
The Effect of University Students’ Levels of Knowledge about HPV Infection and the HPV Vaccine on Their Health Beliefs: Health Sciences Students


Abstract
:1. Introduction
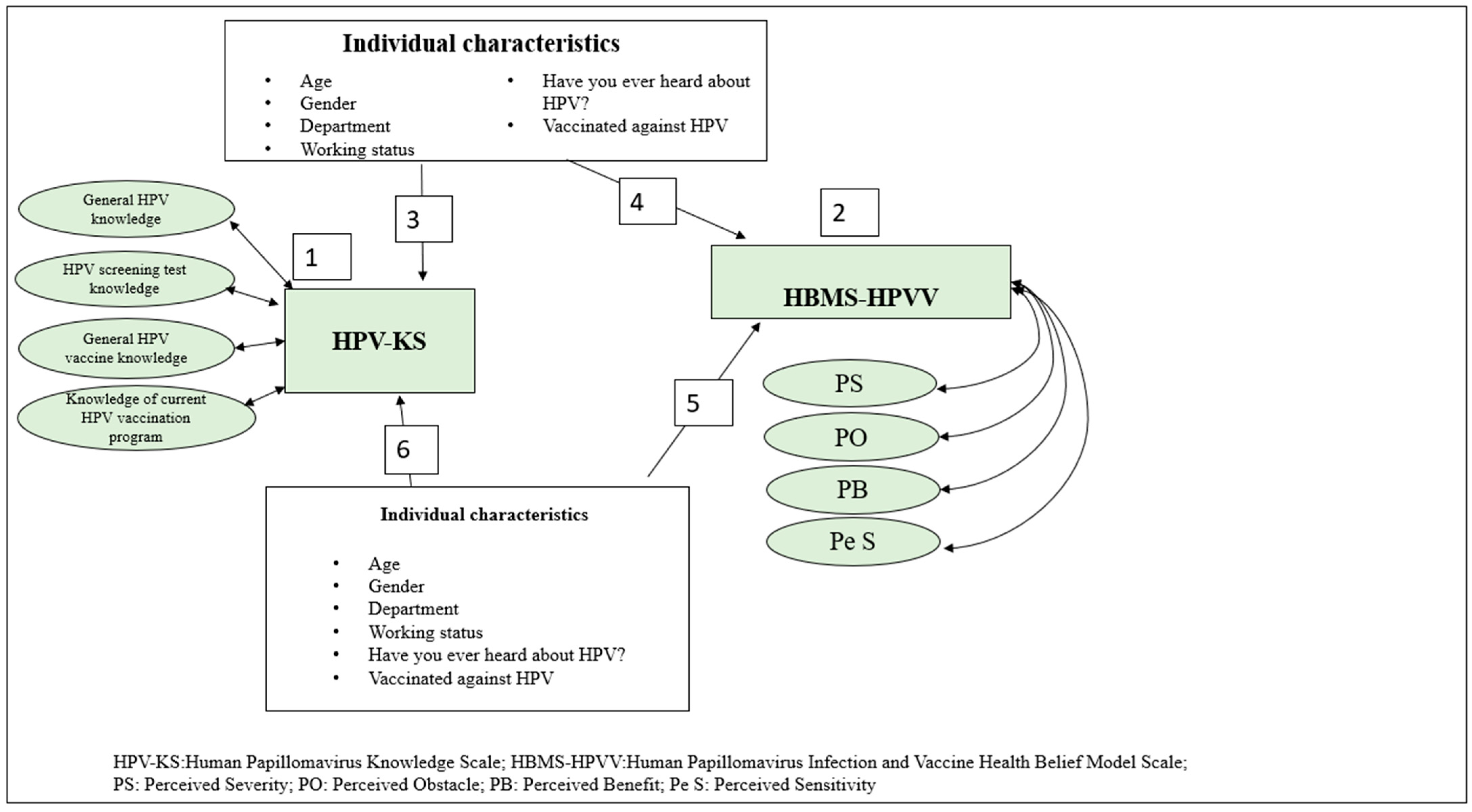
- What are the students’ levels of knowledge about HPV infection and the vaccine?
- What are the students’ health beliefs regarding HPV infection and the vaccine?
- What individual characteristics of the students create a significant difference in their levels of knowledge of HPV infection and the vaccine?
- What individual characteristics of the students create a significant difference in their health beliefs regarding HPV infection and the vaccine?
- Does at least one of the students’ characteristics predict their health belief regarding HPV infection and the vaccine?
- Does at least one of the students’ characteristics predict their level of knowledge about HPV infection and the vaccine? (Figure 1).
2. Methods
2.1. Study Design and Sample
2.2. Measures
2.3. Statistical Analysis
2.4. Ethics
3. Results
3.1. Sociodemographic Characteristics
3.2. Comparison of Health Beliefs about HPV Infection/Vaccination and HPV Knowledge Levels according to Sociodemographic Characteristics
3.3. Health Beliefs of Students Regarding HPV Infection/Vaccination and HPV Knowledge Levels
3.4. Multiple Linear Regression Analysis of Factors Influencing Students’ Health Beliefs about HPV Infection/Vaccination
3.5. Results of Multiple Linear Regression Analysis for the Factors Affecting Students’ HPV Knowledge Levels
4. Discussion
4.1. Comparison of Health Beliefs about HPV Infection/Vaccination and HPV Knowledge Levels according to Sociodemographic Characteristics
4.2. Health Beliefs of Students Regarding HPV Infection/Vaccination and HPV Knowledge Levels
4.3. Multiple Linear Regression Analysis of Factors Influencing Students’ Health Beliefs about HPV Infection/Vaccination and HPV Knowledge Levels
4.4. Limitations of the Study
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Human Papillomavirus Vaccines: WHO Position Paper, May 2017. Wkly. Epidemiol. Rec. 2017, 19, 241–268. Available online: https://www.who.int/publications/i/item/who-wer9219-241-268 (accessed on 14 June 2022).
- Meites, E.; Gee, J.; Unger, E.; Markowitz, L. Human Popillomavirus. In Epidemiology and Prevention of Vaccine-Preventable Diseases, 14th ed.; Hall, E., Wodi, A.P., Hamborsky, J., Morelli, V., Schillie, S., Eds.; Centers for Disease Control and Prevention; Public Health Foundation: Washington, DC, USA, 2021; pp. 165–178. Available online: https://www.cdc.gov/vaccines/pubs/pinkbook/downloads/hpv.pdf (accessed on 15 August 2022).
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Collado, J.J.; Gómez, D.; Muñoz, J.; Bosch, F.X.; de Sanjosé, S. Human Papillomavirus and Related Diseases in Turkey; Summary Report; ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre): Barcelona, Spain, 10 March 2023; Available online: https://hpvcentre.net/statistics/reports/TUR.pdf (accessed on 14 March 2023).
- World Health Organization. Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/initiatives/cervical-cancer-elimination-initiative#cms (accessed on 2 June 2023).
- Bora Başara, B.; Aygün, A.; Soytutan Çağlar, İ.; Kulali, B. Health Statistics Yearbook 2020 Newsletter; General Directorate of Health Information Systems; Ministry of Health: Ankara, Turkey, 2021. Available online: https://sbsgm.saglik.gov.tr/Eklenti/41611/0/haber-bulteni-2020pdf.pdf (accessed on 15 August 2022).
- Senkomago, V.; Duran, D.; Loharikar, A.; Hyde, T.B.; Markowitz, L.E.; Unger, E.R.; Saraiya, M. CDC Activities for Improving Implementation of Human Papillomavirus Vaccination, Cervical Cancer Screening, and Surveillance Worldwide. Emerg. Infect. Dis. 2017, 23, S101–S107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Immunization Coverage. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 14 March 2023).
- Vaidakis, D.; Moustaki, I.; Zervas, I.; Barbouni, A.; Merakou, K.; Chrysi, M.S.; Creatsa, G.; Panoskaltsis, T. Knowledge of Greek adolescents on Human Papilloma Virus (HPV) and vaccination: A national epidemiologic study. Medicine 2017, 96, e5287. [Google Scholar] [CrossRef] [Green Version]
- Akalın, A. Human Papillomavirus (HPV) Infection and current approaches to HPV vaccine. Androl Bul. 2021, 24, 133–139. [Google Scholar] [CrossRef]
- Markowitz, L.E.; Dunne, E.F.; Saraiya, M.; Chesson, H.W.; Curtis, C.R.; Gee, J.; Bocchini, J.A., Jr.; Unger, E.R. Human Papillomavirus vaccination: Recommendations of the Advisory Committee on Immunization Practices (ACIP). Morb. Mortal. Wkly. Rep. 2014, 63, 1–30. [Google Scholar]
- Petrosky, E.; Bocchini, J.A., Jr.; Hariri, S.; Chesson, H.; Curtis, C.R.; Saraiya, M.; Unger, E.R.; Markowitz, L.E.; Centers for Disease Control and Prevention (CDC). Use of 9-valent human papillomavirus (HPV) vaccine: Updated HPV vaccination recommendations of the advisory committee on immunization practices. Morb. Mortal. Wkly. Rep. 2015, 64, 300–304. [Google Scholar]
- Fontenot, H.B.; Collins Fantasia, H.; Charyk, A.; Sutherland, M.A. Human papillomavirus (hpv) risk factors, vaccination patterns, and vaccine perceptions among a sample of male college students. J. Am. Coll. Health 2014, 62, 186–192. [Google Scholar] [CrossRef]
- Cheung, T.; Lau, J.T.F.; Wang, J.Z.; Mo, P.K.H.; Ho, Y.S. Acceptability of HPV vaccines and associations with perceptions related to HPV and HPV vaccines among male baccalaureate students in Hong Kong. PLoS ONE 2018, 13, e0198615. [Google Scholar] [CrossRef] [Green Version]
- Duval, B.; Gilca, V.; Boulianne, N.V.; Pielak, K.; Halperin, B.; Simpson, M.A.; Sauvageau, C.; Ouakki, M.; Dube, E.; Lavoie, F. Cervical cancer prevention by vaccination: Nurses’ knowledge, attitudes and intentions. J. Adv. Nurs. 2009, 65, 499–508. [Google Scholar] [CrossRef]
- Altıntaş, R.Y.; Erciyas, Ş.K.; Ertem, G. Determination of health belief levels of faculty of health sciences students regarding cervical cancer and human papilloma virus ınfection vaccination. E-J. Dokuz Eylul Univ. Nurs. Fac. 2022, 15, 40–49. [Google Scholar] [CrossRef]
- Khatiwada, M.; Kartasasmita, C.; Mediani, H.S.; Delprat, C.; Van Hal, G.; Dochez, C. Knowledge, attitude and acceptability of the human papilloma virus vaccine and vaccination among university students in Indonesia. Front. Public Health 2021, 9, 616456. [Google Scholar] [CrossRef] [PubMed]
- Güvenç, G.; Seven, M.; Akyüz, A. Health belief model scale for human papilloma virus and its vaccination: Adaptation and psychometric testing. J. Pediatr. Adolesc. Gynecol. 2016, 29, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Demir, F. Validity and Reliability of the Turkish Version of Human Papilloma Virus Knowledge Scale. Master’s Thesis, University of Health Sciences, Ankara, Turkey, 2019. Available online: https://tez.yok.gov.tr/UlusalTezMerkezi/tezDetay.jsp?id=PbXEf_W5BPYbJWlM7wlVgQ&no=3YBI6ZjejEkzQxqlVU-UQw (accessed on 18 August 2022).
- Çınar, İ.O.; Ozkan, S.; Aslan, G.K.; Alatas, E. Knowledge and behavior of university students toward human papillomavirus and vaccination. Asia Pac. J. Oncol. Nurs. 2019, 6, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Seo, J.W.; Ryu, E. Korean college students’ attitudes and health behaviour regarding human papillomavirus vaccination. Collegian 2021, 28, 57–62. [Google Scholar] [CrossRef]
- Du, E.Y.; Adjei Boakye, E.; Taylor, D.B.; Kuziez, D.; Rohde, R.L.; Pannu, J.S.; Simpson, M.C.; Patterson, R.H.; Varvares, M.A.; Osazuwa-Peters, N. Medical students’ knowledge of HPV, HPV vaccine, and HPV-associated head and neck cancer. Hum. Vaccines Immunother. 2022, 7, 2109892. [Google Scholar] [CrossRef]
- Galvão, M.P.S.P.; Araújo, T.M.E.; Rocha, S.S. Knowledge, attitudes, and practices of adolescents regarding human papillomavirus. Rev. Saude Publica 2022, 56, 12. [Google Scholar] [CrossRef]
- Serrano, B.; Brotons, M.; Bosch, F.X.; Bruni, L. Epidemiology and burden of HPV-related disease. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 47, 14–26. [Google Scholar] [CrossRef]
- Suhaila, K.; Mukherjee, A.; Maharjan, B.; Dhakal, A.; Lama, M.; Junkins, A.; Khakurel, U.; Jha, A.N.; Jolly, P.E.; Lhaki, P.; et al. Human papillomavirus, related diseases, and vaccination: Knowledge and awareness among health care students and professionals in Nepal. J. Cancer Educ. 2021, 37, 1727–1735. [Google Scholar] [CrossRef]
- Ramesh, P.S.; Krishnamurthy, S.; Shrestha, S.; Nataraj, S.M.; Devegowda, D. Knowledge, awareness and prevalence of human papillomavirus among local university students and healthcare workers in South India: A cross-sectional study. Clin. Epidemiol. Glob. Health 2021, 12, 100839. [Google Scholar] [CrossRef]
- Ersin, F.; Kıssal, A.; Polat, P.; Koca, B.D.; Erdoğan, M. Perception of female medical personnel toward cervical cancer and the affecting factors. J. Res. Dev. Nurs. 2016, 18, 31–43. Available online: http://hemarge.org.tr/ckfinder/userfiles/files/2016/vol18num2-3/4%20(1).pdf (accessed on 14 August 2022).
- Barnard, M.; George, P.; Perryman, M.L.; Wolff, L.A. Human papillomavirus (HPV) vaccine knowledge, attitudes, and uptake in college students: Implications from the precaution adoption process model. PLoS ONE 2017, 12, e0182266. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.T.; Simms, K.T.; Lew, J.B.; Smith, M.A.; Brotherton, J.M.; Saville, M.; Frazer, I.H.; Canfell, K. The projected timeframe until cervical cancer elimination in australia: A modelling study. Lancet Public Health 2019, 4, e19–e27. [Google Scholar] [CrossRef] [Green Version]
- Arbyn, M.; Xu, L.; Simoens, C.; Martin-Hirsch, P.P. Prophylactic vaccination against human papillomaviruses to prevent cervical cancer and its precursors. Cochrane Database Syst. Rev. 2018, 5, CD009069. [Google Scholar] [CrossRef]
- Paraskevaidis, E.; Athanasiou, A.; Paraskevaidi, M.; Bilirakis, E.; Galazios, G.; Kontomanolis, E.; Dinas, K.; Loufopoulos, A.; Nasioutziki, M.; Kalogiannidis, I.; et al. Cervical Pathology Following HPV Vaccination in Greece: A 10-year HeCPA Observational Cohort Study. In Vivo 2020, 34, 1445–1449. [Google Scholar] [CrossRef] [PubMed]
- Szarewski, A.; Poppe, W.A.; Skinner, S.R.; Wheeler, C.M.; Paavonen, J.; Naud, P.; Salmeron, J.; Chow, S.N.; Apter, D.; Kitchener, H.; et al. Efficacy of the human papillomavirus (HPV)-16/18 as04-adjuvanted vaccine in women aged 15–25 years with and without serological evidence of previous exposure to HPV-16/18. Int. J. Cancer 2012, 131, 106–116. [Google Scholar] [CrossRef]
- D’Errico, M.P.; Tung, W.C.; Lu, M.; D’Errico, R. Knowledge, attitudes, and practices related to human papillomavirus vaccination among college students in a state university: Implications for nurse practitioners. J. Am. Assoc. Nurse Pract. 2020, 33, 709–718. [Google Scholar] [CrossRef]
- Park, A.S. The influence of cervical cancer, HPV knowledge and health beliefs on HPV vaccination among undergraduate students. J. Korea Acad.-Ind. Coop. Soc. 2015, 16, 7708–7717. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.W. Knowledge about human papillomavirus (HPV) and health beliefs and intention to recommend HPV vaccination for girls and boys among Korean health teachers. Vaccine 2012, 30, 5327–5334. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Bi, W.; Liu, T.; Jiang, Y.; Wang, Q.; Fan, R. Factors associated with intention of human papillomavirus vaccination among Chinese college students: İmplications for health promotion. Hum. Vaccines Immunother. 2021, 17, 5426–5432. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | N | % | HBMS-HPVV | HPV-KS | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Perceived Severity Mean ± SD | Perceived Obstacle Mean ± SD | Perceived Benefit Mean ± SD | Perceived Sensitivity Mean ± SD | General HPV Knowledge Mean ± SD | HPV Screening Test Knowledge Mean ± SD | General HPV Vaccine Knowledge Mean ± SD | Knowledge of Current HPV Vaccination Program Mean ± SD | |||
| Mean age (yrs) | 20.92 ± 1.60 | |||||||||
| Gender | ||||||||||
| Female | 677 | 82.2 | 2.52 ± 0.85 | 1.87 ± 0.59 | 2.72 ± 0.90 | 2.35 ± 0.81 | 7.50 ± 4.05 | 1.66 ± 1.55 | 2.27 ± 1.69 | 1.36 ± 1.39 |
| Male | 147 | 17.8 | 2.38 ± 0.83 | 1.93 ± 0.71 | 2.42 ± 0.84 | 2.33 ± 0.83 | 5.72 ± 3.89 | 1.06 ± 1.19 | 1.34 ± 1.39 | 1.07 ± 1.36 |
| t = 1.924; p = 0.055 | t = −1.119; p = 0.263 | t = 3.633; p = 0.000 ** | t = 0.228; p = 0.820 | t = 4.865; p =0.000 ** | t = 4.351; p = 0.000 * | t = 6.225; p = 0.000 ** | t = 2.134; p = 0.021 * | |||
| Department | ||||||||||
| Nursing | 450 | 54.6 | 2.43 ± 0.85 | 1.92 ± 0.68 | 2.57 ± 0.87 | 2.34 ± 0.84 | 6.62 ± 3.80 | 1.29 ± 1.32 | 1.77 ± 1.50 | 1.16 ± 1.31 |
| Midwifery | 267 | 32.4 | 2.77 ± 0.73 | 1.88 ± 0.47 | 3.05 ± 0.76 | 2.44 ± 0.70 | 9.50 ± 3.21 | 2.26 ± 1.71 | 3.08 ± 1.60 | 1.79 ± 1.48 |
| Physical Therapy and Rehabilitation | 107 | 13.0 | 2.11 ± 0.92 | 1.72 ± 0.62 | 2.11 ± 0.90 | 2.13 ± 0.94 | 3.79 ± 3.99 | 0.87 ± 0.96 | 1.03 ± 1.35 | 0.76 ± 1.12 |
| F = 27.260; p = 0.000 **, c < a,b * | F = 4.290; p = 0.014 *, c < a * | F = 54.023; p = 0.000 **, c < a,b * | F = 5.600; p = 0.004 *, c < a,b * | F = 105.458; p = 0.000 **, c < a,b * | F = 52.343; p = 0.000 **, c < a,b * | F = 93.464; p = 0.000 **, c < a,b * | F = 2.492; p = 0.000 **, c < a,b * | |||
| Working status | ||||||||||
| Yes | 77 | 9.3 | 2.44 ± 0.89 | 1.97 ± 0.75 | 2.50 ± 1.02 | 2.37 ± 0.93 | 7.22 ± 4.08 | 1.66 ± 1.72 | 2.22 ± 1.72 | 0.94 ± 1.27 |
| No | 747 | 90.7 | 2.50 ± 0.84 | 1.87 ± 0.60 | 2.68 ± 0.88 | 2.34 ± 0.80 | 7.18 ± 4.08 | 1.54 ± 148 | 2.09 ± 1.67 | 1.35 ± 1.40 |
| t = −0.668; p = 0.504 | t = 1.257; p = 0.209 | t = −1.732; p = 0.084 | t = 0.217; p = 0.828 | t = 0.076; p = 0.939 | t = 0.656; p = 0.512 | t = 0.639; p = 0.523 | t = −2.435; p = 0.015 * | |||
| Have you ever heard about HPV? | ||||||||||
| Yes | 590 | 71.6 | 2.76 ± 0.69 | 1.97 ± 0.56 | 2.97 ± 0.70 | 2.53 ± 0.71 | 8.89 ± 3.04 | 1.91 ± 1.54 | 2.62 ± 1.60 | 1.60 ± 1.42 |
| No | 234 | 28.4 | 1.83 ± 0.84 | 1.67 ± 0.69 | 1.89 ± 0.85 | 1.87 ± 0.87 | 2.87 ± 3.07 | 0.63 ± 0.92 | 0.80 ± 1.02 | 0.80 ± 1.02 |
| t = 16.245; p = 0.000 * | t = 6.421; p = 0.000 ** | t = 18.568; p = 0.000 ** | t = 11.264; p = 0.000 ** | t =25.574; p = 0.000 * | t = 11.870; p = 0.000 ** | t = 16.037; p = 0.000 ** | t = 9.883; p = 0.000 ** | |||
| Vaccinated against HPV | ||||||||||
| Yes | 57 | 6.9 | 2.75 ± 0.73 | 1.82 ± 0.51 | 2.89 ± 0.65 | 2.63 ± 0.74 | 8.29 ± 2.58 | 1.85 ± 1.43 | 2.24 ± 1.58 | 2.05 ± 1.48 |
| No | 767 | 93.1 | 2.48 ± 0.85 | 1.89 ± 0.62 | 2.65 ± 0.91 | 2.32 ± 0.82 | 7.10 ± 4.16 | 1.53 ± 1.51 | 2.09 ± 1.68 | 1.26 ± 1.37 |
| t = 2.352; p = 0.019 * | t = −0.786; p = 0.432 | t = 1.955; p = 0.051 | t = 2.685; p = 0.007 * | t = 29.015; p = 0.000 * | t = 1.034; p = 0.310 | t = 1.433; p = 0.232 | t = 0.169; p = 0.681 | |||
| Marital status | ||||||||||
| Single | 824 | 100.0 | ||||||||
| Variable | Subscales | Mean ± SD | Min–Max | Items | Skewness | Kurtosis |
|---|---|---|---|---|---|---|
| HPV-KS | General HPV knowledge | 7.88 ± 4.08 | 0–15 | 16 | −0.306 | −1.209 |
| HPV screening test knowledge | 1.55 ± 1.51 | 0–6 | 6 | 0.846 | −0.141 | |
| General HPV vaccine knowledge | 2.10 ± 1.67 | 0–5 | 5 | 0.204 | −1.273 | |
| Knowledge of current HPV vaccination program | 1.31 ± 1.39 | 0–6 | 6 | 0.816 | −0.0400 | |
| Total score | 12.16 ± 7.21 | 0–27 | 33 | −0.045 | −1.134 | |
| HBMS-HPVV | Perceived severity | 2.50 ± 0.85 | 1–4 | 4 | −0.264 | −0.698 |
| Perceived obstacle | 1.88 ± 0.62 | 1–4 | 5 | 0.513 | 0.329 | |
| Perceived benefit | 2.67 ± 0.89 | 1–4 | 3 | −0.381 | −0.677 | |
| Perceived sensitivity | 2.35 ± 0.82 | 1–4 | 2 | 0.072 | −0.553 | |
| Total score | 32.16 ± 8.91 | 14–56 | 14 | −0.551 | 0.108 |
| Unstandardized Coefficients | Standardized Coefficients | 95% CI | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Model | B | SD | β | t | p | Lower | Upper | R2 |
| Perceived severity | Constant | 0.322 | 0.37 | 0.860 | 0.390 | −0.413 | 1.058 | 0.26 | |
| Age | 0.069 | 0.01 | 0.12 | 3.980 | 0.000 * | 0.035 | 0.103 | ||
| Cinsiyet (reference: boy) | −0.011 | 0.07 | −0.00 | −0.155 | 0.877 | −0.152 | 0.129 | ||
| Department (reference: Physiotherapy and Rehabilitation) | |||||||||
| Nurse | 0.036 | 0.82 | 0.02 | 0.444 | 0.657 | −0.124 | 0.197 | ||
| Midwifery | 0.205 | 0.09 | 0.11 | 2.243 | 0.025 * | 0.026 | 0.384 | ||
| Working status (reference: no) | 0.094 | 0.08 | 0.03 | 1.064 | 0.287 | −0.080 | 0.268 | ||
| Have you ever heard about HPV? (reference: no) | 0.799 | 0.06 | 0.42 | 12.723 | 0.000 * | 0.676 | 0.922 | ||
| HPV vaccination status (reference: no) | 0.126 | 0.10 | 0.10 | 1.222 | 0.222 | −0.076 | 0.329 | ||
| Perceived obstacle | Constant | 1.057 | 0.30 | 3.436 | 0.001 * | 0.453 | 1.660 | 0.06 | |
| Age | 0.034 | 0.01 | 0.08 | 2.380 | 0.018 * | 0.006 | 0.062 | ||
| Cinsiyet (reference: boy) | −0.072 | 0.05 | −0.04 | −1.230 | 0.219 | −0.188 | 0.043 | ||
| Department (reference: Physiotherapy and Rehabilitation) | |||||||||
| Nurse | 0.083 | 0.06 | 0.06 | 1.232 | 0.218 | −0.049 | 0.214 | ||
| Midwifery | −0.010 | 0.07 | −0.00 | −0.138 | 0.890 | −0.158 | 0.137 | ||
| Working status (reference: no) | −0.064 | 0.07 | −0.03 | −0.877 | 0.381 | 0.207 | 0.079 | ||
| Have you ever heard about HPV? (reference: no) | 0.296 | 0.05 | 0.21 | 5.739 | 0.000 * | 0.195 | 0.397 | ||
| HPV vaccination status (reference: no) | −0.167 | 0.08 | −0.06 | −1.975 | 0.049 * | −0.334 | −0.001 | ||
| Perceived benefit | Constant | 0.762 | 0.37 | 2.023 | 0.043 * | 0.023 | 1.502 | 0.32 | |
| Age | 0.038 | 0.01 | 0.06 | 2.171 | 0.030 * | 0.004 | 0.072 | ||
| Cinsiyet (reference: boy) | 0.058 | 0.07 | 0.02 | 0.806 | 0.421 | −0.083 | 0.199 | ||
| Department (reference: Physiotherapy and Rehabilitation) | |||||||||
| Nurse | 0.188 | 0.08 | 0.10 | 2.290 | 0.022 * | 0.027 | 0.349 | ||
| Midwifery | 0.460 | 0.09 | 0.24 | 5.003 | 0.000 * | 0.279 | 0.640 | ||
| Working status (reference: no) | 0.170 | 0.08 | 0.05 | 1.912 | 0.056 | −0.005 | 0.345 | ||
| Have you ever heard about HPV? (reference: no) | 0.920 | 0.06 | 0.46 | 14.570 | 0.000 * | 0.796 | 1.044 | ||
| HPV vaccination status (reference: no) | 0.106 | 0.10 | 0.03 | 1.019 | 0.309 | −0.098 | 0.310 | ||
| Perceived sensitivity | Constant | 1.410 | 0.39 | 3.598 | 0.000 * | 0.641 | 2.179 | 0.13 | |
| Age | 0.025 | 0.01 | 0.04 | 1.363 | 0.173 | −0.011 | 0.060 | ||
| Cinsiyet (reference: boy) | −0.058 | 0.07 | −0.02 | −0.780 | 0.432 | −0.205 | 0.089 | ||
| Department (reference: Physiotherapy and Rehabilitation) | |||||||||
| Nurse | 0.017 | 0.08 | 0.01 | 0.203 | 0.839 | −0.150 | 0.185 | ||
| Midwifery | 0.012 | 0.09 | 0.07 | 0.121 | 0.904 | −0.176 | 0.199 | ||
| Working status (reference: no) | −0.004 | 0.09 | −0.02 | −0.048 | 0.962 | −0.186 | 0.178 | ||
| Have you ever heard about HPV? (reference: no) | 0.635 | 0.06 | 0.34 | 9.661 | 0.000 * | 0.506 | 0.763 | ||
| HPV vaccination status (reference: no) | 0.144 | 0.108 | 0.04 | 1.337 | 0.182 | −0.068 | 0.356 | ||
| Unstandardized Coefficients | Standardized Coefficients | 95% CI | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Model | B | SD | β | t | p | Lower | Upper | R2 |
| General HPV knowledge | Constant | −0.3.917 | 1.45 | −2.688 | 0.007 * | −6.777 | −1.057 | 0.51 | |
| Age | 0.265 | 0.06 | 0.10 | 3.953 | 0.000 * | 0.134 | 0.397 | ||
| Cinsiyet (reference: boy) | 0.455 | 0.27 | 0.04 | 1.635 | 0.102 | −0.091 | 1.001 | ||
| Department (reference: Physiotherapy and Rehabilitation) | |||||||||
| Nurse | 1.329 | 0.31 | 0.16 | 4.182 | 0.000 * | 0.705 | 1.952 | ||
| Midwifery | 3.058 | 0.35 | 0.35 | 8.606 | 0.000 * | 2.360 | 3.755 | ||
| Working status (reference: no) | −0.131 | 0.34 | −0.00 | −0.379 | 0.705 | −0.807 | 0.546 | ||
| Have you ever heard about HPV? (reference: no) | 4.944 | 0.24 | 0.54 | 20.247 | 0.000 * | 4.464 | 5.423 | ||
| HPV vaccination status (reference: no) | 0.570 | 0.40 | 0.03 | 0.156 | 0.156 | −0.218 | 1.358 | ||
| HPV screening test knowledge | Constant | −3.373 | 0.67 | −4.975 | 0.000 * | −4.703 | −2.042 | 0.23 | |
| Age | 0.186 | 0.03 | 0.19 | 5.968 | 0.000 * | 0.125 | 0.248 | ||
| Cinsiyet (reference: boy) | 0.275 | 0.12 | 0.07 | 2.123 | 0.034 * | 0.021 | 0.529 | ||
| Department (reference: Physiotherapy and Rehabilitation) | |||||||||
| Nurse | 0.028 | 0.14 | 0.00 | 0.190 | 0.850 | −0.262 | 0.318 | ||
| Midwifery | 0.735 | 0.16 | 0.22 | 4.444 | 0.000 * | 0.410 | 1.059 | ||
| Working status (reference: no) | −0.081 | 0.16 | −0.01 | 0.505 | 0.613 | −0.396 | 0.234 | ||
| Have you ever heard about HPV? (reference: no) | 0.835 | 0.11 | 0.24 | 7.348 | 0.000 * | 0.612 | 1.058 | ||
| HPV vaccination status (reference: no) | 0.341 | 0.18 | 0.05 | 1.825 | 0.068 | −0.026 | 0.708 | ||
| General HPV vaccine knowledge | Constant | −1.567 | 0.70 | −2.234 | 0.026 * | −2.943 | −0.190 | 0.33 | |
| Age | 0.093 | 0.03 | 0.08 | 2.889 | 0.004 * | 0.030 | 0.157 | ||
| Cinsiyet (reference: boy) | 0.400 | 0.13 | 0.09 | 2.990 | 0.003 * | 0.138 | 0.663 | ||
| Department (reference: Physiotherapy and Rehabilitation) | |||||||||
| Nurse | 0.329 | 0.15 | 0.09 | 2.153 | 0.032 * | 0.029 | 0.629 | ||
| Midwifery | 1.252 | 0.17 | 0.34 | 7.320 | 0.000 * | 0.916 | 1.587 | ||
| Working status (reference: no) | −0.194 | 0.16 | −0.03 | −1.167 | 0.243 | −0.519 | 0.132 | ||
| Have you ever heard about HPV? (reference: no) | 1.354 | 0.11 | 0.36 | 11.524 | 0.000 * | 1.124 | 1.585 | ||
| HPV vaccination status (reference: no) | 0.131 | 0.19 | 0.02 | 0.679 | 0.498 | −0.248 | 0.511 | ||
| Knowledge of current HPV vaccination program | Constant | 0.819 | 0.65 | 1.243 | 0.214 | −0.474 | 2.112 | 0.15 | |
| Age | −0.037 | 0.03 | −0.04 | −1.216 | 0.224 | −0.096 | 0.023 | ||
| Cinsiyet (reference: boy) | −0.009 | 0.12 | −0.00 | −0.073 | 0.942 | −0.256 | 0.283 | ||
| Department (reference: Physiotherapy and Rehabilitation) | |||||||||
| Nurse | 0.212 | 0.14 | 0.07 | 1.475 | 0.141 | −0.070 | 0.494 | ||
| Midwifery | 0.730 | 0.16 | 0.24 | 4.546 | 0.000 * | 0.415 | 1.045 | ||
| Working status (reference: no) | 0.321 | 0.15 | 0.06 | 2.060 | 0.040 * | 0.015 | 0.627 | ||
| Have you ever heard about HPV? (reference: no) | 0.813 | 0.11 | 0.26 | 7.368 | 0.000 * | 0.597 | 1.030 | ||
| HPV vaccination status (reference: no) | 0.731 | 0.18 | 0.13 | 4.029 | 0.000 * | 0.375 | 1.088 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ergün, S. The Effect of University Students’ Levels of Knowledge about HPV Infection and the HPV Vaccine on Their Health Beliefs: Health Sciences Students. Vaccines 2023, 11, 1126. https://doi.org/10.3390/vaccines11061126
Ergün S. The Effect of University Students’ Levels of Knowledge about HPV Infection and the HPV Vaccine on Their Health Beliefs: Health Sciences Students. Vaccines. 2023; 11(6):1126. https://doi.org/10.3390/vaccines11061126
Chicago/Turabian StyleErgün, Sibel. 2023. "The Effect of University Students’ Levels of Knowledge about HPV Infection and the HPV Vaccine on Their Health Beliefs: Health Sciences Students" Vaccines 11, no. 6: 1126. https://doi.org/10.3390/vaccines11061126