
The Shifting Epidemiology of Hepatitis A in the World Health Organization Western Pacific Region
 ,
,
Abstract
:1. Introduction
2. Vaccination Programs in Countries in the WPR
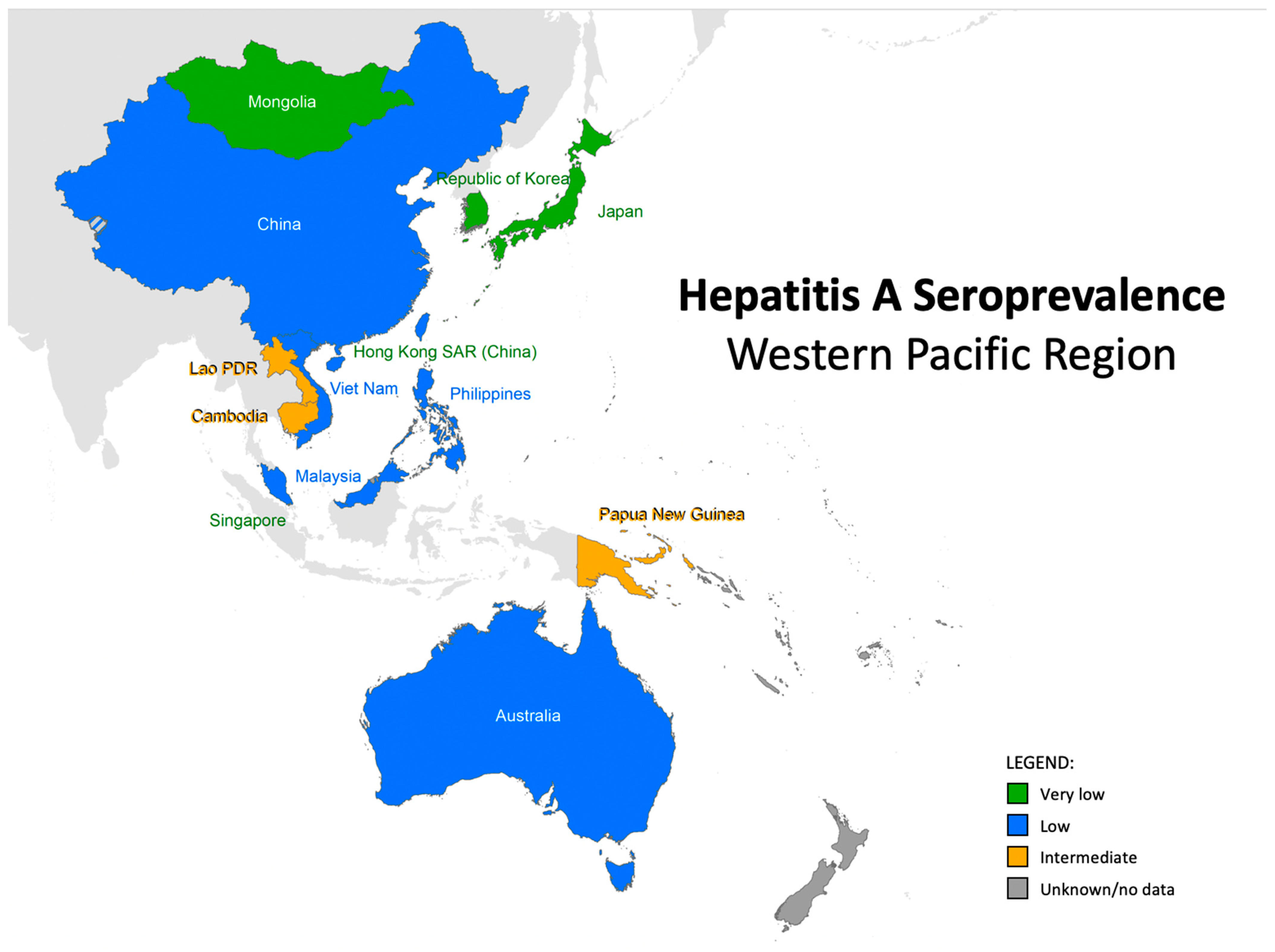
3. Epidemiology and Seroepidemiology of Hepatitis A in the WHO WPR
3.1. Australia
3.2. Cambodia
3.3. China
3.4. Hong Kong
3.5. Japan
3.6. Republic of Korea
3.7. Lao PDR
3.8. Malaysia
3.9. Mongolia
3.10. New Zealand
3.11. Papua New Guinea
3.12. Pacific Island Countries and Areas
3.13. Philippines
3.14. Singapore
3.15. Vietnam
4. Discussion and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feinstone, S.M.; Kapikian, A.Z.; Purcell, R.H. Hepatitis A: Detection by immune electron microscopy of a viruslike antigen associated with acute illness. Science 1973, 182, 1026–1028. [Google Scholar] [CrossRef]
- Mackinney-Novelo, I.; Barahona-Garrido, J.; Castillo-Albarran, F.; Santiago-Hernández, J.J.; Méndez-Sánchez, N.; Uribe, M.; Chávez-Tapia, N. Clinical course and management of acute hepatitis A infection in adults. Ann. Hepatol. 2012, 11, 652–657. [Google Scholar] [CrossRef] [PubMed]
- Leal, P.R.; de Guimarães, R.J.P.S.E.; Kampel, M. Associations Between Environmental and Sociodemographic Data and Hepatitis-A Transmission in Pará State (Brazil). GeoHealth 2021, 5, e2020GH000327. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, K.H.; Wiersma, S.T. Hepatitis A virus seroprevalence by age and world region, 1990 and 2005. Vaccine 2010, 28, 6653–6657. [Google Scholar] [CrossRef] [PubMed]
- Barzaga, B.N. Hepatitis A shifting epidemiology in South-East Asia and China. Vaccine 2000, 18 (Suppl. S1), S61–S64. [Google Scholar] [CrossRef] [PubMed]
- Cao, G.; Jing, W.; Liu, J.; Liu, M. The global trends and regional differences in incidence and mortality of hepatitis A from 1990 to 2019 and implications for its prevention. Hepatol. Int. 2021, 15, 1068–1082. [Google Scholar] [CrossRef]
- Zeng, D.-Y.; Li, J.-M.; Lin, S.; Dong, X.; You, J.; Xing, Q.-Q.; Ren, Y.-D.; Chen, W.-M.; Cai, Y.-Y.; Fang, K.; et al. Global burden of acute viral hepatitis and its association with socioeconomic development status, 1990–2019. J. Hepatol. 2021, 75, 547–556. [Google Scholar] [CrossRef]
- Gripenberg, M.; Aloysia D’Cor, N.; L’Azou, M.; Marsh, G.; Druelles, S.; Nealon, J. Changing sero-epidemiology of hepatitis A in Asia Pacific countries: A systematic review. Int. J. Infect. Dis. 2018, 68, 13–17. [Google Scholar] [CrossRef]
- Chakravarti, A. Epidemiology of Hepatitis A: Past and Current Trends; Streba, C.T., Vere, C.C., Rogoveanu, I., Tripodi, V., Lucangioli, S., Eds.; IntechOpen: Rijeka, Croatia, 2020; Chapter 1. [Google Scholar] [CrossRef]
- Lemon, S.M.; Ott, J.J.; Van Damme, P.; Shouval, D. Type A viral hepatitis: A summary and update on the molecular virology, epidemiology, pathogenesis and prevention. J. Hepatol. 2017, 68, 167–184. [Google Scholar] [CrossRef]
- World Health Organization. SAGE April 2022 Meeting Highlights. 2022. Available online: https://www.who.int/news/item/11-04-2022-sage-april-2022-meeting-highlights (accessed on 19 October 2022).
- David, A.M. Hepatitis A outbreaks—Methods of intervention in South-East Asian countries. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2004, 8, 201–209. [Google Scholar] [CrossRef]
- Australian Government Department of Health. National Immunisation Program Schedule for All People. 2020. Available online: https://www.health.gov.au/resources/publications/national-immunisation-program-schedule-for-all-people (accessed on 19 December 2020).
- Chinese Center for Disease Control and Prevenetion. Childhood Immunization Schedule for National Immunization Program Vaccines—China (Version 2021). 2022. Available online: https://en.chinacdc.cn/health_topics/immunization/202203/t20220302_257317.html (accessed on 14 November 2023).
- World Health Organization. Viral Hepatitis Is Mongolia: Situation and Response; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- New Zealand Government. Hepatitis A (Hep A) Vaccine. 2023. Available online: https://www.immunise.health.nz/about-vaccines/nz-immunisations/hepatitis-a-hep-a-vaccine/ (accessed on 14 November 2023).
- Korea Disease Control and Prevention Agency. National Immunization Program for Children. 2020. Available online: http://www.kdca.go.kr/contents.es?mid=a30333000000 (accessed on 17 August 2021).
- Kang, S.H.; Kim, M.Y.; Baikm, S.K. Perspectives on Acute Hepatitis A Control in Korea. J. Korean Med. Sci. 2019, 34, e230. [Google Scholar] [CrossRef] [PubMed]
- Amin, J.; Heath, T.; Morrell, S. Hepatitis A in Australia in the 1990s: Future directions in surveillance and control. Commun. Dis. Intell. 1999, 23, 113–120. [Google Scholar] [PubMed]
- Franklin, N.; Camphor, H.; Wright, R.; Stafford, R.; Glasgow, K.; Sheppeard, V. Outbreak of hepatitis A genotype IB in Australia associated with imported frozen pomegranate arils. Epidemiol. Infect. 2019, 147, e74. [Google Scholar] [CrossRef]
- Australian Institute of Food Safety. Hepatitis A Outbreak in NSW, ACT Launches Public Health Investigation. 2019. Available online: https://www.foodsafety.com.au/news/hepatitis-outbreak-nsw-act-launches-public-health-investigation (accessed on 27 August 2022).
- Food Safety News. Hepatitis A Found in Tuna; Time Limited for Post Exposure Shots. 2017. Available online: https://www.foodsafetynews.com/2017/06/hepatitis-a-found-in-tuna-time-limited-for-post-exposure-shots-2/#more-140609 (accessed on 16 August 2021).
- Thüring, E.G.; Joller-Jemelka, H.I.; Sareth, H.; Sokhan, U.; Reth, C.; Grob, P. Prevalence of markers of hepatitis viruses A, B, C and of HIV in healthy individuals and patients of a Cambodian province. Southeast Asian J. Trop. Med. Public Health 1993, 24, 239–249. [Google Scholar]
- Chhour, Y.M.; Ruble, G.; Hong, R.; Minn, K.; Kdan, Y.; Sok, T.; Nisalak, A.; Myint, K.S.A.; Vaughn, D.W.; Endy, T.P. Hospital-based diagnosis of hemorrhagic fever, encephalitis, and hepatitis in Cambodian children. Emerg. Infect. Dis. 2002, 8, 485–489. [Google Scholar] [CrossRef]
- Poovorawan, Y.; Chongsrisawat, V.; Praianantathavorn, K.; Theamboonlers, A. High seroprevalence of hepatitis A virus among migrant workers from Myanmar, Cambodia and Laos who are living in Thailand. Ann. Trop. Med. Parasitol. 2009, 103, 361–363. [Google Scholar] [CrossRef] [PubMed]
- Nagashima, S.; Ko, K.; Yamamoto, C.; Bunthen, E.; Ouoba, S.; Chuon, C.; Ohisa, M.; Sugiyama, A.; Akita, T.; Hossain, S.; et al. Prevalence of total hepatitis A antibody among 5 to 7 years old children and their mothers in Cambodia. Sci. Rep. 2021, 11, 4778. [Google Scholar] [CrossRef] [PubMed]
- Main, B.; Lower, T.; James, R.; Rouse, I. Changes in Expanded Program for Immunization coverage for mother and child in Krakor, Cambodia 1996—1998. Trop. Med. Int. Health 2001, 6, 526–528. [Google Scholar] [CrossRef]
- Wang, Z.; Chen, Y.; Xie, S.; Lv, H. Changing Epidemiological Characteristics of Hepatitis A in Zhejiang Province, China: Increased Susceptibility in Adults. PLoS ONE 2016, 11, e0153804. [Google Scholar] [CrossRef]
- Cui, F.; Hadler, S.C.; Zheng, H.; Wang, F.; Wang, Z.; Hu, Y.; Gong, X.; Chen, Y.; Liang, X. Hepatitis A surveillance and vaccine use in China from 1990 through 2007. J. Epidemiol. 2009, 19, 189–195. [Google Scholar] [CrossRef]
- Wang, F.; Sun, X.; Wang, F.; Zheng, H.; Jia, Z.; Zhang, G.; Bi, S.; Miao, N.; Zhang, S.; Cui, F.; et al. Changing Epidemiology of Hepatitis A in China: Evidence From Three National Serological Surveys and the National Notifiable Disease Reporting System. Hepatology 2021, 73, 1251–1260. [Google Scholar] [CrossRef] [PubMed]
- Yan, B.; Lv, J.; Liu, J.; Feng, Y.; Wu, W.; Xu, A.; Zhang, L. Changes in seroprevalence of hepatitis A after the implementation of universal childhood vaccination in Shandong Province, China: A comparison between 2006 and 2014. Int. J. Infect. Dis. 2019, 82, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhang, X.-J.; Zhao, Y.-L.; Zhang, Y.-H.; Wang, S.-M.; Hao, Z.-Y.; Zhang, Z.-Y.; Ma, J.-C.; Fang, Y.; Wang, X.-Y. Waning of anti-HAV immunity in Shijiazhuang prefecture, Hebei province, China: A comparison of seroprevalence between 1992 and 2011. Vaccine 2014, 32, 6227–6232. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.-J.; Zhang, G.-M.; Zhou, R.-J.; Zheng, H.; Miao, N.; Yin, Z.-D.; Wang, F.-Z. Changes in the epidemiology of hepatitis A in three socio-economic regions of China, 1990–2017. Infect. Dis. Poverty 2019, 8, 80. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Wu, R.; Xu, H.; Uhanova, J.; Gish, R.; Wen, X.; Jin, Q.; Gerald, M.Y.; Nguyen, M.H.; Gao, Y.; et al. Changing incidence of reported viral hepatitis in China from 2004 to 2016: An observational study. BMJ Open 2019, 9, e028248. [Google Scholar] [CrossRef]
- Cao, J.; Wang, Y.; Song, H.; Meng, Q.; Sheng, L.; Bian, T.; Mahemuti, W.; Yierhali, A.; Omata, M.; Bi, S. Hepatitis A outbreaks in China during 2006: Application of molecular epidemiology. Hepatol. Int. 2009, 3, 356–363. [Google Scholar] [CrossRef]
- Sun, J.; Li, Y.; Fang, X.; Wang, Y.; Liu, Y.; Cao, J.; Zhou, W.; Zheng, H.; Yao, W. An Epidemic of Hepatitis A—Liaoning Province, 2020. CCDC Wkly. 2020, 2, 570–574. [Google Scholar] [CrossRef]
- Jiang, W.-P.; Chen, J.-T.; Wang, X.; Wang, Y.-L.; Liu, Y.; Chen, W.-Y.; Xu, W.-G.; Qiu, Y.-Z.; Yin, W.-D. Immunogenicity and safety of three consecutive lots of a new preservative-free inactivated hepatitis A vaccine (Healive): A double-blind, randomized and controlled trial. Vaccine 2008, 26, 2297–2301. [Google Scholar] [CrossRef]
- Mao, J.S.; Chai, S.A.; Xie, R.Y.; Chen, N.L.; Jiang, Q.; Zhu, X.Z.; Zhang, S.; Huang, H.; Mao, H.; Bao, X.; et al. Further evaluation of the safety and protective efficacy of live attenuated hepatitis A vaccine (H2-strain) in humans. Vaccine 1997, 15, 944–947. [Google Scholar] [CrossRef]
- Wang, X.-Y.; Xu, Z.-Y.; Ma, J.-C.; von Seidlein, L.; Zhang, Y.; Hao, Z.-Y.; Han, O.P.; Zhang, Y.-L.; Tian, M.-Y.; Ouyang, P.-Y.; et al. Long-term immunogenicity after single and booster dose of a live attenuated hepatitis A vaccine: Results from 8-year follow-up. Vaccine 2007, 25, 446–449. [Google Scholar] [CrossRef]
- Zhuang, F.; Qian, W.; Mao, Z.; Gong, Y.; Jiang, Q.; Jiang, L.; Chen, N.-L.; Chai, S.-A.; Mao, J.-S. Persistent efficacy of live attenuated hepatitis A vaccine (H2-strain) after a mass vaccination program. Chin. Med. J. 2005, 118, 1851–1856. [Google Scholar] [PubMed]
- Hu, Y.; Chen, Y. Evaluating Childhood Vaccination Coverage of NIP Vaccines: Coverage Survey versus Zhejiang Provincial Immunization Information System. Int. J. Environ. Res. Public Health 2017, 14, 758. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Rodewald, L.; Yang, J.; Qin, Y.; Pang, M.; Feng, L.; Yu, H. The landscape of vaccines in China: History, classification, supply, and price. BMC Infect. Dis. 2018, 18, 502. [Google Scholar] [CrossRef]
- Jacobsen, K. The Global Prevalence of Hepatitis A Virus Infection and Susceptibility: A Systematic Review. 2009, p. 50. Available online: https://apps.who.int/iris/bitstream/handle/10665/70180/WHO_IVB_10.01_eng.pdf;jsessionid=0C1C2E62AAE1BD76FB1E062E61F94BC5?sequence=1 (accessed on 27 August 2022).
- Wong, K.H.; Liu, Y.M.; Ng, P.S.P.; Young, B.W.Y.; Lee, S.S. Epidemiology of hepatitis A and hepatitis E infection and their determinants in adult Chinese community in Hong Kong. J. Med. Virol. 2004, 72, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Cheng, F.; Lau, L.; Lo, A.; Fabb, W.E. Changing hepatitis A epidemiology among Hong Kong Chinese adolescents: What are the implications? Public Health 1999, 113, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Li, A.M.; Chang, W.K. Hepatitis A and B infections in transfusion-dependent thalassaemia from endemic areas. J. Paediatr. Child Health 1991, 27, 228–231. [Google Scholar] [CrossRef] [PubMed]
- Chin, K.P.; Lok, A.S.; Wong, L.S.; Lai, C.L.; Wu, P.C. Current seroepidemiology of hepatitis A in Hong Kong. J. Med. Virol. 1991, 34, 191–193. [Google Scholar] [CrossRef]
- Chiu, P. Hepatitis A ‘Outbreak’ Prompts Hong Kong Health Authorities to Roll out Free Vaccines across the City. 2017. Available online: https://www.scmp.com/news/hong-kong/health-environment/article/2067562/hepatitis-outbreak-prompts-hong-kong-health (accessed on 5 October 2021).
- Hongkong Department of Health. Surveillance of Viral Hepatitis in Hong Kong 2019 Report; Hongkong Department of Health: Hongkong, China, 2020.
- Department of Health Centre for Health Protection. Surveillance of Viral Hepatitis in Hong Kong—2016 Update Report; Department of Health Centre for Health Protection: Hongkong, China, 2017.
- Department of Health Centre for Health Protection. Changing Epidemiology of Hepatitis A in Hong Kong and Implications on Control Strategies; Department of Health Centre for Health Protection: Hongkong, China, 2006.
- Lai, J. Hepatitis A and E in Hongking. Hongkong Med. J. 1997, 3, 79–82. [Google Scholar]
- Department of Health Family Health Service. Schedule of Hong Kong Childhood Immunisation Programme. 2020. Available online: https://www.fhs.gov.hk/english/main_ser/child_health/child_health_recommend.html (accessed on 16 August 2021).
- National Institutes of Infectious Diseases. Hepatitis A in Japan between 2015 and March 2019. IASR 2019, 40, 147–148. [Google Scholar]
- Kiyohara, T.; Sato, T.; Totsuka, A.; Miyamura, T.; Ito, T.; Yoneyama, T. Shifting seroepidemiology of hepatitis A in Japan, 1973–2003. Microbiol. Immunol. 2007, 51, 185–191. [Google Scholar] [CrossRef]
- Koff, R.S. Clinical manifestations and diagnosis of hepatitis A virus infection. Vaccine 1992, 10 (Suppl. S1), S15–S17. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, C.; Ko, K.; Nagashima, S.; Harakawa, T.; Fujii, T.; Ohisa, M.; Katayama, K.; Takahashi, K.; Okamoto, H.; Tanaka, J. Very low prevalence of anti-HAV in Japan: High potential for future outbreak. Sci. Rep. 2019, 9, 1493. [Google Scholar] [CrossRef] [PubMed]
- Saitoh, A.; Okabe, N. Progress and challenges for the Japanese immunization program: Beyond the “vaccine gap”. Vaccine 2018, 36, 4582–4588. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Infectious Diseases. Routine/Voluntary Immunization Schedule in Japan. 2016. Available online: https://www.niid.go.jp/niid/images/vaccine/schedule/2016/EN20161001.pdf (accessed on 27 August 2022).
- Lim, J.; Kim, K.; Choi, S.; Park, S.M. The effectiveness and limitation of the national childhood hepatitis A vaccination program in the Republic of Korea: Findings from the Korean National Health and Nutrition Examination Survey (KNHANES), 2015. PLoS ONE 2017, 12, e0189210. [Google Scholar] [CrossRef]
- Moon, S.; Han, J.H.; Bae, G.-R.; Cho, E.; Kim, B. Hepatitis A in Korea from 2011 to 2013: Current Epidemiologic Status and Regional Distribution. J. Korean Med. Sci. 2016, 31, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.G.; Choi, M.J.; Yoon, J.W.; Noh, J.Y.; Song, J.Y.; Cheong, H.J.; Kim, W.J. Seroprevalence and disease burden of acute hepatitis A in adult population in South Korea. PLoS ONE 2017, 12, e0186257. [Google Scholar] [CrossRef]
- Yoon, E.L.; Sinn, D.H.; Lee, H.W.; Kim, J.H. Current status and strategies for the control of viral hepatitis A in Korea. Clin. Mol. Hepatol. 2017, 23, 196–204. [Google Scholar] [CrossRef]
- Chang, Y.; Kim, C.; Kim, N.; Kim, J.J.; Lee, H. Hepatitis A Outbreak in a Facility for the Disabled, Gyeonggi Province, Korea: An Epidemiological Investigation. J. Prev. Med. Public Health 2021, 54, 370–375. [Google Scholar] [CrossRef]
- Han-soo, L. KCDC Pegs Salted Clam as Culprit behind Hepatitis A Rise. 2019. Available online: http://www.koreabiomed.com/news/articleView.html?idxno=6431 (accessed on 5 October 2021).
- Lee, D.-Y.; Chae, S.-J.; Cho, S.-R.; Choi, W.; Kim, C.-K.; Han, M.-G. Nationwide seroprevalence of hepatitis A in South Korea from 2009 to 2019. PLoS ONE 2021, 16, e0245162. [Google Scholar] [CrossRef]
- Yoon, J.H.; Cho, S.H.; Kim, D.Y.; Yu, S.J.; Han, K.H. Epidemiological and Clinical History of Viral Hepatitis in Korea. Infect. Chemother. 2021, 53, 159–165. [Google Scholar] [CrossRef]
- Syhavong, B.; Rasachack, B.; Smythe, L.; Rolain, J.-M.; Roque-Afonso, A.-M.; Jenjaroen, K.; Soukkhaserm, V.; Phongmany, S.; Phetsouvanh, R.; Soukkhaserm, S.; et al. The infective causes of hepatitis and jaundice amongst hospitalised patients in Vientiane, Laos. Trans. R. Soc. Trop. Med. Hyg. 2010, 104, 475–483. [Google Scholar] [CrossRef]
- Khounvisith, V.; Xaiyaphet, X.; Chanthavilay, P.; Nouanthong, P.; Vongphachanh, B.; Reinharz, D.; Muller, C.P.; Black, A.P. Hepatitis A Virus in Lao People’s Democratic Republic: Seroprevalence and Risk Factors. Am. J. Trop. Med. Hyg. 2020, 103, 164–168. [Google Scholar] [CrossRef]
- Nanthavong, N.; Black, A.P.; Nouanthong, P.; Souvannaso, C.; Vilivong, K.; Muller, C.P.; Goossens, S.; Quet, F.; Buisson, Y. Diphtheria in Lao PDR: Insufficient Coverage or Ineffective Vaccine? PLoS ONE 2015, 10, e0121749. [Google Scholar] [CrossRef]
- Raihan, R. Hepatitis in Malaysia: Past, Present, and Future. Euroasian J. Hepato-Gastroenterol. 2016, 6, 52–55. [Google Scholar] [CrossRef]
- Ton, S.H.; Thiruselvam, A.; Lopez, C.G.; Noriah, R. Prevalence of hepatitis A virus infection in normal individuals and hospital patients in Kuala Lumpur. Med. J. Malays. 1983, 38, 279–281. [Google Scholar]
- Ahmad, F.; Hamzah, N.A.C.; Mustaffa, N.; Gan, S.H. Anti-hepatitis A seroprevalence among chronic viral hepatitis patients in Kelantan, Malaysia. World J. Gastroenterol. 2011, 17, 4130–4134. [Google Scholar] [CrossRef] [PubMed]
- Yusoff, F.A.; Rahman, R.A.; May, L.H.; Budart, S.B.; Sulaiman, L.H. Investigation of hepatitis A outbreak in district of Manjung, Perak, Malaysia, October 2012. West Pac. Surveil. Response J. WPSAR 2015, 6, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Hospital Sultan Ismail Johoe Bahru. Vaccination for Children in Malaysia. 2019. Available online: http://hsi.moh.gov.my/2019/04/17/vaccination-for-children-in-malaysia-2/ (accessed on 19 December 2020).
- Krishna, D.; Mohd Zulkefli, N.A.; Md Said, S.; Mahmud, A. Sociodemographic and health care factors in determining immunization defaulters among preschool children in Petaling District, Selangor: A cross-sectional study in Malaysia. BMC Public Health 2019, 19, 1275. [Google Scholar] [CrossRef] [PubMed]
- Davaalkham, D.; Enkhoyun, T.; Takahashi, M.; Nakamura, Y.; Okamoto, H. Hepatitis A and E virus infections among children in Mongolia. Am. J. Trop. Med. Hyg. 2009, 81, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Nishizawa, T.; Gotanda, Y.; Tsuda, F.; Komatsu, F.; Kawabata, T.; Hasegawa, K.; Altankhuu, M.; Chimedregzen, U.; Narantuya, L.; et al. High Prevalence of Antibodies to Hepatitis A and E Viruses and Viremia of Hepatitis B, C, and D Viruses among Apparently Healthy Populations in Mongolia. Clin. Diagn. Lab. Immunol. 2004, 11, 392–398. [Google Scholar] [CrossRef]
- Baatarkhuu, O.; Lee, H.W.; George, J.; Munkh-Orshikh, D.; Enkhtuvshin, B.; Ariunaa, S.; Eslam, M.; Ahn, S.H.; Han, K.-H.; Kim, D.Y. Acute hepatiti, A, B and C but not D is still prevalent in Mongolia: A time trend analysis. Clin. Mol. Hepatol. 2017, 23, 147–153. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for the Western Pacific. Viral hepatitis in Mongolia: Situation and Response 2015. 2016. Available online: https://apps.who.int/iris/handle/10665/208324 (accessed on 27 August 2022).
- The Institute of Environmental Science and Research Ltd. Notifiable Diseases in New Zealand: Annual Report 2018. 2020. Available online: https://surv.esr.cri.nz/PDF_surveillance/AnnualRpt/AnnualSurv/2018/2018AnnualNDReport_FINAL.pdf (accessed on 27 August 2022).
- Hu, X.; Collier, M.G.; Xu, F. Hepatitis A Outbreaks in Developed Countries: Detection, Control, and Prevention. Foodborne Pathog. Dis. 2020, 17, 166–171. [Google Scholar] [CrossRef] [PubMed]
- New Zealand Ministry of Health. 2020 Immunisation Schedule Change. 2020. Available online: https://www.health.govt.nz/our-work/preventative-health-wellness/immunisation/new-zealand-immunisation-schedule/2020-immunisation-schedule-change (accessed on 20 December 2020).
- Poland, G.A.; Axelsen, P.H.; Felz, M.W. Hepatitis A and B Infections Among Expatriates in Papua New Guinea: A Missed Opportunity for Immunization. J. Travel. Med. 1996, 3, 209–213. [Google Scholar] [CrossRef] [PubMed]
- National Department of Health-Papua New Guinea. Comprehensive Multi-Year Plan: National Immunization Programme 2011–2015; National Department of Health-Papua New Guinea: Port Moresby, Papua New Guinea, 2010.
- Wong, D.C.; Purcell, R.H.; Rosen, L. Prevalence of antibody to hepatitis a and hepatitis b viruses in selected populations of the south pacific. Am. J. Epidemiol. 1979, 110, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Gust, I.D.; Lehmann, N.I.; Dimitrakakis, M. A seroepidemiologic study of infection with hav and hbv in five pacific islands1. Am. J. Epidemiol. 1979, 110, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Fischer, G.E.; Thompson, N.; Chaves, S.S.; Bower, W.; Goldstein, S.; Armstrong, G.; Williams, I.; Bialek, S. The epidemiology of hepatitis A virus infections in four Pacific Island nations, 1995–2008. Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 906–910. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.; Jim, R.; Pavlin, B.I. Hepatitis A in Pohnpei State, Federated States of Micronesia, 2008–2009. Pac. Health Dialog 2010, 16, 91–97. [Google Scholar]
- Hofmeister, M.G.; McCready, J.A.; Link-Gelles, R.; Cramer, B.G.; Nolen, L.D.; Garstang, H.; Foster, M.A. Notes from the Field: Increase in Hepatitis A Virus Infections—Marshall Islands, 2016–2017. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 504–505. [Google Scholar] [CrossRef]
- Barzaga, N.; Florese, R.; Roxas, J.; Francisco, Z. Seroepidemiology of Hepatitis A virus among Filipinos living in selected communities in and around Metro Manila. Philipp. J. Microbiol. Infect. Dis. 1996, 25, 39–47. [Google Scholar]
- Carlos, J.C. Seroprevalence of Hepatitis A in 3 South East Asian Countries: Indonesia, The Philippines And Vietnam. Philipp. Counc. Health Res. Dev. 2023. Available online: https://registry.healthresearch.ph/index.php/registry?view=research&layout=details&cid=4046 (accessed on 16 November 2023).
- Department of Health. Manual of Procedures for the Philippine Integrated Disease Surveillance and Response; Department of Health: Manila, Philippines, 2014.
- DOH Philippines. Food and Water Borne Diseases Surveillance Reports 2015; DOH Philippines: Manila, Philippines, 2015.
- DOH Philippines. Food and Water Borne Diseases Surveillance Reports 2016; DOH Philippines: Manila, Philippines, 2016.
- DOH Philippines. Food and Water Borne Diseases Surveillance Reports 2017; DOH Philippines: Manila, Philippines, 2017.
- DOH Philippines. Food and Water Borne Diseases Surveillance Reports 2018; DOH Philippines: Manila, Philippines, 2018.
- DOH Philippines. Food and Water Borne Diseases Surveillance Reports 2019; DOH Philippines: Manila, Philippines, 2019.
- Outbreak News Today. Hepatitis A Outbreak Tops 200, Linked to Philippines Scallops. 2016. Available online: http://outbreaknewstoday.com/hepatitis-a-outbreak-tops-200-linked-to-philippines-scallops-34899/ (accessed on 17 August 2021).
- Asia Pacific Emerging Infections Network. Philippines: Health Department Declares Hepatitis A Outbreak. 2012. Available online: https://blogs.uw.edu/apecein/2012/09/14/philippines-health-department-declares-hepatitis-a-outbreak/#.YwnGBy8RqL0 (accessed on 16 August 2021).
- Lee, H.C.; Ang, L.W.; Chiew, P.K.T.; James, L.; Goh, K.T. Changing epidemiological patterns of hepatitis A infection in Singapore. Ann. Acad. Med. Singap. 2011, 40, 439–447. [Google Scholar] [CrossRef]
- Ministry of Health Singapore. Communicable Diseases Surveillance Report 2018. 2018: ISSN 0217-7854. Available online: https://www.moh.gov.sg/resources-statistics/reports/communicable-diseases-surveillance-in-singapore-2018 (accessed on 27 August 2022).
- Ministry of Health Singapore. Nationally Recommended Vaccines. 2021. Available online: https://www.moh.gov.sg/resources-statistics/nationally-recommended-vaccines (accessed on 27 August 2022).
- Hau, C.H.; Hien, T.T.; Tien, N.T.; Khiem, H.B.; Sac, P.K.; Nhung, V.T.; Larasati, R.P.; Khiem, H.B.; Sac, P.K.; Corwin, A.L. Prevalence of enteric hepatitis A and E viruses in the Mekong River delta region of Vietnam. Am. J. Trop. Med. Hyg. 1999, 60, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Skinhøj, P.; Aldershvile, J.; Black, F.; Kjersem, H.; Kryger, P.; Mathiesen, L. Viral hepatitis in southeast Asian refugees. J. Med. Virol. 1981, 7, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.C.; Chang, H.Y.; Kwon, O.Y.; Park, J.H.; Oh, I.S.; Kim, H.J.; Lee, J.H.; Roh, H.-J.; Lee, H.W. Seroepidemiology of Hepatitis Viruses and Hepatitis B Genotypes of Female Marriage Immigrants in Korea. Yonsei Med. J. 2018, 59, 1072–1078. [Google Scholar] [CrossRef] [PubMed]
- Le Hoang, P.; Trong, K.H.; Tran, T.T.; Huy, T.T.T.; Abe, K. Detection of hepatitis A virus RNA from children patients with acute and fulminant hepatitis of unknown etiology in Vietnam: Genomic characterization of Vietnamese HAV strain. Pediatr. Int. 2008, 50, 624–627. [Google Scholar] [CrossRef]
- Nguyen, C.; Grappasonni, I.; Scuri, S.; Nguyen, B.; Nguyen, T.; Petrelli, F. Immunization in Vietnam. Ann. Ig. 2019, 31, 291–305. [Google Scholar] [CrossRef]
- Andani, A.; van Damme, P.; Bunge, E.M.; Salgado, F.; van Hoorn, R.C.; Hoet, B. One or two doses of hepatitis A vaccine in universal vaccination programs in children in 2020: A systematic review. Vaccine 2022, 40, 196–205. [Google Scholar] [CrossRef]
- World Health Organization. WHO Position Paper on Hepatitis A Vaccines. 2022. Available online: https://www.who.int/publications/i/item/who-wer9740-493-512 (accessed on 28 September 2023).
- Hofmeister, M.G.; Xing, J.; Foster, M.A.; Augustine, R.J.; Burkholder, C.; Collins, J.; McBee, S.; Thomasson, E.D.; Thoroughman, D.; Weng, M.K.; et al. Hepatitis A Person-to-Person Outbreaks: Epidemiology, Morbidity Burden, and Factors Associated With Hospitalization—Multiple States, 2016–2019. J. Infect. Dis. 2021, 223, 426–434. [Google Scholar] [CrossRef]
- Zimmermann, R.; Faber, M.; Dudareva, S.; Ingiliz, P.; Jessen, H.; Koch, J.; Marcus, U.; Michaelis, K.; Rieck, T.; Ruscher, C.; et al. Hepatitis A outbreak among MSM in Berlin due to low vaccination coverage: Epidemiology, management, and successful interventions. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2021, 103, 146–153. [Google Scholar] [CrossRef]
- Herzog, C.; Van Herck, K.; Van Damme, P. Hepatitis A vaccination and its immunological and epidemiological long-term effects—A review of the evidence. Hum. Vaccin. Immunother. 2021, 17, 1496–1519. [Google Scholar] [CrossRef]
- Gozlan, Y.; Bar-Or, I.; Volnowitz, H.; Asulin, E.; Rich, R.; Anis, E.; Shemer, Y.; Cohen, M.S.; Dahary, E.L.; Schreiber, L.; et al. Lessons from intensified surveillance of viral hepatitis A, Israel, 2017 and 2018. Euro. Surveill. Bull. Eur. Sur. Les. Mal. Transm. Eur. Commun. Dis. Bull. 2021, 26, 2000001. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Country | Description | Number of Doses | Schedule | Route | Coverage |
|---|---|---|---|---|---|
| Australia | Hepatitis A inactivated vaccine (Vaqta® Paediatric) | 2 | 12 months, 18 months | IM | Aboriginal and Torres Strait Islander people in Queensland Northern Territory, Western Australia, and South Australia |
| China | Hepatitis A vaccine, live (HepaA-L) | 1 | 18 months | SC | Entire country |
| Hepatitis A vaccine, inactivated (HepA-I) | 2 | 18 months, 2 years | IM | Entire country | |
| Mongolia | Hepatitis A inactivated vaccine | 2 | 14 months, 2 years | IM | Entire country |
| New Zealand | Hepatitis A inactivated vaccine (Havrix) | 1 | 16+ years | IM | Transplant patients, close contact of hepatitis A cases |
| Hepatitis A inactivated vaccine (Havrix Junior) | 1 | 1 to 15 years old | IM | Transplant patients, children with chronic liver disease, close contacts of hepatitis A cases | |
| Republic of Korea | Hepatitis A inactivated vaccine | 2 | 12 to 24 months | IM | Entire country |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gloriani, N.G.; de Paz-Silava, S.L.M.; Allison, R.D.; Takashima, Y.; Avagyan, T. The Shifting Epidemiology of Hepatitis A in the World Health Organization Western Pacific Region. Vaccines 2024, 12, 204. https://doi.org/10.3390/vaccines12020204
Gloriani NG, de Paz-Silava SLM, Allison RD, Takashima Y, Avagyan T. The Shifting Epidemiology of Hepatitis A in the World Health Organization Western Pacific Region. Vaccines. 2024; 12(2):204. https://doi.org/10.3390/vaccines12020204
Chicago/Turabian StyleGloriani, Nina G., Sheriah Laine M. de Paz-Silava, Robert D. Allison, Yoshihiro Takashima, and Tigran Avagyan. 2024. "The Shifting Epidemiology of Hepatitis A in the World Health Organization Western Pacific Region" Vaccines 12, no. 2: 204. https://doi.org/10.3390/vaccines12020204