
Key Considerations during the Transition from the Acute Phase of the COVID-19 Pandemic: A Narrative Review

 ,
,  , , , ,
, , , ,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
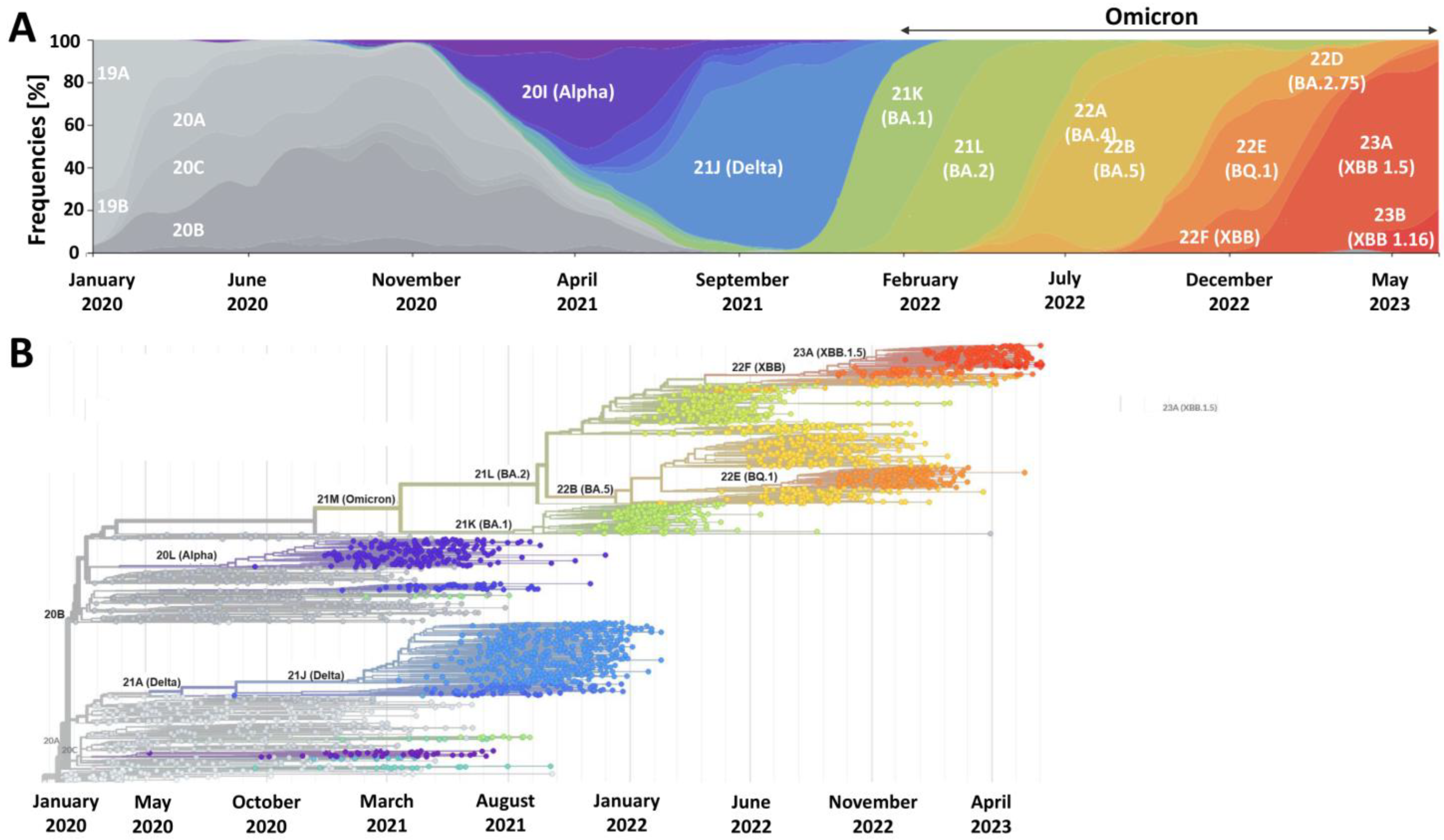
2. SARS-CoV-2 Is Here to Stay and Will Continue to Evolve
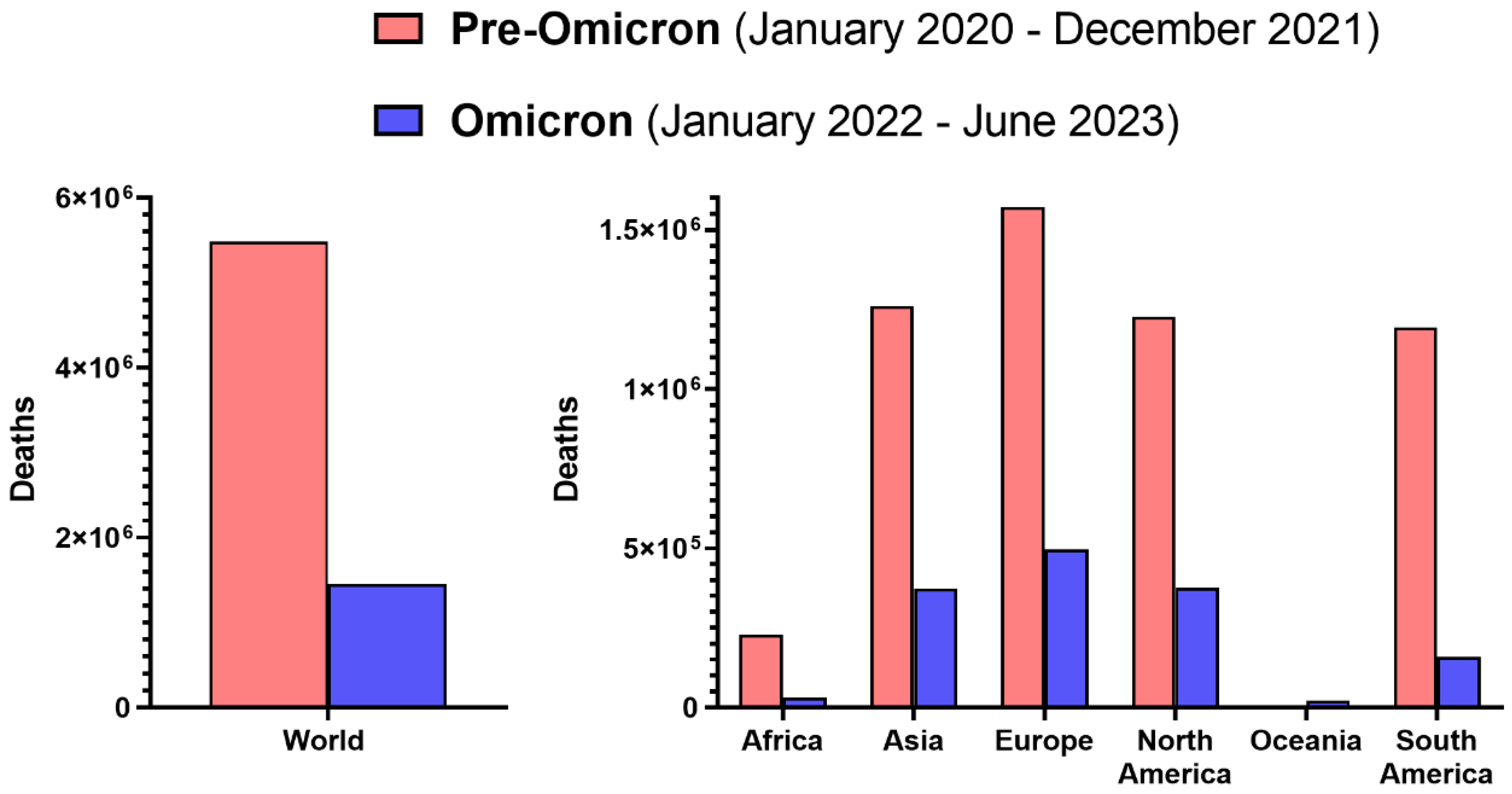
3. Omicron Lineage Is Milder but Not Negligible
4. Future Viral Variants May Not Always Cause Milder Disease
5. Vaccines Remain a Key Component of Primary COVID-19 Prevention
6. Simplifying COVID-19 Booster Vaccination Will Improve Vaccine Acceptance and Intake
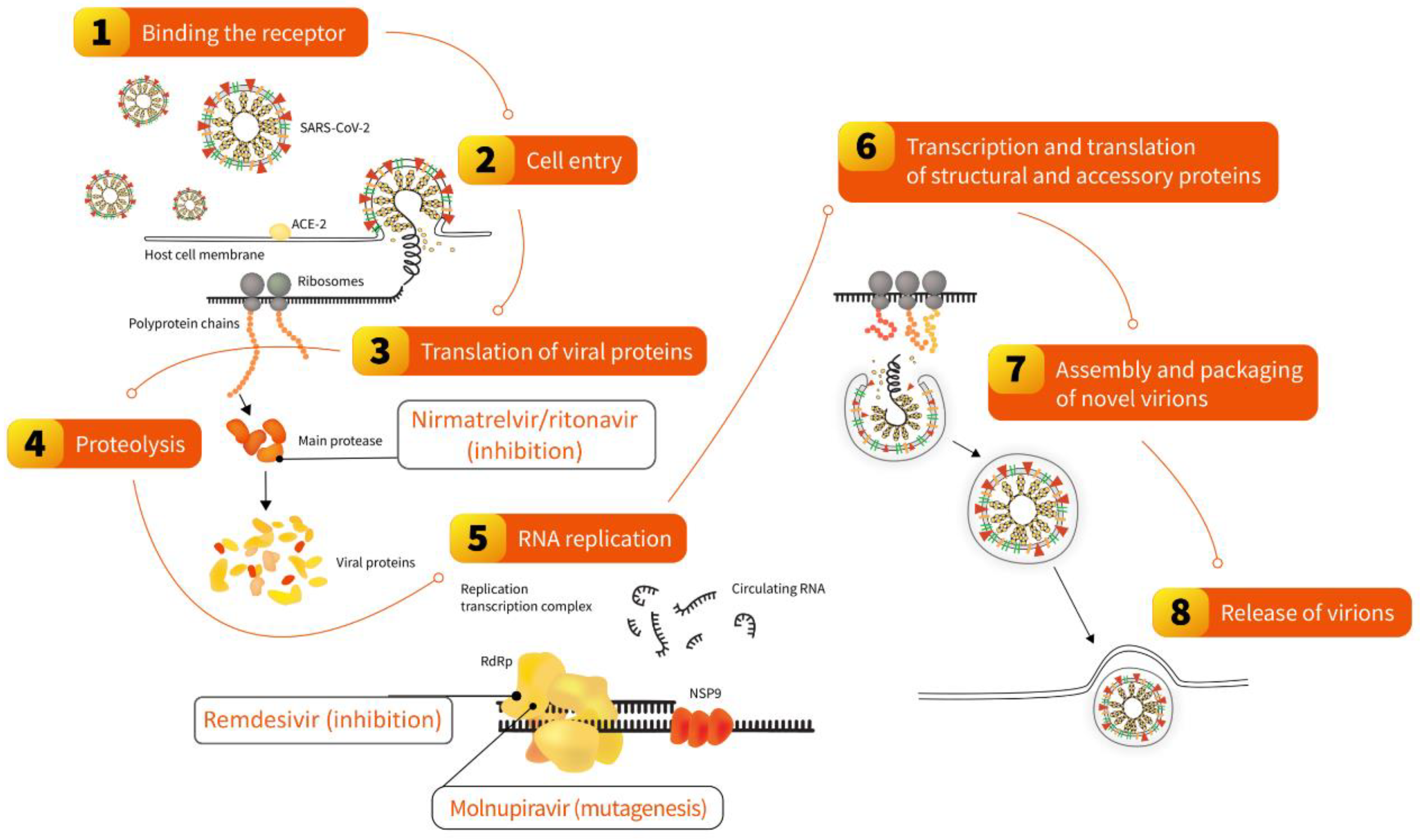
7. Antivirals Represent a Strategy to Adapt to Long-Term Co-Existence with SARS-CoV-2
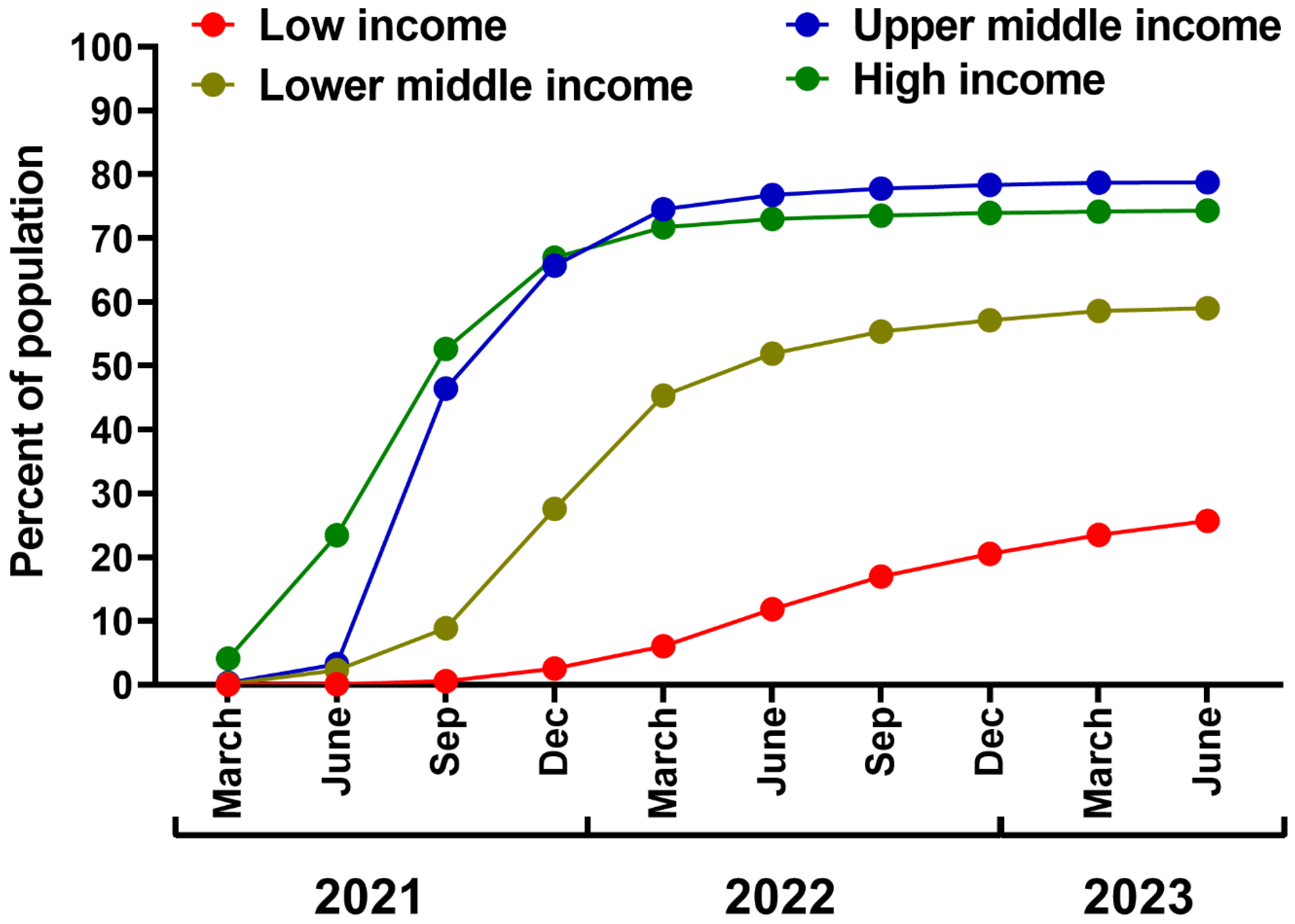
8. Leaving No Country Behind: Low-Income Regions Require Better Access to COVID-19 Vaccines and Antivirals
9. Healthcare Workers Play a Crucial Role in Maintaining Public COVID-19 Awareness
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jiang, S.; Xia, S.; Ying, T.; Lu, L. A Novel Coronavirus (2019-NCoV) Causing Pneumonia-Associated Respiratory Syndrome. Cell. Mol. Immunol. 2020, 17, 554. [Google Scholar] [CrossRef]
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization Declares Global Emergency: A Review of the 2019 Novel Coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef]
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar]
- WHO Statement on the Fifteenth Meeting of the IHR (2005) Emergency Committee on the COVID-19 Pandemic. Available online: https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(COVID-19)-pandemic (accessed on 7 June 2023).
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; Ortiz-Ospina, E.; et al. Coronavirus Pandemic (COVID-19). Our World Data 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 10 August 2023).
- Wang, H.; Paulson, K.R.; Pease, S.A.; Watson, S.; Comfort, H.; Zheng, P.; Aravkin, A.Y.; Bisignano, C.; Barber, R.M.; Alam, T.; et al. Estimating Excess Mortality Due to the COVID-19 Pandemic: A Systematic Analysis of COVID-19-Related Mortality, 2020–2021. Lancet 2022, 399, 1513–1536. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-Acute COVID-19 Syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post-Coronavirus Disease 2019 (COVID-19) Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022, 226, 1593–1607. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Ayuzo Del Valle, N.C.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. Long-COVID in Children and Adolescents: A Systematic Review and Meta-Analyses. Sci. Rep. 2022, 12, 9950. [Google Scholar] [CrossRef]
- WHO Post COVID-19 Condition (Long COVID). Available online: https://www.who.int/europe/news-room/fact-sheets/item/post-COVID-19-condition (accessed on 19 May 2023).
- Schnitzler, L.; Janssen, L.M.M.; Evers, S.M.A.A.; Jackson, L.J.; Paulus, A.T.G.; Roberts, T.E.; Pokhilenko, I. The Broader Societal Impacts of COVID-19 and the Growing Importance of Capturing These in Health Economic Analyses. Int. J. Technol. Assess. Health Care 2021, 37, e43. [Google Scholar] [CrossRef]
- Shang, Y.; Li, H.; Zhang, R. Effects of Pandemic Outbreak on Economies: Evidence from Business History Context. Front. Public Health 2021, 9, 632043. [Google Scholar] [CrossRef]
- Miller, I.F.; Becker, A.D.; Grenfell, B.T.; Metcalf, C.J.E. Disease and Healthcare Burden of COVID-19 in the United States. Nat. Med. 2020, 26, 1212–1217. [Google Scholar] [CrossRef]
- Lenzen, M.; Li, M.; Malik, A.; Pomponi, F.; Sun, Y.-Y.; Wiedmann, T.; Faturay, F.; Fry, J.; Gallego, B.; Geschke, A.; et al. Global Socio-Economic Losses and Environmental Gains from the Coronavirus Pandemic. PLoS ONE 2020, 15, e0235654. [Google Scholar] [CrossRef] [PubMed]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef] [PubMed]
- Onyeaka, H.; Anumudu, C.K.; Al-Sharify, Z.T.; Egele-Godswill, E.; Mbaegbu, P. COVID-19 Pandemic: A Review of the Global Lockdown and Its Far-Reaching Effects. Sci. Prog. 2021, 104, 368504211019854. [Google Scholar] [CrossRef] [PubMed]
- Nowakowska, J.; Sobocińska, J.; Lewicki, M.; Lemańska, Ż.; Rzymski, P. When Science Goes Viral: The Research Response during Three Months of the COVID-19 Outbreak. Biomed. Pharmacother. 2020, 129, 110451. [Google Scholar] [CrossRef]
- Ghebreyesus, T.A.; Swaminathan, S. Scientists Are Sprinting to Outpace the Novel Coronavirus. Lancet 2020, 395, 762–764. [Google Scholar] [CrossRef]
- Cusinato, J.; Cau, Y.; Calvani, A.M.; Mori, M. Repurposing Drugs for the Management of COVID-19. Expert Opin. Ther. Pat. 2021, 31, 295–307. [Google Scholar] [CrossRef]
- Flisiak, R.; Zarębska-Michaluk, D.; Berkan-Kawińska, A.; Tudrujek-Zdunek, M.; Rogalska, M.; Piekarska, A.; Kozielewicz, D.; Kłos, K.; Rorat, M.; Bolewska, B.; et al. Remdesivir-Based Therapy Improved the Recovery of Patients with COVID-19 in the Multicenter, Real-World SARSTer Study. Pol. Arch. Intern. Med. 2021, 131, 103–110. [Google Scholar]
- Zarębska-Michaluk, D.; Jaroszewicz, J.; Rogalska, M.; Martonik, D.; Pabjan, P.; Berkan-Kawińska, A.; Bolewska, B.; Oczko-Grzesik, B.; Kozielewicz, D.; Tudrujek-Zdunek, M.; et al. Effectiveness of Tocilizumab with and without Dexamethasone in Patients with Severe COVID-19: A Retrospective Study. J. Inflamm. Res. 2021, 14, 3359–3366. [Google Scholar] [CrossRef]
- Flisiak, R.; Flisiak-Jackiewicz, M.; Rzymski, P.; Zarębska-Michaluk, D. Tocilizumab for the Treatment of COVID-19. Expert Rev. Anti-Infect. Ther. 2023, 21, 791–797. [Google Scholar] [CrossRef]
- Moniuszko-Malinowska, A.; Czupryna, P.; Zarębska-Michaluk, D.; Tomasiewicz, K.; Pancewicz, S.; Rorat, M.; Dworzańska, A.; Sikorska, K.; Bolewska, B.; Lorenc, B.; et al. Convalescent Plasma Transfusion for the Treatment of COVID-19-Experience from Poland: A Multicenter Study. J. Clin. Med. 2020, 10, 28. [Google Scholar] [CrossRef]
- Simonovich, V.A.; Burgos Pratx, L.D.; Scibona, P.; Beruto, M.V.; Vallone, M.G.; Vázquez, C.; Savoy, N.; Giunta, D.H.; Pérez, L.G.; Sánchez, M.D.L.; et al. A Randomized Trial of Convalescent Plasma in COVID-19 Severe Pneumonia. N. Engl. J. Med. 2021, 384, 619–629. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Hillyer, C.; Du, L. Neutralizing Antibodies against SARS-CoV-2 and Other Human Coronaviruses. Trends Immunol. 2020, 41, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Brobst, B.; Borger, J. Benefits and Risks of Administering Monoclonal Antibody Therapy for Coronavirus (COVID-19). StatPearls Publishing. 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK574507 (accessed on 10 August 2023).
- Rahmah, L.; Abarikwu, S.O.; Arero, A.G.; Jibril, A.T.; Fal, A.; Flisiak, R.; Makuku, R.; Marquez, L.; Mohamed, K.; Ndow, L.; et al. Oral Antiviral Treatments for COVID-19: Opportunities and Challenges. Pharmacol. Rep. 2022, 74, 1255–1278. [Google Scholar] [CrossRef] [PubMed]
- Thanh Le, T.; Andreadakis, Z.; Kumar, A.; Gómez Román, R.; Tollefsen, S.; Saville, M.; Mayhew, S. The COVID-19 Vaccine Development Landscape. Nat. Rev. Drug Discov. 2020, 19, 305–306. [Google Scholar] [CrossRef]
- Rzymski, P.; Borkowski, L.; Drąg, M.; Flisiak, R.; Jemielity, J.; Krajewski, J.; Mastalerz-Migas, A.; Matyja, A.; Pyrć, K.; Simon, K.; et al. The Strategies to Support the COVID-19 Vaccination with Evidence-Based Communication and Tackling Misinformation. Vaccines 2021, 9, 109. [Google Scholar] [CrossRef]
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global Impact of the First Year of COVID-19 Vaccination: A Mathematical Modelling Study. Lancet Infect. Dis. 2022, 22, 1293–1302. [Google Scholar] [CrossRef]
- Zheng, C.; Shao, W.; Chen, X.; Zhang, B.; Wang, G.; Zhang, W. Real-World Effectiveness of COVID-19 Vaccines: A Literature Review and Meta-Analysis. Int. J. Infect. Dis. 2022, 114, 252–260. [Google Scholar] [CrossRef]
- Rzymski, P.; Kasianchuk, N.; Sikora, D.; Poniedziałek, B. COVID-19 Vaccinations and Rates of Infections, Hospitalizations, ICU Admissions, and Deaths in Europe during SARS-CoV-2 Omicron Wave in the First Quarter of 2022. J. Med. Virol. 2022, 95, e28131. [Google Scholar] [CrossRef]
- Ao, D.; He, X.; Hong, W.; Wei, X. The Rapid Rise of SARS-CoV-2 Omicron Subvariants with Immune Evasion Properties: XBB.1.5 and BQ.1.1 Subvariants. MedComm 2023, 4, e239. [Google Scholar] [CrossRef]
- Willett, B.J.; Grove, J.; MacLean, O.A.; Wilkie, C.; De Lorenzo, G.; Furnon, W.; Cantoni, D.; Scott, S.; Logan, N.; Ashraf, S.; et al. SARS-CoV-2 Omicron Is an Immune Escape Variant with an Altered Cell Entry Pathway. Nat. Microbiol. 2022, 7, 1161–1179. [Google Scholar] [CrossRef]
- Qu, P.; Faraone, J.N.; Evans, J.P.; Zheng, Y.-M.; Carlin, C.; Anghelina, M.; Stevens, P.; Fernandez, S.; Jones, D.; Panchal, A.R.; et al. Enhanced Evasion of Neutralizing Antibody Response by Omicron XBB.1.5, CH.1.1, and CA.3.1 Variants. Cell Rep. 2023, 42, 112443. [Google Scholar] [CrossRef] [PubMed]
- Rzymski, P.; Camargo, C.A.; Fal, A.; Flisiak, R.; Gwenzi, W.; Kelishadi, R.; Leemans, A.; Nieto, J.J.; Ozen, A.; Perc, M.; et al. COVID-19 Vaccine Boosters: The Good, the Bad, and the Ugly. Vaccines 2021, 9, 1299. [Google Scholar] [CrossRef] [PubMed]
- Woldemeskel, B.A.; Garliss, C.C.; Blankson, J.N. MRNA Vaccine-Elicited SARS-CoV-2-Specific T Cells Persist at 6 Months and Recognize the Delta Variant. Clin. Infect. Dis. 2021, 75, e898–e901. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.C.; Shin, B.-H.; Gadsden, T.-A.M.; Chu, M.; Petrosyan, A.; Le, C.N.; Zabner, R.; Oft, J.; Pedraza, I.; Cheng, S.; et al. T Cell Immune Responses to SARS-CoV-2 and Variants of Concern (Alpha and Delta) in Infected and Vaccinated Individuals. Cell. Mol. Immunol. 2021, 18, 2554–2556. [Google Scholar] [CrossRef]
- Jergovic, M.; Coplen, C.P.; Uhrlaub, J.L.; Beitel, S.C.; Burgess, J.L.; Lutrick, K.; Ellingson, K.D.; Watanabe, M.; Nikolich-Žugich, J. Resilient T Cell Responses to B.1.1.529 (Omicron) SARS-CoV-2 Variant. medRxiv 2022. [Google Scholar] [CrossRef]
- Collier, D.A.; Ferreira, I.A.T.M.; Kotagiri, P.; Datir, R.P.; Lim, E.Y.; Touizer, E.; Meng, B.; Abdullahi, A.; CITIID-NIHR BioResource COVID-19 Collaboration; Elmer, A.; et al. Age-Related Immune Response Heterogeneity to SARS-CoV-2 Vaccine BNT162b2. Nature 2021, 596, 417–422. [Google Scholar] [CrossRef]
- Brosh-Nissimov, T.; Orenbuch-Harroch, E.; Chowers, M.; Elbaz, M.; Nesher, L.; Stein, M.; Maor, Y.; Cohen, R.; Hussein, K.; Weinberger, M.; et al. BNT162b2 Vaccine Breakthrough: Clinical Characteristics of 152 Fully Vaccinated Hospitalized COVID-19 Patients in Israel. Clin. Microbiol. Infect. 2021, 27, 1652–1657. [Google Scholar] [CrossRef]
- Hallam, J.; Jones, T.; Alley, J.; Kohut, M.L. Exercise after Influenza or COVID-19 Vaccination Increases Serum Antibody without an Increase in Side Effects. Brain Behav. Immun. 2022, 102, 1–10. [Google Scholar] [CrossRef]
- Rzymski, P.; Pazgan-Simon, M.; Kamerys, J.; Moniuszko-Malinowska, A.; Sikorska, K.; Wernik, J.; Zarębska-Michaluk, D.; Supronowicz, Ł.; Sobala-Szczygieł, B.; Skrzat-Klapaczyńska, A.; et al. Severe Breakthrough COVID-19 Cases during Six Months of Delta Variant (B.1.617.2) Domination in Poland. Vaccines 2022, 10, 557. [Google Scholar] [CrossRef]
- WHO. Available online: https://apps.who.int/iris/rest/bitstreams/1484818/retrieve (accessed on 10 August 2023).
- Markov, P.V.; Ghafari, M.; Beer, M.; Lythgoe, K.; Simmonds, P.; Stilianakis, N.I.; Katzourakis, A. The Evolution of SARS-CoV-2. Nat. Rev. Microbiol. 2023, 21, 361–379. [Google Scholar] [CrossRef]
- Strassburg, M.A. The Global Eradication of Smallpox. Am. J. Infect. Control 1982, 10, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Combe, M.; Sanjuán, R. Variation in RNA Virus Mutation Rates across Host Cells. PLoS Pathog. 2014, 10, e1003855. [Google Scholar] [CrossRef] [PubMed]
- Amicone, M.; Borges, V.; Alves, M.J.; Isidro, J.; Zé-Zé, L.; Duarte, S.; Vieira, L.; Guiomar, R.; Gomes, J.P.; Gordo, I. Mutation Rate of SARS-CoV-2 and Emergence of Mutators during Experimental Evolution. Evol. Med. Public Health 2022, 10, 142–155. [Google Scholar] [CrossRef] [PubMed]
- Manzanares-Meza, L.D.; Medina-Contreras, O. SARS-CoV-2 and Influenza: A Comparative Overview and Treatment Implications. Bol. Med. Hosp. Infant. Mex. 2020, 77, 262–273. [Google Scholar] [CrossRef] [PubMed]
- Rawson, J.M.O.; Landman, S.R.; Reilly, C.S.; Mansky, L.M. HIV-1 and HIV-2 Exhibit Similar Mutation Frequencies and Spectra in the Absence of G-to-A Hypermutation. Retrovirology 2015, 12, 60. [Google Scholar] [CrossRef]
- Nakamura, F.; Takeda, H.; Ueda, Y.; Takai, A.; Takahashi, K.; Eso, Y.; Arasawa, S.; Iguchi, E.; Shimizu, T.; Mishima, M.; et al. Mutational Spectrum of Hepatitis C Virus in Patients with Chronic Hepatitis C Determined by Single Molecule Real-Time Sequencing. Sci. Rep. 2022, 12, 7083. [Google Scholar] [CrossRef]
- Korber, B.; Fischer, W.M.; Gnanakaran, S.; Yoon, H.; Theiler, J.; Abfalterer, W.; Hengartner, N.; Giorgi, E.E.; Bhattacharya, T.; Foley, B.; et al. Tracking Changes in SARS-CoV-2 Spike: Evidence That D614G Increases Infectivity of the COVID-19 Virus. Cell 2020, 182, 812–827.e19. [Google Scholar] [CrossRef]
- Jackson, B.; Boni, M.F.; Bull, M.J.; Colleran, A.; Colquhoun, R.M.; Darby, A.C.; Haldenby, S.; Hill, V.; Lucaci, A.; McCrone, J.T.; et al. Generation and Transmission of Interlineage Recombinants in the SARS-CoV-2 Pandemic. Cell 2021, 184, 5179–5188.e8. [Google Scholar] [CrossRef]
- Chakraborty, C.; Bhattacharya, M.; Chopra, H.; Islam, M.A.; Saikumar, G.; Dhama, K. The SARS-CoV-2 Omicron Recombinant Subvariants XBB, XBB.1, and XBB.1.5 Are Expanding Rapidly with Unique Mutations, Antibody Evasion, and Immune Escape Properties—An Alarming Global Threat of a Surge in COVID-19 Cases Again? Int. J. Surg. 2023, 109, 1041–1043. [Google Scholar] [CrossRef]
- Parums, D.V. Editorial: The XBB.1.5 (‘Kraken’) Subvariant of Omicron SARS-CoV-2 and Its Rapid Global Spread. Med. Sci. Monit. 2023, 29, e939580. [Google Scholar] [CrossRef]
- Wang, R.; Chen, J.; Wei, G.-W. Mechanisms of SARS-CoV-2 Evolution Revealing Vaccine-Resistant Mutations in Europe and America. J. Phys. Chem. Lett. 2021, 12, 11850–11857. [Google Scholar] [CrossRef] [PubMed]
- Sadarangani, M.; Marchant, A.; Kollmann, T.R. Immunological Mechanisms of Vaccine-Induced Protection against COVID-19 in Humans. Nat. Rev. Immunol. 2021, 21, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Lasrado, N.; Collier, A.-R.Y.; Miller, J.; Hachmann, N.P.; Liu, J.; Sciacca, M.; Wu, C.; Anand, T.; Bondzie, E.A.; Fisher, J.L.; et al. Waning Immunity against XBB.1.5 Following Bivalent MRNA Boosters. bioRxiv 2023. [Google Scholar] [CrossRef]
- Muik, A.; Lui, B.G.; Diao, H.; Fu, Y.; Bacher, M.; Toker, A.; Grosser, J.; Ozhelvaci, O.; Grikscheit, K.; Hoehl, S.; et al. Progressive Loss of Conserved Spike Protein Neutralizing Antibody Sites in Omicron Sublineages Is Balanced by Preserved T Cell Immunity. Cell Rep. 2023, 42, 112888. [Google Scholar] [CrossRef]
- Abbasian, M.H.; Mahmanzar, M.; Rahimian, K.; Mahdavi, B.; Tokhanbigli, S.; Moradi, B.; Sisakht, M.M.; Deng, Y. Global Landscape of SARS-CoV-2 Mutations and Conserved Regions. J. Transl. Med. 2023, 21, 152. [Google Scholar] [CrossRef]
- McCafferty, S.; Haque, A.K.M.A.; Vandierendonck, A.; Weidensee, B.; Plovyt, M.; Stuchlíková, M.; François, N.; Valembois, S.; Heyndrickx, L.; Michiels, J.; et al. A Dual-Antigen Self-Amplifying RNA SARS-CoV-2 Vaccine Induces Potent Humoral and Cellular Immune Responses and Protects against SARS-CoV-2 Variants through T Cell-Mediated Immunity. Mol. Ther. 2022, 30, 2968–2983. [Google Scholar] [CrossRef]
- Nextstrain Genomic Epidemiology of SARS-CoV-2 with Subsampling Focused Globally since Pandemic Start. Available online: https://nextstrain.org/ncov/ (accessed on 14 June 2023).
- Viana, R.; Moyo, S.; Amoako, D.G.; Tegally, H.; Scheepers, C.; Althaus, C.L.; Anyaneji, U.J.; Bester, P.A.; Boni, M.F.; Chand, M.; et al. Rapid Epidemic Expansion of the SARS-CoV-2 Omicron Variant in Southern Africa. Nature 2022, 603, 679–686. [Google Scholar] [CrossRef]
- Arora, P.; Zhang, L.; Rocha, C.; Sidarovich, A.; Kempf, A.; Schulz, S.; Cossmann, A.; Manger, B.; Baier, E.; Tampe, B.; et al. Comparable Neutralisation Evasion of SARS-CoV-2 Omicron Subvariants BA.1, BA.2, and BA.3. Lancet Infect. Dis. 2022, 22, 766–767. [Google Scholar] [CrossRef]
- Liu, L.; Iketani, S.; Guo, Y.; Chan, J.F.-W.; Wang, M.; Liu, L.; Luo, Y.; Chu, H.; Huang, Y.; Nair, M.S.; et al. Striking Antibody Evasion Manifested by the Omicron Variant of SARS-CoV-2. Nature 2021, 602, 676–681. [Google Scholar] [CrossRef]
- Hui, K.P.Y.; Ho, J.C.W.; Cheung, M.-C.; Ng, K.-C.; Ching, R.H.H.; Lai, K.-L.; Kam, T.T.; Gu, H.; Sit, K.-Y.; Hsin, M.K.Y.; et al. SARS-CoV-2 Omicron Variant Replication in Human Bronchus and Lung Ex Vivo. Nature 2022, 603, 715–720. [Google Scholar] [CrossRef]
- Suzuki, R.; Yamasoba, D.; Kimura, I.; Wang, L.; Kishimoto, M.; Ito, J.; Morioka, Y.; Nao, N.; Nasser, H.; Uriu, K.; et al. Attenuated Fusogenicity and Pathogenicity of SARS-CoV-2 Omicron Variant. Nature 2022, 603, 700–705. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.-J.; Yao, L.; Zhang, H.-Y.; Zhu, K.-L.; Zhao, J.; Zhan, B.-D.; Li, Y.-K.; He, X.-J.; Huang, C.; Wang, Z.-Y.; et al. Neutralization Sensitivity, Fusogenicity, and Infectivity of Omicron Subvariants. Genome Med. 2022, 14, 146. [Google Scholar] [CrossRef] [PubMed]
- Halfmann, P.J.; Iida, S.; Iwatsuki-Horimoto, K.; Maemura, T.; Kiso, M.; Scheaffer, S.M.; Darling, T.L.; Joshi, A.; Loeber, S.; Singh, G.; et al. SARS-CoV-2 Omicron Virus Causes Attenuated Disease in Mice and Hamsters. Nature 2022, 603, 687–692. [Google Scholar] [CrossRef] [PubMed]
- Abdelnabi, R.; Foo, C.S.; Zhang, X.; Lemmens, V.; Maes, P.; Slechten, B.; Raymenants, J.; André, E.; Weynand, B.; Dallmeier, K.; et al. The Omicron (B.1.1.529) SARS-CoV-2 Variant of Concern Does Not Readily Infect Syrian Hamsters. Antivir. Res. 2022, 198, 105253. [Google Scholar] [CrossRef]
- McMahan, K.; Giffin, V.; Tostanoski, L.H.; Chung, B.; Siamatu, M.; Suthar, M.S.; Halfmann, P.; Kawaoka, Y.; Piedra-Mora, C.; Jain, N.; et al. Reduced Pathogenicity of the SARS-CoV-2 Omicron Variant in Hamsters. Med 2022, 3, 262–268.e4. [Google Scholar] [CrossRef]
- Chan, J.F.-W.; Chu, H. Pathogenicity of SARS-CoV-2 Omicron BA.1.1 in Hamsters. EBioMedicine 2022, 80, 104035. [Google Scholar] [CrossRef]
- Yu, W.; Wang, J.; Yang, Y.; Tang, C.; Yang, C.; Li, B.; Wang, H.; Zhou, Y.; Huang, Q.; Yang, H.; et al. SARS-CoV-2 Omicron (B.1.1.529) Infection in Rhesus Macaques, Hamsters, and BALB/c Mice with Severe Lung Histopathological Damage. J. Med. Virol. 2023, 95, e28846. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.M.; Polidori, L.; Antonelli, M.; Penamakuri, S.; Nogal, A.; Louca, P.; May, A.; Figueiredo, J.C.; Hu, C.; et al. Symptom Prevalence, Duration, and Risk of Hospital Admission in Individuals Infected with SARS-CoV-2 during Periods of Omicron and Delta Variant Dominance: A Prospective Observational Study from the ZOE COVID Study. Lancet 2022, 399, 1618–1624. [Google Scholar] [CrossRef]
- Flisiak, R.; Rzymski, P.; Zarębska-Michaluk, D.; Ciechanowski, P.; Dobrowolska, K.; Rogalska, M.; Jaroszewicz, J.; Szymanek-Pasternak, A.; Rorat, M.; Kozielewicz, D.; et al. Variability in the Clinical Course of COVID-19 in a Retrospective Analysis of a Large Real-World Database. Viruses 2023, 15, 149. [Google Scholar] [CrossRef]
- Consolazio, D.; Murtas, R.; Tunesi, S.; Lamberti, A.; Senatore, S.; Faccini, M.; Russo, A.G. A Comparison between Omicron and Earlier COVID-19 Variants’ Disease Severity in the Milan Area, Italy. Front. Epidemiol. 2022, 2, 891162. [Google Scholar] [CrossRef]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative Analysis of the Risks of Hospitalisation and Death Associated with SARS-CoV-2 Omicron (B.1.1.529) and Delta (B.1.617.2) Variants in England: A Cohort Study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef]
- Bager, P.; Wohlfahrt, J.; Bhatt, S.; Stegger, M.; Legarth, R.; Møller, C.H.; Skov, R.L.; Valentiner-Branth, P.; Voldstedlund, M.; Fischer, T.K.; et al. Risk of Hospitalisation Associated with Infection with SARS-CoV-2 Omicron Variant versus Delta Variant in Denmark: An Observational Cohort Study. Lancet Infect. Dis. 2022, 22, 967–976. [Google Scholar] [CrossRef]
- Jassat, W.; Abdool Karim, S.S.; Ozougwu, L.; Welch, R.; Mudara, C.; Masha, M.; Rousseau, P.; Wolmarans, M.; Selikow, A.; Govender, N.; et al. Trends in Cases, Hospitalizations, and Mortality Related to the Omicron BA.4/BA.5 Subvariants in South Africa. Clin. Infect. Dis. 2023, 76, 1468–1475. [Google Scholar] [CrossRef]
- Pung, R.; Kong, X.P.; Cui, L.; Chae, S.-R.; Chen, M.I.-C.; Lee, V.J.; Marc Ho, Z.J. Severity of SARS-CoV-2 Omicron XBB Subvariants in Singapore. Lancet Reg. Health—West. Pac. 2023, 37, 100849. [Google Scholar]
- Karyakarte, R.P.; Das, R.; Rajmane, M.V.; Dudhate, S.; Agarasen, J.; Pillai, P.; Chandankhede, P.M.; Labhshetwar, R.S.; Gadiyal, Y.; Kulkarni, P.P.; et al. Chasing SARS-CoV-2 XBB.1.16 Recombinant Lineage in India and the Clinical Profile of XBB.1.16 Cases in Maharashtra, India. Cureus 2023, 15, e39816. [Google Scholar] [CrossRef]
- Flisiak, R.; Zarębska-Michaluk, D.; Dobrowolska, K.; Rorat, M.; Rogalska, M.; Kryńska, J.A.; Moniuszko-Malinowska, A.; Czupryna, P.; Kozielewicz, D.; Jaroszewicz, J.; et al. Change in the Clinical Picture of Hospitalized Patients with COVID-19 between the Early and Late Period of Dominance of the Omicron SARS-CoV-2 Variant. J. Clin. Med. 2023, 12, 5572. [Google Scholar] [CrossRef]
- World Health Organization Influenza. Available online: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal) (accessed on 14 June 2023).
- Portmann, L.; de Kraker, M.E.A.; Fröhlich, G.; Thiabaud, A.; Roelens, M.; Schreiber, P.W.; Troillet, N.; Iten, A.; Widmer, A.; Harbarth, S.; et al. Hospital Outcomes of Community-Acquired SARS-CoV-2 Omicron Variant Infection Compared with Influenza Infection in Switzerland. JAMA Netw. Open 2023, 6, e2255599. [Google Scholar] [CrossRef]
- Taylor, C.A.; Whitaker, M.; Anglin, O.; Milucky, J.; Patel, K.; Pham, H.; Chai, S.J.; Alden, N.B.; Yousey-Hindes, K.; Anderson, E.J.; et al. COVID-19-Associated Hospitalizations among Adults during SARS-CoV-2 Delta and Omicron Variant Predominance, by Race/Ethnicity and Vaccination Status—COVID-NET, 14 States, July 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 466–473. [Google Scholar] [CrossRef]
- Antonelli, M.; Pujol, J.C.; Spector, T.D.; Ourselin, S.; Steves, C.J. Risk of Long COVID Associated with Delta versus Omicron Variants of SARS-CoV-2. Lancet 2022, 399, 2263–2264. [Google Scholar] [CrossRef]
- Thaweethai, T.; Jolley, S.E.; Karlson, E.W.; Levitan, E.B.; Levy, B.; McComsey, G.A.; McCorkell, L.; Nadkarni, G.N.; Parthasarathy, S.; Singh, U.; et al. Development of a Definition of Postacute Sequelae of SARS-CoV-2 Infection. JAMA 2023, 329, 1934–1946. [Google Scholar] [CrossRef]
- Li Wan Po, A. Omicron Variant as Nature’s Solution to the COVID-19 Pandemic. J. Clin. Pharm. Ther. 2022, 47, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Pascall, D.J.; Vink, E.; Blacow, R.; Bulteel, N.; Campbell, A.; Campbell, R.; Clifford, S.; Davis, C.; da Silva Filipe, A.; El Sakka, N.; et al. Directions of Change in Intrinsic Case Severity across Successive SARS-CoV-2 Variant Waves Have Been Inconsistent. J. Infect. 2023, 87, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Earnest, R.; Uddin, R.; Matluk, N.; Renzette, N.; Turbett, S.E.; Siddle, K.J.; Loreth, C.; Adams, G.; Tomkins-Tinch, C.H.; Petrone, M.E.; et al. Comparative Transmissibility of SARS-CoV-2 Variants Delta and Alpha in New England, USA. Cell Rep. Med. 2022, 3, 100583. [Google Scholar] [CrossRef] [PubMed]
- King, K.L.; Wilson, S.; Napolitano, J.M.; Sell, K.J.; Rennert, L.; Parkinson, C.L.; Dean, D. SARS-CoV-2 Variants of Concern Alpha and Delta Show Increased Viral Load in Saliva. PLoS ONE 2022, 17, e0267750. [Google Scholar] [CrossRef]
- Yuasa, S.; Nakajima, J.; Takatsuki, Y.; Takahashi, Y.; Tani-Sassa, C.; Iwasaki, Y.; Nagano, K.; Sonobe, K.; Yoshimoto, T.; Nukui, Y.; et al. Viral Load of SARS-CoV-2 Omicron Is Not High despite Its High Infectivity. J. Med. Virol. 2022, 94, 5543–5546. [Google Scholar] [CrossRef]
- Laitman, A.M.; Lieberman, J.A.; Hoffman, N.G.; Roychoudhury, P.; Mathias, P.C.; Greninger, A.L. The SARS-CoV-2 Omicron Variant Does Not Have Higher Nasal Viral Loads Compared to the Delta Variant in Symptomatic and Asymptomatic Individuals. J. Clin. Microbiol. 2022, 60, e0013922. [Google Scholar] [CrossRef]
- Puhach, O.; Adea, K.; Hulo, N.; Sattonnet, P.; Genecand, C.; Iten, A.; Jacquérioz, F.; Kaiser, L.; Vetter, P.; Eckerle, I.; et al. Infectious Viral Load in Unvaccinated and Vaccinated Individuals Infected with Ancestral, Delta or Omicron SARS-CoV-2. Nat. Med. 2022, 28, 1491–1500. [Google Scholar] [CrossRef]
- Wu, L.; Zhou, L.; Mo, M.; Liu, T.; Wu, C.; Gong, C.; Lu, K.; Gong, L.; Zhu, W.; Xu, Z. SARS-CoV-2 Omicron RBD Shows Weaker Binding Affinity than the Currently Dominant Delta Variant to Human ACE2. Signal Transduct. Target. Ther. 2022, 7, 8. [Google Scholar] [CrossRef]
- Meng, B.; Abdullahi, A.; Ferreira, I.A.T.M.; Goonawardane, N.; Saito, A.; Kimura, I.; Yamasoba, D.; Gerber, P.P.; Fatihi, S.; Rathore, S.; et al. Altered TMPRSS2 Usage by SARS-CoV-2 Omicron Impacts Infectivity and Fusogenicity. Nature 2022, 603, 706–714. [Google Scholar] [CrossRef]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal Dynamics in Viral Shedding and Transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef]
- Manica, M.; De Bellis, A.; Guzzetta, G.; Mancuso, P.; Vicentini, M.; Venturelli, F.; Zerbini, A.; Bisaccia, E.; Litvinova, M.; Menegale, F.; et al. Intrinsic Generation Time of the SARS-CoV-2 Omicron Variant: An Observational Study of Household Transmission. Lancet Reg. Health Eur. 2022, 19, 100446. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Tang, L.; Zhu, L.; Zhu, Y.; Yang, S.; Chen, W.; Fan, Y.; Yang, X.; Yang, S.; Zheng, Y.; et al. Viral Dynamics during SARS-CoV-2 Omicron Infection Highlight Presymptomatic and Asymptomatic Infectiousness. J. Infect. 2023, 86, 537–539. [Google Scholar] [CrossRef] [PubMed]
- Fajnzylber, J.; Regan, J.; Coxen, K.; Corry, H.; Wong, C.; Rosenthal, A.; Worrall, D.; Giguel, F.; Piechocka-Trocha, A.; Atyeo, C.; et al. SARS-CoV-2 Viral Load Is Associated with Increased Disease Severity and Mortality. Nat. Commun. 2020, 11, 5493. [Google Scholar] [CrossRef]
- Saito, A.; Irie, T.; Suzuki, R.; Maemura, T.; Nasser, H.; Uriu, K.; Kosugi, Y.; Shirakawa, K.; Sadamasu, K.; Kimura, I.; et al. Enhanced Fusogenicity and Pathogenicity of SARS-CoV-2 Delta P681R Mutation. Nature 2022, 602, 300–306. [Google Scholar] [CrossRef]
- Kimura, I.; Yamasoba, D.; Tamura, T.; Nao, N.; Suzuki, T.; Oda, Y.; Mitoma, S.; Ito, J.; Nasser, H.; Zahradnik, J.; et al. Virological Characteristics of the SARS-CoV-2 Omicron BA.2 Subvariants, Including BA.4 and BA.5. Cell 2022, 185, 3992–4007.e16. [Google Scholar] [CrossRef] [PubMed]
- Xia, S.; Wang, L.; Jiao, F.; Yu, X.; Xu, W.; Huang, Z.; Li, X.; Wang, Q.; Zhu, Y.; Man, Q.; et al. SARS-CoV-2 Omicron Subvariants Exhibit Distinct Fusogenicity, but Similar Sensitivity, to Pan-CoV Fusion Inhibitors. Emerg. Microbes Infect. 2023, 12, 2178241. [Google Scholar] [CrossRef]
- Xia, S.; Jiao, F.; Wang, L.; Yu, X.; Lu, T.; Fu, Y.; Huang, Z.; Li, X.; Huang, J.; Wang, Q.; et al. SARS-CoV-2 Omicron XBB Subvariants Exhibit Enhanced Fusogenicity and Substantial Immune Evasion in Elderly Population, but High Sensitivity to Pan-Coronavirus Fusion Inhibitors. J. Med. Virol. 2023, 95, e28641. [Google Scholar] [CrossRef]
- Yuan, S.; Ye, Z.-W.; Liang, R.; Tang, K.; Zhang, A.J.; Lu, G.; Ong, C.P.; Man Poon, V.K.; Chan, C.C.-S.; Mok, B.W.-Y.; et al. Pathogenicity, Transmissibility, and Fitness of SARS-CoV-2 Omicron in Syrian Hamsters. Science 2022, 377, 428–433. [Google Scholar] [CrossRef]
- Hoffmann, M.; Wong, L.-Y.R.; Arora, P.; Zhang, L.; Rocha, C.; Odle, A.; Nehlmeier, I.; Kempf, A.; Richter, A.; Halwe, N.J.; et al. Omicron Subvariant BA.5 Efficiently Infects Lung Cells. Nat. Commun. 2023, 14, 3500. [Google Scholar] [CrossRef]
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.J.; Amoako, D.G.; Everatt, J.; Bhiman, J.N.; Scheepers, C.; et al. Clinical Severity of SARS-CoV-2 Omicron BA.4 and BA.5 Lineages Compared to BA.1 and Delta in South Africa. Nat. Commun. 2022, 13, 5860. [Google Scholar] [CrossRef]
- Robertson, C.; Kerr, S.; Sheikh, A. Severity of Omicron BA.5 Variant and Protective Effect of Vaccination: National Cohort and Matched Analyses in Scotland. Lancet Reg. Health Eur. 2023, 28, 100638. [Google Scholar] [CrossRef] [PubMed]
- Ciuffreda, L.; Lorenzo-Salazar, J.M.; García-Martínez de Artola, D.; Gil-Campesino, H.; Alcoba-Florez, J.; Rodríguez-Pérez, H.; Íñigo-Campos, A.; Salas-Hernández, J.; Rodríguez-Nuñez, J.; Muñoz-Barrera, A.; et al. Reinfection Rate and Disease Severity of the BA.5 Omicron SARS-CoV-2 Lineage Compared to Previously Circulating Variants of Concern in the Canary Islands (Spain). Emerg. Microbes Infect. 2023, 12, 2202281. [Google Scholar] [CrossRef] [PubMed]
- Oude Munnink, B.B.; Sikkema, R.S.; Nieuwenhuijse, D.F.; Molenaar, R.J.; Munger, E.; Molenkamp, R.; van der Spek, A.; Tolsma, P.; Rietveld, A.; Brouwer, M.; et al. Transmission of SARS-CoV-2 on Mink Farms between Humans and Mink and Back to Humans. Science 2021, 371, 172–177. [Google Scholar] [CrossRef]
- Hoffmann, M.; Zhang, L.; Krüger, N.; Graichen, L.; Kleine-Weber, H.; Hofmann-Winkler, H.; Kempf, A.; Nessler, S.; Riggert, J.; Winkler, M.S.; et al. SARS-CoV-2 Mutations Acquired in Mink Reduce Antibody-Mediated Neutralization. Cell Rep. 2021, 35, 109017. [Google Scholar] [CrossRef]
- Domańska-Blicharz, K.; Orłowska, A.; Smreczak, M.; Niemczuk, K.; Iwan, E.; Bomba, A.; Lisowska, A.; Opolska, J.; Trębas, P.; Potyrało, P.; et al. Mink SARS-CoV-2 Infection in Poland—Short Communication. J. Vet. Res. 2021, 65, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Palmer, M.V.; Martins, M.; Falkenberg, S.; Buckley, A.; Caserta, L.C.; Mitchell, P.K.; Cassmann, E.D.; Rollins, A.; Zylich, N.C.; Renshaw, R.W.; et al. Susceptibility of White-Tailed Deer (Odocoileus Virginianus) to SARS-CoV-2. J. Virol. 2021, 95, e00083-2. [Google Scholar] [CrossRef]
- Chandler, J.C.; Bevins, S.N.; Ellis, J.W.; Linder, T.J.; Tell, R.M.; Jenkins-Moore, M.; Root, J.J.; Lenoch, J.B.; Robbe-Austerman, S.; DeLiberto, T.J.; et al. SARS-CoV-2 Exposure in Wild White-Tailed Deer (Odocoileus Virginianus). Proc. Natl. Acad. Sci. USA 2021, 118, e2114828118. [Google Scholar] [CrossRef]
- Li, L.; Han, P.; Huang, B.; Xie, Y.; Li, W.; Zhang, D.; Han, P.; Xu, Z.; Bai, B.; Zhou, J.; et al. Broader-Species Receptor Binding and Structural Bases of Omicron SARS-CoV-2 to Both Mouse and Palm-Civet ACE2s. Cell Discov. 2022, 8, 65. [Google Scholar] [CrossRef]
- Konishi, T. SARS-CoV-2 Mutations among Minks Show Reduced Lethality and Infectivity to Humans. PLoS ONE 2021, 16, e0247626. [Google Scholar] [CrossRef]
- Devaux, C.A.; Pinault, L.; Delerce, J.; Raoult, D.; Levasseur, A.; Frutos, R. Spread of Mink SARS-CoV-2 Variants in Humans: A Model of Sarbecovirus Interspecies Evolution. Front. Microbiol. 2021, 12, 675528. [Google Scholar] [CrossRef]
- Willgert, K.; Didelot, X.; Surendran-Nair, M.; Kuchipudi, S.V.; Ruden, R.M.; Yon, M.; Nissly, R.H.; Vandegrift, K.J.; Nelli, R.K.; Li, L.; et al. Transmission History of SARS-CoV-2 in Humans and White-Tailed Deer. Sci. Rep. 2022, 12, 12094. [Google Scholar] [CrossRef] [PubMed]
- Kuchipudi, S.V.; Surendran-Nair, M.; Ruden, R.M.; Yon, M.; Nissly, R.H.; Vandegrift, K.J.; Nelli, R.K.; Li, L.; Jayarao, B.M.; Maranas, C.D.; et al. Multiple Spillovers from Humans and Onward Transmission of SARS-CoV-2 in White-Tailed Deer. Proc. Natl. Acad. Sci. USA 2022, 119, e2121644119. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Cantor, J.; Simon, K.I.; Bento, A.I.; Wing, C.; Whaley, C.M. Vaccinations against COVID-19 May Have Averted up to 140,000 Deaths in the United States. Health Aff. 2021, 40, 1465–1472. [Google Scholar] [CrossRef]
- Kayano, T.; Sasanami, M.; Kobayashi, T.; Ko, Y.K.; Otani, K.; Suzuki, M.; Nishiura, H. Number of Averted COVID-19 Cases and Deaths Attributable to Reduced Risk in Vaccinated Individuals in Japan. Lancet Reg. Health West. Pac. 2022, 28, 100571. [Google Scholar] [CrossRef]
- Mattiuzzi, C.; Henry, B.M.; Lippi, G. COVID-19 Vaccination Uptake Strongly Predicts Averted Deaths of Older People across Europe. Biomed. J. 2022, 45, 961–962. [Google Scholar] [CrossRef] [PubMed]
- Sikora, D.; Rzymski, P. COVID-19 Vaccination and Rates of Infections, Hospitalizations, ICU Admissions, and Deaths in the European Economic Area during Autumn 2021 Wave of SARS-CoV-2. Vaccines 2022, 10, 437. [Google Scholar] [CrossRef]
- Yi, S.; Choe, Y.J.; Lim, D.S.; Lee, H.R.; Kim, J.; Kim, Y.-Y.; Kim, R.K.; Jang, E.J.; Lee, S.; Park, E.; et al. Impact of National COVID-19 Vaccination Campaign, South Korea. Vaccine 2022, 40, 3670–3675. [Google Scholar] [CrossRef]
- McCarthy, C.V.; O’Mara, O.; van Leeuwen, E.; CMMID COVID-19 Working Group; Jit, M.; Sandmann, F. The Impact of COVID-19 Vaccination in Prisons in England and Wales: A Metapopulation Model. BMC Public Health 2022, 22, 1003. [Google Scholar] [CrossRef]
- Santos, C.V.B.D.; de Noronha, T.G.; Werneck, G.L.; Struchiner, C.J.; Villela, D.A.M. Estimated COVID-19 Severe Cases and Deaths Averted in the First Year of the Vaccination Campaign in Brazil: A Retrospective Observational Study. Lancet Reg. Health Am. 2023, 17, 100418. [Google Scholar] [CrossRef]
- Haas, E.J.; McLaughlin, J.M.; Khan, F.; Angulo, F.J.; Anis, E.; Lipsitch, M.; Singer, S.R.; Mircus, G.; Brooks, N.; Smaja, M.; et al. Infections, Hospitalisations, and Deaths Averted via a Nationwide Vaccination Campaign Using the Pfizer-BioNTech BNT162b2 MRNA COVID-19 Vaccine in Israel: A Retrospective Surveillance Study. Lancet Infect. Dis. 2022, 22, 357–366. [Google Scholar] [CrossRef]
- Sacco, C.; Mateo-Urdiales, A.; Petrone, D.; Spuri, M.; Fabiani, M.; Vescio, M.F.; Bressi, M.; Riccardo, F.; Del Manso, M.; Bella, A.; et al. Estimating Averted COVID-19 Cases, Hospitalisations, Intensive Care Unit Admissions and Deaths by COVID-19 Vaccination, Italy, January-September 2021. Eurosurveillance 2021, 26, 2101001. [Google Scholar] [CrossRef] [PubMed]
- Brannock, M.D.; Chew, R.F.; Preiss, A.J.; Hadley, E.C.; Redfield, S.; McMurry, J.A.; Leese, P.J.; Girvin, A.T.; Crosskey, M.; Zhou, A.G.; et al. Long COVID Risk and Pre-COVID Vaccination in an EHR-Based Cohort Study from the RECOVER Program. Nat. Commun. 2023, 14, 2914. [Google Scholar] [CrossRef] [PubMed]
- Simon, M.A.; Luginbuhl, R.D.; Parker, R. Reduced Incidence of Long-COVID Symptoms Related to Administration of COVID-19 Vaccines Both before COVID-19 Diagnosis and up to 12 Weeks After. medRxiv 2021. [Google Scholar] [CrossRef]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk Factors and Disease Profile of Post-Vaccination SARS-CoV-2 Infection in UK Users of the COVID Symptom Study App: A Prospective, Community-Based, Nested, Case-Control Study. Lancet Infect. Dis. 2022, 22, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Senjam, S.S.; Balhara, Y.P.S.; Kumar, P.; Nichal, N.; Manna, S.; Madan, K.; Ahmed, N.H.; Gupta, N.; Sharma, R.; Gupta, Y.; et al. Assessment of Post COVID-19 Health Problems and Its Determinants in North India: A Descriptive Cross Section Study. medRxiv 2021. [Google Scholar] [CrossRef]
- Ayoubkhani, D.; Bosworth, M.L.; King, S.; Pouwels, K.B.; Glickman, M.; Nafilyan, V.; Zaccardi, F.; Khunti, K.; Alwan, N.A.; Walker, A.S. Risk of Long COVID in People Infected with Severe Acute Respiratory Syndrome Coronavirus 2 after 2 Doses of a Coronavirus Disease 2019 Vaccine: Community-Based, Matched Cohort Study. Open Forum Infect. Dis. 2022, 9, ofac464. [Google Scholar] [CrossRef] [PubMed]
- Al-Aly, Z.; Bowe, B.; Xie, Y. Long COVID after Breakthrough SARS-CoV-2 Infection. Nat. Med. 2022, 28, 1461–1467. [Google Scholar] [CrossRef]
- Taquet, M.; Dercon, Q.; Harrison, P.J. Six-Month Sequelae of Post-Vaccination SARS-CoV-2 Infection: A Retrospective Cohort Study of 10,024 Breakthrough Infections. Brain Behav. Immun. 2022, 103, 154–162. [Google Scholar] [CrossRef]
- Notarte, K.I.; Catahay, J.A.; Velasco, J.V.; Pastrana, A.; Ver, A.T.; Pangilinan, F.C.; Peligro, P.J.; Casimiro, M.; Guerrero, J.J.; Gellaco, M.M.L.; et al. Impact of COVID-19 Vaccination on the Risk of Developing Long-COVID and on Existing Long-COVID Symptoms: A Systematic Review. EClinicalMedicine 2022, 53, 101624. [Google Scholar] [CrossRef]
- Yu, X.; Wei, D.; Xu, W.; Li, Y.; Li, X.; Zhang, X.; Qu, J.; Yang, Z.; Chen, E. Reduced Sensitivity of SARS-CoV-2 Omicron Variant to Antibody Neutralization Elicited by Booster Vaccination. Cell Discov. 2022, 8, 4. [Google Scholar] [CrossRef]
- Yu, J.; Collier, A.-R.Y.; Rowe, M.; Mardas, F.; Ventura, J.D.; Wan, H.; Miller, J.; Powers, O.; Chung, B.; Siamatu, M.; et al. Neutralization of the SARS-CoV-2 Omicron BA.1 and BA.2 Variants. N. Engl. J. Med. 2022, 386, 1579–1580. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.J.; Cheng, S.M.S.; Leung, K.; Lee, C.K.; Hachim, A.; Tsang, L.C.H.; Yam, K.W.H.; Chaothai, S.; Kwan, K.K.H.; Chai, Z.Y.H.; et al. Real-World COVID-19 Vaccine Effectiveness against the Omicron BA.2 Variant in a SARS-CoV-2 Infection-Naive Population. Nat. Med. 2023, 29, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, H.; Pham-Tran, D.D.; Yeoh, Z.Y.M.; Wang, B.; McMillan, M.; Andraweera, P.H.; Marshall, H.S. A Systematic Review and Meta-Analysis on the Real-World Effectiveness of COVID-19 Vaccines against Infection, Symptomatic and Severe COVID-19 Disease Caused by the Omicron Variant (B.1.1.529). Vaccines 2023, 11, 224. [Google Scholar] [CrossRef]
- Zarębska-Michaluk, D.; Hu, C.; Brzdęk, M.; Flisiak, R.; Rzymski, P. COVID-19 Vaccine Booster Strategies for Omicron SARS-CoV-2 Variant: Effectiveness and Future Prospects. Vaccines 2022, 10, 1223. [Google Scholar] [CrossRef]
- Solante, R.; Alvarez-Moreno, C.; Burhan, E.; Chariyalertsak, S.; Chiu, N.-C.; Chuenkitmongkol, S.; Dung, D.V.; Hwang, K.-P.; Ortiz Ibarra, J.; Kiertiburanakul, S.; et al. Expert Review of Global Real-World Data on COVID-19 Vaccine Booster Effectiveness and Safety during the Omicron-Dominant Phase of the Pandemic. Expert Rev. Vaccines 2023, 22, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Wu, N.; Joyal-Desmarais, K.; Ribeiro, P.A.B.; Vieira, A.M.; Stojanovic, J.; Sanuade, C.; Yip, D.; Bacon, S.L. Long-Term Effectiveness of COVID-19 Vaccines against Infections, Hospitalisations, and Mortality in Adults: Findings from a Rapid Living Systematic Evidence Synthesis and Meta-Analysis up to December, 2022. Lancet Respir. Med. 2023, 11, 439–452. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Liang, H.; Ding, X.; Cao, Y.; Yang, D.; Duan, Y. Effectiveness of COVID-19 Vaccine in Children and Adolescents with the Omicron Variant: A Systematic Review and Meta-Analysis. J. Infect. 2023, 86, e64–e66. [Google Scholar] [CrossRef]
- Mendes, D.; Chapman, R.; Aruffo, E.; Gal, P.; Nguyen, J.L.; Hamson, L.; Di Fusco, M.; Czudek, C.; Yang, J. Public Health Impact of UK COVID-19 Booster Vaccination Programs during Omicron Predominance. Expert Rev. Vaccines 2023, 22, 90–103. [Google Scholar] [CrossRef]
- Link-Gelles, R.; Ciesla, A.A.; Fleming-Dutra, K.E.; Smith, Z.R.; Britton, A.; Wiegand, R.E.; Miller, J.D.; Accorsi, E.K.; Schrag, S.J.; Verani, J.R.; et al. Effectiveness of Bivalent MRNA Vaccines in Preventing Symptomatic SARS-CoV-2 Infection—Increasing Community Access to Testing Program, United States, September-November 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1526–1530. [Google Scholar] [CrossRef]
- Link-Gelles, R.; Ciesla, A.A.; Roper, L.E.; Scobie, H.M.; Ali, A.R.; Miller, J.D.; Wiegand, R.E.; Accorsi, E.K.; Verani, J.R.; Shang, N.; et al. Early Estimates of Bivalent MRNA Booster Dose Vaccine Effectiveness in Preventing Symptomatic SARS-CoV-2 Infection Attributable to Omicron BA.5- and XBB/XBB.1.5-Related Sublineages among Immunocompetent Adults—Increasing Community Access to Testing Program, United States, December 2022-January 2023. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 119–124. [Google Scholar]
- Arbel, R.; Peretz, A.; Sergienko, R.; Friger, M.; Beckenstein, T.; Duskin-Bitan, H.; Yaron, S.; Hammerman, A.; Bilenko, N.; Netzer, D. Effectiveness of a Bivalent MRNA Vaccine Booster Dose to Prevent Severe COVID-19 Outcomes: A Retrospective Cohort Study. Lancet Infect. Dis. 2023, 23, 914–921. [Google Scholar] [CrossRef]
- Collier, A.-R.Y.; Miller, J.; Hachmann, N.P.; McMahan, K.; Liu, J.; Bondzie, E.A.; Gallup, L.; Rowe, M.; Schonberg, E.; Thai, S.; et al. Immunogenicity of BA.5 Bivalent MRNA Vaccine Boosters. N. Engl. J. Med. 2023, 388, 565–567. [Google Scholar] [CrossRef]
- Offit, P.A. Bivalent COVID-19 Vaccines—A Cautionary Tale. N. Engl. J. Med. 2023, 388, 481–483. [Google Scholar] [CrossRef]
- Wang, Q.; Bowen, A.; Valdez, R.; Gherasim, C.; Gordon, A.; Liu, L.; Ho, D.D. Antibody Response to Omicron BA.4-BA.5 Bivalent Booster. N. Engl. J. Med. 2023, 388, 567–569. [Google Scholar] [CrossRef] [PubMed]
- Carreño, J.M.; Singh, G.; Simon, V.; Krammer, F.; PVI Study Group. Bivalent COVID-19 Booster Vaccines and the Absence of BA.5-Specific Antibodies. Lancet Microbe 2023, 4, e569. [Google Scholar] [CrossRef]
- WHO Statement on the Antigen Composition of COVID-19 Vaccines. Available online: https://www.who.int/news/item/18-05-2023-statement-on-the-antigen-composition-of-COVID-19-vaccines (accessed on 18 June 2023).
- Ballouz, T.; Menges, D.; Kaufmann, M.; Amati, R.; Frei, A.; von Wyl, V.; Fehr, J.S.; Albanese, E.; Puhan, M.A. Post COVID-19 Condition after Wildtype, Delta, and Omicron SARS-CoV-2 Infection and Prior Vaccination: Pooled Analysis of Two Population-Based Cohorts. PLoS ONE 2023, 18, e0281429. [Google Scholar] [CrossRef] [PubMed]
- Rzymski, P.; Szuster-Ciesielska, A.; Dzieciątkowski, T.; Gwenzi, W.; Fal, A. MRNA Vaccines: The Future of Prevention of Viral Infections? J. Med. Virol. 2023, 95, e28572. [Google Scholar] [CrossRef] [PubMed]
- Hajnik, R.L.; Plante, J.A.; Liang, Y.; Alameh, M.-G.; Tang, J.; Bonam, S.R.; Zhong, C.; Adam, A.; Scharton, D.; Rafael, G.H.; et al. Dual Spike and Nucleocapsid MRNA Vaccination Confer Protection against SARS-CoV-2 Omicron and Delta Variants in Preclinical Models. Sci. Transl. Med. 2022, 14, eabq1945. [Google Scholar] [CrossRef]
- Alu, A.; Chen, L.; Lei, H.; Wei, Y.; Tian, X.; Wei, X. Intranasal COVID-19 Vaccines: From Bench to Bed. EBioMedicine 2022, 76, 103841. [Google Scholar] [CrossRef]
- Ramvikas, M.; Arumugam, M.; Chakrabarti, S.R.; Jaganathan, K.S. Nasal Vaccine Delivery. In Micro and Nanotechnology in Vaccine Development; Elsevier: Amsterdam, The Netherlands, 2017; pp. 279–301. ISBN 9780323399814. [Google Scholar]
- Sengupta, A.; Azharuddin, M.; Cardona, M.E.; Devito, C.; von Castelmur, E.; Wehlin, A.; Pietras, Z.; Sunnerhagen, M.; Selegård, R.; Aili, D.; et al. Intranasal Coronavirus SARS-CoV-2 Immunization with Lipid Adjuvants Provides Systemic and Mucosal Immune Response against SARS-CoV-2 S1 Spike and Nucleocapsid Protein. Vaccines 2022, 10, 504. [Google Scholar] [CrossRef]
- Shim, S.; Soh, S.H.; Im, Y.B.; Ahn, C.; Park, H.-T.; Park, H.-E.; Park, W.B.; Kim, S.; Yoo, H.S. Induction of Systemic Immunity through Nasal-Associated Lymphoid Tissue (NALT) of Mice Intranasally Immunized with Brucella Abortus Malate Dehydrogenase-Loaded Chitosan Nanoparticles. PLoS ONE 2020, 15, e0228463. [Google Scholar] [CrossRef]
- McLenon, J.; Rogers, M.A.M. The Fear of Needles: A Systematic Review and Meta-Analysis. J. Adv. Nurs. 2019, 75, 30–42. [Google Scholar] [CrossRef]
- Oladoye, M.J. Intranasal Vaccines: A Panacea to Vaccine Hesitancy? Med. Res. J. 2022, 7, 274–275. [Google Scholar] [CrossRef]
- Dhama, K.; Dhawan, M.; Tiwari, R.; Emran, T.B.; Mitra, S.; Rabaan, A.A.; Alhumaid, S.; Alawi, Z.A.; Al Mutair, A. COVID-19 Intranasal Vaccines: Current Progress, Advantages, Prospects, and Challenges. Hum. Vaccin. Immunother. 2022, 18, 2045853. [Google Scholar] [CrossRef] [PubMed]
- Madhavan, M.; Ritchie, A.J.; Aboagye, J.; Jenkin, D.; Provstgaad-Morys, S.; Tarbet, I.; Woods, D.; Davies, S.; Baker, M.; Platt, A.; et al. Tolerability and Immunogenicity of an Intranasally-Administered Adenovirus-Vectored COVID-19 Vaccine: An Open-Label Partially-Randomised Ascending Dose Phase I Trial. EBioMedicine 2022, 85, 104298. [Google Scholar] [CrossRef] [PubMed]
- van Doremalen, N.; Purushotham, J.N.; Schulz, J.E.; Holbrook, M.G.; Bushmaker, T.; Carmody, A.; Port, J.R.; Yinda, C.K.; Okumura, A.; Saturday, G.; et al. Intranasal ChAdOx1 NCoV-19/AZD1222 Vaccination Reduces Viral Shedding after SARS-CoV-2 D614G Challenge in Preclinical Models. Sci. Transl. Med. 2021, 13, eabh0755. [Google Scholar] [CrossRef]
- Ndeupen, S.; Qin, Z.; Jacobsen, S.; Bouteau, A.; Estanbouli, H.; Igyártó, B.Z. The MRNA-LNP Platform’s Lipid Nanoparticle Component Used in Preclinical Vaccine Studies Is Highly Inflammatory. iScience 2021, 24, 103479. [Google Scholar] [CrossRef] [PubMed]
- Đaković Rode, O.; Bodulić, K.; Zember, S.; Cetinić Balent, N.; Novokmet, A.; Čulo, M.; Rašić, Ž.; Mikulić, R.; Markotić, A. Decline of Anti-SARS-CoV-2 IgG Antibody Levels 6 Months after Complete BNT162b2 Vaccination in Healthcare Workers to Levels Observed Following the First Vaccine Dose. Vaccines 2022, 10, 153. [Google Scholar] [CrossRef]
- Hosseinian, S.; de Assis, R.; Khalil, G.; Luu, M.K.; Jain, A.; Horvath, P.; Nakajima, R.; Palma, A.M.; Hoang, A.; Razzak, E.; et al. Analysis and Comparison of SARS-CoV-2 Variant Antibodies and Neutralizing Activity for 6 Months after a Booster MRNA Vaccine in a Healthcare Worker Population. Front. Immunol. 2023, 14, 1166261. [Google Scholar] [CrossRef]
- Silva, M.F.S.; Pinto, A.C.M.D.; de Oliveira, F.d.C.E.; Caetano, L.F.; Araújo, F.M.d.C.; Fonseca, M.H.G. Antibody Response 6 Months after the Booster Dose of Pfizer in Previous Recipients of CoronaVac. J. Med. Virol. 2023, 95, e28169. [Google Scholar] [CrossRef]
- Townsend, J.P.; Hassler, H.B.; Dornburg, A. Infection by SARS-CoV-2 with Alternate Frequencies of MRNA Vaccine Boosting. J. Med. Virol. 2023, 95, e28461. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control COVID-19 Vaccine Tracker. Available online: https://vaccinetracker.ecdc.europa.eu/public/extensions/COVID-19/vaccine-tracker.html (accessed on 31 January 2022).
- Fieselmann, J.; Annac, K.; Erdsiek, F.; Yilmaz-Aslan, Y.; Brzoska, P. What Are the Reasons for Refusing a COVID-19 Vaccine? A Qualitative Analysis of Social Media in Germany. BMC Public Health 2022, 22, 846. [Google Scholar] [CrossRef]
- Rzymski, P.; Poniedziałek, B.; Fal, A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines 2021, 9, 1286. [Google Scholar] [CrossRef]
- Rzymski, P.; Sikora, D.; Zeyland, J.; Poniedziałek, B.; Kiedik, D.; Falfushynska, H.; Fal, A. Frequency and Nuisance Level of Adverse Events in Individuals Receiving Homologous and Heterologous COVID-19 Booster Vaccine. Vaccines 2022, 10, 754. [Google Scholar] [CrossRef]
- Sobierajski, T.; Rzymski, P.; Wanke-Rytt, M. Impact of the COVID-19 Pandemic on Attitudes toward Vaccination: Representative Study of Polish Society. Vaccines 2023, 11, 1069. [Google Scholar] [CrossRef]
- Capurro, G.; Tustin, J.; Jardine, C.G.; Driedger, S.M. When Good Messages Go Wrong: Perspectives on COVID-19 Vaccines and Vaccine Communication from Generally Vaccine Accepting Individuals in Canada. Hum. Vaccin. Immunother. 2022, 18, 2145822. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, N.; Caetano-Anollés, G. Worldwide Correlations Support COVID-19 Seasonal Behavior and Impact of Global Change. Evol. Bioinform. Online 2023, 19, 11769343231169376. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, F.; Marmiere, M.; Righetti, B.; Scquizzato, T.; Zangrillo, A.; Puglisi, R.; Landoni, G. COVID-19 Seasonality in Temperate Countries. Environ. Res. 2022, 206, 112614. [Google Scholar] [CrossRef] [PubMed]
- Wiemken, T.L.; Khan, F.; Puzniak, L.; Yang, W.; Simmering, J.; Polgreen, P.; Nguyen, J.L.; Jodar, L.; McLaughlin, J.M. Seasonal Trends in COVID-19 Cases, Hospitalizations, and Mortality in the United States and Europe. Sci. Rep. 2023, 13, 3886. [Google Scholar] [CrossRef] [PubMed]
- Gavenčiak, T.; Monrad, J.T.; Leech, G.; Sharma, M.; Mindermann, S.; Bhatt, S.; Brauner, J.; Kulveit, J. Seasonal Variation in SARS-CoV-2 Transmission in Temperate Climates: A Bayesian Modelling Study in 143 European Regions. PLoS Comput. Biol. 2022, 18, e1010435. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention National Emergency Department Visits for COVID-19, Influenza, and Respiratory Syncytial Virus. Available online: https://www.cdc.gov/ncird/surveillance/respiratory-illnesses/index.html (accessed on 14 June 2023).
- Harris, E. FDA Clears RSV Vaccine for Adults Aged 60 Years or Older. JAMA 2023, 329, 1817. [Google Scholar] [CrossRef] [PubMed]
- Dulfer, E.A.; Geckin, B.; Taks, E.J.M.; GeurtsvanKessel, C.H.; Dijkstra, H.; van Emst, L.; van der Gaast-de Jongh, C.E.; van Mourik, D.; Koopmans, P.C.; Domínguez-Andrés, J.; et al. Timing and Sequence of Vaccination against COVID-19 and Influenza (TACTIC): A Single-Blind, Placebo-Controlled Randomized Clinical Trial. Lancet Reg. Health Eur. 2023, 29, 100628. [Google Scholar] [CrossRef] [PubMed]
- ECDC-EMA Statement on Updating COVID-19 Vaccines Composition for New SARS-CoV-2 Virus Variants. Available online: https://www.ecdc.europa.eu/en/news-events/ecdc-ema-statement-updating-COVID-19-vaccines-composition-new-sars-cov-2-virus-variants (accessed on 14 June 2023).
- Imai, M.; Ito, M.; Kiso, M.; Yamayoshi, S.; Uraki, R.; Fukushi, S.; Watanabe, S.; Suzuki, T.; Maeda, K.; Sakai-Tagawa, Y.; et al. Efficacy of Antiviral Agents against Omicron Subvariants BQ.1.1 and XBB. N. Engl. J. Med. 2023, 388, 89–91. [Google Scholar] [CrossRef]
- Wan, E.Y.F.; Yan, V.K.C.; Mok, A.H.Y.; Wang, B.; Xu, W.; Cheng, F.W.T.; Lai, F.T.T.; Chui, C.S.L.; Li, X.; Wong, C.K.H.; et al. Effectiveness of Molnupiravir and Nirmatrelvir-Ritonavir in Hospitalized Patients with COVID-19: A Target Trial Emulation Study. Ann. Intern. Med. 2023, 176, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Weng, C.; Xie, R.; Han, G.; Yuan, Y.; Li, S.; Wang, C.; Wang, X.; Jiang, W.; Jiang, L. Safety and Efficacy of Paxlovid against Omicron Variants of Coronavirus Disease 2019 in Elderly Patients. Infect. Dis. Ther. 2023, 12, 649–662. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, K.L.; Wang, J.; Tadrous, M.; Langford, B.J.; Daneman, N.; Leung, V.; Gomes, T.; Friedman, L.; Daley, P.; Brown, K.A. Population-Based Evaluation of the Effectiveness of Nirmatrelvir-Ritonavir for Reducing Hospital Admissions and Mortality from COVID-19. CMAJ 2023, 195, E220–E226. [Google Scholar] [CrossRef]
- Xie, Y.; Choi, T.; Al-Aly, Z. Association of Treatment with Nirmatrelvir and the Risk of Post-COVID-19 Condition. JAMA Intern. Med. 2023, 183, 554–564. [Google Scholar] [CrossRef]
- Imran, M.; Kumar Arora, M.; Asdaq, S.M.B.; Khan, S.A.; Alaqel, S.I.; Alshammari, M.K.; Alshehri, M.M.; Alshrari, A.S.; Mateq Ali, A.; Al-Shammeri, A.M.; et al. Discovery, Development, and Patent Trends on Molnupiravir: A Prospective Oral Treatment for COVID-19. Molecules 2021, 26, 5795. [Google Scholar] [CrossRef]
- Agostini, M.L.; Pruijssers, A.J.; Chappell, J.D.; Gribble, J.; Lu, X.; Andres, E.L.; Bluemling, G.R.; Lockwood, M.A.; Sheahan, T.P.; Sims, A.C.; et al. Small-Molecule Antiviral β-d-N 4-Hydroxycytidine Inhibits a Proofreading-Intact Coronavirus with a High Genetic Barrier to Resistance. J. Virol. 2019, 93, e01348-19. [Google Scholar] [CrossRef]
- Barnard, D.L.; Hubbard, V.D.; Burton, J.; Smee, D.F.; Morrey, J.D.; Otto, M.J.; Sidwell, R.W. Inhibition of Severe Acute Respiratory Syndrome-Associated Coronavirus (SARSCoV) by Calpain Inhibitors and Beta-D-N4-Hydroxycytidine. Antivir. Chem. Chemother. 2004, 15, 15–22. [Google Scholar] [CrossRef]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of COVID-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Arribas, J.R.; Bhagani, S.; Lobo, S.M.; Khaertynova, I.; Mateu, L.; Fishchuk, R.; Park, W.Y.; Hussein, K.; Kim, S.W.; Ghosn, J.; et al. Randomized Trial of Molnupiravir or Placebo in Patients Hospitalized with COVID-19. NEJM Evid. 2022, 1, EVIDoa2100044. [Google Scholar] [CrossRef]
- Wong, C.K.H.; Au, I.C.H.; Lau, K.T.K.; Lau, E.H.Y.; Cowling, B.J.; Leung, G.M. Real-World Effectiveness of Early Molnupiravir or Nirmatrelvir-Ritonavir in Hospitalised Patients with COVID-19 without Supplemental Oxygen Requirement on Admission during Hong Kong’s Omicron BA.2 Wave: A Retrospective Cohort Study. Lancet Infect. Dis. 2022, 22, 1681–1693. [Google Scholar] [CrossRef] [PubMed]
- Flisiak, R.; Zarębska-Michaluk, D.; Rogalska, M.; Kryńska, J.A.; Kowalska, J.; Dutkiewicz, E.; Dobrowolska, K.; Jaroszewicz, J.; Moniuszko-Malinowska, A.; Rorat, M.; et al. Real-World Experience with Molnupiravir during the Period of SARS-CoV-2 Omicron Variant Dominance. Pharmacol. Rep. 2022, 74, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Choi, T.; Al-Aly, Z. Molnupiravir and Risk of Post-Acute Sequelae of COVID-19: Cohort Study. BMJ 2023, 381, e074572. [Google Scholar] [CrossRef]
- EMA Veklury. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/veklury (accessed on 22 January 2023).
- Dobrowolska, K.; Zarębska-Michaluk, D.; Brzdęk, M.; Rzymski, P.; Rogalska, M.; Moniuszko-Malinowska, A.; Kozielewicz, D.; Hawro, M.; Rorat, M.; Sikorska, K.; et al. Retrospective Analysis of the Effectiveness of Remdesivir in COVID-19 Treatment during Periods Dominated by Delta and Omicron SARS-CoV-2 Variants in Clinical Settings. J. Clin. Med. 2023, 12, 2371. [Google Scholar] [CrossRef]
- Sandin, R.; Harrison, C.; Draica, F.; Wiemken, T.L.; Ma, C.; Fusco, M.D.; Markson, L.; Dzingina, M. Estimated Impact of Oral Nirmatrelvir;Ritonavir on Reductions in Hospitalizations and Associated Costs within High-Risk COVID-19 Patients in the US. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Savinkina, A.; Paltiel, A.D.; Ross, J.S.; Gonsalves, G. Population-Level Strategies for Nirmatrelvir/Ritonavir Prescribing-A Cost-Effectiveness Analysis. Open Forum Infect. Dis. 2022, 9, ofac637. [Google Scholar] [CrossRef]
- Wai, A.K.-C.; Chan, C.Y.; Cheung, A.W.-L.; Wang, K.; Chan, S.C.-L.; Lee, T.T.-L.; Luk, L.Y.-F.; Yip, E.T.-F.; Ho, J.W.-K.; Tsui, O.W.-K.; et al. Association of Molnupiravir and Nirmatrelvir-Ritonavir with Preventable Mortality, Hospital Admissions and Related Avoidable Healthcare System Cost among High-Risk Patients with Mild to Moderate COVID-19. Lancet Reg. Health West. Pac. 2023, 30, 100602. [Google Scholar] [CrossRef]
- Marangoni, D.; Antonello, R.M.; Coppi, M.; Palazzo, M.; Nassi, L.; Streva, N.; Povolo, L.; Malentacchi, F.; Zammarchi, L.; Rossolini, G.M.; et al. Combination Regimen of Nirmatrelvir/Ritonavir and Molnupiravir for the Treatment of Persistent SARS-CoV-2 Infection: A Case Report and a Scoping Review of the Literature. Int. J. Infect. Dis. 2023, 133, 53–56. [Google Scholar] [CrossRef]
- Jeong, J.H.; Chokkakula, S.; Min, S.C.; Kim, B.K.; Choi, W.-S.; Oh, S.; Yun, Y.S.; Kang, D.H.; Lee, O.-J.; Kim, E.-G.; et al. Combination Therapy with Nirmatrelvir and Molnupiravir Improves the Survival of SARS-CoV-2 Infected Mice. Antivir. Res. 2022, 208, 105430. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.A.; Cowen, L.E. Using Combination Therapy to Thwart Drug Resistance. Future Microbiol. 2015, 10, 1719–1726. [Google Scholar] [CrossRef] [PubMed]
- Moreno, S.; Perno, C.F.; Mallon, P.W.; Behrens, G.; Corbeau, P.; Routy, J.-P.; Darcis, G. Two-Drug vs. Three-Drug Combinations for HIV-1: Do We Have Enough Data to Make the Switch? HIV Med. 2019, 20 (Suppl. 4), 2–12. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.; Lin, Y.; Wang, X.; Gao, Y.; Ye, S. Paxlovid in Patients Who Are Immunocompromised and Hospitalised with SARS-CoV-2 Infection. Lancet Infect. Dis. 2022, 22, 1279. [Google Scholar] [CrossRef] [PubMed]
- Helleberg, M.; Niemann, C.U.; Moestrup, K.S.; Kirk, O.; Lebech, A.-M.; Lane, C.; Lundgren, J. Persistent COVID-19 in an Immunocompromised Patient Temporarily Responsive to Two Courses of Remdesivir Therapy. J. Infect. Dis. 2020, 222, 1103–1107. [Google Scholar] [CrossRef]
- Camprubí, D.; Gaya, A.; Marcos, M.A.; Martí-Soler, H.; Soriano, A.; Mosquera, M.D.M.; Oliver, A.; Santos, M.; Muñoz, J.; García-Vidal, C. Persistent Replication of SARS-CoV-2 in a Severely Immunocompromised Patient Treated with Several Courses of Remdesivir. Int. J. Infect. Dis. 2021, 104, 379–381. [Google Scholar] [CrossRef]
- European Medicines Agency Use of Molnupiravir for the Treatment of COVID-19. Available online: https://www.ema.europa.eu/en/documents/referral/lagevrio-also-known-molnupiravir-mk-4482-COVID-19-article-53-procedure-assessment-report_en.pdf (accessed on 14 June 2023).
- European Medicines Agency Paxlovid. Assessment Report. Available online: https://www.ema.europa.eu/en/documents/assessment-report/paxlovid-epar-public-assessment-report_en.pdf (accessed on 14 June 2023).
- Stegemann, S.; Gosch, M.; Breitkreutz, J. Swallowing Dysfunction and Dysphagia Is an Unrecognized Challenge for Oral Drug Therapy. Int. J. Pharm. 2012, 430, 197–206. [Google Scholar] [CrossRef]
- Hummler, H.; Stillhart, C.; Meilicke, L.; Grimm, M.; Krause, E.; Mannaa, M.; Gollasch, M.; Weitschies, W.; Page, S. Impact of Tablet Size and Shape on the Swallowability in Older Adults. Pharmaceutics 2023, 15, 1042. [Google Scholar] [CrossRef]
- Lawal, Y. Africa’s Low COVID-19 Mortality Rate: A Paradox? Int. J. Infect. Dis. 2021, 102, 118–122. [Google Scholar] [CrossRef]
- Osei, S.A.; Biney, R.P.; Anning, A.S.; Nortey, L.N.; Ghartey-Kwansah, G. Low Incidence of COVID-19 Case Severity and Mortality in Africa; Could Malaria Co-Infection Provide the Missing Link? BMC Infect. Dis. 2022, 22, 78. [Google Scholar] [CrossRef]
- Ashworth, J.; Mathie, D.; Scott, F.; Mahendran, Y.; Woolhouse, M.; Stoevesandt, O.; Mduluza, T.; Mutapi, F. Peptide Microarray IgM and IgG Screening of Pre-SARS-CoV-2 Human Serum Samples from Zimbabwe for Reactivity with Peptides from All Seven Human Coronaviruses: A Cross-Sectional Study. Lancet Microbe 2023, 4, e215–e227. [Google Scholar] [CrossRef]
- Diop, B.Z.; Ngom, M.; Pougué Biyong, C.; Pougué Biyong, J.N. The Relatively Young and Rural Population May Limit the Spread and Severity of COVID-19 in Africa: A Modelling Study. BMJ Glob. Health 2020, 5, e002699. [Google Scholar] [CrossRef] [PubMed]
- Gill, C.J.; Mwananyanda, L.; MacLeod, W.B.; Kwenda, G.; Pieciak, R.C.; Etter, L.; Bridges, D.; Chikoti, C.; Chirwa, S.; Chimoga, C.; et al. What Is the Prevalence of COVID-19 Detection by PCR among Deceased Individuals in Lusaka, Zambia? A Postmortem Surveillance Study. BMJ Open 2022, 12, e066763. [Google Scholar] [CrossRef]
- Levin, A.T.; Owusu-Boaitey, N.; Pugh, S.; Fosdick, B.K.; Zwi, A.B.; Malani, A.; Soman, S.; Besançon, L.; Kashnitsky, I.; Ganesh, S.; et al. Assessing the Burden of COVID-19 in Developing Countries: Systematic Review, Meta-Analysis and Public Policy Implications. BMJ Glob. Health 2022, 7, e008477. [Google Scholar] [CrossRef] [PubMed]
- Kunyenje, C.A.; Chirwa, G.C.; Mboma, S.M.; Ng’ambi, W.; Mnjowe, E.; Nkhoma, D.; Ngwira, L.G.; Chawani, M.S.; Chilima, B.; Mitambo, C.; et al. COVID-19 Vaccine Inequity in African Low-Income Countries. Front. Public Health 2023, 11, 1087662. [Google Scholar] [CrossRef] [PubMed]
- Member State Briefing Update on Global COVID-19 Vaccination. Available online: https://apps.who.int/gb/COVID-19/pdf_files/2023/05_01/Item1.pdf (accessed on 18 June 2023).
- U.S. International COVID-19 Vaccine Donations Tracker. Available online: https://www.kff.org/global-health-policy/issue-brief/u-s-international-COVID-19-vaccine-donations-tracker/ (accessed on 11 June 2023).
- Hassan, F.; Yamey, G.; Abbasi, K. Profiteering from Vaccine Inequity: A Crime against Humanity? BMJ 2021, 374, n2027. [Google Scholar] [CrossRef]
- Rzymski, P.; Szuster-Ciesielska, A. The COVID-19 Vaccination Still Matters: Omicron Variant Is a Final Wake-up Call for the Rich to Help the Poor. Vaccines 2022, 10, 1070. [Google Scholar] [CrossRef]
- WHO COVAX Allocation. Available online: https://www.who.int/initiatives/act-accelerator/covax/allocation (accessed on 15 May 2022).
- Savinkina, A.; Bilinski, A.; Fitzpatrick, M.; Paltiel, A.D.; Rizvi, Z.; Salomon, J.; Thornhill, T.; Gonsalves, G. Estimating Deaths Averted and Cost per Life Saved by Scaling up MRNA COVID-19 Vaccination in Low-Income and Lower-Middle-Income Countries in the COVID-19 Omicron Variant Era: A Modelling Study. BMJ Open 2022, 12, e061752. [Google Scholar] [CrossRef]
- Hoffman, S.A.; Costales, C.; Sahoo, M.K.; Palanisamy, S.; Yamamoto, F.; Huang, C.; Verghese, M.; Solis, D.A.; Sibai, M.; Subramanian, A.; et al. SARS-CoV-2 Neutralization Resistance Mutations in Patient with HIV/AIDS, California, USA. Emerg. Infect. Dis. 2021, 27, 2720–2723. [Google Scholar] [CrossRef]
- Cele, S.; Karim, F.; Lustig, G.; San, J.E.; Hermanus, T.; Tegally, H.; Snyman, J.; Moyo-Gwete, T.; Wilkinson, E.; Bernstein, M.; et al. SARS-CoV-2 Prolonged Infection during Advanced HIV Disease Evolves Extensive Immune Escape. Cell Host Microbe 2022, 30, 154–162.e5. [Google Scholar] [CrossRef]
- Gonzalez-Reiche, A.S. SARS-CoV-2 in Low-Income Countries: The Need for Sustained Genomic Surveillance. Lancet Glob. Health 2023, 11, e815–e816. [Google Scholar] [CrossRef] [PubMed]
- Le, T.; Sun, C.; Chang, J.; Zhang, G.; Yin, X. MRNA Vaccine Development for Emerging Animal and Zoonotic Diseases. Viruses 2022, 14, 401. [Google Scholar] [CrossRef]
- Chauhan, R.P.; Dessie, Z.G.; Noreddin, A.; El Zowalaty, M.E. Systematic Review of Important Viral Diseases in Africa in Light of the “One Health” Concept. Pathogens 2020, 9, 301. [Google Scholar] [CrossRef] [PubMed]
- Gwenzi, W.; Skirmuntt, E.C.; Musvuugwa, T.; Teta, C.; Halabowski, D.; Rzymski, P. Grappling with (Re)-Emerging Infectious Zoonoses: Risk Assessment, Mitigation Framework, and Future Directions. Int. J. Disaster Risk Reduct. 2022, 82, 103350. [Google Scholar] [CrossRef]
- Iacobucci, G. COVID-19: “Grotesque Inequity” That Only a Quarter of Paxlovid Courses Go to Poorer Countries. BMJ 2022, 379, o2795. [Google Scholar] [CrossRef] [PubMed]
- Beasley, D. Price of COVID Treatments from Pfizer, Merck, GSK Align with Patient Benefits-Report. Reuters 2022. Available online: https://www.reuters.com/business/healthcare-pharmaceuticals/price-covid-treatments-pfizer-merck-gsk-align-with-patient-benefits-report-2022-02-03/ (accessed on 10 August 2023).
- Baker, R.E.; Mahmud, A.S.; Miller, I.F.; Rajeev, M.; Rasambainarivo, F.; Rice, B.L.; Takahashi, S.; Tatem, A.J.; Wagner, C.E.; Wang, L.-F.; et al. Infectious Disease in an Era of Global Change. Nat. Rev. Microbiol. 2022, 20, 193–205. [Google Scholar] [CrossRef]
- Watts, M.S. Physicians as Role Models in Society. West. J. Med. 1990, 152, 292. [Google Scholar]
- Betancourt, J.A.; Rosenberg, M.A.; Zevallos, A.; Brown, J.R.; Mileski, M. The Impact of COVID-19 on Telemedicine Utilization Across Multiple Service Lines in the United States. Healthcare 2020, 8, 380. [Google Scholar] [CrossRef]
- Bazan, D.; Nowicki, M.; Rzymski, P. Medical Students as the Volunteer Workforce during the COVID-19 Pandemic: Polish Experience. Int. J. Disaster Risk Reduct. 2021, 55, 102109. [Google Scholar] [CrossRef]
- Benfante, A.; Di Tella, M.; Romeo, A.; Castelli, L. Traumatic Stress in Healthcare Workers during COVID-19 Pandemic: A Review of the Immediate Impact. Front. Psychol. 2020, 11, 569935. [Google Scholar] [CrossRef]
- Wittenberg, E.; Goldsmith, J.V.; Chen, C.; Prince-Paul, M.; Johnson, R.R. Opportunities to Improve COVID-19 Provider Communication Resources: A Systematic Review. Patient Educ. Couns. 2021, 104, 438–451. [Google Scholar] [CrossRef]
- Mach, K.J.; Salas Reyes, R.; Pentz, B.; Taylor, J.; Costa, C.A.; Cruz, S.G.; Thomas, K.E.; Arnott, J.C.; Donald, R.; Jagannathan, K.; et al. News Media Coverage of COVID-19 Public Health and Policy Information. Humanit. Soc. Sci. Commun. 2021, 8, 220. [Google Scholar] [CrossRef]
- Fotiadis, K.; Dadouli, K.; Avakian, I.; Bogogiannidou, Z.; Mouchtouri, V.A.; Gogosis, K.; Speletas, M.; Koureas, M.; Lagoudaki, E.; Kokkini, S.; et al. Factors Associated with Healthcare Workers’ (HCWs) Acceptance of COVID-19 Vaccinations and Indications of a Role Model towards Population Vaccinations from a Cross-Sectional Survey in Greece, May 2021. Int. J. Environ. Res. Public Health 2021, 18, 10558. [Google Scholar] [CrossRef]
- World Health Organization. Evaluation Report for the Training Module “Communicating with Patients about COVID-19 Vaccination”: Greece; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- Burson, R.C.; Buttenheim, A.M.; Armstrong, A.; Feemster, K.A. Community Pharmacies as Sites of Adult Vaccination: A Systematic Review. Hum. Vaccines Immunother. 2016, 12, 3146–3159. [Google Scholar] [CrossRef]
- Sobierajski, T.; Rzymski, P.; Wanke-Rytt, M. The Influence of Recommendation of Medical and Non-Medical Authorities on the Decision to Vaccinate against Influenza from a Social Vaccinology Perspective: Cross-Sectional, Representative Study of Polish Society. Vaccines 2023, 11, 994. [Google Scholar] [CrossRef]
- Paudyal, V.; Fialová, D.; Henman, M.C.; Hazen, A.; Okuyan, B.; Lutters, M.; Cadogan, C.; da Costa, F.A.; Galfrascoli, E.; Pudritz, Y.M.; et al. Pharmacists’ Involvement in COVID-19 Vaccination across Europe: A Situational Analysis of Current Practice and Policy. Int. J. Clin. Pharm. 2021, 43, 1139–1148. [Google Scholar] [CrossRef]
- Queeno, B.V. Evaluation of Inpatient Influenza and Pneumococcal Vaccination Acceptance Rates with Pharmacist Education. J. Pharm. Pract. 2017, 30, 202–208. [Google Scholar] [CrossRef]
- Pullagura, G.R.; Waite, N.M.; Houle, S.K.D.; Violette, R.; Wong, W.W.L. Cost-Utility Analysis of Offering a Novel Remunerated Community Pharmacist Consultation Service on Influenza Vaccination for Seniors in Ontario, Canada. J. Am. Pharm. Assoc. 2019, 59, 489–497.e1. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rzymski, P.; Pokorska-Śpiewak, M.; Jackowska, T.; Kuchar, E.; Nitsch-Osuch, A.; Pawłowska, M.; Babicki, M.; Jaroszewicz, J.; Szenborn, L.; Wysocki, J.; et al. Key Considerations during the Transition from the Acute Phase of the COVID-19 Pandemic: A Narrative Review. Vaccines 2023, 11, 1502. https://doi.org/10.3390/vaccines11091502
Rzymski P, Pokorska-Śpiewak M, Jackowska T, Kuchar E, Nitsch-Osuch A, Pawłowska M, Babicki M, Jaroszewicz J, Szenborn L, Wysocki J, et al. Key Considerations during the Transition from the Acute Phase of the COVID-19 Pandemic: A Narrative Review. Vaccines. 2023; 11(9):1502. https://doi.org/10.3390/vaccines11091502
Chicago/Turabian StyleRzymski, Piotr, Maria Pokorska-Śpiewak, Teresa Jackowska, Ernest Kuchar, Aneta Nitsch-Osuch, Małgorzata Pawłowska, Mateusz Babicki, Jerzy Jaroszewicz, Leszek Szenborn, Jacek Wysocki, and et al. 2023. "Key Considerations during the Transition from the Acute Phase of the COVID-19 Pandemic: A Narrative Review" Vaccines 11, no. 9: 1502. https://doi.org/10.3390/vaccines11091502