
Understanding COVID-19 Vaccine Acceptance among Latin American Health Workers: Implications for Designing Interventions
 , , and
, , and 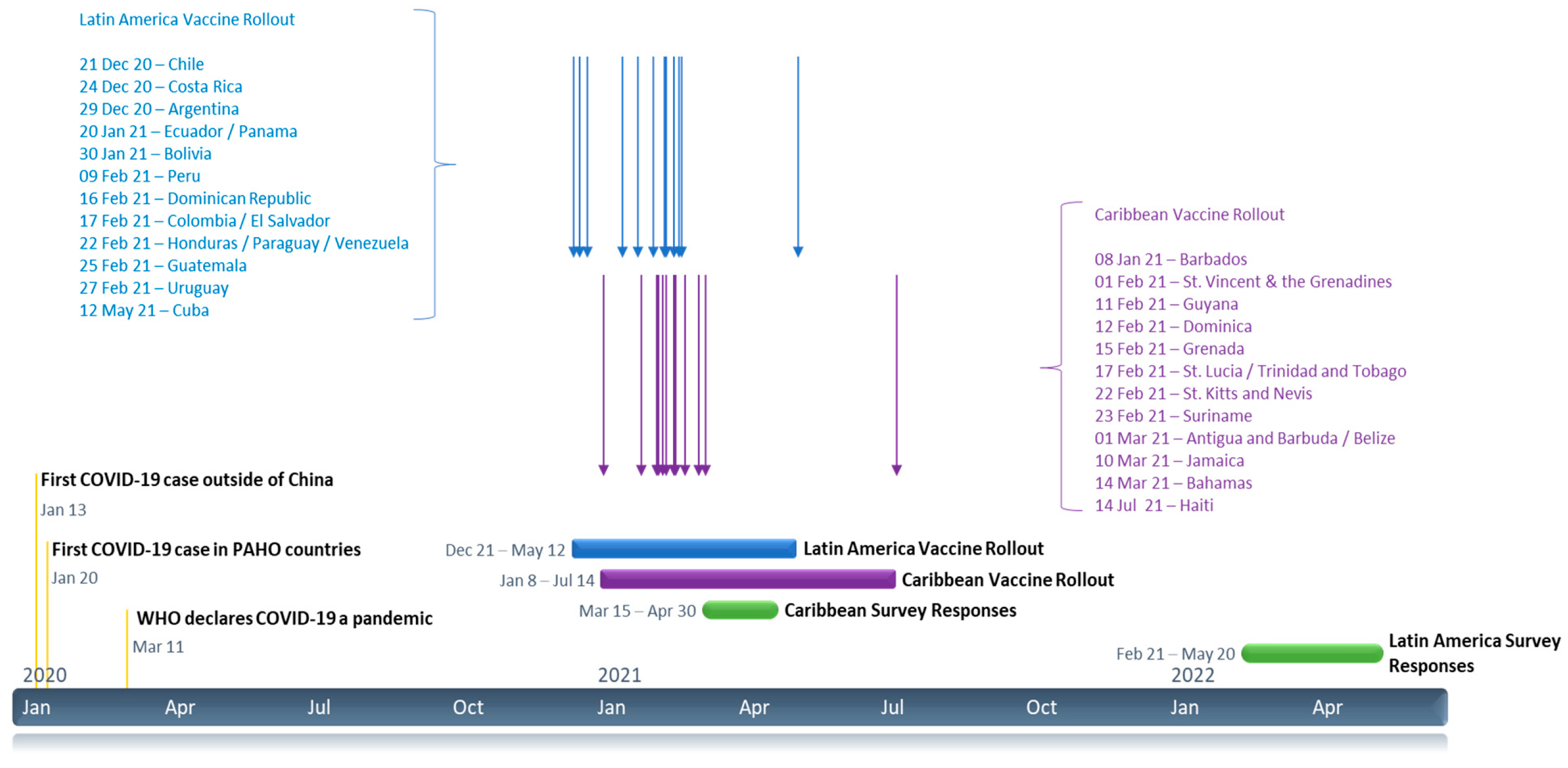{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
Context and Study Overview
- To estimate the percentage of Latin American HWs who were accepting of the COVID-19 vaccine at the time of the survey.
- To explore whether there were differences in the magnitude of COVID-19 vaccine acceptance among demographic and geographic subgroups of the study population.
- To explore demographic predictors of COVID-19 vaccine acceptance in Latin American HWs.
2. Materials and Methods
2.1. Survey Instrument
2.2. Sample Size
2.3. Survey Implementation
2.4. Analysis
2.5. Summary of Free-Response Questions
3. Results
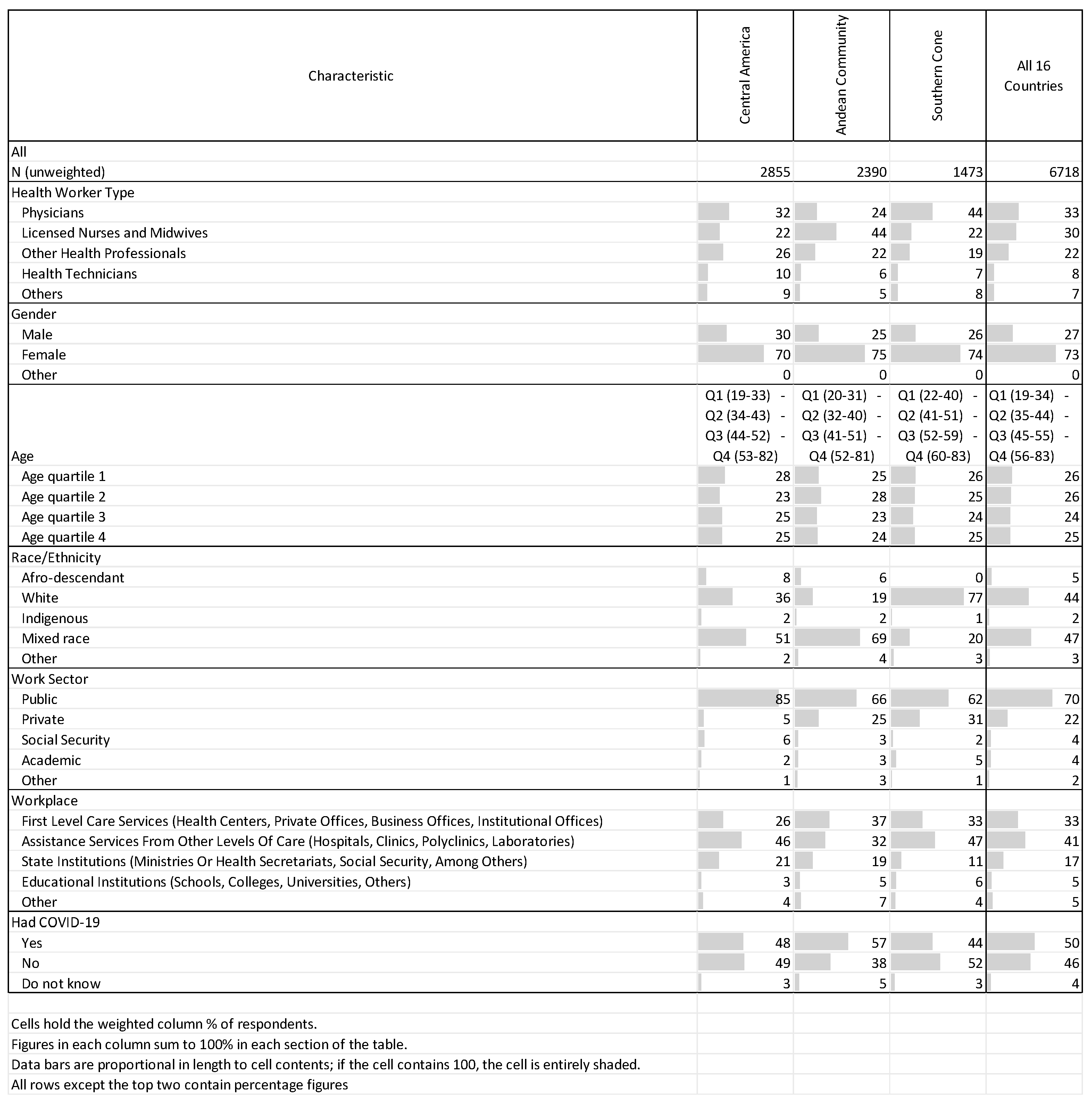
3.1. Respondent Characteristics
3.2. Vaccine Acceptance
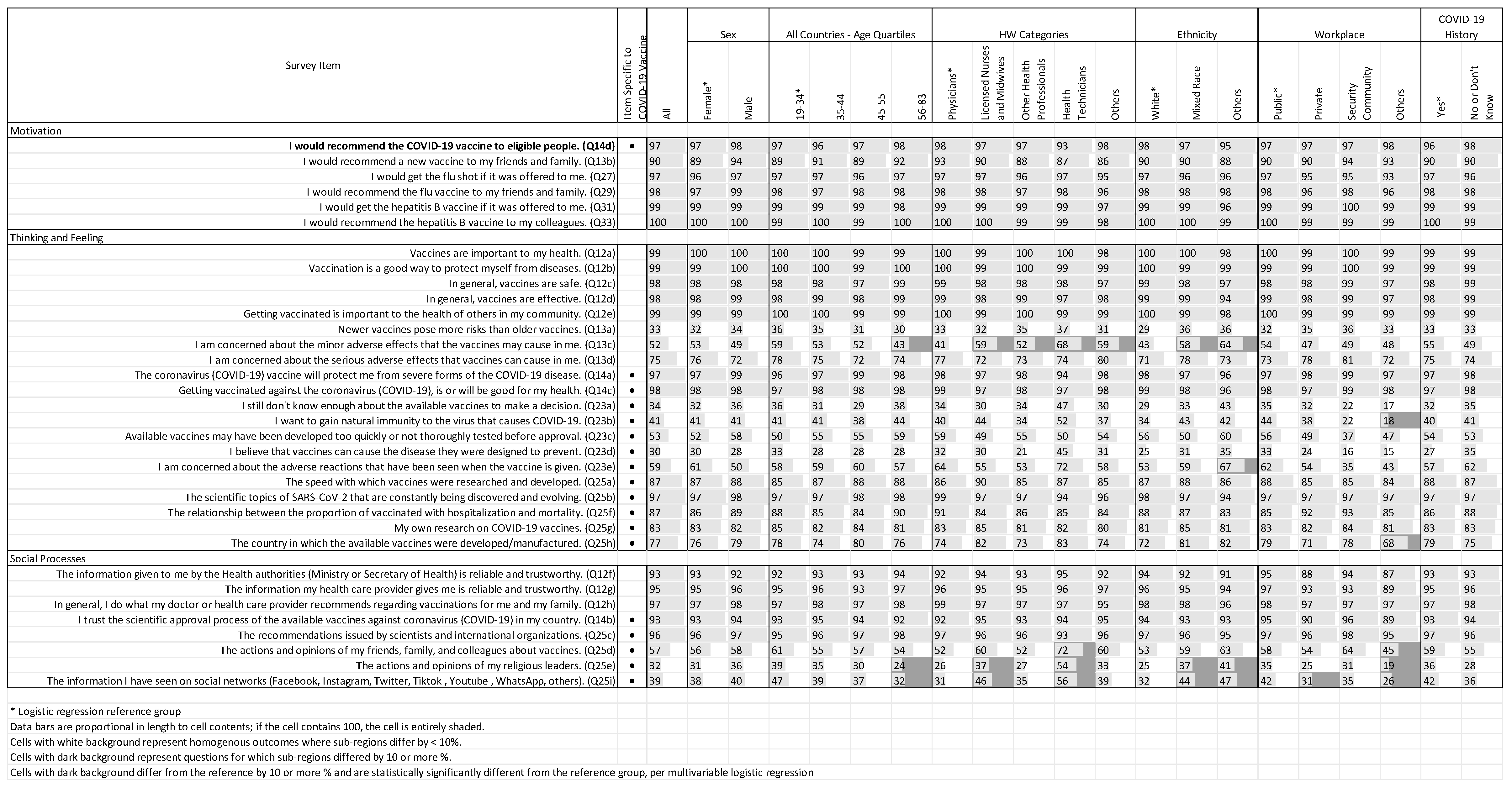
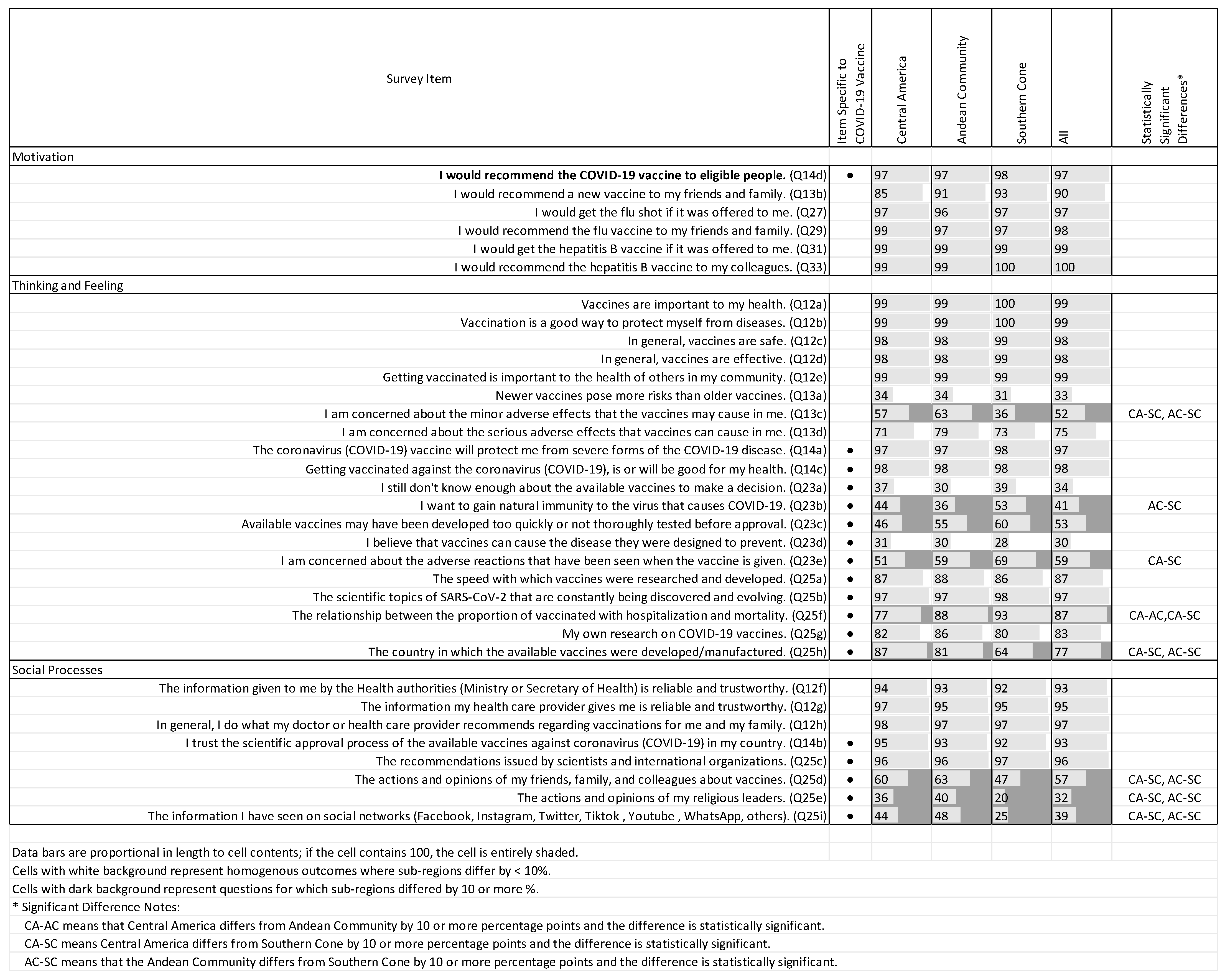
3.3. Attitudes and Opinions Regarding Vaccines
3.3.1. Thinking and Feeling
3.3.2. Social Processes
3.3.3. General Opinions of Vaccines
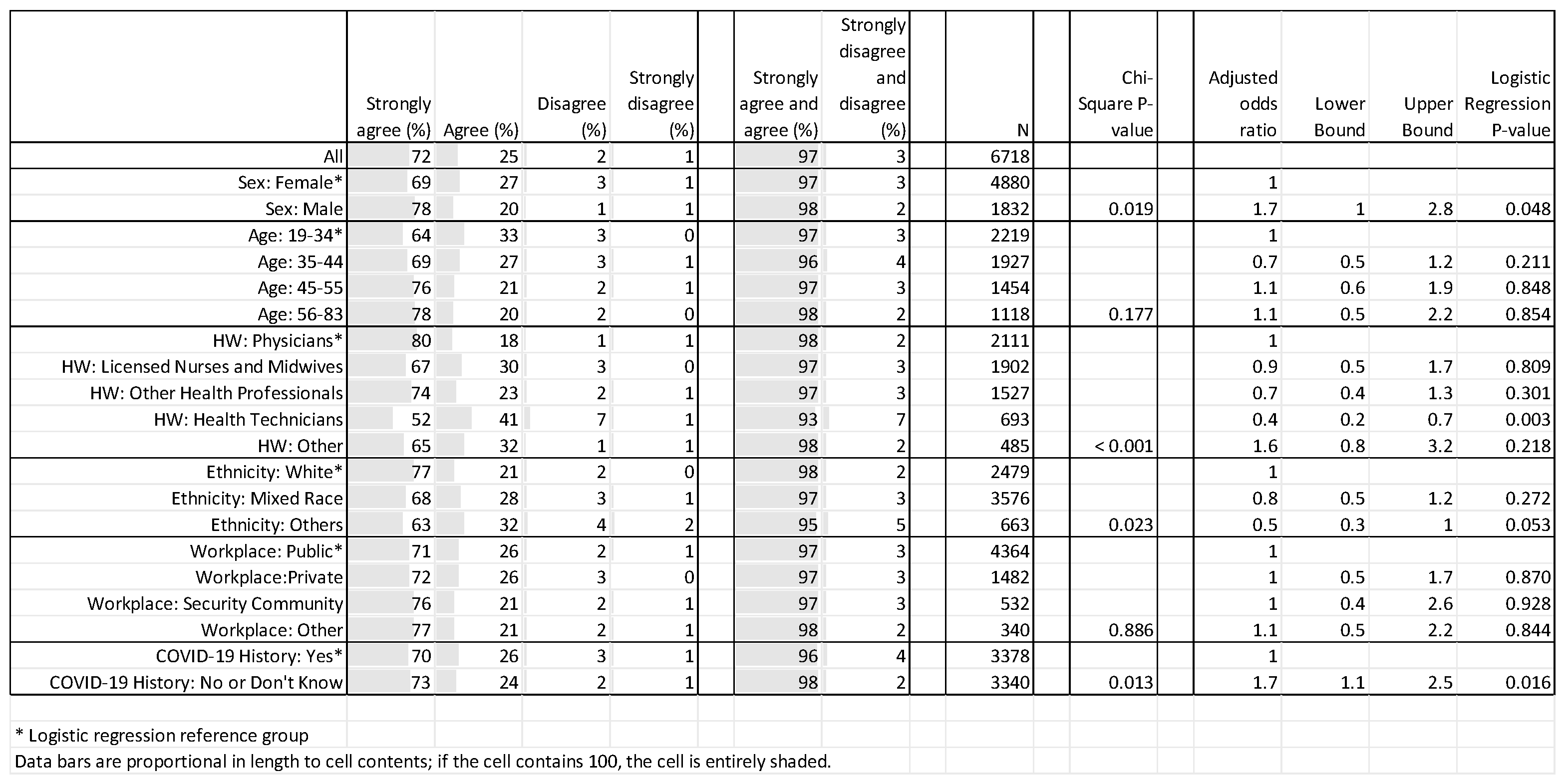
3.3.4. Vaccine Acceptance: Bivariate and Multivariate Analyses
4. Discussion
4.1. Key Findings
4.1.1. Vaccine Acceptance
4.1.2. Vaccine Safety and Effectiveness, and Concerns about Side Effects
4.1.3. Influence of Social Processes
4.2. Recommendations
4.2.1. Integration with Essential Public Health Functions
4.2.2. Emphasize Safety in Information Campaigns
4.2.3. Ensure Messages Are Delivered through Trusted and Preferred Information Channels
4.2.4. Educate HWs to Be Critical Consumers of News and Other Information
4.3. Strengths and Limitations
- The study was publicized widely in medical networks.
- The survey was available online for three months.
- Workers at 50 health facilities in Cuba were afforded the opportunity to complete a paper version of the questionnaire.
- Pre-testing helped clarify questions for respondents.
- Seventy-three percent of respondents were female, which is reflective of the composition of the health workforce in Latin America [31].
- The survey findings correspond to a single point in time, and the results cannot be projected into the future.
- Participants were a convenience sample of Latin American HWs. The respondents were limited to those who heard of the study, had the capability to participate online, and decided to do so. The sample is not likely to be representative of all HWs in any Latin American country or subregion, nor does it have respondents from Mexico or Brazil. For this reason, the results should not be generalized to all HWs in Latin America.
- The open invitation to participate was circulated through numerous professional networks, but it is not possible to know what portion of HWs heard about the survey in time to participate, nor whether those who learned about the survey are similar in demographics and attitude to those who did not.
- The data collection mode was different in Cuba than the other countries (paper for the former; electronic data collection for the latter), and the survey was only available to persons who worked at one of the institutions that was furnished with paper forms—all of which were in Havana.
4.4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global impact of the first year of COVID-19 vaccination: A mathematical modelling study. Lancet Infect. Dis. 2022, 22, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard; World Health Organization: Geneva, Switzerland, 2022; Available online: https://covid19.who.int/ (accessed on 10 June 2022).
- Desye, B. Prevalence and determinants of COVID-19 vaccine acceptance among healthcare workers: A systematic review. Front. Public Health 2022, 10, 941206. [Google Scholar] [CrossRef] [PubMed]
- Wake, A.D. Healthcare workers and nonhealthcare workers pro-vaccination attitude and its associated factors towards COVID-19 vaccine globally: A systematic review and meta-analysis. Interdiscip. Perspect. Infect. Dis. 2022, 2022, 2443785. [Google Scholar] [CrossRef] [PubMed]
- Askarian, M.; Semenov, A.; Llopis, F.; Rubulotta, F.; Dragovac, G.; Pshenichnaya, N.; Assadian, O.; Ruch, Y.; Shayan, Z.; Padilla Fortunatti, C.; et al. The COVID-19 vaccination acceptance/hesitancy rate and its determinants among healthcare workers of 91 countries: A multicenter cross-sectional study. EXCLI J. 2022, 21, 93. [Google Scholar] [PubMed]
- Noushad, M.; Rastam, S.; Nassani, M.Z.; Al-Saqqaf, I.S.; Hussain, M.; Yaroko, A.A.; Arshad, M.; Kirfi, A.M.; Koppolu, P.; Niazi, F.H.; et al. A global survey of COVID-19 vaccine acceptance among healthcare workers. Front. Public Health 2022, 9, 794673. [Google Scholar] [CrossRef] [PubMed]
- Lubad, M.A.; Abu-Helalah, M.A.; Alahmad, I.F.; Al-Tamimi, M.M.; QawaQzeh, M.S.; Al-kharabsheh, A.M.; Alzoubi, H.; Alnawafleh, A.H.; Kheirallah, K.A. Willingness of healthcare workers to recommend or receive a third COVID-19 vaccine dose: A cross-sectional study from Jordan. Infect. Dis. Rep. 2023, 15, 210–221. [Google Scholar] [CrossRef] [PubMed]
- Peterson, C.J.; Lee, B.; Nugent, K. COVID-19 vaccination hesitancy among healthcare workers—A review. Vaccines 2022, 10, 948. [Google Scholar] [CrossRef] [PubMed]
- Biswas, N.; Mustapha, T.; Khubchandani, J.; Price, J.H. The nature and extent of COVID-19 vaccination hesitancy in healthcare workers. J. Community Health 2021, 46, 1244–1251. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization Epidemiological Update: Coronavirus Disease (COVID-19)—02 December 2021. Available online: https://www.paho.org/en/documents/epidemiological-update-coronavirus-disease-covid-19-2-december-2021 (accessed on 17 January 2023).
- Pan American Health Organization. Country Reports to Immunization; PAHO: Washington, DC, USA, 2023. [Google Scholar]
- Puertas, E.B.; Velandia-Gonzalez, M.; Vulanovic, L.; Bayley, L.; Broome, K.; Ortiz, C.; Rise, N.; Vera Antelo, M.; Rhoda, D.A. Concerns, attitudes, and intended practices of Caribbean healthcare workers concerning COVID-19 vaccination: A cross-sectional study. Lancet Reg. Health-Am. 2022, 9, 100193. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization. Concerns, Attitudes, and Intended Practices of Healthcare Workers toward COVID-19 Vaccination in the Caribbean; PAHO: Washington, DC, USA, 2021; Available online: https://iris.paho.org/handle/10665.2/54964 (accessed on 1 May 2023).
- World Health Organization. Understanding the behavioural and social drivers of vaccine uptake WHO position paper—May 2022. Wkly. Epidemiol. Rec. 2022, 97, 209–224. [Google Scholar]
- Kabamba Nzaji, M.; Kabamba Ngombe, L.; Ngoie Mwamba, G.; Banza Ndala, D.B.; Mbidi Miema, J.; Luhata Lungoyo, C.; Lora Mwimba, B.; Cikomola Mwana Bene, A.; Mukamba Musenga, E. Acceptability of vaccination against COVID-19 among healthcare workers in the Democratic Republic of the Congo. Pragmatic Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention CDC Museum COVID-19 Timeline. Available online: https://www.cdc.gov/museum/timeline/covid19.html (accessed on 24 April 2023).
- Pan American Health Organization. COVID-19 Situation Report; PAHO: Washington, DC, USA, 2020. Available online: https://iris.paho.org/handle/10665.2/52403 (accessed on 24 April 2023).
- Pan American Health Organization. COVID-19 Vaccination Dashboard Weekly Monitoring Database; Internal Use Document; PAHO: Washington, DC, USA, 2020. [Google Scholar]
- WHO; UNICEF. Data for Action: Achieving High Uptake of COVID-19 Vaccines: Gathering and Using Data on the Behavioural and Social Drivers of Vaccination: A Guidebook for Immunization Programmes and Implementing Partners: Interim Guidance; World Health Organization: Geneva, Switzerland, 2021; Available online: https://apps.who.int/iris/handle/10665/339452 (accessed on 18 January 2022).
- Gadoth, A.; Halbrook, M.; Martin-Blais, R.; Gray, A.; Tobin, N.H.; Ferbas, K.G.; Aldrovandi, G.M.; Rimoin, A.W. Cross-sectional assessment of COVID-19 vaccine acceptance among health care workers in Los Angeles. Ann. Intern Med. 2021, 174, 882–885. [Google Scholar] [CrossRef] [PubMed]
- Dubé, È.; Ward, J.K.; Verger, P.; MacDonald, N.E. Vaccine hesitancy, acceptance, and anti-vaccination: Trends and future prospects for public health. Annu. Rev. Public Health 2021, 42, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization. Knowledge, Attitudes, and Practices of Health Workers Regarding COVID-19 Vaccines in Latin America; Report No.: OPS/FPL/IM/COVID-19/22-0056; PAHO: Washington, DC, USA, 2023; Available online: https://iris.paho.org/handle/10665.2/57454 (accessed on 21 April 2023).
- Alarcón-Braga, E.; Hernandez-Bustamante, E.; Salazar-Valdivia, F. Acceptance towards COVID-19 vaccination in Latin America and the Caribbean: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2022, 49, 102369. [Google Scholar] [CrossRef] [PubMed]
- Di Gennaro, F.; Murri, R.; Segala, F.V.; Cerruti, L.; Abdulle, A.; Saracino, A.; Bavaro, D.F.; Fantoni, M. Attitudes towards Anti-SARS-CoV2 Vaccination among Healthcare Workers: Results from a National Survey in Italy. Viruses 2021, 13, 371. [Google Scholar] [CrossRef] [PubMed]
- Guzman-Holst, A.; DeAntonio, R.; Prado-Cohrs, D.; Juliao, P. Barriers to vaccination in Latin America: A systematic literature review. Vaccine 2020, 38, 470–481. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization. Guide for the Preparation of a Risk Communication Strategy for COVID-19 Vaccines: A Resource for the Countries of the Americas; Report No.: PAHO/IMS/FPL/COVID-19/21-0009; PAHO: Washington, DC, USA, 2021; Available online: https://www.paho.org/en/documents/guide-preparation-risk-communication-strategy-covid-19-vaccines-resource-countries (accessed on 21 April 2023).
- Priebe, J.; Silber, H.; Beuthner, C.; Pötzschke, S. How (not) to mobilize health workers in the fight against vaccine hesitancy: Experimental evidence from Germany’s AstraZeneca controversy. BMC Public Health 2022, 22, 516. [Google Scholar] [CrossRef] [PubMed]
- News Literacy Project Website. Available online: https://newslit.org/ (accessed on 21 April 2023).
- News Literacy Project; Planet Word Museum: Washington, DC, USA, 2023.
- Hernandez, R.G.; Hagen, L.; Walker, K.; O’Leary, H.; Lengacher, C. The COVID-19 vaccine social media infodemic: Healthcare providers’ missed dose in addressing misinformation and vaccine hesitancy. Hum. Vaccines Immunother. 2021, 17, 2962–2964. [Google Scholar] [CrossRef] [PubMed]
- CEPAL. The Economic Autonomy of Women in a Sustainable Recovery with Equality. 2021 Feb. Report No.: 9. Available online: https://www.cepal.org/en/publications/46634-economic-autonomy-women-sustainable-recovery-equality (accessed on 29 August 2023).





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivera, T.; Brustrom, J.; Vera Antelo, M.; Puertas, E.B.; Rhoda, D.A.; Velandia-Gonzalez, M. Understanding COVID-19 Vaccine Acceptance among Latin American Health Workers: Implications for Designing Interventions. Vaccines 2023, 11, 1471. https://doi.org/10.3390/vaccines11091471
Rivera T, Brustrom J, Vera Antelo M, Puertas EB, Rhoda DA, Velandia-Gonzalez M. Understanding COVID-19 Vaccine Acceptance among Latin American Health Workers: Implications for Designing Interventions. Vaccines. 2023; 11(9):1471. https://doi.org/10.3390/vaccines11091471
Chicago/Turabian StyleRivera, Tamara, Jennifer Brustrom, Maite Vera Antelo, E. Benjamin Puertas, Dale A. Rhoda, and Martha Velandia-Gonzalez. 2023. "Understanding COVID-19 Vaccine Acceptance among Latin American Health Workers: Implications for Designing Interventions" Vaccines 11, no. 9: 1471. https://doi.org/10.3390/vaccines11091471