

Cost-Effectiveness of Pneumococcal Vaccination in Adults in Italy: Comparing New Alternatives and Exploring the Role of GMT Ratios in Informing Vaccine Effectiveness
 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
1.1. Pneumococcal Epidemiology
1.2. Pneumococcal Vaccination in Italy
1.3. Objective
2. Materials and Methods
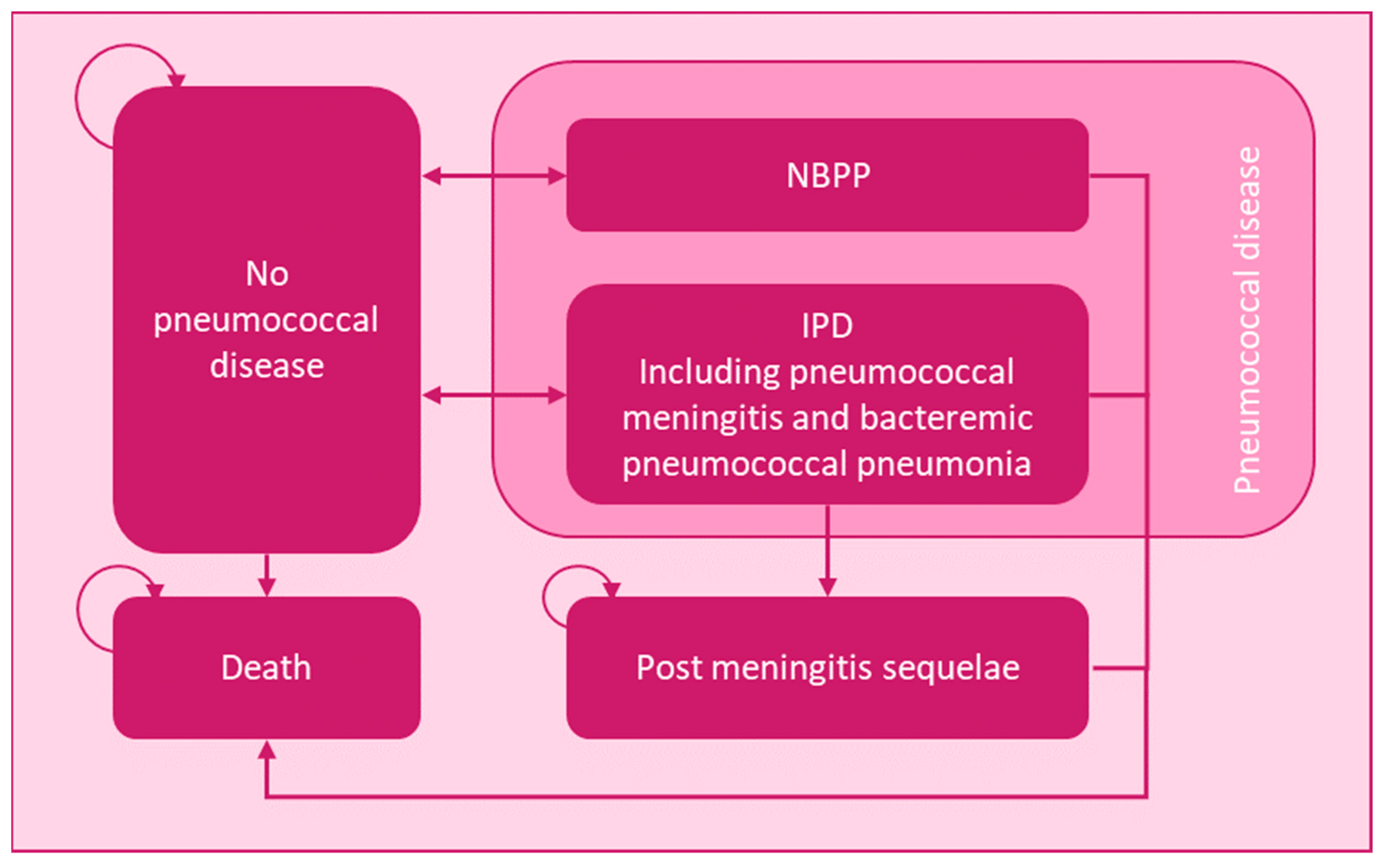
2.1. Model Structure
2.2. Population, Intervention, and Comparator
2.3. Clinical Inputs
2.4. Utilities
2.5. Cost Inputs
2.6. Outcomes
3. Results
3.1. Base Case Results
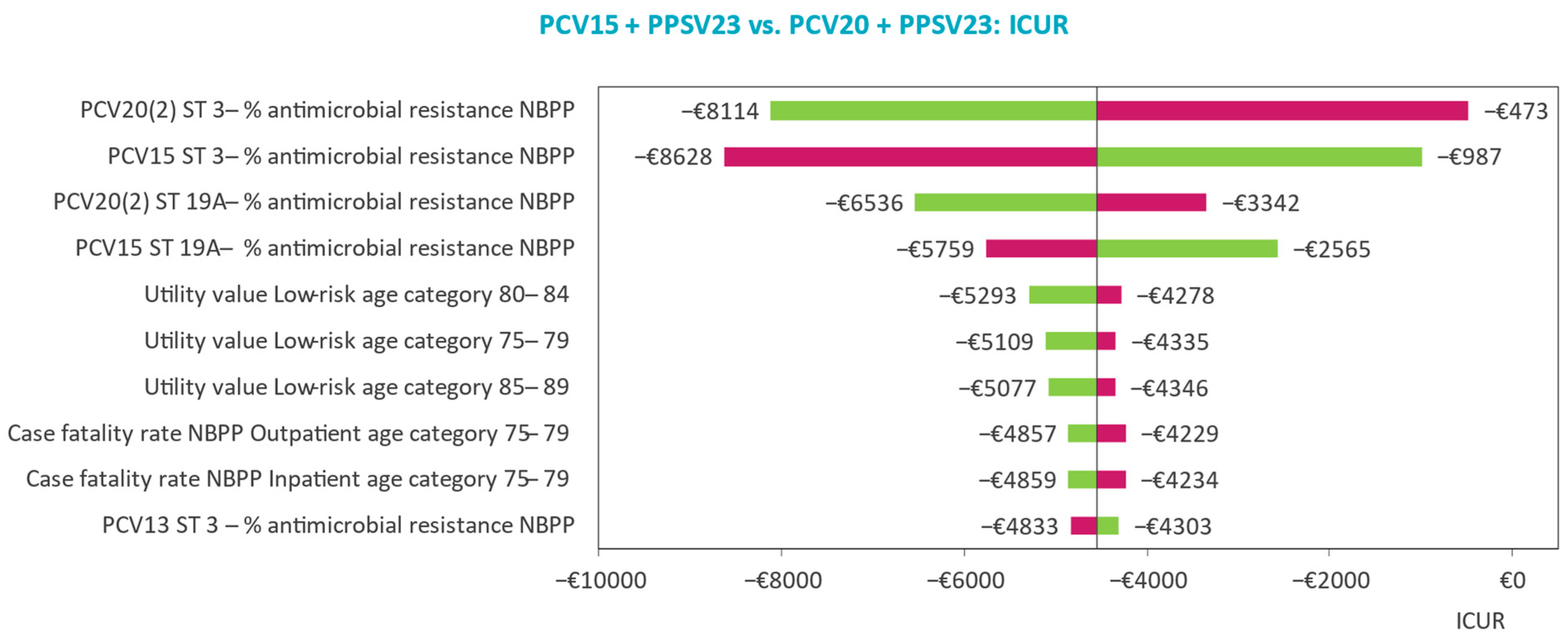
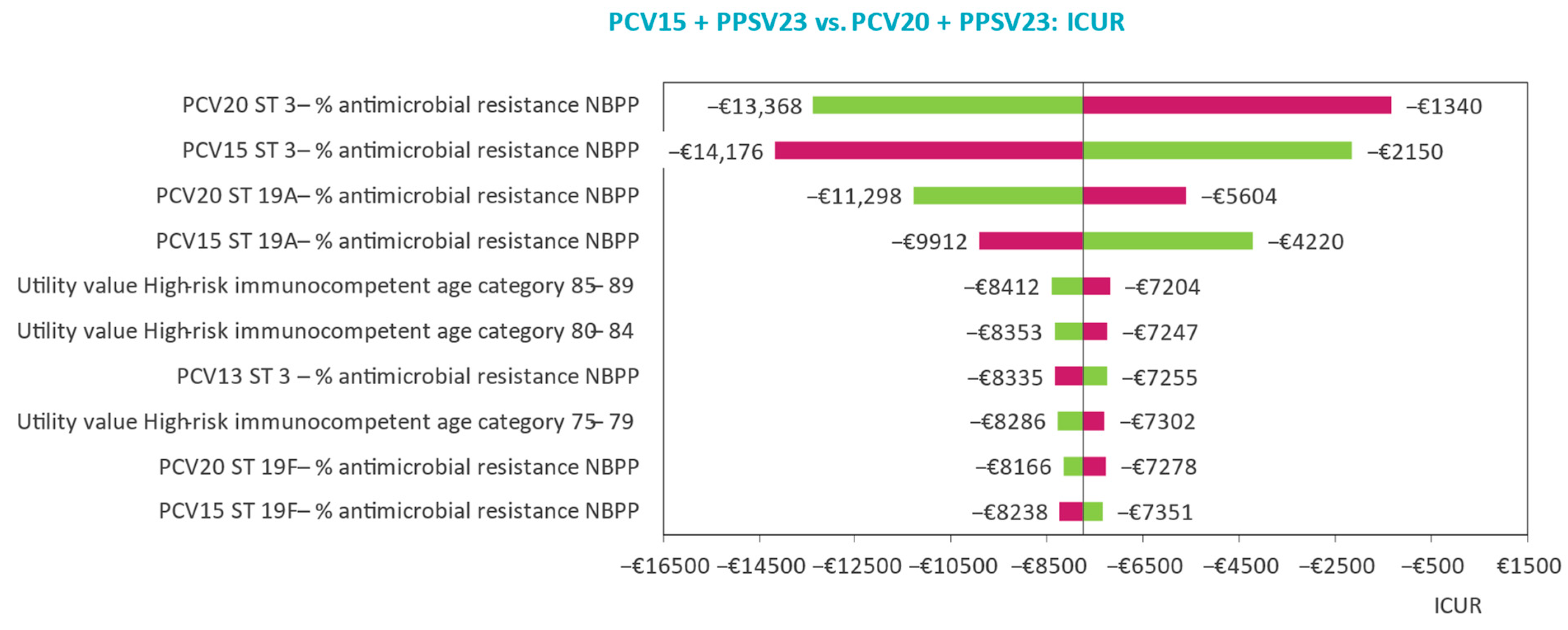
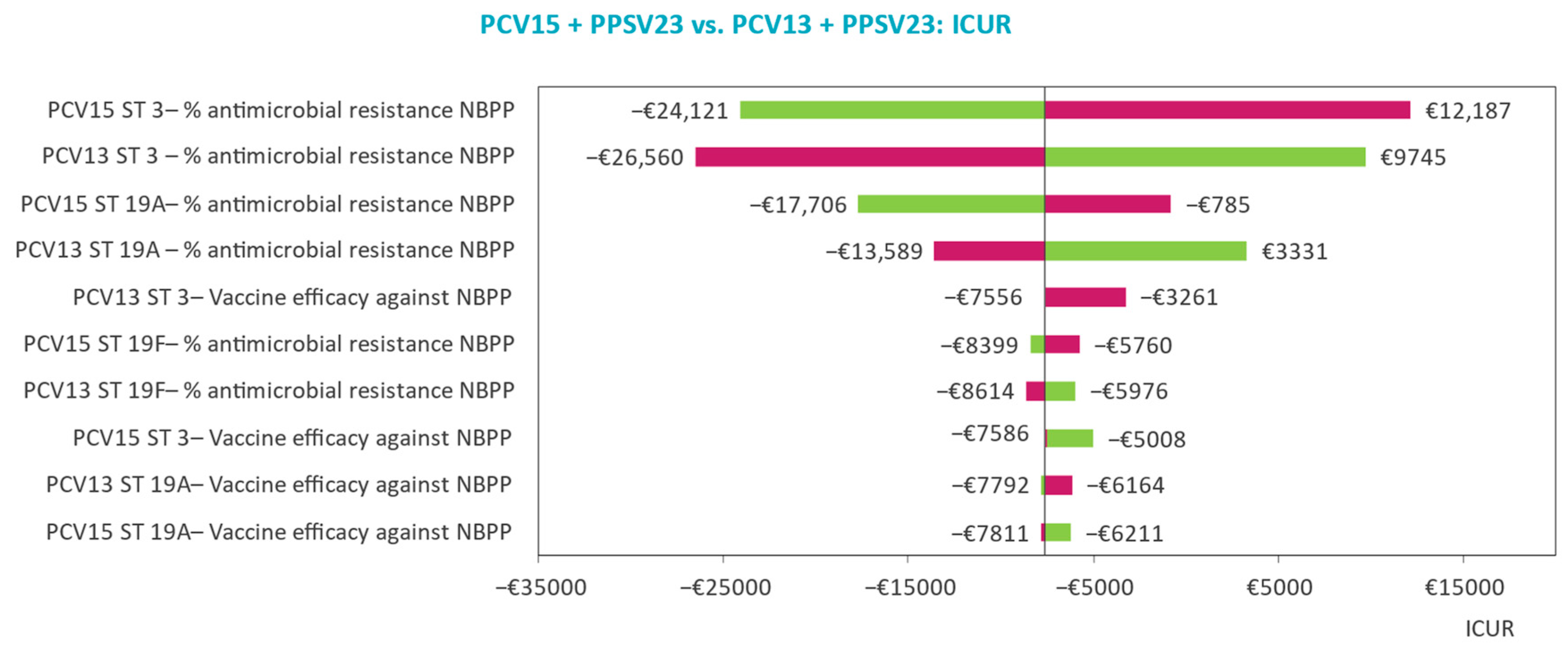
3.2. Deterministic Sensitivity Analyses
3.3. Probabilistic Sensitivity Analyses
3.4. Scenario Analyses
4. Discussion
4.1. Base Case Findings
4.2. Sensitivity and Scenario Analyses Findings
4.3. Analysis Strengths
4.4. Comparison with Existing Literature
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Pneumococcal Disease. Available online: http://www.who.int/ith/diseases/pneumococcal/en/ (accessed on 17 March 2023).
- World Health Organization. International Travel and Health: Pneumococcal Disease 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Istituto Superiore di Sanità. Sorveglianza delle Malattie Batteriche Invasive Aggiornati al 3 Aprile 2017; Rome, Italy, 2020. Available online: https://www.iss.it/documents/20126/0/Rapporto+consolidato+MIB+2019.pdf/1faeb457-9859-f800-b9aa-bf8aea405093?t=1612517562338 (accessed on 17 March 2023).
- Lombardi, D.P.C. Le Malattie Batteriche Invasive in Piemonte. Report 2019 ed. 2020. Available online: https://www.seremi.it/sites/default/files/REPORT%20MIB%202019%20ed%202020.pdf (accessed on 17 March 2023).
- Monali, R.; De Vita, E.; Mariottini, F.; Privitera, G. Impact of vaccination on invasive pneumococcal disease in Italy 2007–2017: Surveillance challenges and epidemiological changes. Epidemiol. Infect. 2020, 148, e187. [Google Scholar] [CrossRef]
- Baldo, V.; Cocchio, S.; Gallo, T.; Furlan, P.; Clagnan, E.; Del Zotto, S.; Saia, M.; Bertoncello, C.; Buja, A.; Baldovin, T. Impact of pneumococcal conjugate vaccination: A retrospective study of hospitalization for pneumonia in North-East Italy. J. Prev. Med. Hyg. 2016, 57, E61–E68. [Google Scholar]
- Baldovin, T.; Lazzari, R.; Russo, F.; Bertoncello, C.; Buja, A.; Furlan, P.; Cocchio, S.; Palù, G.; Baldo, V. A surveillance system of Invasive Pneumococcal Disease in North-Eastern Italy. Ann. Ig. 2016, 28, 15–24. [Google Scholar] [PubMed]
- World Health Organization. Pneumococcal Vaccines. 2003. Available online: https://archives.who.int/vaccines/en/pneumococcus.shtml (accessed on 17 March 2023).
- Hu, T.; Weiss, T.; Bencina, G.; Owusu-Edusei, K.; Petigara, T. Health and economic burden of invasive pneumococcal disease associated with 15-valent pneumococcal conjugate vaccine serotypes in children across eight European countries. J. Med. Econ. 2021, 24, 1098–1107. [Google Scholar] [CrossRef] [PubMed]
- Ministero della Salute. Piano Nazionale Prevenzione Vaccinale 2017–2019; Ministero della Salute: Rome, Italy, 2017. [Google Scholar]
- European Medicines Agency. Summary of Opinion Vaxneuvance; European Medicines Agency: Amsterdam, The Netherlands, 2022. [Google Scholar]
- European Medicines Agency. Summary of Opinion Apexxnar; European Medicines Agency: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Mt-Isa, S.; Abderhalden, L.A.; Musey, L.; Weiss, T. Matching-adjusted indirect comparison of pneumococcal vaccines V114 and PCV20. Expert. Rev. Vaccines 2022, 21, 115–123. [Google Scholar] [CrossRef]
- Deb, A.; Guggisberg, P.; Mutschler, T.; Owusu-Edusei, K.; Bencina, G.; Johnson, K.D.; Ignacio, T.; Mathijssen, D.A.R.; Qendri, V. Cost-effectiveness of the 15-valent pneumococcal conjugate vaccine for high-risk adults in Switzerland. Expert. Rev. Vaccines 2022, 21, 711–722. [Google Scholar] [CrossRef] [PubMed]
- Stoecker, C.; Kobayashi, M.; Matanock, A.; Cho, B.H.; Pilishvili, T. Cost-effectiveness of continuing pneumococcal conjugate vaccination at age 65 in the context of indirect effects from the childhood immunization program. Vaccine 2020, 38, 1770–1777. [Google Scholar] [CrossRef]
- Instituto Nazionale di Statistica. Resident Population on 1st January 2020 by Age. 2020. Available online: http://dati.istat.it/Index.aspx?QueryId=42869&lang=en (accessed on 17 March 2023).
- Instituto Nazionale di Statistica. Indagine Multiscopo Sulle Famiglie: Aspetti Della Vita Quotidiana, Condivzioni di Salute. 2019. Available online: https://www.istat.it/it/archivio/91926 (accessed on 17 March 2023).
- Veneto. Flussi Informativi Delle Meningiti e Delle Malattie Batteriche Invasive Presenti Nella Regione Veneto. 2021. Available online: https://www.regione.veneto.it/web/sanita/malattie-batterico-invasive (accessed on 17 March 2023).
- European Medicines Agency. Summary of Risk Management Plan for Apexxnar (20-Valent Pneumococcal Polysaccharide Conjugate Vaccine [20vpnc]); European Medicines Agency: Amsterdam, The Netherlands, 2022. [Google Scholar]
- European Centre for Disease Prevention and Control. Invasive Pneumococcal Disease: Annual Epidemiological Report for 2018; European Centre for Disease Prevention and Control: Stockholm, Switzerland, 2020. [Google Scholar]
- Ochoa-Gondar, O.; Vila-Corcoles, A.; Rodriguez-Blanco, T.; Gomez-Bertomeu, F.; Figuerola-Massana, E.; Raga-Luria, X.; Hospital-Guardiola, I. Effectiveness of the 23-Valent Pneumococcal Polysaccharide Vaccine Against Community-Acquired Pneumonia in the General Population Aged ≥60 Years: 3 Years of Follow-up in the CAPAMIS Study. Clin. Infect. Dis 2014, 58, 909–917. [Google Scholar] [CrossRef]
- Pilishvili, T.; Almendares, O.M.; Nanduri, S.; Warnock, R.; Wu, X.; McKean, S.; Kelman, J.; Farley, M.M.; Schaffner, W.; Thomas, A.; et al. Evaluation of Pneumococcal Vaccine Effectiveness Against Invasive Pneumococcal Disease among US Medicare Beneficiaries ≥65 Years Old. Open. Forum. Infect. 2018, 5 (Suppl. S1), S10–S11. [Google Scholar] [CrossRef]
- Pilishvili, T. 13-Valent Pneumococcal Conjugate Vaccine (PCV13) Effects on Disease Caused by Serotype 3. In Proceedings of the Virtual ACIP Meeting, Atlanta, GA, USA, 28 February 2019; National Center for Immunization & Respiratory Diseases, 2019. Available online: https://stacks.cdc.gov/view/cdc/78091 (accessed on 17 March 2023).
- Bonten, M.J.; Huijts, S.M.; Bolkenbaas, M. Vaccine against Pneumococcal Pneumonia in Adults. N. Engl. J. Med. 2015, 373, 93. [Google Scholar]
- Falkenhorst, G.; Remschmidt, C.; Harder, T.; Hummers-Pradier, E.; Wichmann, O.; Bogdan, C. Effectiveness of the 23-Valent Pneumococcal Polysaccharide Vaccine (PPV23) against Pneumococcal Disease in the Elderly: Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169368. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Dhoubhadel, B.G.; Ishifuji, T.; Yasunami, M.; Yaegashi, M.; Asoh, N.; Ishida, M.; Hamaguchi, S.; Aoshima, M.; Ariyoshi, K.; et al. Serotype-specific effectiveness of 23-valent pneumococcal polysaccharide vaccine against pneumococcal pneumonia in adults aged 65 years or older: A multicentre, prospective, test-negative design study. Lancet Infect. Dis. 2017, 17, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Suaya, J.A.; Mendes, R.E.; Sings, H.L.; Arguedas, A.; Reinert, R.R.; Jodar, L.; Isturiz, R.E.; Gessner, B.D. Streptococcus pneumoniae serotype distribution and antimicrobial nonsusceptibility trends among adults with pneumonia in the United States, 2009–2017. J. Infect. 2020, 81, 557–566. [Google Scholar] [CrossRef]
- Treskova, M.; Scholz, S.M.; Kuhlmann, A. Cost Effectiveness of Elderly Pneumococcal Vaccination in Presence of Higher-Valent Pneumococcal Conjugate Childhood Vaccination: Systematic Literature Review with Focus on Methods and Assumptions. Pharmacoeconomics 2019, 37, 1093–1127. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines on Clinical Evaluation of Vaccines: Regulatory Expectations. In WHO Technical Report Series 1004; World Health Organization: Geneva, Switzerland, 2017; p. 72. [Google Scholar]
- Agenzia Italiana del Farmaco. National Report on Medicines Use in Italy. Available online: https://www.aifa.gov.it/en/web/guest/uso-dei-farmaci-in-italia (accessed on 17 March 2023).
- Sanduzzi, A.; Canora, A.; Belfiore, P.; Bocchino, M.; Liguori, R.; Liguori, G. Impact of 13Valent Vaccine for Prevention of Pneumococcal Diseases in Children and Adults at Risk: Possible Scenarios in Campania Region. Infect. Disord. Drug. Targets 2019, 19, 403–408. [Google Scholar] [CrossRef]
- National Law N. 386/1974, National Official Bulletin “GU Serie Generale n.225 del 29-08-1974 art. N. 9. 1974. Available online: https://www.gazzettaufficiale.it/eli/id/1974/08/29/074U0386/sg (accessed on 17 March 2023).
- Ministero della Salute. Nomenclatore Dell’assistenza Specialistica Ambulatoriale. Available online: https://www.salute.gov.it/portale/temi/p2_6.jsp?lingua=italiano&id=1767&area=programmazioneSanitariaLea&menu=lea (accessed on 17 March 2023).
- Ansaldi, F.; Pugh, S.; Amicizia, D.; Di Virgilio, R.; Trucchi, C.; Orsi, A.; Zollo, A.; Icardi, G. Estimating the Clinical and Economic Impact of Switching from the 13-Valent Pneumococcal Conjugate Vaccine (PCV13) to the 10-Valent Pneumococcal Conjugate Vaccine (PCV10) in Italy. Pathogens 2020, 9, 76. [Google Scholar] [CrossRef] [Green Version]
- Astengo, M.; Paganino, C.; Amicizia, D.; Trucchi, C.; Tassinari, F.; Sticchi, C.; Sticchi, L.; Orsi, A.; Icardi, G.; Piazza, M.F.; et al. Economic Burden of Pneumococcal Disease in Individuals Aged 15 Years and Older in the Liguria Region of Italy. Vaccines 2021, 9, 1380. [Google Scholar] [CrossRef]
- Mennini, F.S.; Marcellusi, A.; Giannantoni, P.; Valente, S.; Rinaldi, A.; Franco, E. Budget impact of pneumococcal vaccination in adults and elderly in Italy. Glob. Reg. Health Technol. Assess. 2015, 2, 43–52. [Google Scholar] [CrossRef]
- Delgleize, E.; Leeuwenkamp, O.; Theodorou, E.; Van de Velde, N. Cost-effectiveness analysis of routine pneumococcal vaccination in the UK: A comparison of the PHiD-CV vaccine and the PCV-13 vaccine using a Markov model. BMJ Open 2016, 6, e010776. [Google Scholar] [CrossRef]
- Fattore, G. Proposta di linee guida per la valutazione economica degli interventi sanitari in Italia. Pharmacoeconomics 2013, 11, 83–93. [Google Scholar] [CrossRef]
- Mangen, M.J.; Rozenbaum, M.H.; Huijts, S.M.; van Werkhoven, C.H.; Postma, D.F.; Atwood, M.; van Deursen, A.M.; van der Ende, A.; Grobbee, D.E.; Sanders, E.A.; et al. Cost-effectiveness of adult pneumococcal conjugate vaccination in the Netherlands. Eur. Respir. J. 2015, 46, 1407–1416. [Google Scholar] [CrossRef] [Green Version]
- Hoshi, S.-l.; Kondo, M.; Okubo, I. Economic Evaluation of Immunisation Programme of 23-Valent Pneumococcal Polysaccharide Vaccine and the Inclusion of 13-Valent Pneumococcal Conjugate Vaccine in the List for Single-Dose Subsidy to the Elderly in Japan. PLoS ONE 2015, 10, e0139140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiri, T.; Khan, K.; Keaney, K.; Mukherjee, G.; McCarthy, N.D.; Petrou, S. Pneumococcal Disease: A Systematic Review of Health Utilities, Resource Use, Costs, and Economic Evaluations of Interventions. Value Health 2019, 22, 1329–1344. [Google Scholar] [CrossRef] [PubMed]
- Leidner, A.J. Summary of Three Economic Models Assessing Pneumococcal Vaccines in US Adults; Centers for Disease Control and Prevention, 2021. Available online: https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-09-29/02-Pneumococcal-Leidner-508.pdf (accessed on 17 March 2023).
- Cripps, A.W.; Folaranmi, T.; Johnson, K.D.; Musey, L.; Niederman, M.S.; Buchwald, U.K. Immunogenicity following revaccination or sequential vaccination with 23-valent pneumococcal polysaccharide vaccine (PPSV23) in older adults and those at increased risk of pneumococcal disease: A review of the literature. Expert. Rev. Vaccines 2021, 20, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Ministero della Salute. Vaccinazioni dell'età Pediatrica e dell’adolescenza—Coperture Vaccinali. Available online: https://www.salute.gov.it/portale/documentazione/p6_2_8_3_1.jsp?lingua=italiano&id=20 (accessed on 17 March 2023).
- Sisk, J.E.; Whang, W.; Butler, J.C.; Sneller, V.P.; Whitney, C.G. Cost-effectiveness of vaccination against invasive pneumo-coccal disease among people 50 through 64 years of age: Role of comorbid conditions and race. Ann. Intern. Med. 2003, 138, 960–968. [Google Scholar] [CrossRef]
- des Portes, V. Quel suivi à long terme pour quels patients? Séquelles des méningites bactériennes chez l’enfant et chez l’adulte: Incidence, types, modes d’évaluation. Med. Mal. Infect. 2009, 39, 572–580. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Serotype | PCVs 1 | PPSV23 | |||
|---|---|---|---|---|---|
| IPD 2,3 | NBPP 4 | Serotype | IPD 5 | NBPP 6 | |
| ST 3 | 26% | 23% | All STs | 73% | 33.5% |
| All STs but 3 | 75% | 45% | |||
| NVT bucket | 0% | 0% | NVT bucket | 0% | 0% |
| Serotype | PCVs | PPSV23 |
|---|---|---|
| %AMR in IPD and NBPP 1 | ||
| ST 3 | 24% | |
| ST 11A | 2% | |
| ST 19A | 76% | |
| ST 19F | 14% | |
| ST 22F | 2% | |
| All other STs | 0% | |
| NVT bucket | Varying depending on the baseline serotype distribution | |
| Vaccine Strategy | Acquisition Cost Per Dose | Administration Cost Per Dose | Reference |
|---|---|---|---|
| Any single PCV | €44.63 | €6.80 | Awarded tenders in Italy and OsMed cost per DDD data GPs’ single vaccine administration tariff system [33] |
| PPSV23 single | €19.13 | ||
| PCV + PPSV23 | €63.76 | €13.60 | Sum of PCV and PPSV23 prices |
| Costs Per Case in Euros 1 (€) | ||
|---|---|---|
| Category | Medical Costs 2,3 | Indirect Costs 4,5 |
| IPD | €8395 | €433.30 |
| NBPP (inpatient) | €4463 | €826.47 |
| NBPP (outpatient) | €333 | €417.25 |
| Meningitis | €9227 | €1460.37 |
| PMS (first and consecutive years) | €94 | Not applicable |
| 18–29 years old | Not applicable | €1604.80 |
| 30–49 years old | €1838.40 | |
| 50+ years old | €2009.60 | |
| AMR in IPD | €2518.50 | €129.99 |
| AMR in NBPP | €1338.90 | €247.94 |
| No. of Events |
Low-Risk Age 65 (n = 387,993) |
At-Risk Ages 50–100 (n = 10,255,405) |
High-Risk Ages 18–100 (n = 4,552,553) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PCV15 + PPSV23 | PCV20 + PPSV23 | PCV13 + PPSV23 | PCV20 (Single) | No Vaccination | PCV15 + PPSV23 | PCV20 + PPSV23 | PCV13 + PPSV23 | PCV20 (Single) | No Vaccination | PCV15 + PPSV23 | PCV13 + PPSV23 | No Vaccination | |
| IPD cases | 201 | 195 | 203 | 199 | 225 | 47,841 | 47,010 | 48,004 | 47,354 | 49,871 | 41,867 | 42,046 | 44,154 |
| Meningitis cases | 40 | 39 | 41 | 40 | 45 | 9568 | 9402 | 9601 | 9471 | 9974 | 8373 | 8409 | 8831 |
| NBPP inpatient cases | 6252 | 6137 | 6285 | 6212 | 6522 | 1,018,625 | 1,007,015 | 1,020,915 | 1,011,016 | 1,040,928 | 843,429 | 846,735 | 878,903 |
| NBPP outpatient cases | 2265 | 2231 | 2275 | 2257 | 2337 | 1,013,362 | 1,003,586 | 1,015,291 | 1,007,500 | 1,031,464 | 1,451,278 | 1,455,284 | 1,490,351 |
| PMS cases | 28 | 27 | 28 | 28 | 32 | 6698 | 6581 | 6721 | 6630 | 6982 | 5861 | 5886 | 6181 |
| AMR cases | 590 | 590 | 591 | 597 | 631 | 128,966 | 129,035 | 129,430 | 133,533 | 128,966 | 143,690 | 143,811 | 151,852 |
| PD deaths a | 742 | 14 | 744 | 740 | 763 | 208,914 | 206,919 | 209,308 | 207,745 | 212,638 | 224,507 | 225,077 | 229,932 |
| Total Costs |
Low-Risk Age 65 (n = 387,993) |
At-Risk Ages 50–100 (n = 10,255,405) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| PCV15 + PPSV23 | PCV20 + PPSV23 | PCV13 + PPSV23 | PCV20 (Single) | No Vaccination | PCV15 + PPSV23 | PCV20 + PPSV23 | PCV13 + PPSV23 | PCV20 (Single) | No Vaccination | |
| Acquisition | €15,708,857 | €15,708,857 | €15,708,857 | €11,255,476 | €0 | €153,661,857 | €153,661,857 | €153,661,857 | €114,424,678 | €0 |
| Admin | €3,297,939 | €3,297,939 | €3,297,939 | €1,714,928 | €0 | €31,381,538 | €31,381,538 | €31,381,538 | €17,434,188 | €0 |
| IPD | €1,191,165 | €1,148,479 | €1,204,274 | €1,177,956 | €1,364,516 | €290,093,224 | €284,285,798 | €291,229,861 | €286,441,134 | €305,094,047 |
| Meningitis | €294,692 | €284,132 | €297,936 | €291,425 | €337,579 | €71,768,640 | €70,331,891 | €72,049,842 | €70,865,118 | €75,479,821 |
| NBPP inpatient | €7,114,763 | €6,988,619 | €7,151,113 | €7,072,914 | €7,410,795 | €3,410,395,384 | €3,368,930,653 | €3,418,569,460 | €3,382,338,422 | €3,491,474,514 |
| NBPP outpatient | €3,263,961 | €3,194,326 | €3,284,163 | €3,234,499 | €3,441,777 | €572,977,610 | €565,102,575 | €574,529,698 | €572,977,610 | €588,752,990 |
| PMS | €618,706 | €594,093 | €626,344 | €610,328 | €726,565 | €164,259,512 | €160,789,407 | €164,938,481 | €162,029,684 | €173,360,343 |
| AMR | €914,930 | €914,504 | €915,912 | €925,804 | €981,449 | €200,985,595 | €200,959,918 | €201,073,996 | €201,679,448 | €208,402,985 |
| Total Costs |
High-Risk Ages 18–100 (n = 4,552,553) | ||
|---|---|---|---|
| PCV15 + PPSV23 | PCV13 + PPSV23 | No Vaccination | |
| Acquisition | €140,822,386 | €140,822,386 | €0 |
| Admin | €29,418,165 | €29,418,165 | €0 |
| IPD | €195,237,793 | €196,364,290 | €211,730,448 |
| Meningitis | €48,237,798 | €48,515,923 | €52,308,220 |
| NBPP inpatient | €423,097,802 | €425,219,605 | €447,293,205 |
| NBPP outpatient | €3,910,848,526 | €3,926,584,461 | €4,081,797,384 |
| PMS | €243,720,914 | €244,535,830 | €260,648,727 |
| AMR | €124,297,937 | €125,053,666 | €135,573,387 |
|
PCV15 + PPSV23 vs. |
Low-Risk Age 65 (n = 387,993) |
At-Risk Ages 50–100 (n = 10,255,405) |
High-Risk Ages 18–100 (n = 4,552,553) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| PCV13 + PPSV23 | PCV20 + PPSV23 | PCV20 (Single) | No Vaccination | PCV13 + PPSV23 | PCV20 + PPSV23 | PCV20 (Single) | No Vaccination | PCV13 + PPSV23 | No Vaccination | |
| Incremental costs | −€78,281 | €263,505 | €6,118,416 | €18,185,218 | −€11,630,171 | €58,642,975 | €92,033,528 | €56,669,841 | −€19,967,763 | −€65,752,706 |
| Incremental QALYs | 17 | −58 | −23 | 168 | 1488 | −7559 | −5255 | 15,718 | 2778 | 31,811 |
| Incremental LYs | 35 | −119 | −43 | 325 | 4414 | −22,401 | −14,493 | 44,783 | 9279 | 98,142 |
| ICUR | PCV15 + PPSV23 Dominant over PCV13 + PPSV23 | PCV15 + PPSV23 Dominated by PCV20 + PPSV23 | PCV15 + PPSV23 Dominated by PCV20 | €108,542 | PCV15 + PPSV23 Dominant over PCV13 + PPSV23 | PCV15 + PPSV23 Dominated by PCV20 + PPSV23 | PCV15 + PPSV23 Dominated by PCV20 | €3605 | PCV15 + PPSV23 Dominant over PCV13 + PPSV23 | PCV15 + PPSV23 Dominant over No Vaccination |
|
PCV15 + PPSV23 vs. |
Low-Risk Age 65 |
At-Risk Ages 50–100 |
High-Risk Ages 18–100 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| PCV13 + PPSV23 | PCV20 + PPSV23 | PCV20 (Single) | No Vaccination | PCV13 + PPSV23 | PCV20 + PPSV23 | PCV20 (Single) | No Vaccination | PCV13 + PPSV23 | No Vaccination | |
| OPA GMT ratios only | ||||||||||
| Incremental costs | −€171,374 | −€40,640 | €5,842,648 | €18,092,125 | −€25,444,719 | €9,005,298 | €45,138,016 | €42,855,293 | −€98,877,804 | −€144,662,747 |
| Incremental QALYs | 34 | 4 | 33 | 185 | 3046 | −1506 | 492 | 17,276 | 13,308 | 42,340 |
| Incremental LYs | 69 | 4 | 67 | 359 | 8909 | −4920 | 1835 | 49,278 | 42,645 | 131,507 |
| ICUR | Dominant | Dominant | €175,909 | €98,009 | Dominant | Dominated | €91,825 | €2481 | Dominant | Dominant |
| OPA GMT ratios + price discount | ||||||||||
| Incremental costs | −€734,148 | -€603,414 | €5,279,874 | €17,529,351 | −€31,165,953 | €3,284,065 | €39,416,782 | €37,134,059 | −€103,958,813 | −€149,743,756 |
| Incremental QALYs | 34 | 4 | 33 | 185 | 3046 | −1506 | 492 | 17,276 | 13,308 | 42,340 |
| Incremental LYs | 69 | 4 | 67 | 359 | 8909 | −4920 | 1835 | 49,278 | 42,645 | 131,507 |
| ICUR | Dominant | Dominant | €158,966 | €94,960 | Dominant | Dominated | €80,186 | €2150 | Dominant | Dominant |
| OPA GMT ratios + increased VCRs | ||||||||||
| Incremental costs | −€197,424 | −€49,374 | €6,814,461 | €20,948,474 | −€97,905,094 | €10,292,467 | €181,922,875 | €172,791,981 | −€207,119,789 | −€310,331,707 |
| Incremental QALYs | 39 | 5 | 39 | 214 | 11,641 | −2662 | 6827 | 73,963 | 27,868 | 2,759,229 |
| Incremental LYs | 79 | 5 | 80 | 416 | 34,330 | −10,662 | 21,428 | 211,200 | 89,655 | 282,173 |
| ICUR | Dominant | Dominant | €173,638 | €97,928 | Dominant | Dominated | €26,647 | €2336 | Dominant | Dominant |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Restivo, V.; Baldo, V.; Sticchi, L.; Senese, F.; Prandi, G.M.; Pronk, L.; Owusu-Edusei, K.; Johnson, K.D.; Ignacio, T. Cost-Effectiveness of Pneumococcal Vaccination in Adults in Italy: Comparing New Alternatives and Exploring the Role of GMT Ratios in Informing Vaccine Effectiveness. Vaccines 2023, 11, 1253. https://doi.org/10.3390/vaccines11071253
Restivo V, Baldo V, Sticchi L, Senese F, Prandi GM, Pronk L, Owusu-Edusei K, Johnson KD, Ignacio T. Cost-Effectiveness of Pneumococcal Vaccination in Adults in Italy: Comparing New Alternatives and Exploring the Role of GMT Ratios in Informing Vaccine Effectiveness. Vaccines. 2023; 11(7):1253. https://doi.org/10.3390/vaccines11071253
Chicago/Turabian StyleRestivo, Vincenzo, Vincenzo Baldo, Laura Sticchi, Francesca Senese, Gian Marco Prandi, Linde Pronk, Kwame Owusu-Edusei, Kelly D. Johnson, and Tim Ignacio. 2023. "Cost-Effectiveness of Pneumococcal Vaccination in Adults in Italy: Comparing New Alternatives and Exploring the Role of GMT Ratios in Informing Vaccine Effectiveness" Vaccines 11, no. 7: 1253. https://doi.org/10.3390/vaccines11071253