
A Systematic Review of Behaviour Change Techniques within Interventions to Increase Vaccine Uptake among Ethnic Minority Populations

Abstract
:1. Introduction
Review Questions
2. Methodology
2.1. Search Strategy and Selection Criteria
2.2. Eligibility Criteria
- Population: studies that included patients and the general public from racial and ethnic minority groups and excluded studies with a majority white ethnic population (i.e., studies with ≥50% white ethnic sample size). Ethnic minority groups were defined as groups that are not part of the majority ethnicity in the country of the study;
- Interventions: reported interventions, which included specific strategies designed to improve vaccination services and uptake in racial and ethnic minority groups, focusing on respiratory and routinely recommended vaccine-preventable diseases. Studies were excluded that did not provide details of the interventions;
- Comparator: included any reported comparator such as pre-intervention data, alternative intervention, or control group;
- Outcomes: studies were included if they reported vaccine behaviour-related data (intention, behaviour and uptake) after implementation of the intervention;
- Study Design: all study designs, including quantitative and qualitative, were included, except case studies and case series.
3. Screening
3.1. Data Extraction
3.1.1. Intervention Study Details
3.1.2. BCT and BCW Intervention Details
3.2. Risk of Bias
3.3. Synthesis Method
4. Results
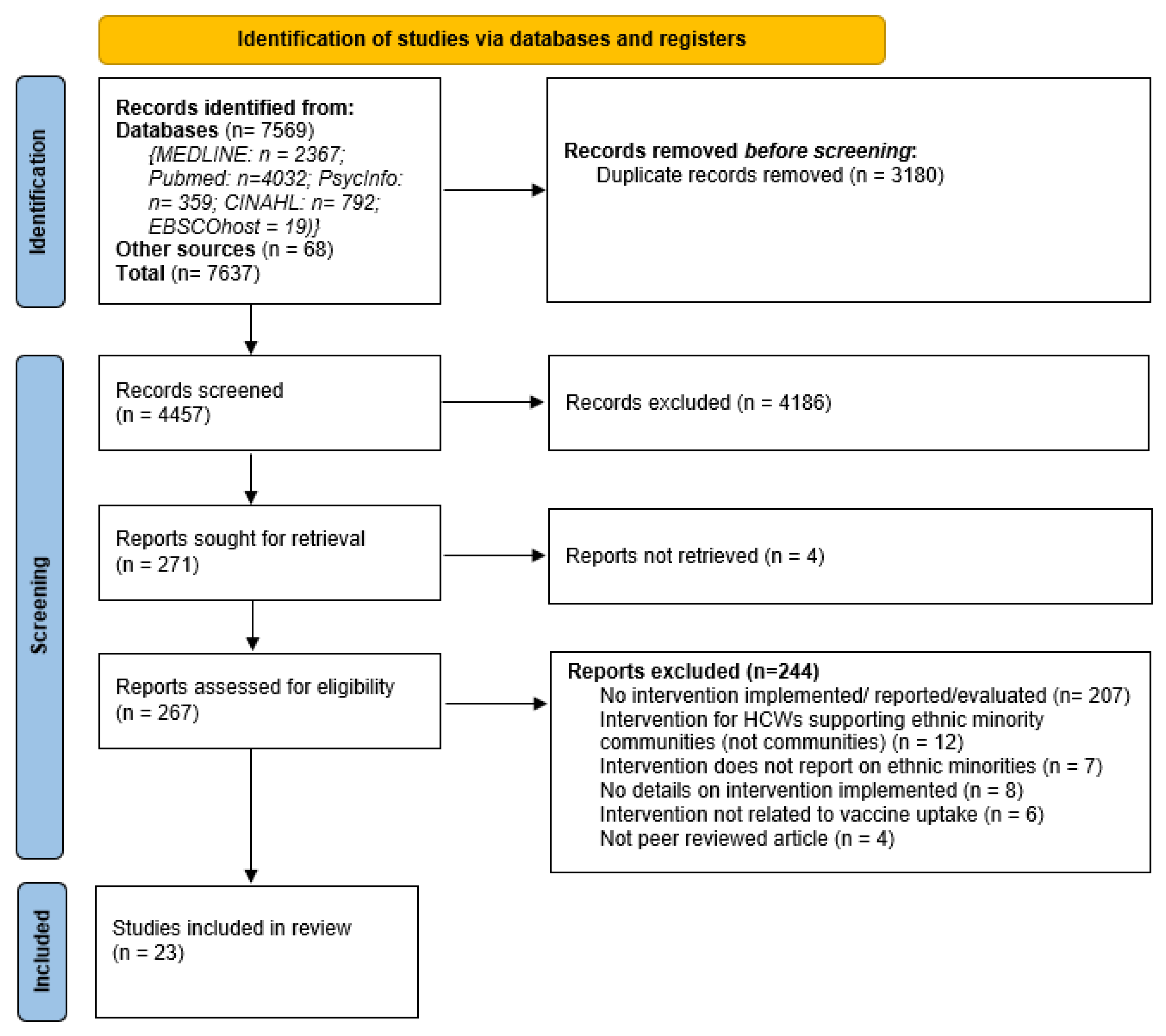
4.1. Search Results
4.2. Study Characteristics
4.3. Risk of Bias
4.4. Intervention Effects and Outcomes
4.5. Intervention Behaviour Change Components
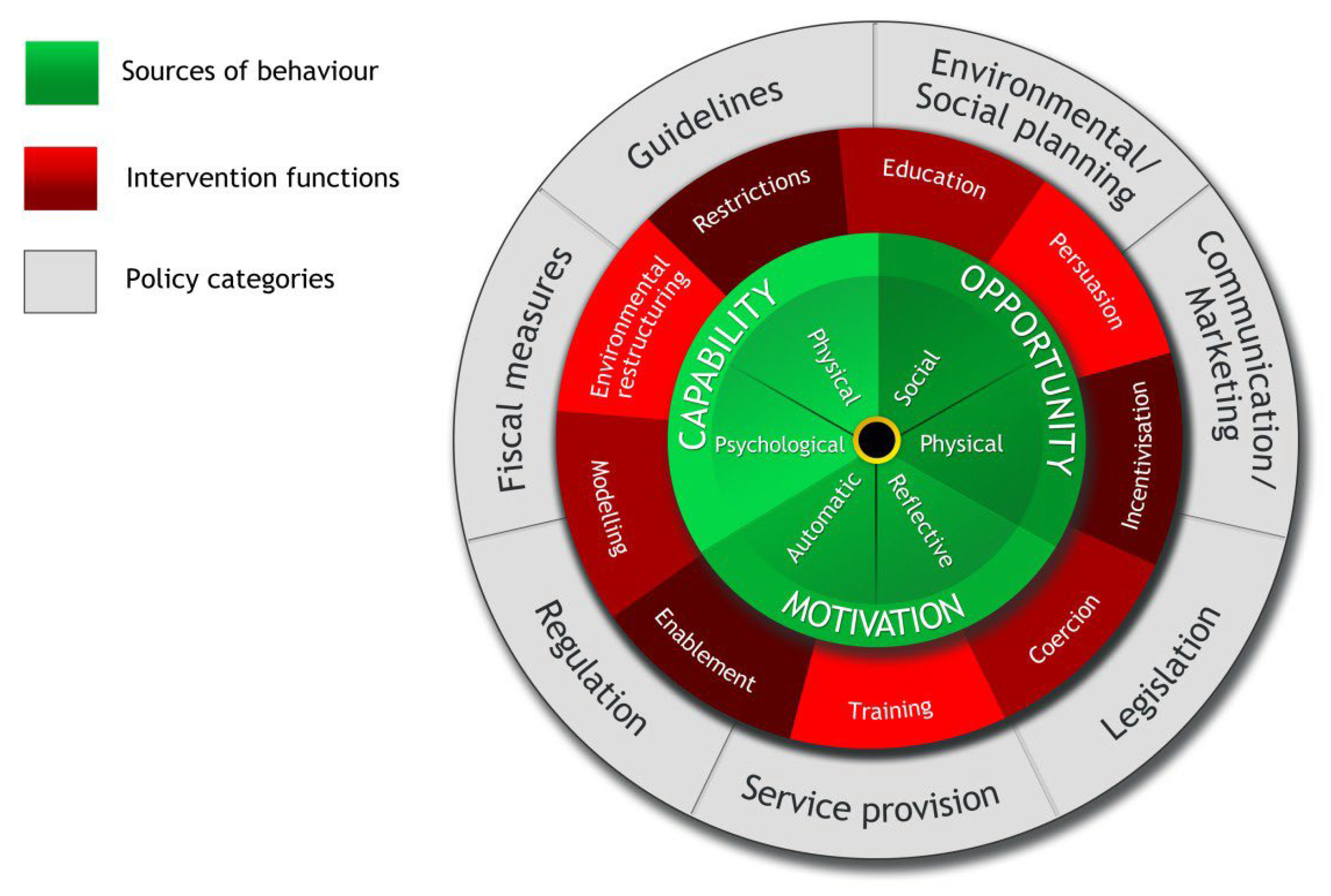
4.6. Intervention Functions and Policy Categories
4.6.1. Education
4.6.2. Persuasion
4.6.3. Environmental Restructuring
4.6.4. Enablement
4.6.5. Incentivisation
4.6.6. Modelling
4.7. Predictors, Barriers and Facilitators That Influence Vaccination Uptake
4.7.1. Barriers to Vaccine Uptake That Affect Ethnic Minority Communities
4.7.2. Facilitators of Vaccine Uptake in Ethnic Minority Communities
4.7.3. Challenges of Intervention Implementation
5. Discussion
5.1. Limitations of the Review
5.2. Recommendations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sze, S.; Pan, D.; Nevill, C.R.; Gray, L.J.; Martin, C.A.; Nazareth, J.; Minhas, J.S.; Divall, P.; Khunti, K.; Abrams, K.R.; et al. Ethnicity and clinical outcomes in COVID-19: A systematic review and meta-analysis. EClinicalMedicine 2020, 29, 100630. [Google Scholar] [CrossRef] [PubMed]
- Robertson, E.; Reeve, K.S.; Niedzwiedz, C.L.; Moore, J.; Blake, M.; Green, M.; Katikireddi, S.V.; Benzeval, M.J. Predictors of COVID-19 vaccine hesitancy in the UK household longitudinal study. Brain Behav. Immun. 2021, 94, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg. Health Eur. 2021, 1, 100012. [Google Scholar] [CrossRef] [PubMed]
- Ekezie, W.; Czyznikowska, B.M.; Rohit, S.; Harrison, J.; Miah, N.; Campbell-Morris, P.; Khunti, K. The views of ethnic minority and vulnerable communities towards participation in COVID-19 vaccine trials. J. Public Health 2020, 43, e258–e260. [Google Scholar] [CrossRef]
- Gaughan, C.H.; Razieh, C.; Khunti, K.; Banerjee, A.; Chudasama, Y.V.; Davies, M.J.; Dolby, T.; Gillies, C.L.; Lawson, C.; Mirkes, E.M.; et al. COVID-19 vaccination uptake amongst ethnic minority communities in England: A linked study exploring the drivers of differential vaccination rates. J. Public Health 2023, 45, e65–e74. [Google Scholar] [CrossRef]
- Public Health England. Disparities in the Risk and Outcomes of COVID-19; Public Health England: London, UK, 2021. [Google Scholar]
- OpenSAFELY Collaborative; MacKenna, B.; Curtis, H.J.; Morton, C.E.; Inglesby, P.; Walker, A.J.; Morley, J.; Mehrkar, A.; Bacon, S.; Hickman, G.; et al. Trends, regional variation, and clinical characteristics of COVID-19 vaccine recipients: A retrospective cohort study in 23.4 million patients using OpenSAFELY. MedRxiv 2021. [Google Scholar] [CrossRef]
- ONS. Coronavirus and Vaccine Hesitancy, Great Britain: 26 May to 20 June 2021; Office of National Statistics: London, UK, 2021. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandwellbeing/bulletins/coronavirusandvaccinehesitancygreatbritain/26mayto20june2021 (accessed on 27 April 2023).
- Weinstein, N.D.; Kwitel, A.; McCaul, K.D.; Magnan, R.E.; Gerrard, M.; Gibbons, F.X. Risk perceptions: Assessment and relationship to influenza vaccination. Health Psychol. 2007, 26, 146–151. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- SAGE. Factors Influencing COVID-19 Vaccine Uptake among Minority Ethnic Groups; Executive Summary; Scientific Advisory Group for Emergencies: London, UK, 2020. [Google Scholar]
- Curtis, H.J.; Inglesby, P.; Morton, C.E.; MacKenna, B.; Green, A.; Hulme, W.; Walker, A.J.; Morley, J.; Mehrkar, A.; Bacon, S.; et al. Trends and clinical characteristics of COVID-19 vaccine recipients: A federated analysis of 57.9 million patients’ primary care records in situ using OpenSAFELY. Br. J. Gen. Pract. 2021, 72, e51–e62. [Google Scholar] [CrossRef]
- Reid, J.A.; Mabhala, M.A. Ethnic and minority group differences in engagement with COVID-19 vaccination programmes-at Pandemic Pace; when vaccine confidence in mass rollout meets local vaccine hesitancy. Isreal J. Health Policy Res. 2021, 10, 33. [Google Scholar] [CrossRef]
- WHO. Ten Threats to Global Health in 2019; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Marshall, S.; Fleming, A.; Sahm, L.J.; Moore, A.C. Identifying intervention strategies to improve HPV vaccine decision-making using behaviour change theory. Vaccine 2023, 41, 1368–1377. [Google Scholar] [CrossRef] [PubMed]
- Sabnis, S.S.; Conway, J.H. Overcoming Challenges to Childhood Immunizations Status. Pediatr. Clin. N. Am. 2015, 62, 1093–1109. [Google Scholar] [CrossRef] [PubMed]
- Hardt, K.; Bonanni, P.; King, S.; Santos, J.I.; El-Hodhod, M.; Zimet, G.D.; Preiss, S. Vaccine strategies: Optimising outcomes. Vaccine 2016, 34, 6691–6699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witteman, H.O. Addressing Vaccine Hesitancy with Values. Pediatrics 2015, 136, 215–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ala, A.; Edge, C.; Zumla, A.; Shafi, S. Specific COVID-19 messaging targeting ethnic minority communities. EClinicalMedicine 2021, 35, 100862. [Google Scholar] [CrossRef]
- Control ECfDPa. Guidance on Infection Prevention and Control of Coronavirus Disease (COVID-19) in Migrant and Refugee Reception and Detention Centres in the EU/EEA and the United Kingdom—June 2020; ECDC: Stockholm, Sweden, 2020. [Google Scholar]
- Corker, E.; Marques, M.; Johnston, M.; West, R.; Hastings, J.; Michie, S. Behaviour change techniques taxonomy v1: Feedback to inform the development of an ontology. Wellcome Open Res. 2023, 7, 211. [Google Scholar] [CrossRef]
- Howlett, N.; García-Iglesias, J.; Bontoft, C.; Breslin, G.; Bartington, S.; Freethy, I.; Huerga-Malillos, M.; Jones, J.; Lloyd, N.; Marshall, T.; et al. A systematic review and behaviour change technique analysis of remotely delivered alcohol and/or substance misuse interventions for adults. Drug Alcohol Depend. 2022, 239, 109597. [Google Scholar] [CrossRef]
- WHO. Strategies for Addressing Vaccine Hesitancy-A Systematic Review; WHO SAGE Working Group Dealing with Vaccine Hesitancy; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Bazargan, M.; Wisseh, C.; Adinkrah, E.; Ameli, H.; Santana, D.; Cobb, S.; Assari, S. Influenza Vaccination among Underserved African-American Older Adults. BioMed Res. Int. 2020, 2020, 2160894. [Google Scholar] [CrossRef]
- Hoppe, K.K.; Eckert, L.O. Achieving high coverage of H1N1 influenza vaccine in an ethnically diverse obstetric population: Success of a multifaceted approach. Infect. Dis. Obstet. Gynecol. 2011, 2011, 746214. [Google Scholar] [CrossRef] [Green Version]
- Pritchard, E.N.; Jutel, A.; Tollafield, S. Positive provider interventions for enhancing influenza vaccination uptake among Pacific peoples in New Zealand. N. Z. Med. J. 2011, 124, 75–82. [Google Scholar]
- NICE. Behaviour Change: Individual Approaches; National Institute for Health and Care Excellence: London, UK, 2014. [Google Scholar]
- Epton, T.; Lawes-Wickwar, S.; Ghio, D.; Shorter, G.W.; Whittaker, E.; Arden, M.A.; Armitage, C.; Byrne-Davis, L.; Chadwick, P.; Drury, J.; et al. Optimising Vaccination Uptake for COVID-19; British Psychological Society: London, UK, 2021. [Google Scholar]
- Wooten, K.G.; Wortley, P.M.; Singleton, J.A.; Euler, G.L. Perceptions matter: Beliefs about influenza vaccine and vaccination behavior among elderly white, black and Hispanic Americans. Vaccine 2012, 30, 6927–6934. [Google Scholar] [CrossRef]
- MRC. A Framework for the Development and Evaluation of RCTs for Complex Interventions to Improve Health; Medical Research Council: London, UK, 2000. [Google Scholar]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. Int. J. Nurs. Stud. 2013, 50, 587–592. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Sallis, A.; Bunten, A.; Bonus, A.; James, A.; Chadborn, T.; Berry, D. The effectiveness of an enhanced invitation letter on uptake of National Health Service Health Checks in primary care: A pragmatic quasi-randomised controlled trial. BMC Fam. Pract. 2016, 17, 35. [Google Scholar] [CrossRef] [Green Version]
- Garnett, C.V.; Crane, D.; Brown, J.; Kaner, E.F.S.; Beyer, F.R.; Muirhead, C.R.; Hickman, M.; Beard, E.; Redmore, J.; de Vocht, F.; et al. Behavior Change Techniques Used in Digital Behavior Change Interventions to Reduce Excessive Alcohol Consumption: A Meta-regression. Ann. Behav. Med. 2018, 52, 530–5433. [Google Scholar] [CrossRef] [Green Version]
- Alageel, S.; Gulliford, M.C.; McDermott, L.; Wright, A.J. Multiple health behaviour change interventions for primary prevention of cardiovascular disease in primary care: Systematic review and meta-analysis. BMJ Open 2017, 7, e015375. [Google Scholar] [CrossRef] [Green Version]
- Heron, N.; Kee, F.; Donnelly, M.; Cardwell, C.; Tully, M.A.; Cupples, M.E. Behaviour change techniques in home-based cardiac rehabilitation: A systematic review. Br. J. Gen. Pract. J. R. Coll. Gen. Pract. 2016, 66, e747–e757. [Google Scholar] [CrossRef] [Green Version]
- Laba, T.-L.; Bleasel, J.; Brien, J.-A.; Cass, A.; Howard, K.; Peiris, D.; Redfern, J.; Salam, M.A.; Usherwood, T.; Jan, S. Strategies to improve adherence to medications for cardiovascular diseases in socioeconomically disadvantaged populations: A systematic review. Int. J. Cardiol. 2013, 167, 2430–2440. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Kamal, A.; Ekezie, W.; Farooqi, A.; Khunti, K. A Systematic Review of Drivers of Vaccine Hesitancy and Strategies to Reduce Vaccine Hesitancy in Ethnic Minority Populations. PROSPERO 2021 CRD42021239010 2021. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021239010 (accessed on 23 February 2021).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CASP. Critical Appraisal Skills Programme Checklists 2018: Critical Appraisal Skills Programme. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 18 April 2021).
- Frew, P.M.; Kriss, J.L.; Chamberlain, A.T.; Malik, F.; Chung, Y.; Cortés, M.; Omer, S.B. A randomized trial of maternal influenza immunization decision-making: A test of persuasive messaging models. Hum. Vaccines Immunother. 2016, 12, 1989–1996. [Google Scholar] [CrossRef] [PubMed]
- Kriss, J.L.; Frew, P.M.; Cortes, M.; Malik, F.A.; Chamberlain, A.T.; Seib, K.; Flowers, L.; Ault, K.A.; Howards, P.; Orenstein, W.A.; et al. Evaluation of two vaccine education interventions to improve pertussis vaccination among pregnant African American women: A randomized controlled trial. Vaccine 2017, 35, 1551–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, K.; Berlin, M.; Schwartz, J.S.; Propert, K.; Ubel, P.A. Educational content and the effectiveness of influenza vaccination reminders. J. Gen. Intern. Med. 1999, 14, 695–698. [Google Scholar] [CrossRef] [Green Version]
- Daniels, N.A.; Juarbe, T.; Moreno-John, G.; Pérez-Stable, E.J. Effectiveness of adult vaccination programs in faith-based organizations. Ethn. Dis. 2007, 17, 15–22. [Google Scholar]
- Findley, S.E.; Irigoyen, M.; Sanchez, M.; Stockwell, M.S.; Mejia, M.; Guzman, L.; Ferreira, R.; Pena, O.; Chen, S.; Andres-Martinez, R. Effectiveness of a Community Coalition for Improving Child Vaccination Rates in New York City. Am. J. Public Health 2008, 98, 1959–1962. [Google Scholar] [CrossRef]
- Frew, P.M.; Zhang, S.; Saint-Victor, D.S.; Schade, A.C.; Benedict, S.; Banan, M.; Ren, X.; Omer, S.B. Influenza vaccination acceptance among diverse pregnant women and its impact on infant immunization. Hum. Vaccines Immunother. 2013, 9, 2591–2602. [Google Scholar] [CrossRef] [Green Version]
- Frew, P.M.; Owens, L.E.; Saint-Victor, D.S.; Benedict, S.; Zhang, S.; Omer, S.B. Factors associated with maternal influenza immunization decision-making: Evidence of immunization history and message framing effects. Hum. Vaccines Immunother. 2014, 10, 2576–2583. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Kalogriopoulou, K.; Pergialiotis, V.; Siahanidou, T.; Skiathitou, A.V.; Katerelos, P.; Goumalatsos, N.; Kostis, E.; Antsaklis, A.; Theodoridou, M. Acceptance of a post-partum influenza vaccination (cocooning) strategy for neonates in Greece. Vaccine 2012, 30, 5871–5874. [Google Scholar] [CrossRef]
- Nicoleau, A.; Nicoleau, C.A.; Balzora, J.D.; Oboh, A.; Siddiqui, N.; Rosenberg, C. Elderly African-Americans and the influenza vaccine: The impact of the primary care physician. J. Am. Med. Dir. Assoc. 2001, 2, 56–59. [Google Scholar] [CrossRef]
- Schwartz, K.L.; Neale, A.V.; Northrup, J.; Monsur, J.; Patel, D.A.; Tobar, R., Jr.; Wortley, P.M. Racial Similarities in Response to Standardized Offer of Influenza Vaccination A MetroNet Study. J. Gen. Intern. Med. 2006, 21, 346–351. [Google Scholar] [CrossRef]
- Wood, D.; Halfon, N.; Donald-Sherbourne, C.; Mazel, R.M.; Schuster, M.; Hamlin, J.S.; Pereyra, M.; Camp, P.; Grabowsky, M.; Duan, N. Increasing immunization rates among inner-city, African American children: A randomized trial of case management. J. Am. Med. Assoc. 1998, 279, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Callahan, A.G.; Strassberg, E.R.; Rhoades, C.P.; Varghese, L.; Schulkin, J.; Power, M.L. Pregnant Women’s Opinions and Acceptance of Influenza and Tdap Vaccines. J. Women’s Health 2022, 31, 656–664. [Google Scholar] [CrossRef]
- DiTosto, J.D.; Weiss, R.E.; Yee, L.M.; Badreldin, N. Association of Tdap vaccine guidelines with vaccine uptake during pregnancy. PLoS ONE 2021, 16, e0254863. [Google Scholar] [CrossRef]
- Larcher, V.F.; Bourne, J.; Aitken, C.; Jeffries, D.; Hodes, D. Overcoming barriers to hepatitis B immunisation by a dedicated hepatitis B immunisation service. Arch. Dis. Child. 2001, 84, 114–119. [Google Scholar] [CrossRef]
- Ma, G.X.; Gao, W.; Tan, Y.; Chae, W.G.; Rhee, J. A Community-Based Participatory Approach to a Hepatitis B Intervention for Korean Americans. Prog. Community Health Partnersh. Res. Educ. Action 2012, 6, 7–16. [Google Scholar] [CrossRef] [Green Version]
- McPhee, S.J.; Nguyen, T.; Euler, G.L.; Mock, J.; Wong, C.; Lam, T.; Nguyen, W.; Nguyen, S.; Ha, M.Q.H.; Do, S.T.; et al. Successful Promotion of Hepatitis B Vaccinations among Vietnamese-American Children Ages 3 to 18: Results of a Controlled Trial. Pediatrics 2003, 111, 1278–1288. [Google Scholar] [CrossRef] [Green Version]
- Nyamathi, A.; Salem, B.E.; Zhang, S.; Farabee, D.; Hall, B.; Khalilifard, F.; Leake, B. Nursing Case Management, Peer Coaching, and Hepatitis A and B Vaccine Completion among Homeless Men Recently Released on Parole: Randomized Clinical Trial. Nurs. Res. 2015, 64, 177–189. [Google Scholar] [CrossRef] [Green Version]
- Stringer, M.; Ratcliffe, S.; Gross, R. Acceptance of hepatitis B vaccination by pregnant adolescents. MCN Am. J. Matern. Nurs. 2006, 31, 54–60. [Google Scholar] [CrossRef]
- Zibrik, L.; Huang, A.; Wong, V.; Lauscher, H.N.; Choo, Q.; Yoshida, E.M.; Ho, K. Let’s Talk About B: Barriers to Hepatitis B Screening and Vaccination among Asian and South Asian Immigrants in British Columbia. J. Racial Ethn. Health Disparities 2018, 5, 1337–1345. [Google Scholar] [CrossRef]
- Dunn, R.A.; Shenouda, P.E.; Martin, D.R.; Schultz, A.J. Videotape Increases Parent Knowledge About Poliovirus Vaccines and Choices of Polio Vaccination Schedules. Pediatrics 1998, 102, e26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sagy, I.; Novack, V.; Gdalevich, M.; Greenberg, D. Mass media effect on vaccines uptake during silent polio outbreak. Vaccine 2018, 36, 1556–1560. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, B.; Jain, P.; Holder, B.S.; Lindsey, B.; Regan, L.; Kampmann, B. What determines uptake of pertussis vaccine in pregnancy? A cross sectional survey in an ethnically diverse population of pregnant women in London. Vaccine 2015, 33, 5822–5828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, P.; McNabb, P.; Maddali, S.R.; Heath, J.; Santibañez, S. Engaging Communities to Reach Immigrant and Minority Populations: The Minnesota Immunization Networking Initiative (MINI), 2006–2017. Public Health Rep. 2019, 134, 241–248. [Google Scholar] [CrossRef]
- Daniels, N.A.; Gouveia, S.; Null, D.; Gildengorin, G.L.; Winston, C.A. Acceptance of pneumococcal vaccine under standing orders by race and ethnicity. J. Natl. Med. Assoc. 2006, 98, 1089–1094. [Google Scholar]
- Bish, A.; Yardley, L.; Nicoll, A.; Michie, S. Factors associated with uptake of vaccination against pandemic influenza: A systematic review. Vaccine 2011, 29, 6472–6484. [Google Scholar] [CrossRef]
- Brien, S.; Kwong, J.C.; Buckeridge, D.L. The determinants of 2009 pandemic A/H1N1 influenza vaccination: A systematic review. Vaccine 2012, 30, 1255–1264. [Google Scholar] [CrossRef]
- Ekezie, W.; Maxwell, A.; Byron, M.; Czyznikowska, B.; Osman, I.; Moylan, K.; Gong, S.; Pareek, M. Health Communication and Inequalities in Primary Care Access during the COVID-19 Pandemic among Ethnic Minorities in the United Kingdom: Lived Experiences and Recommendations. Int. J. Environ. Res. Public Health 2022, 19, 15166. [Google Scholar] [CrossRef]
- Mowbray, F.; Marcu, A.; Godinho, C.A.; Michie, S.; Yardley, L. Communicating to increase public uptake of pandemic flu vaccination in the UK: Which messages work? Vaccine 2016, 34, 3268–3274. [Google Scholar] [CrossRef]
- O’Keefe, D.J.; Jensen, J.D. The relative persuasiveness of gain-framed and loss-framed messages for encouraging disease prevention behaviors: A meta-analytic review. J. Health Commun. 2007, 12, 623–644. [Google Scholar] [CrossRef]
- Chevallier, C.; Hacquin, A.-S.; Mercier, H. COVID-19 Vaccine Hesitancy: Shortening the Last Mile. Trends Cogn. Sci. 2021, 25, 331–333. [Google Scholar] [CrossRef]
- Mercier, H. Not Born Yesterday: The Science of Who We Trust and What We Believe; Princeton University Press: Princeton, NJ, USA, 2020. [Google Scholar]
- Vann, J.C.J.; Jacobson, R.M.; Coyne-Beasley, T.; Asafu-Adjei, J.K.; Szilagyi, P.G. Patient reminder and recall interventions to improve immunization rates (Review). Cochrane Database Syst. Rev. 2018, 1, CD003941. [Google Scholar] [CrossRef]
- Ekezie, W.; Awwad, S.; Krauchenberg, A.; Karara, N.; Dembiński, Ł.; Grossman, Z.; del Torso, S.; Dornbusch, H.J.; Neves, A.; Copley, S.; et al. Access to Vaccination among Disadvantaged, Isolated and Difficult-to-Reach Communities in the WHO European Region: A Systematic Review. Vaccines 2022, 10, 1038. [Google Scholar] [CrossRef]
- Crawshaw, A.F.; Deal, A.; Rustage, K.; Forster, A.S.; Campos-Matos, I.; Vandrevala, T.; Würz, A.; Pharris, A.; Suk, J.E.; Kinsman, J.; et al. What must be done to tackle vaccine hesitancy and barriers to COVID-19 vaccination in migrants? J. Travel Med. 2021, 28, taab048. [Google Scholar] [CrossRef]
- Caspi, G.; Dayan, A.; Eshal, Y.; Liverant-Taub, S.; Twig, G.; Shalit, U.; Lewis, Y.; Shina, A.; Caspi, O. Socioeconomic disparities and COVID-19 vaccination acceptance: A nationwide ecologic study. Clin. Microbiol. Infect. 2021, 27, 1502–1506. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Concept | Key Words |
|---|---|
| Vaccine hesitancy | vaccin* AND (hesitan* OR refus* OR confiden* OR accept* OR uptake* OR adopt*) |
| Minority ethnic groups | (ethnic group*) OR (ethnic minorit*) OR (minority group*) OR ethnic* OR minorit* OR race* OR racial OR Black* OR African* OR Asian* OR (South Asian*) OR Bangladeshi* OR(Pakistani*) OR Japanese OR Chinese or Korean* OR Arab* OR BME OR BAME OR Roma* OR Hispanic* OR Caribbean* OR (people of color) OR (person of color) OR Jewish OR Jews OR gyps* |
| Intervention | Interven* OR communicat* OR train* OR motiv* OR strateg* OR guid* OR program* OR support* OR polic* OR approach* OR procedure* OR plan* OR engag* |
| Study | Vaccine Focus | Study Design/ Study Period/ (Intervention Duration) | Country(s) of Study | Reported Ethnic Minority Group | Setting/Study Population Sample | Intervention/ Comparison (Control) | Intervention Outcomes | Vaccine Coverage/Uptake | Study Quality |
|---|---|---|---|---|---|---|---|---|---|
| Armstrong et al., 1999 [46] | Influenza | RCT 1996–1997 (7 months) | United States | African American | Primary care clinic n = 740 community-dwelling individuals | Education brochure Mailed postcard reminder Comparison Mailed postcard reminder without educational content |
| Educational brochure group more likely to be vaccinated than postcard reminder group (66.4% vs. 56.9%, p = 0.04) | Moderate |
| Callahan et al., 2022 [55] | Influenza, Tetanus, Diphtheria, Pertussis (Tdap) | Cross-sectional (Survey) 2019–2021 (15 months) | United States | Black | Hospital n = 664 women | Reading informational text | Influenza vaccination during pregnancy: 52.5% already vaccinated, 10% planned to be vaccinated, 3.1% planned to be vaccinated after giving birth; 34.0% did not plan to receive the influenza vaccine this season, 0.4% did not answer Tdap vaccination during pregnancy: 25.5% already received; at 3rd trimester (63.7% vaccinated; 30.9% not planning to be vaccinated), 37.8% of unvaccinated planned to be vaccinated Ethnicity
| NR | High |
| Daniels et al., 2007 [47] | Influenza, Pneumococcal | RCT 2003–2004 (2 months) 2005–2006 (4 months) | United States | African American Asian Latino | Community (Faith based-Churches) n = 330 | Vaccine educationOn-site vaccination Comparison Vaccine education only |
| Vaccine utilisation
| Moderate |
| DiTosto et al., 2021 [56] | Influenza, Tetanus, Diphtheria, Pertussis (Tdap) Pneumococcal | Cohort (Retrospective) 2011–2015 (4 years) | United States | Non-Hispanic White Non-Hispanic Black Asian Hispanic | Hospital n = 2294 women | Guideline | Received prenatal care post-guideline: 70.2% (n = 1610/2294) Post-guideline cohort:
| Vaccine uptake pre- and post-guideline
| High |
| Donaldson et al., 2015 [65] | Pertussis | Cross-sectional 2013–2014 (14 months) | United Kingdom | Asian Black | Healthcare centre/clinic n = 200 women | Communication campaign Comparison Standard routine vaccination |
|
| High |
| Dunn et al., 1998 [63] | Polio | RCT 1997 (4 months) | United States | African-American Hispanic/Latino Asian Native American | Paediatric offices and local health department immunization clinic n = 287 parents/guardians | Education Comparison Usual routines with respect to presentation of VIS and vaccine discussions and recommendations with the parent/guardian |
| NR | Moderate |
| Findley et al., 2008 [48] | Diphtheria, Tetanus, Pertussis, Polio, Measles, Mumps, Rubella, Haemophilus Influenza, Hepatitis | Cohort (Retrospective) 2006–2007 | United States | Latino | Community n = 10,857 children | Outreach Education Reminders Comparison No intervention |
|
| High |
| Frew et al., 2013 [49] | Influenza | RCT 2011–2012 (9 months) | United States | Black/African American Hispanic/Latino | Clinics n = 261 pregnant women | Message framing Control Usual care |
| NR | Moderate |
| Frew et al., 2014 [50] | Influenza | RCT 2011–2012 (9 months) | United States | Black/African American Hispanic/Latino | Clinics n = 251 women | Message framing Comparison Control messages |
| NR | Moderate |
| Frew et al., 2016 [44] | Influenza | RCT 2013 (4 months) | United States | Black/African American | Antenatal clinic n = 65 pregnant women | Video Comparison 34 participants-comparison condition (receipt of the Influenza Vaccine Information Statement) |
| Arm 1 (comparison group) = 12% (4/34) Arm 2 (pregnant pause movie) = 13% (4/31) Arm 3 (vaccines for a healthy pregnancy iBook) = 7% (2/30) | Moderate |
| Kriss et al., 2017 [45] | Diphtheria, Tetanus, Pertussis | RCT 2013 (4 months) | United States | African American | Antenatal clinics n = 106 women | Messaging video and a cognitive messaging iBook Comparison Standard CDC Vaccine Information Statements (VIS) |
| Prenatal Tdap vaccination: Control (18%), iBook group (50%), video group (29%) | High |
| Larcher et al., 2001 [57] | Hepatitis B | Cross-sectional (Retrospective) Babies born 1992–1996 (5 years) | United Kingdom | Black African Caribbean Asian Turkish Vietnamese | Hospitals (clinic) n = 265 infants born to hepatitis B carrier mothers | National program (Hackney residents) Comparison Hackney non-residents |
|
| Moderate |
| Ma et al., 2012 [58] | Hepatitis B | Mixed methods (Quasi-experiment (RCT), interview, survey, workshops) 12 months | United States | Korean American (Asian) | Community (Faith based-Churches) n = 330 | Community-based participatory research (CBPR) Comparison Concurrent control group with no intervention offered | Short-term intervention effects of primary outcomes
| Vaccination prevalence rate: 33% (33% vs. 0%) | High |
| Maltezou et al., 2012 [51] | Influenza | Cohort (Prospective) 2011–2012 | Greece | RomaImmigrants | Tertiary hospital (clinic) n = 224 mothers | Household vaccination recommendation |
|
| High |
| McPhee et al., 2003 [59] | Hepatitis B | RCT 1998–2000 (2 years) | United States | Vietnamese American (Asian) | Community n = 2648 1547 parents; 1101 providers (for Children 3 to 18 years) | Media-led information and education outreach campaigns. Comparison Children living in the control (Washington, DC) area. different location so received none of the interventions. |
| Receipt of 3 hepatitis B vaccinations: increased in community mobilization (26.6% to 38.8%) and media intervention (28.5% to 39.4%) areas; declined in control community (37.8% to 33.5%) | Moderate |
| Nicoleau et al., 2001 [51] | Influenza | Cohort (Prospective) 1999 (2 months) | United States | African American | Private clinic n = 231 | Discussion with physician Comparison Before discussion with physician |
| NR | High |
| Nyamathi et al., 2015 [60] | Hepatitis A and B | RCT 2010–2013 (12 months) | United States | African American Latino Asian/Pacific Islander | Community n = 600 recently paroled men | Coaching Comparison None (or “Usual care”) |
| Vaccine completion rate for ≥3 doses: 73% among all three interventions | Moderate |
| Peterson et al., 2019 [66] | General | Cross Sectional (Program report) 2006–2017 (3 years) | United States | Black/African Asian/Pacific Islander Hispanic/Latino American Indian | Community (Faith based-Churches) n = 5910 | Community-based vaccination clinics |
| 5910 first time vaccine administered through 99 community-based vaccination clinics (uninsured (43.1%)) | Moderate |
| Sagy et al., 2018 [64] | Polio | Cross-sectional (Retrospective) 2013 (3 months) | Israel | Jewish Non-Jewish | Medical records (clinic) n = 138,799 OPV vaccines administered | National programme |
| 138,799 bOPV vaccines given (80–90% coverage) | Moderate |
| Schwartz et al., 2006 [53] | Influenza | Cross-sectional (Prospective) 2003–2004 (4 months) | United States | African American | Primary care clinics n = 454 patients | Medical assistant (MA)-initiated universal standardized vaccination |
| African–American (62.1%) White (68.9%) | High |
| Stringer et al., 2006 [61] | Hepatitis B | Cohort 1999–2000 (12 months) | United States | African American | Tertiary clinic n = 160 | Information pamphlet Reoffering vaccine |
| Actual vaccination uptake (86%, 131/154) | Moderate |
| Wood et al., 1998 [54] | Diphtheria Tetanus Pertussis vaccinations, Polio Haemophilus Influenza B | RCT 15 months | United States | African American | Community n = 419 infants | Case management Health passport Comparison Health passport only |
| Immunization completion: - Case management group (63.8%). - Control (50.6%) | Moderate |
| Zibrik et al., 2018 [62] | Hepatitis B | Cohort (Mixed methods) 2014 (12 months) | Canada | Asian/South Asian | Community n = 827 | Workshop |
| Vaccinated against HBV: 41.3% (n = 331) | High |
| Study (Author, Year) | Components | Model of Behaviour | Intervention Function | Policy Categories | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Capability | Opportunity | Motivation | Physical Capability | Psychological Capability | Physical Opportunity | Social Opportunity | Reflective Motivation | Automatic Motivation | Education | Persuasion | Incentivisation | Coercion | Training | Restriction | Environmental Restructuring | Modelling | Enablement | Communication/Marketing | Guidelines | Fiscal | Regulation | Legislation | Environmental/Social Planning | Service Provision | |
| Armstrong et al., 1999 [46] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||
| Callahan et al., 2022 [55] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||||
| Daniels et al., 2007 [47] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||
| DiTosto et al., 2021 [56] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||
| Donaldson et al., 2015 [65] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||
| Dunn et al., 1998 [63] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||||||
| Findley et al., 2008 [48] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||
| Frew et al., 2013 [49] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||||||
| Frew et al., 2014 [50] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||||||
| Frew et al., 2016 [44] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||
| Kriss et al., 2017 [45] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||
| Larcher et al., 2001 [57] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||||||
| Ma et al., 2012 [58] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||
| Maltezou et al., 2012 [51] | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||||||
| McPhee et al., 2003 [59] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||
| Nicoleau A et al., 2001 [51] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||
| Nyamathi et al., 2015 [60] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||
| Peterson et al., 2019 [66] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||
| Sagy et al., 2018 [64] | ✓ | ✓ | ✓ | ✓ | |||||||||||||||||||||
| Schwartz et al., 2006 [53] | ✓ | ✓ | ✓ | ✓ | |||||||||||||||||||||
| Stringer et al., 2006 [61] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||||
| Wood et al., 1998 [54] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||
| Zibrik et al., 2018 [62] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||
| TOTAL (n = studies) | 19 | 15 | 19 | 2 | 20 | 7 | 8 | 18 | 1 | 21 | 17 | 2 | 0 | 0 | 0 | 8 | 1 | 9 | 17 | 19 | 2 | 6 | 0 | 9 | 11 |
| BCT Group | BCT | Armstrong et al., 1999 [46] | Callahan et al., 2022 [55] | Daniels et al., 2007 [47] | DiTosto et al., 2021 [56] | Donaldson et al., 2015 [65] | Dunn et al., 1998 [63] | Findley et al., 2008 [48] | Frew et al., 2013 [49] | Frew et al., 2014 [50] | Frew et al., 2016 [44] | Kriss et al., 2017 [45] | Larcher et al., 2001 [57] | Ma et al., 2012 [58] | Maltezou et al., 2012 [51] | McPhee et al., 2003 [59] | Nicoleau A et al., 2001 [51] | Nyamathi et al., 2015 [60] | Peterson et al., 2019 [66] | Sagy et al., 2018 [64] | Schwartz et al., 2006 [53] | Stringer et al., 2006 [61] | Wood et al., 1998 [54] | Zibrik et al., 2018 [62] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Goals and planning | 1.2. Problem solving | ✓ | ||||||||||||||||||||||
| 1.3. Goal setting (outcome) | ✓ | |||||||||||||||||||||||
| 2. Feedback and monitoring | 2.1. Monitoring of behaviour by others without feedback | ✓ | ✓ | ✓ | ||||||||||||||||||||
| 2.5. Monitoring of outcome(s) of behaviour without feedback | ✓ | |||||||||||||||||||||||
| 3. Social support | 3.1. Social support (unspecified) | ✓ | ||||||||||||||||||||||
| 3.2. Social support (practical) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||||
| 4. Shaping knowledge | 4.1. Instruction on how to perform the behaviour | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||
| 4.2. Information about Antecedents | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||
| 5. Natural consequences | 5.1. Information about health consequences | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||
| 5.2. Salience of consequences | ✓ | ✓ | ✓ | |||||||||||||||||||||
| 5.3. Information about social and environmental consequences | ✓ | |||||||||||||||||||||||
| 5.5. Anticipated regret | ✓ | |||||||||||||||||||||||
| 6. Comparison of behaviour | 6.1 Demonstration of the behaviour | ✓ | ||||||||||||||||||||||
| 6.2. Social comparison | ✓ | ✓ | ||||||||||||||||||||||
| 7. Association | 7.1. Prompts/cues | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||
| 7.7 Exposure | ✓ | |||||||||||||||||||||||
| 8. Repetition and substitution | 8.1. Behavioural practice/rehearsal | ✓ | ||||||||||||||||||||||
| 9. Comparison of outcomes | 9.1. Credible source | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||
| 9.2. Pros and cons | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||||||
| 9.3. Comparative imagining of future outcomes | ✓ | |||||||||||||||||||||||
| 10. Reward and threat | 10.1. Material incentive (behaviour) | ✓ | ✓ | |||||||||||||||||||||
| 10.10. Reward (outcome) | ✓ | |||||||||||||||||||||||
| 12. Antecedents | 12.1. Restructuring the physical environment | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||
| 12.2. Restructuring the social environment | ✓ | |||||||||||||||||||||||
| 12.5. Adding objects to the environment | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||||
| 13. Identity | 13.2. Framing/reframing | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||
| No. of BCT within each study | 4 | 2 | 3 | 4 | 5 | 4 | 8 | 7 | 4 | 4 | 5 | 5 | 7 | 3 | 9 | 3 | 9 | 6 | 1 | 1 | 1 | 6 | 5 | |
| Study | Hesitancy/ Predictors Factors | Barriers to Uptake | Facilitators to Uptake | Intervention Challenges |
|---|---|---|---|---|
| Callahan et al., 2022 [55] |
|
|
|
|
| Daniels et al., 2007 [47] | Reasons for declining: Fear of shots; need more information; fear of vaccine-related illness; do not believe it is necessary. |
| NR | NR |
| DiTosto et al., 2021 [56] |
| NR |
|
|
| Donaldson et al., 2015 [65] |
|
|
| |
| Dunn et al., 1998 [63] | NR |
| NR |
|
| Frew et al., 2013 [49] | NR | NR |
| NR |
| Frew et al., 2014 [50] | NR | NR |
| |
| Frew et al., 2016 [44] | NR |
| NR |
|
| Kriss et al., 2017 [45] | NR |
| NR |
|
| Larcher et al., 2001 [57] | NR |
| NR |
|
| Ma et al., 2012 [58] | NR | NR | NR |
|
| Maltezou et al., 2012 [51] | Reasons for vaccine refusal: not wanting the vaccine, self-perception of not being at risk for contacting influenza. | NR | Significant factors associated with increased vaccination rates: being of Roma origin or an immigrant, giving birth to neonate with birth weight < 2500 g, and residing in a family with ≥4 family members. |
|
| McPhee et al., 2003 [59] | Predictors for three doses of HepB: older children, number of years since the parent immigrated, household income above the poverty line, having health insurance. |
|
|
|
| Nicoleau et al., 2001 [51] | Vaccine not recommended or not recommended strongly; perception of no benefit of taking vaccine; history of sickness after vaccination; too afraid; know people who became ill; egg allergy; never had influenza. | NR | NR | NR |
| Nyamathi et al., 2015 [60] | Predictors of vaccine noncompletion: Asian and Pacific Islander ethnicity; experiencing high levels of hostility; positive social support; history of injection drug use; released early from California prisons; admitted for psychiatric illness. | NR |
|
|
| Peterson et al., 2019 [66] | Refusal due to perceptions around importance and efficacy. Factors affecting vaccine uptake, delivery and PHC access: challenges to navigating the health system; transnational use of health services; language and literacy; expectations of vaccination delivery (comparison of vaccination programmes between countries); vaccine acceptance; vaccine accessibility (appointment booking and appointment length and Vaccination reminders); trust. | NR | NR |
|
| Schwartz et al., 2006 [53] | History of sickness from past vaccination; knowing someone who got sick; fear of side effects; vaccine will not prevent flu; fear of needles; not wanting it; flu not a serious disease; do not want to get the flu. | NR | NR | - Vaccine supplies exhausted before expected study end date. |
| Stringer et al., 2006 [61] | There were no differences between the acceptors and non-acceptors with respect to their behavioural and attitudinal HBV beliefs. | NR |
|
|
| Wood et al., 1998 [54] | NR | NR |
|
|
| Zibrik et al., 2018 [62] | NR |
| NR |
|
| Recommendation | BCT |
|---|---|
| Include a range of educational resources that are written (e.g., brochures and information sheets), visual (e.g., video) and interactive (e.g., workshops) to increase awareness Multiple message exposure is likely to be more effective than single message exposure. | Instruction on how to perform the behaviour Prompts/cues Adding objects to the environment Information about health consequences |
The content of vaccine messages should:
| Information about Antecedents Information about health consequences Pros and cons Comparative imagining of future outcomes Framing/reframing |
| Provide culturally specific information and interpretation in the local languages of the ethnic minority groups. | Information about Antecedents Information about health consequences Adding objects to the environment Framing/reframing |
| Use a combination of public health strategies/campaigns with direct contact and follow-up services available in a timely manner to address any vaccine queries or concerns. | Exposure Problem solving Credible source Information about health consequences |
| Train peer health educators and credible sources within the community (e.g., religious leaders) to promote vaccine uptake in community settings. | Restructuring the social environment Credible source Social support |
| Include family and close contacts when providing vaccine services by sharing educational resources and opportunities for dialogue. | Social support |
| Use community settings (e.g., community clinics, faith, etc.) to inform people about vaccination. | Restructuring the social environment Restructuring the physical environment Information about health consequences |
| Provide flexible vaccine clinic hours. | Restructuring the physical environment |
| Include bilingual medical staff in the community. | Restructuring the social environment |
| Provide vaccines free of charge to remove the cost barrier from patients. | Material incentive |
| Use problem-solving of barriers (such as identifying financial barriers or problems with transportation), goal setting and provide instructions on how to take action. | Problem solving Goal setting Instruction on how to perform the behaviour |
| Include encouragement from professionals to address uncertainties about the risk and benefits of vaccines. | Credible source Monitoring of behaviour by others |
| Monitoring from credible sources to contact families that do not receive vaccinations, and subsequent contact from health visitors to reinforce the importance of vaccine uptake. | Monitoring of behaviour by others |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ekezie, W.; Connor, A.; Gibson, E.; Khunti, K.; Kamal, A. A Systematic Review of Behaviour Change Techniques within Interventions to Increase Vaccine Uptake among Ethnic Minority Populations. Vaccines 2023, 11, 1259. https://doi.org/10.3390/vaccines11071259
Ekezie W, Connor A, Gibson E, Khunti K, Kamal A. A Systematic Review of Behaviour Change Techniques within Interventions to Increase Vaccine Uptake among Ethnic Minority Populations. Vaccines. 2023; 11(7):1259. https://doi.org/10.3390/vaccines11071259
Chicago/Turabian StyleEkezie, Winifred, Aaisha Connor, Emma Gibson, Kamlesh Khunti, and Atiya Kamal. 2023. "A Systematic Review of Behaviour Change Techniques within Interventions to Increase Vaccine Uptake among Ethnic Minority Populations" Vaccines 11, no. 7: 1259. https://doi.org/10.3390/vaccines11071259