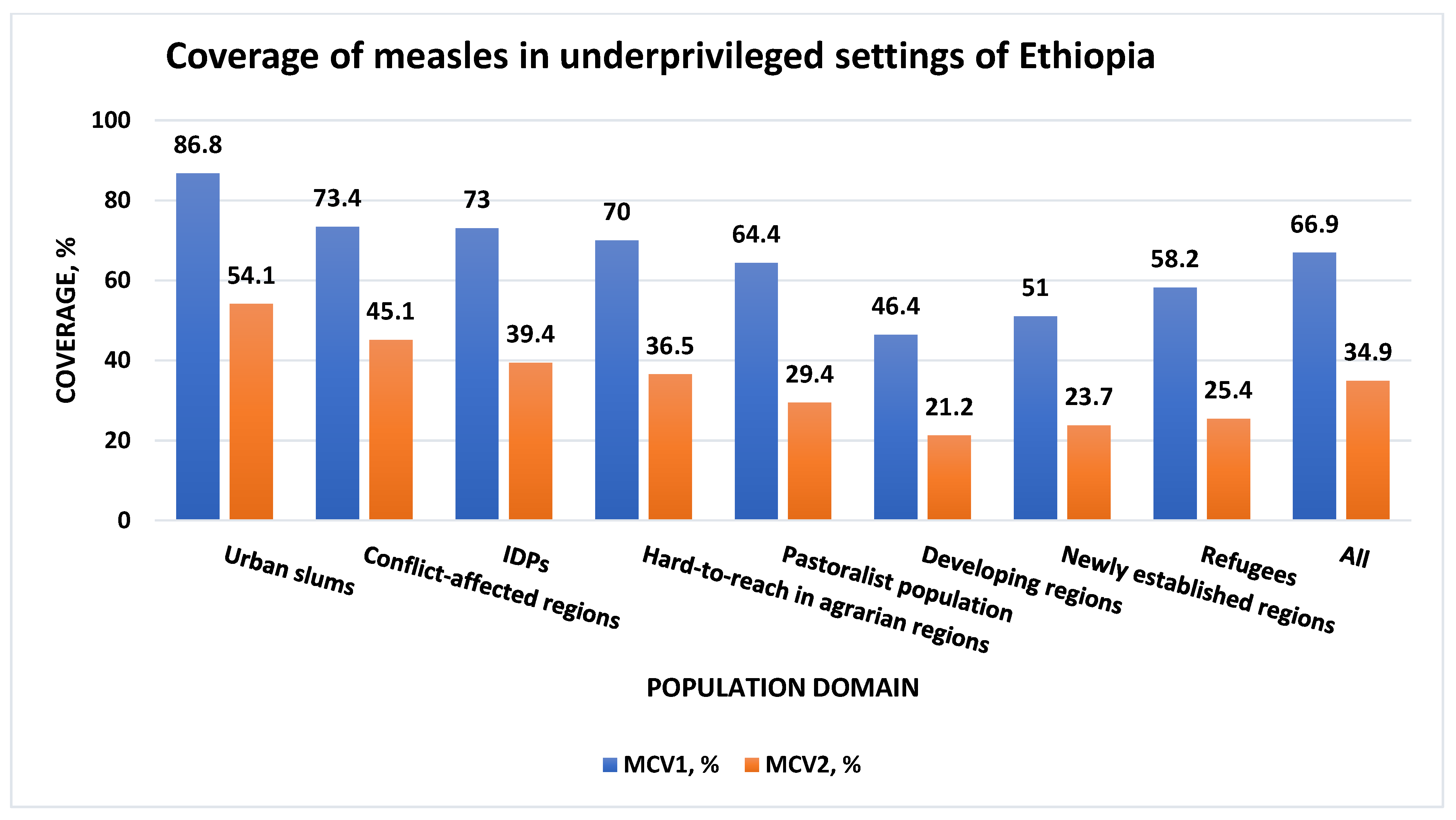
3.2. Coverage of Measles in Remote and Underserved Settings of Ethiopia
3.3. Measles Vaccination Dropout Estimates in Remote and Underserved Settings of Ethiopia
3.4. Spatial Autocorrelation Analysis
3.5. Hot Spot Analysis of Measles Vaccination Dropout Cases
4. Discussion
5. Conclusions and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Minta, A.A.; Ferrari, M.; Antoni, S.; Portnoy, A.; Sbarra, A.; Lambert, B.; Hauryski, S.; Hatcher, C.; Nedelec, Y.; Datta, D.; et al. Progress Toward Regional Measles Elimination—Worldwide, 2000–2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1489–1495. [Google Scholar] [CrossRef]
- World Health Organization. Measles Vaccines: WHO Position Paper—April 2017. Wkly. Epidemiol. Rec. 2017, 17, 205–228. [Google Scholar]
- Venkatesan, P. Worrying global decline in measles immunisation. Lancet Microbe 2022, 3, e9. [Google Scholar] [CrossRef]
- Guerra, F.M.; Bolotin, S.; Lim, G.; Heffernan, J.; Deeks, S.L.; Li, Y.; Crowcroft, N.S. The basic reproduction number (R(0)) of measles: A systematic review. Lancet Infect. Dis. 2017, 17, e420–e428. [Google Scholar] [CrossRef]
- Pond, B.; Bekele, A.; Mounier-Jack, S.; Teklie, H.; Getachew, T. Estimation of Ethiopia’s immunization coverage—20 years of discrepancies. BMC Health Serv. Res. 2021, 21 (Suppl. S1), 587. [Google Scholar] [CrossRef] [PubMed]
- Central Statistical Agency (CSA) and ICF. Ethiopia Demographic and Health Survey 2016; CSA: Addis Ababa, Ethiopia; ICF: Rockville, MD, USA, 2016. [Google Scholar]
- Ethiopia Federal Ministry of Health. Expanded Program on Immunization (EPI). 2021. Available online: https://www.moh.gov.et/initiatives-4-col/Expanded_Program_on_Immunization (accessed on 18 March 2024).
- Masresha, B.G.; Hatcher, C.; Lebo, E.; Tanifum, P.; Bwaka, A.M.; Minta, A.A.; Antoni, S.; Grant, G.B.; Perry, R.T.; O’Connor, P. Progress Toward Measles Elimination—African Region, 2017–2021. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 985–991. [Google Scholar] [CrossRef] [PubMed]
- Yitbarek, K.; Tilahun, T.; Debela, T.; Abdena, D.; Girma, T. Measles epidemiology and vaccination coverage in Oromia Region, Ethiopia: Evidence from surveillance, 2011–2018. Vaccine 2021, 39, 4351–4358. [Google Scholar] [CrossRef]
- Goshu Muluneh, A.; Woldemariam Merid, M.; Tigabu, B.; Getie Ferede, M.; Molla Kassa, G.; Animut, Y. Less than one-fifth of Ethiopian children were vaccinated for measles second dose; evidence from the Ethiopian mini demographic and health survey 2019. Vaccine X 2022, 12, 100217. [Google Scholar] [CrossRef]
- Tadesse, A.W.; Sahlu, D.; Benayew, M. Second-dose measles vaccination and associated factors among under-five children in urban areas of North Shoa Zone, Central Ethiopia, 2022. Front. Public Health 2022, 10, 1029740. [Google Scholar] [CrossRef]
- World Health Organization. Measles Vaccination Coverage. 2021. Available online: https://immunizationdata.who.int/pages/coverage/mcv.html?CODE=ETH&ANTIGEN=MCV2&YEAR= (accessed on 15 January 2024).
- World Health Organization. Analysis and Use of Health Facility Data: Guidance for Immunization Programme Managers; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Mmanga, K.; Mwenyenkulu, T.E.; Nkoka, O.; Ntenda, P.A.M. Tracking immunization coverage, dropout and equity gaps among children ages 12–23 months in Malawi—Bottleneck analysis of the Malawi Demographic and Health Survey. Int. Health 2022, 14, 250–259. [Google Scholar] [CrossRef]
- Powelson, J.; Magadzire, B.P.; Draiva, A.; Denno, D.; Ibraimo, A.; Benate, B.B.L.; Jahar, L.C.; Marrune, Z.; Chilundo, B.; Chinai, J.E.; et al. Determinants of immunisation dropout among children under the age of 2 in Zambezia province, Mozambique: A community-based participatory research study using Photovoice. BMJ Open 2022, 12, e057245. [Google Scholar] [CrossRef]
- Hailu, C.; Fisseha, G.; Gebreyesus, A. Determinants of measles vaccination dropout among 12–23 months aged children in pastoralist community of Afar, Ethiopia. BMC Infect. Dis. 2022, 22, 376. [Google Scholar] [CrossRef]
- Shiferie, F.; Gebremedhin, S.; Andargie, G.; Tsegaye, D.A.; Alemayehu, W.A.; Mekuria, L.A.; Wondie, T.; Fenta, T.G. Vaccination dropout and wealth related inequality among children aged 12–35 months in remote and underserved settings of Ethiopia: A cross-sectional evaluation survey. Front. Pediatr. 2023, 11, 1280746. [Google Scholar] [CrossRef]
- World Health Organization. African Regional Guidelines for Measles and Rubella Surveillance; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Gavi, The Vaccine Alliance. Routine Immunisation Worldwide Holds Firm Despite the Pandemic. 2021. Available online: https://www.gavi.org/vaccineswork/routine-immunisation-worldwide-holds-firm-despite-pandemic (accessed on 15 January 2024).
- Project HOPE, Ethiopia Federal Ministry of Health. Reaching Zero-Dose and Underimmunized Children in Remote and Underserved Settings of Ethiopia: Evaluation; Project HOPE: Addis Ababa, Ethiopia, 2022. [Google Scholar]
- World Health Organization. Vaccination Coverage Cluster Surveys: Reference Manual; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Cochran, W.G. Sampling Techniques, 3rd ed.; John Wiley & Sons: New York, NY, USA, 1977. [Google Scholar]
- Pourhoseingholi, M.A.; Vahedi, M.; Rahimzadeh, M. Sample size calculation in medical studies. Gastroenterol. Hepatol. Bed Bench 2013, 6, 14–17. [Google Scholar]
- World Health Organization. Practical Guide for the Design, Use and Promotion of Home-Based Records in Immunization Programmes. 2015. Available online: https://www.who.int/publications/i/item/WHO-IVB-15.05 (accessed on 10 January 2024).
- Dimagi. CommCare. 2007. Available online: https://www.dimagi.com (accessed on 15 January 2023).
- StataCorp. Stata Statistical Software; StataCorp LLC: College Station, TX, USA, 2021; Available online: https://www.stata.com/ (accessed on 16 December 2023).
- Tesfa, G.A.; Demeke, A.D.; Hailegebreal, S.; Amede, E.S.; Ngusie, H.S.; Kasie, M.N.; Seboka, B.T. Spatial distribution and associated factors of measles vaccination among children aged 12–23 months in Ethiopia. A spatial and multilevel analysis. Hum. Vaccin. Immunother. 2022, 18, 2035558. [Google Scholar] [CrossRef]
- Geremew, T.T.; Gezie, L.D.; Abejie, A.N. Geographical variation and associated factors of childhood measles vaccination in Ethiopia: A spatial and multilevel analysis. BMC Public. Health 2019, 19, 1194. [Google Scholar] [CrossRef]
- Tessema, F.; Kidanne, L.; Bisrat, F.; Asres, M.; Tadesse, T.; Asress, A.; Asegdew, B.; Zeleke, S.; Bederu, N. Child vaccination coverage and dropout rates in pastoral and semi-pastoral regions in Ethiopia: CORE group polio project implementation areas. Ethiop. J. Health Dev. 2019, 33, 1–9. [Google Scholar]
- Awol, M.; Alemu, Z.A.; Moges, N.A.; Jemal, K. Geographical variations and associated factors of defaulting from immunization among children aged 12 to 23 months in Ethiopia: Using spatial and multilevel analysis of 2016 Ethiopian Demographic and Health Survey. Environ. Health Prev. Med. 2021, 26, 65. [Google Scholar] [CrossRef] [PubMed]
- Ethiopian Public Health Institute (EPHI) and ICF. Ethiopia Mini Demographic and Health Survey 2019: Final Report; EPHI and ICF: Rockville, MD, USA, 2021. [Google Scholar]
- Ketema, D.B.; Assemie, M.A.; Alamneh, A.A.; Alene, M.; Chane, K.Y.; Alamneh, Y.M.; Birhanu, M.Y.; Alebel, A. Full vaccination coverage among children aged 12-23 months in Ethiopia: A systematic review and meta-analysis. BMC Public. Health 2020, 20, 777. [Google Scholar] [CrossRef]
- Atalell, K.A.; Liyew, A.M.; Alene, K.A. Spatial distribution of rotavirus immunization coverage in Ethiopia: A geospatial analysis using the Bayesian approach. BMC Infect. Dis. 2022, 22, 830. [Google Scholar] [CrossRef] [PubMed]
- Atalell, K.A.; Alemayehu, M.A.; Teshager, N.W.; Belay, G.M.; Alemu, T.G.; Anlay, D.Z.; Wondim, A.; Alene, K.A. Mapping BCG vaccination coverage in Ethiopia between 2000 and 2019. BMC Infect. Dis. 2022, 22, 569. [Google Scholar] [CrossRef] [PubMed]
- Tesfa, G.A.; Yehualashet, D.E.; Getnet, A.; Bimer, K.B.; Seboka, B.T. Spatial distribution of complete basic childhood vaccination and associated factors among children aged 12–23 months in Ethiopia. A spatial and multilevel analysis. PLoS ONE 2023, 18, e0279399. [Google Scholar] [CrossRef] [PubMed]
- Lakew, Y.; Bekele, A.; Biadgilign, S. Factors influencing full immunization coverage among 12–23 months of age children in Ethiopia: Evidence from the national demographic and health survey in 2011. BMC Public Health 2015, 15, 728. [Google Scholar] [CrossRef] [PubMed]
- Tamirat, K.S.; Sisay, M.M. Full immunization coverage and its associated factors among children aged 12–23 months in Ethiopia: Further analysis from the 2016 Ethiopia demographic and health survey. BMC Public Health 2019, 19, 1019. [Google Scholar] [CrossRef]
- Nour, T.Y.; Farah, A.M.; Ali, O.M.; Abate, K.H. Immunization coverage in Ethiopia among 12-23 month old children: Systematic review and meta-analysis. BMC Public. Health 2020, 20, 1134. [Google Scholar] [CrossRef]
- Sheik-Mohamed, A.; Velema, J.P. Where health care has no access: The nomadic populations of sub-Saharan Africa. Trop. Med. Int. Health 1999, 4, 695–707. [Google Scholar] [CrossRef]
- Teklegiorgis, K.; Tadesse, K.; Mirutse, G.; Terefe, W. Factors Associated with Low Level of Health Information Utilization in Resources Limited Setting, Eastern Ethiopia. Int. J. Intell. Inf. Syst. 2014, 3, 69–75. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population Domain | Description | |
|---|---|---|
| 1 | Pastoralist regions and populations | Afar and Somali regions and specific pastoralist or semi-pastoralist settings in Oromia, SNNP, Southwest Ethiopia, and Gambella regions |
| 2 | Developing regions | Afar, Somali, Gambella, and Benishangul Gumuz regions |
| 3 | Newly established regions | Sidama and Southwest Ethiopia regions |
| 4 | Conflict-affected areas | Selected settings in Afar, Amhara, Oromia, and Benishangul Gumuz regions |
| 5 | Underserved urban slums | Urban slums in six selected cities (Addis Ababa, Bahirdar, Hawassa, Dire Dawa, Harar, and Adama) and rural areas under Dire Dawa City Administration and Harari Region |
| 6 | Hard-to-reach areas in major regions | Selected remote districts in Amhara, Oromia, and SNNP regions |
| 7 | Internally displaced populations (IDPs) | Selected IDP centers in Afar, Amhara, Oromia, and Benishangul Gumuz regions |
| 8 | Refugees | Refugees from selected camps in Somali, Afar, and Gambella regions |
| Characteristics | Frequency | Percent |
|---|---|---|
| Child’s sex | ||
| Male | 1985 | 54.4 |
| Female | 1661 | 45.6 |
| Child’s age (months) | ||
| 12–23 | 1849 | 50.7 |
| 24–35 | 1797 | 49.3 |
| Mother’s/Caregiver’s age (years) | ||
| 15–24 | 875 | 24.0 |
| 25–34 | 1969 | 54.0 |
| 35–44 | 572 | 15.7 |
| 45 or above | 104 | 2.9 |
| Do not know | 126 | 3.5 |
| Mother’s/Caregiver’s educational status | ||
| No formal education or preschool | 2158 | 59.2 |
| Primary education | 788 | 21.6 |
| Secondary education | 616 | 16.9 |
| Tertiary education | 84 | 2.3 |
| Marital status | ||
| Not ever married | 43 | 1.2 |
| Married/Living together | 3312 | 90.8 |
| Separated | 83 | 2.3 |
| Divorced | 110 | 3.0 |
| Widowed | 98 | 2.7 |
| Place of residence | ||
| Urban | 677 | 18.6 |
| Rural | 2969 | 81.4 |
| Caregiver’s employment status | ||
| Unemployed | 2098 | 57.6 |
| Employed | 1548 | 42.4 |
| Region * | ||
| Afar | 636 | 17.4 |
| Amhara | 372 | 10.2 |
| Oromia | 431 | 11.8 |
| Somali | 480 | 13.2 |
| Benishangul Gumuz | 216 | 5.9 |
| Southern Nations, Nationalities, and Peoples | 300 | 8.2 |
| Sidama | 239 | 6.6 |
| Southwest Ethiopia | 181 | 5.0 |
| Gambella | 479 | 13.1 |
| Harari | 60 | 1.6 |
| Addis Ababa | 192 | 5.3 |
| Dire Dawa | 60 | 1.6 |
| Household size | ||
| 2–5 | 2044 | 56.0 |
| 6 or above | 1602 | 44.0 |
| Target Population Domain | MCV1 to MCV2 Dropout Estimate * n (%) |
|---|---|
| Urban slums | 145 (37.7) |
| Conflict-affected regions | 78 (38.5) |
| IDPs | 89 (46.2) |
| Hard-to-reach in agrarian regions | 264 (47.9) |
| Pastoralist population | 469 (54.3) |
| Developing regions | 348 (54.4) |
| Newly established regions | 114 (53.5) |
| Refugees | 102 (56.4) |
| All † | 1158 (48.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shiferie, F.; Gebremedhin, S.; Andargie, G.; Tsegaye, D.A.; Alemayehu, W.A.; Fenta, T.G. Low Measles Vaccination Coverage and Spatial Analysis of High Measles Vaccination Dropout in Ethiopia’s Underprivileged Areas. Vaccines 2024, 12, 328. https://doi.org/10.3390/vaccines12030328
Shiferie F, Gebremedhin S, Andargie G, Tsegaye DA, Alemayehu WA, Fenta TG. Low Measles Vaccination Coverage and Spatial Analysis of High Measles Vaccination Dropout in Ethiopia’s Underprivileged Areas. Vaccines. 2024; 12(3):328. https://doi.org/10.3390/vaccines12030328
Chicago/Turabian StyleShiferie, Fisseha, Samson Gebremedhin, Gashaw Andargie, Dawit A. Tsegaye, Wondwossen A. Alemayehu, and Teferi Gedif Fenta. 2024. "Low Measles Vaccination Coverage and Spatial Analysis of High Measles Vaccination Dropout in Ethiopia’s Underprivileged Areas" Vaccines 12, no. 3: 328. https://doi.org/10.3390/vaccines12030328