
Neurological Disorders following COVID-19 Vaccination

Department of Infectious Diseases, Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, Hangzhou 310052, China
*
Author to whom correspondence should be addressed.
Vaccines 2023, 11(6), 1114; https://doi.org/10.3390/vaccines11061114
Submission received: 30 April 2023
/
Revised: 8 June 2023
/
Accepted: 14 June 2023
/
Published: 19 June 2023
(This article belongs to the Special Issue Safety, Efficacy and Optimization of the COVID-19 Vaccines)
Abstract
:Nowadays, people all over the world have been receiving different types of coronavirus disease 2019 (COVID-19) vaccines. While their effectiveness has been well recognized, various post-vaccination disorders are not fully understood. In this review, we discuss neurological disorders related to vascular, immune, infectious, and functional factors following COVID-19 vaccination, and attempt to provide neuroscientists, psychiatrists, and vaccination staff with a reference for the diagnosis and treatment of these diseases. These disorders may present as a recurrence of previous neurological disorders or new-onset diseases. Their incidence rate, host and vaccine characteristics, clinical manifestations, treatment, and prognosis differ significantly. The pathogenesis of many of them remains unclear, and further studies are needed to provide more evidence. The incidence rate of severe neurological disorders is relatively low, most of which are reversible or treatable. Therefore, the benefits of vaccination outweigh the risk of COVID-19 infection, especially among fragile populations.
1. Introduction
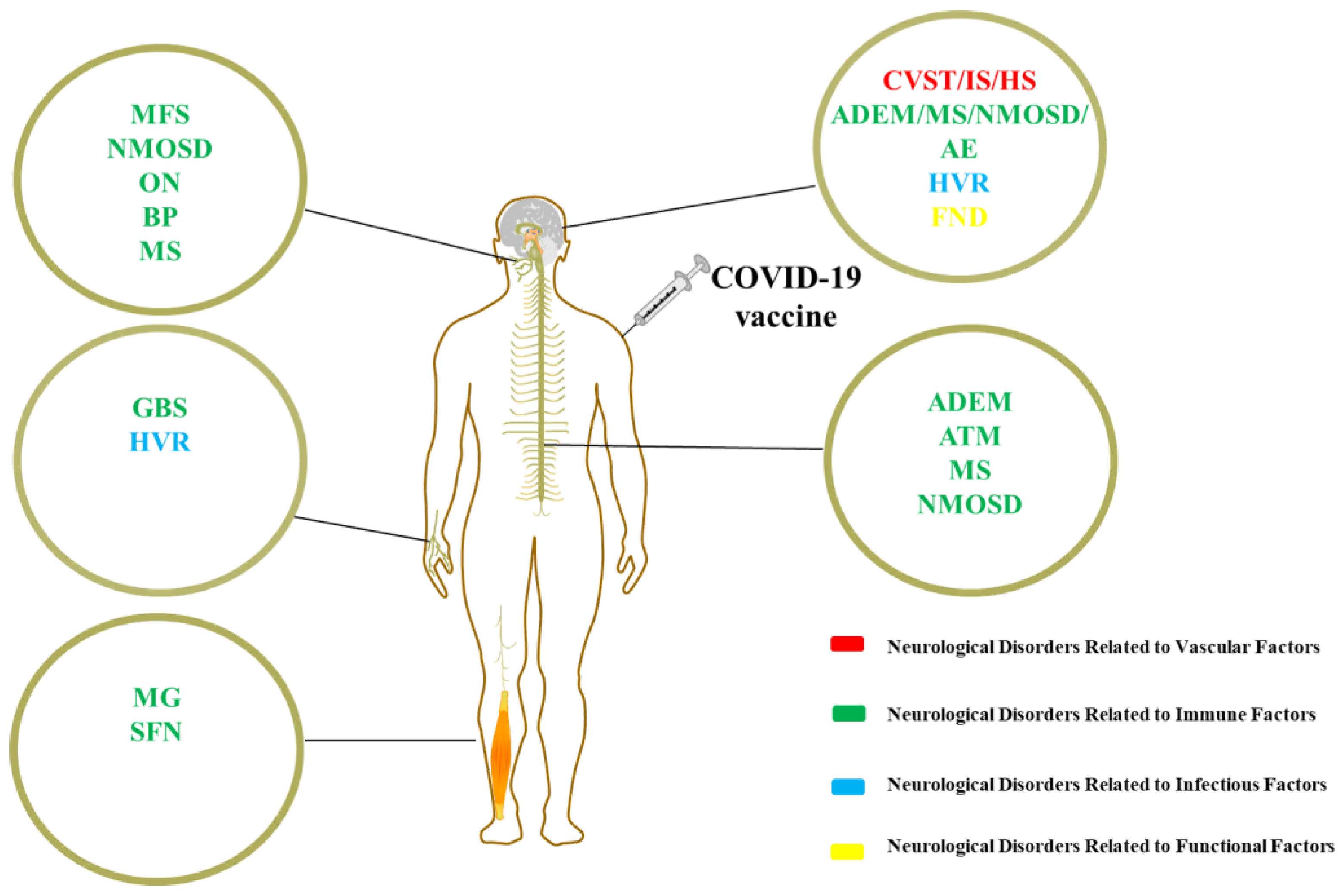
Coronavirus disease 2019 (COVID-19) is predominantly characterized by lung damage and hypoxia, leading to systemic complications and even death. As of the writing of this review, the World Health Organization has reported over 700 million confirmed cases, including over 6 million deaths [1]. COVID-19 vaccines have provided new hope for effectively combating the deadly pandemic. Several vaccines were developed during the pandemic, including inactivated or attenuated virus vaccines, recombinant protein vaccines, virus vector-based vaccines, and messenger RNA (mRNA) vaccines [2]. Safe vaccination with high uptake is crucial to the COVID-19 pandemic response. However, since the emergency authorization of different COVID-19 vaccines, there have been several reports of related diseases, with neurological complications being of significant concern, as they may be persistent and leave sequelae [3]. Almost all types of COVID-19 vaccines may cause neurological complications, and although the association between these vaccines and neurological complications is not yet clear, multiple hypotheses attempt to explain it. Many of these hypotheses are inferred from previous research about other vaccines [4]. Most cases of neurological disorders were anecdotal reports, and more in-depth analysis is needed. In this review, the authors divided them into four categories: neurological disorders related to vascular, immune, infectious, and functional factors, and summarized their characteristics (Figure 1). It aims to provide neuroscientists, psychiatrists, and vaccination staff with a reference for the diagnosis and treatment of these diseases.
2. Discussion
2.1. Neurological Disorders Related to Vascular Factors
Cerebrovascular disease is not uncommon among COVID-19 vaccine recipients [5]. They can range from mild transient cerebral ischemia to fatal cerebrovascular events. Recently, vascular events associated with vaccine-induced immune thrombotic thrombocytopenia (VITT) have drawn much attention. It is speculated that platelet factor-4 (PF4) /polyanion complexes play a pathogenic role. Specific ingredients in the vaccine trigger a strong anti-PF4 immune response, leading to thrombosis with thrombocytopenia syndrome [6]. VITT- and non-VITT-associated vascular events exhibit different clinical features.
2.1.1. Cranial Venous Sinus Thrombosis
Cranial venous sinus thrombosis (CVST) is a cerebrovascular disease with blocked blood flow due to venous sinus thrombosis. It has been reported that over 70% of CVST cases following COVID-19 vaccination are related to VITT, which occurs in recipients of adenoviral vector-based vaccines [7,8]. Despite its low incidence (0.00009% per dose, 0.0005% per individual), it has a high mortality rate (47%) [9,10]. Most cases occur in individuals under 60 years old, with women being more commonly affected, and often accompanied by thrombosis in other parts of the body. The peak onset is between 4 days and 4 weeks after vaccination. Persistent headache is the most common clinical manifestation, along with sensory abnormalities, visual impairment, and so on [9]. Blood tests typically show decreased platelet count, increased D-dimer, and the presence of anti-PF4 antibodies. For suspected cases, cranial magnetic resonance imaging (MRI) combined with contrast-enhanced venous magnetic resonance angiography can aid in the diagnosis [11]. A high dose of intravenous immunoglobulin (IVIG) plus non-heparin anticoagulation is the main therapy strategy, while steroids may be another treatment option to improve the platelet level [6,12]. Nevertheless, CVST cases following COVID-19 vaccination outside the spectrum of VITT have also been reported [8]. Compared to VITT-CVST, non-VITT-CVST shows its own characteristics [7,13] (Table 1).
2.1.2. Ischemic Stroke
Ischemic stroke (IS) is a cerebrovascular disease featured by brain infarction due to the occlusion of cerebral arteries. Its incidence among the COVID-19 vaccine recipients has been reported to range from 0.29 to 1.76/million vaccinations [14,15,16]. Cases of IS have been found after receiving various vaccine types [15]. Previous reports have reached different conclusions on whether vaccination increases the risk of IS. A study based on hospitalized patients recently vaccinated with mRNA COVID-19 vaccines showed that the incidence of IS was within the local baseline for the same period. They explained these cases by pre-existing cardiovascular risk factors rather than vaccines [15]. Another study monitored over 10 million vaccine-eligible members and found no increased IS risk after receiving the BNT162b2 vaccine [17]. A similar result was found in France among adults under 75 years old who received mRNA vaccines within 3 weeks [18]. However, data on approximately 30 million vaccinated patients in the United Kingdom showed that the risk of IS significantly increased after BNT162b2 vaccination [19]. IS after vaccination is characterized by advanced age (mean age of 68~71 years) and is predominantly male [14,15,20]. Many of these patients have previous high-risk factors for stroke. In an observational study based on hospitalized patients after mRNA vaccination, all patients had at least one cardiovascular risk factor (old age, hypertension, hyperlipidemia, diabetes, heart disease, obesity, smoking, atrial fibrillation, etc.) [14]. It is worth mentioning that atrial fibrillation is a risk factor only in female patients [21]. Diabetes is also a study-proven risk factor for IS, with the risk found to be higher in patients with diabetes [22]. The average interval from vaccination to symptoms is 9 days [14,15]. The macrovascular type is the most common subtype, and the anterior circulation is often involved [14,15,23]. Some patients receive revascularization therapy, including intravenous thrombolysis and mechanical thrombectomy, while others receive standardized care [14]. There was no difference in mortality rates between vaccinated IS patients and unvaccinated IS patients [23]. It is worth noting that some cases of IS are related to VITT, accounting for 3.1% [15]. In the VITT-IS group, female and younger patients are more common, many of whom are recipients of adenoviral vector-based vaccines and often accompanied by thrombosis in other sites [24]. Most patients lack previous cardiovascular risk factors, and intravenous thrombolysis is contraindicated [25,26]. High-dose IVIG should be initiated immediately, and non-heparin anticoagulant therapy should start 24 h after stroke onset. Mechanical thrombectomy is considered an effective treatment [27,28].VITT-IS is prone to conversion into malignant embolism (up to 41%) and has a high mortality rate (up to 20.8%) [25].
2.1.3. Hemorrhagic Stroke
Hemorrhagic stroke (HS) is a cerebrovascular disease characterized by cerebral vascular rupture and bleeding. It is reported that the incidence of HS after COVID-19 is 364.7 events per million person-years [17]. HS has distinct gender differences, with a higher risk for females [29]. The occurrence of HS is related to race, with a high proportion in Asian populations [30]. HS occurs after various types of COVID-19 vaccines, especially mRNA vaccines [31]. The pathogenesis of the disease has not been fully exposed. Since most cases lack thrombocytopenia, they may not share a similar mechanism as VITT [17]. Whether COVID-19 vaccination increases the risk of HS remains controversial. A study found that after BNT162b2 vaccination, the risk of HS increased, and the incidence rate ratio (RR) was 1.24 (95% confidence interval (CI) 1.07~1.43) [29]. The report claimed that after being vaccinated with BNT162b2, there were 60 extra cases of HS per 10 million people in 1~28 days [29]. Additional studies further indicated that the risk of bleeding caused by BNT162b2 was specific to the brain rather than to other parts of the body [31]. However, in another study among BNT162b2 recipients, no association was found with HS, with a RR of 0.90 (95% CI 0.72~1.13) [17]. The mortality rate of HS is quite high, reaching 23% in a specific group of adults under 75 years old in France [18]. The mortality rate of COVID-19 in patients with previous HS has increased, making vaccination highly necessary [32]. However, the safety and effectiveness of the COVID-19 vaccine in this population remain unclear due to the lack of sufficient research.
2.2. Neurological Disorders Related to Immune Factors
There are various kinds of neurological disorders related to immune factors reported following COVID-19 vaccination. However, their pathogenesis is still under-researched, so scholars attempt to infer from other vaccines. The most popular hypothesis is molecular mimicry. Based on the similarity between pathogen-derived peptides in vaccines and the human nervous system, the immune response targeting the nervous system may be triggered. For example, mice immunized with influenza virus vaccines produced specific antibodies, supporting the association between influenza vaccines and Guillain–Barre syndrome [33]. COVID-19 vaccines could theoretically trigger cross-reactivity with brain tissue, spinal cord, nerve fibers, and neuromuscular junctions, inducing immune-related neurological disorders. The presence of various antibodies in patients with immune-related neurological disorders after the COVID-19 vaccines further confirms this hypothesis. However, a study conducted in the United Kingdom showed that there was no structural similarity between COVID-19 protein and peripheral nerve protein, although the possibility that the post-translational modification led to a similarity could not be ruled out [34]. The second hypothesis is bystander activation, which means adaptive immune cells are activated by cytokines induced by non-homologous antigens [35]. Susan van Aalst et alreported the bystander activation of irrelevant CD4 + T cells following vaccination occurs in the presence and absence of an adjuvant [36]. Bystander activation is sufficient to induce autoimmune disease, and it seems to better explain the short interval of some neurological disorders after COVID-19 vaccination [37]. In addition, vaccines activate innate immunity through pattern recognition receptors. The adjuvant of the COVID-19 vaccine has been reported to be able to activate toll-like receptors 3, 7, and 9 and produce interferon-α [38]. Interferon-α is related to Bell’s palsy after COVID-19 vaccination [39].
2.2.1. Bell’s Palsy
Bell’s palsy (BP) is an acute peripheral facial nerve paralysis, accounting for 35.7% of all neurological disorders reported after COVID-19 vaccination [40]. The incidence has been estimated to range from 42.8 to 106 cases per 100,000 person-years [41,42]. It is most commonly reported to occur after mRNA vaccines but can also be seen with the inactivated or adenoviral vector-based COVID-19 vaccines [43]. BP occurs after the first or second dose of the vaccine, with a higher occurrence rate after the first dose [44]. There are reports of recurrence in patients with a previous history of BP [45]. The interval from vaccination to palsy is between 6 and 14 days [46,47]. The occurrence has gender differences: It is more common in females after mRNA vaccines but more common in males after inactivated vaccines [41,48,49]. Age difference has been found in some studies, with older people having a higher risk [45]. The mean age ranges from 49.7 to 62.6 years old [29,49,50]. It shows selection in location, with the left side being more commonly affected than the right side [46]. IVIG, steroids, and plasma exchange are first-line treatments, with most patients gaining recovery [44]. Studies draw different conclusions on the correlation between BP and the COVID-19 vaccines. A case-control study on 37 patients with facial nerve palsy who were recently vaccinated with the Pfizer-BioNTech vaccine failed to confirm the association between vaccines and BP (odds ratio (OR) 0.84, 95% CI, 0.37~1.90) [51]. However, a study conducted in Hong Kong assessed the risk of BP within 42 days following vaccination with BNT162b2 or CoronaVac and found a significantly increased risk (OR 2.385, 95% CI 1.415~4.022 for CoronaVac and OR 1.755, 95% CI 0.886~3.477 for BNT162b2) [41]. An analysis of a self-reporting database found BP was significantly more frequently reported after the administration of COVID-19 mRNA vaccines [50]. Fortunately, the excess risk of BP is low, with data from the largest healthcare provider in Israel showing approximately an extra 4.5 cases per 100,000 individuals among the highest associated group [45].
2.2.2. Guillain–Barre Syndrome and Miller–Fisher Syndrome
Guillain–Barre syndrome (GBS) is an acute immune-mediated polyradiculoneuropathy that affects myelinated nerves. GBS is a severe complication after COVID-19 vaccination and a common cause of intensive care unit admission [2,52]. Most GBS cases were reported after the first dose of the vaccine [53,54,55,56]. The onset is usually within 2 weeks after vaccination, with a highly variable range from hours to weeks (within 6 weeks) [54,57,58]. The affected population’s age ranges widely, from 20 to 90 years old, and the incidence rate increases with age, with the mean age being in the 40 s to 60 s [54,55,57,59,60,61]. Most studies showed that males were the most susceptible gender [53,54,60]. Many studies have supported the high risk of GBS caused by adenoviral vector-based vaccines. A cohort study in the United States showed that the incidence rate of GBS during 1 to 21 days after Ad.26.COV2.S was 32.4/100,000 person-years, significantly higher than the background rate. In a head-to-head comparison, the adjusted RR of Ad.26.COV2.S for GBS was 20.56 [62]. Another study showed that within the 42-day window, the reporting rate of GBS after adenoviral vector-based vaccines was 5.57/100,000 person-years, while the background incidence rate was only 1.2~3.1/100,000 person-years [63]. Classic GBS is the most common clinical phenotype, with acute inflammatory demyelinating polyneuropathy (AIDP) as the most common neurophysiological subtype [59,60,64]. Anti-ganglioside antibodies are usually absent in these patients [60]. A recently reported GBS variant after the vaccine is highly characteristic: male dominance, frequent albuminocytological dissociation, and AIDP pattern [65]. Treatment usually includes IVIG and plasma exchange in severe patients, and the prognosis varies greatly [57]. Shaun Kai Kiat Chua et al conducted a review and pooled analysis of the data from 57 published cases. At the beginning of treatment, 60% reported improvement. However, post-treatment outcomes showed that 33% had a GBS disability scale score of 4 or more, indicating that they were either bedridden, needed ventilation support, or died [66]. A detailed customized rehabilitation program is necessary for them [67]. The recurrence risk of COVID-19 vaccination for patients with a GBS history is still uncertain, but some research results show the safety signal. A study showed that only 3.5% of patients have relapsed after vaccination [68]. Adája E Baars et al conducted a prospective, multicenter cohort study on patients with a history of GBS and found that none had a recurrence after vaccination [69].
Miller–Fisher syndrome (MFS) is rare after COVID-19 vaccination, characterized by ataxia, ametropia, ophthalmoplegia, and ametropia triad. It has been reported that the majority of MFS after the COVID-19 vaccine were males, and the median age was 65 years old. Various MFS phenotypes have been reported, including typical MFS, partial MFS, and even involvement of limbs and respiratory muscles. Cerebrospinal fluid (CSF) analysis shows typical albuminocytological dissociation and positive anti-GQ1b ganglioside antibody [70]. IVIG is the main treatment, and the prognosis for most patients is good [71,72]. Although it is a variant of GBS, it differs from GBS in many aspects [70,71,72] (Table 2).
2.2.3. Myasthenia Gravis
Myasthenia gravis (MG) is an autoimmune disease caused by antibodies that bind to neuromuscular junction components, resulting in weakness of skeletal muscles. Cases of MG have been reported after COVID-19 vaccination, including both new-onset and worsening of previous MG [73,74]. These cases have been described following various COVID-19 vaccines and different doses [73,75,76]. The incidence reported varies greatly, ranging from 1% to 14.5% [77,78]. Acetylcholine receptor and muscle-specific receptor tyrosine kinase antibodies are only found in some patients [79]. New-onset patients usually have a short onset time (0~8 days) after vaccination, while the recurrence shows a longer interval (up to 3 months) [74,75]. Mild patients do not require additional medication, while severe ones need enhanced immunotherapy, such as steroids, IVIG, and plasma exchange. Patients with respiratory muscle involvement always receive tracheal intubation [78,80]. The prognosis may be variable. In a prospective study, patients only experienced temporary deterioration and responded well to treatment [77]. However, there were reports of fatal cases due to the MG crisis [81,82]. Patients with MG (pwMG) have poor outcomes of COVID-19 infection, which are also known as fragile populations. A retrospective observational study of MG patients in Brazil found that 87% of MG-COVID cases required intensive care, 73% needed mechanical ventilation, and 30% died [83]. COVID-19 infection in vaccinated MG patients would be milder, so this population needs vaccination during the epidemic. Some studies have shown the safety of the COVID-19 vaccine in pwMG. A study compared the deterioration rate of MG after COVID-19 vaccination with that of previous years and found that vaccination did not increase the risk of MG worsening [73]. The relationship between the stability of the previous MG and the deterioration after vaccination is still unclear. Some patients with unstable MG did not experience worsening symptoms, while others with well-controlled conditions deteriorated after vaccination [75].
2.2.4. Demyelinating Diseases
Optic Neuritis
Optic neuritis (ON) is an inflammatory disorder that affects the optic nerve, with demyelination being a common pathology subtype. ON is relatively common after COVID-19 vaccination. Cases of ON have been reported following various vaccines, including inactivated vaccines, adenoviral vector-based vaccines, and mRNA vaccines [84,85,86]. Both the first and second doses of vaccine-related ON have been reported, with an interval time of 0~19 days [85,87,88]. One or both sides of the optic nerve will be affected, typically presenting with visual impairment and eye pain, rarely presenting only papilledema [87,88]. Myelin oligodendrocyte glycoprotein (MOG) IgG is present in some patients [85]. Patients usually receive steroid therapy, and severe ones need a combination of plasma exchange [89]. A study involving 715 patients found that affected individuals were mainly females, elderly, and American and Europe residents. A total of 73% of cases belonged to severe cases, and only 11% of patients completely recovered after treatments, although there were no fatal cases in this study. Since partial patients may ultimately be diagnosed with multiple sclerosis or neuromyelitis optica spectrum disorder, it is difficult to accurately determine the incidence rate from the reports [90].
Acute Transverse Myelitis
Acute transverse myelitis (ATM) is an acquired demyelinating disease of the spinal cord. ATM following COVID-19 vaccination is rare, with an incidence of approximately 1~4 cases per million people [61]. Interestingly, there were quite a few reports of a subtype called longitudinally extended transfer myelitis, which involves three or more vertebral segments [91]. The mean age of patients was typically in the 40 s to 50 s, and a large proportion of patients had previous autoimmune diseases [92,93]. Compared with COVID-19-related ATMs, vaccine-related ones show shorter intervals and milder clinical manifestations [92,93]. They occur after various types of COVID-19 vaccines, with the adenoviral vector-based vaccine being the most common [91,94,95,96]. Cases are characterized by quadriplegia or lower limb paralysis, transverse sensory level, and rectal or bladder dysfunction. The thoracic spine is the most frequently involved [92]. Some patients’ CSF may show an increase in leukocyte count and protein. Specific oligoclonal bands may appear in CSF, and MOG and aquaporin protein-4 (AQP4) antibodies are usually absent. MRI may show a high signal of the spinal cord on T2 or fluid-attenuated inversion recovery (FLAIR) sequence, and the lesion may involve an extensive spinal cord. High-dose steroids are the basic treatment, and in severe cases, a combination of IVIG, immunosuppressive agents, or plasma exchange is needed [97]. Most patients have a good prognosis, with only a few deaths [92]. Older age, the second dose of vaccine, and a modified Rankin score of ≥3 are indicators of poor prognosis [92].
Acute Disseminated Encephalomyelitis
Acute disseminated encephalomyelitis (ADEM) is an acute or subacute demyelinating disease that affects multiple parts of the central nervous system, accompanied by encephalopathy. According to reports, the incidence of ADEM following COVID-19 vaccination was as low as 0.36 cases per million people [98]. Unlike previous ADEM, ADEM after COVID-19 vaccination predominantly affects female adults, and most patients have no underlying diseases or immunosuppressive medication usage [99,100]. ADEM can occur among different vaccine recipients, with adenovirus vector-based vaccines dominating [100,101]. Most patients initially show clinical symptoms within 1 to 35 days after COVID-19 vaccination, which is shorter than other demyelinating diseases [100,102]. It may manifest as the only clinical condition or a part of multiple autoimmune syndromes [103]. MOG antibodies are present in the serum of some patients with COVID-19 vaccine-related ADEM [102]. The key therapy for severe patients includes IVIG, steroids, and plasma exchange [100]. ADEM usually presents as a monophasic course, although a few recurrent cases have been reported [104]. Fortunately, most patients have a good prognosis after treatment, with a few fatal cases [102].
Multiple Sclerosis
Multiple sclerosis (MS) is a central nervous system chronic immune-inflammatory demyelinating disease that can lead to irreversible disability. Patients with MS (pwMS) are at greater risk and have poorer outcomes of COVID-19 infection [105]. PwMS are considered fragile populations, and statements have been released in many countries that pwMS need vaccination against COVID-19 [106,107]. There are reports of new-onset and recurrent MS cases after COVID-19 vaccination [93,108]. According to a systematic review, the affected population was mainly young adults, with a mean age of 33.5 years [105]. Similar to the previously reported MS, the cases after COVID-19 vaccination are mainly females [93,109,110,111,112]. Studies showed that the mean onset time was 6 to 9 days, and sensory abnormality was the most common clinical manifestation [93,109]. MRI shows new emerging signals on the T2 and FLAIR sequences. The brain is the most commonly affected, followed by the spinal cord. Specific oligoclonal bands could be present in CSF [93]. MS usually occurs after adenoviral vector-based and mRNA vaccines [109,113]. It is worth mentioning that the MRI of some newly diagnosed cases showed a mix of new and old lesions, so we cannot completely rule out a previously pre-clinical MS [114]. Karlo Toljan et al. reported that some patients responded to high-dose steroids, while others needed additional plasmapheresis [114]. The lesions disappear in most patients after treatments, but unfortunately, a few could not recover to baseline [109]. Different conclusions have been drawn from studies about whether the COVID-19 vaccines increased the recurrence risk of MS. Epidemiological survey showed that after the first and second doses of vaccination, the acute recurrence rates were 0.65 to 2.1% and 0.85 to 1.6%, respectively. It is hard to separate these from natural recurrence rates since they were too close to non-vaccination ones during the same period [115,116]. However, other studies showed that COVID-19 vaccination increased the recurrence risk of MS due to different vaccine types and follow-up periods [113].
Neuromyelitis Optica Spectrum Disorder
Neuromyelitis optica spectrum disorder (NMOSD) is a neuro-inflammatory demyelinating disease in the optic nerves and spinal cord. Vaccines can be a trigger for NMOSD, including the COVID-19 vaccine. NMOSD can occur in various COVID-19 vaccine recipients, with adenoviral vector-based vaccines being the most common [100,117]. Some patients have previous autoimmune diseases [118]. Most patients reported the initiation of symptoms after receiving the first dose of the vaccine with a median interval of 6 to 10 days [100,117]. Females are more commonly affected, and the age ranges widely, from young people to the elderly [100,117,119]. Acute medullary syndrome is the most common clinical manifestation [100]. CSF analysis shows elevated monocyte lymphocyte and protein levels [117]. Most patients improve through high-dose steroids or plasma exchange, while some patients need maintenance treatments, including rituximab and azathioprine [117]. Even after active treatment, some patients may have sequelae, while elderly patients may experience death [100,119]. The specific biomarker of NMOSD (AQP4 antibody) is present in the majority of patients (up to 83.3%) [117]. Regarding clinical relapse after vaccination among patients with NMOSD, it has been reported that the mean occurrence time was 49.75 days with an incidence rate of 4.67%. Patients are mainly females, and AQP4 IgG or MOG IgG is usually present. Some patients need immunotherapy, such as rituximab, azathioprine, and steroids. The clinical recovery of most patients is well [117]. Recurrence seems to be related to the disease status before vaccination. A recent study revealed a higher risk of vaccination-associated relapse in untreated patients [120].
2.2.5. Autoimmune Encephalitis
Autoimmune encephalitis (AE) is a disease where antibodies target brain tissue, leading to cognitive disorders, mental disorders, and seizures. AE after COVID-19 vaccination is rare. A systematic review showed 14 cases of AE after COVID-19 vaccination and summarized their clinical characteristics: It often occurs in young adults, with a median age of 32 [121]. Different from the COVID-19-related AE, the majority of AE after vaccination are females [121]. AE occurs after both adenoviral vector-based and mRNA vaccines, and most happen at the first dose [99]. Symptoms appear quickly after vaccination, with a median time interval of 5 days [121]. The N-methyl-D-aspartate-receptor (NMDAR) antibody and leucine-rich glioma inactivated gene-1 antibody are found only in some of the patients [99,122]. Consciousness decline and speech or memory disorder are common clinical manifestations [121]. Brain MRI suggests abnormal lesions on the cerebral cortex and deep gray matter, with the temporal lobe being the more commonly affected site [121]. Many patients may have MRI-negative findings, and a positron emission tomography/computed tomography is needed [121]. Inflammatory biomarkers of peripheral blood do not increase, but lymphocytes, protein, and glucose elevate in CSF [121,123,124]. Electroencephalography indicates θ and δ rhythm [121]. Patients show improvements through single or combined immunotherapy, including steroids, IVIG, and rituximab. However, sequelae are found among many patients [121]. Concern has been raised about the recurrence among patients with AE (pwAE) after the COVID-19 vaccination. A cross-sectional survey showed that only 3.3% of 121 pwAE recurred after inactivated COVID-19 vaccination, one recurred within 1 month, and three recurred 3 months later [125]. Unlike new-onset AE, the recurrent cases are mostly NMDARpositive. In addition, the median interval is significantly longer than that of new-onset AE.
2.2.6. Small Fiber Neuropathy
Small fiber neuropathy (SFN) is a peripheral neuropathy involving small nerve fibers. Previous studies have shown that a large proportion of SFN cases occurring after the COVID-19 vaccine involve autoantibodies, indicating that the disease has the basis of autoimmunity [126,127,128]. One study found that the titers of antibodies to adrenergic receptors, muscarinic cholinergic receptors, and angiotensin-converting enzyme 2 increased in an SFN patient after the COVID-19 vaccine [127]. Antibodies to fibroblast growth factor receptor 3 were found in another case [126]. They may either be a new-onset case or a recurrence of the previous condition [129]. Acute sensory abnormality is one of the outstanding clinical features, such as burning dysesthesias, numbness, tingling sensation, and tinnitus [127,130]. Another feature is dysautonomia, and postnatal orthostatic tachycardia syndrome has been reported as a typical manifestation [127]. Electromyography shows normal peripheral nerves, while skin biopsy indicates that the density of nerve fibers decreases [126,130]. Patients with mild symptoms only need painkillers to release. Considering the autoimmune basis of the disease, the use of steroids and IVIG is also helpful [126,127]. Some patients recover quickly, while others experience symptoms for a prolonged period [126].
2.3. Neurological Disorders Related to Infectious Factors
Sporadic reports emerge about the occurrence of infectious diseases in the nervous system after COVID-19 vaccination. Although the precise mechanism is unknown, innate or cell-mediated immune defense failure caused by vaccines has been considered a potential factor [131]. A study by Walsh et al on the safety and immunogenicity of the BNT162b2 vaccine found a brief decrease in lymphocyte count after vaccination [132].
Herpes virus reactivation (HVR) refers to the proliferation of the herpes virus latent in the human body previously, leading to the worsening of infection. HVR after the COVID-19 vaccination, especially the varicella-zoster virus (VZV) causes great concern. Psichogiou et al claimed that temporary disability of VZV-specific CD8 + T cell function could reactivate the virus in the body [133]. The incidence was reported to be as high as 0.22%, significantly higher than that of non-vaccinated people [134]. Almost all types of COVID-19 vaccines may cause reactivation, especially the mRNA vaccines [135,136,137,138]. A study showed that mRNA COVID-19 vaccines were associated with higher reports of VZV reactivation compared with the influenza vaccine (OR 1.9, 95% CI 1.8~2.1) [139]. Mild cases present VZV radiculitis and neurofibroitis, while severe cases endanger the eyes and central nervous system [139]. Either the first or second dose of the vaccine faces this risk. A systematic review showed that there were more cases reported after the first vaccination [136]. A large portion of affected individuals previously have varying degrees of immunosuppression. A study found that up to 23% of patients were receiving immunosuppressive therapy or having autoimmune diseases [136]. Another risk factor is age, and the affected individuals have characteristics of advanced age. Compared to the elderly, the risk of VZV reactivation was reduced in people under 40 years old (OR 0.39, 95% CI 0.36~0.41) [139]. Other high-risk factors include diabetes and chronic hepatitis B virus infection [140]. No significant difference in the incidence between males and females was found [141]. The onset time depends on the type of recurrence: For those, the central nervous system is not involved, the mean onset time is 7.2 days, while for those where the central nervous system is affected, the mean time lengthens to 17.5 days [139]. A self-controlled case series and nested case-control study found that the high-risk period for VZV recurrence was from the first dose to 14 days after the second dose of the mRNA vaccines [137]. Most patients receive standard antiviral treatment, while some need hospitalization [139,141].
2.4. Neurological Disorders Related to Functional Factors
Neurological disorders related to functional factors following the COVID-19 vaccine are neither related to vaccine composition nor immunological factors [142]. They are contributing to biological, environmental, or psychosocial factors: misunderstanding of COVID-19, excessive stress associated with the pandemic, and the painful sensation of vaccination [143]. Among them, functional neurological disorder (FND) has drawn much attention.
FND is a disease related to brain network function, rather than the structure of the nervous system [144]. FND after vaccination has been reported with other vaccines, and COVID-19 vaccine-related FND has aroused great interest from clinicians due to it being widespread [145]. COVID-19 vaccine-related FND accounts for 2.88 to 3.5% of COVID-19 vaccine-related neurological complications [40,146]. Some patients with existing FND reported worsening symptoms, while new-onset cases are rapidly increasing. FND occurs after almost every type of COVID-19 vaccine [147]. There are diverse clinical manifestations, including motor, sensory, visual, and hypersensitivity [146]. The onset time varies from several minutes to weeks, but most cases attack suddenly with a mean onset time of 1 day [146,147]. Even with the intervention of psychologists, some patients remain with disabilities [148]. Compared with the COVID-19 related-FND, vaccine-related FND has unique characteristics. A comparing study found that patients were younger, female-dominated, had more acute onset, and had no neuropsychiatric abnormalities previously [148]. FND is treatable and requires early intervention to prevent chronic disease progression. A detailed explanation of the side effects of vaccines is an important measure for prevention [149].
3. Conclusions
A variety of neurological disorders may occur among individuals who have recently received the COVID-19 vaccines. These disorders can be classified into four categories: those related to vascular factors, immune factors, infectious factors, and functional factors, and some may be related to multiple factors. Their possible pathogenesis, incidence rate, host and vaccine characteristics, clinical manifestations, treatments, and prognosis differ significantly. Neurological disorders can present as new-onset cases or as a recurrence of existing diseases. The pathogenesis of many neurological disorders following the COVID-19 vaccines remains unclear, and more in-depth studies are needed to clarify current hypotheses and provide additional evidence. The incidence rate of severe neurological disorders is relatively low, and the benefits of vaccination outweigh the risk of COVID-19 infection, especially among fragile populations.
Author Contributions
Writing—original draft preparation, Y.Y.; supervision, L.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We thank our English editing staff for their contributions to this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 17 May 2023).
- Mendez-Lizarraga, C.A.; Chacon-Cruz, E.; Carrillo-Meza, R.; Hernández-Milán, N.S.; Inustroza-Sánchez, L.C.; Ovalle-Marroquín, D.F.; Machado-Contreras, J.R.; Ceballos Zuñiga, O.; Bejarano-Ramírez, V.; Aguilar-Aguayo, C.; et al. Report of Adverse Effects Following Population-Wide COVID-19 Vaccination: A Comparative Study between Six Different Vaccines in Baja-California, Mexico. Vaccines 2022, 10, 1196. [Google Scholar] [CrossRef] [PubMed]
- Mohseni Afshar, Z.; Sharma, A.; Babazadeh, A.; Alizadeh-Khatir, A.; Sio, T.T.; Taghizadeh Moghadam, M.A.; Tavakolli Pirzaman, A.; Mojadad, A.; Hosseinzadeh, R.; Barary, M.; et al. A review of the potential neurological adverse events of COVID-19 vaccines. Acta Neurol. Belg. 2023, 123, 9–44. [Google Scholar] [CrossRef] [PubMed]
- Allahyari, F.; Molaee, H.; Hosseini Nejad, J. COVID-19 vaccines and neurological complications: A systematic review. Z. Naturforschung. C J. Biosci. 2023, 78, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Azorin, D.; Baykan, B.; Beghi, E.; Doheim, M.F.; Fernandez-de-Las-Penas, C.; Gezegen, H.; Guekht, A.; Hoo, F.K.; Santacatterina, M.; Sejvar, J.; et al. Timing of headache after COVID-19 vaccines and its association with cerebrovascular events: An analysis of 41,700 VAERS reports. Cephalalgia Int. J. Headache 2022, 42, 1207–1217. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Warkentin, T.E. Recognizing Vaccine-Induced Immune Thrombotic Thrombocytopenia. Crit. Care Med. 2022, 50, e80–e86. [Google Scholar] [CrossRef] [PubMed]
- Palaiodimou, L.; Stefanou, M.I.; de Sousa, D.A.; Coutinho, J.M.; Papadopoulou, M.; Papaevangelou, V.; Vassilakopoulos, T.I.; Tsiodras, S.; Filippou, D.K.; Tsivgoulis, G. Cerebral venous sinus thrombosis in the setting of COVID-19 vaccination: A systematic review and meta-analysis. J. Neurol. 2022, 269, 3413–3419. [Google Scholar] [CrossRef]
- Krzywicka, K.; van de Munckhof, A.; Sánchez van Kammen, M.; Heldner, M.R.; Jood, K.; Lindgren, E.; Tatlisumak, T.; Putaala, J.; Kremer Hovinga, J.A.; Middeldorp, S.; et al. Age-Stratified Risk of Cerebral Venous Sinus Thrombosis After SARS-CoV-2 Vaccination. Neurology 2022, 98, e759–e768. [Google Scholar] [CrossRef]
- Fervers, P.; Kottlors, J.; Persigehl, T.; Lennartz, S.; Maus, V.; Fischer, S.; Styczen, H.; Deuschl, C.; Schlamann, M.; Mpotsaris, A.; et al. Meaningful use of imaging resources to rule out cerebral venous sinus thrombosis after ChAdOx1 COVID-19 vaccination: Evaluation of the AHA diagnostic algorithm with a clinical cohort and a systematic data review. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2022, 102, 5–12. [Google Scholar] [CrossRef]
- Sánchez van Kammen, M.; Aguiar de Sousa, D.; Poli, S.; Cordonnier, C.; Heldner, M.R.; van de Munckhof, A.; Krzywicka, K.; van Haaps, T.; Ciccone, A.; Middeldorp, S.; et al. Characteristics and Outcomes of Patients With Cerebral Venous Sinus Thrombosis in SARS-CoV-2 Vaccine-Induced Immune Thrombotic Thrombocytopenia. JAMA Neurol. 2021, 78, 1314–1323. [Google Scholar] [CrossRef]
- Wittstock, M.; Walter, U.; Volmer, E.; Storch, A.; Weber, M.A.; Großmann, A. Cerebral venous sinus thrombosis after adenovirus-vectored COVID-19 vaccination: Review of the neurological-neuroradiological procedure. Neuroradiology 2022, 64, 865–874. [Google Scholar] [CrossRef]
- Islam, A.; Bashir, M.S.; Joyce, K.; Rashid, H.; Laher, I.; Elshazly, S. An Update on COVID-19 Vaccine Induced Thrombotic Thrombocytopenia Syndrome and Some Management Recommendations. Molecules 2021, 26, 5004. [Google Scholar] [CrossRef] [PubMed]
- Sharifian-Dorche, M.; Bahmanyar, M.; Sharifian-Dorche, A.; Mohammadi, P.; Nomovi, M.; Mowla, A. Vaccine-induced immune thrombotic thrombocytopenia and cerebral venous sinus thrombosis post COVID-19 vaccination; a systematic review. J. Neurol. Sci. 2021, 428, 117607. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.S.; Hoe, R.H.M.; Yong, M.H.; Chiew, H.J.; Goh, Y.; Yong, K.P.; Tu, T.M.; Chan, D.W.S.; Tan, B.Y.; Yeo, L.L.L.; et al. Hospital-based observational study of neurological disorders in patients recently vaccinated with COVID-19 mRNA vaccines. J. Neurol. Sci. 2021, 430, 120030. [Google Scholar] [CrossRef] [PubMed]
- Stefanou, M.I.; Palaiodimou, L.; Aguiar de Sousa, D.; Theodorou, A.; Bakola, E.; Katsaros, D.E.; Halvatsiotis, P.; Tzavellas, E.; Naska, A.; Coutinho, J.M.; et al. Acute Arterial Ischemic Stroke Following COVID-19 Vaccination: A Systematic Review and Meta-analysis. Neurology 2022, 99, e1465–e1474. [Google Scholar] [CrossRef] [PubMed]
- López-Mena, D.; García-Grimshaw, M.; Saldivar-Dávila, S.; Hernandez-Vanegas, L.E.; Saniger-Alba, M.D.M.; Gutiérrez-Romero, A.; Carrillo-Mezo, R.; Valdez-Ruvalcaba, H.E.; Cano-Nigenda, V.; Flores-Silva, F.D.; et al. Stroke Among SARS-CoV-2 Vaccine Recipients in Mexico: A Nationwide Descriptive Study. Neurology 2022, 98, e1933–e1941. [Google Scholar] [CrossRef] [PubMed]
- Klein, N.P.; Lewis, N.; Goddard, K.; Fireman, B.; Zerbo, O.; Hanson, K.E.; Donahue, J.G.; Kharbanda, E.O.; Naleway, A.; Nelson, J.C.; et al. Surveillance for Adverse Events After COVID-19 mRNA Vaccination. JAMA 2021, 326, 1390–1399. [Google Scholar] [CrossRef]
- Botton, J.; Jabagi, M.J.; Bertrand, M.; Baricault, B.; Drouin, J.; Le Vu, S.; Weill, A.; Farrington, P.; Zureik, M.; Dray-Spira, R. Risk for Myocardial Infarction, Stroke, and Pulmonary Embolism Following COVID-19 Vaccines in Adults Younger Than 75 Years in France. Ann. Intern. Med. 2022, 175, 1250–1257. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Patone, M.; Mei, X.W.; Saatci, D.; Dixon, S.; Khunti, K.; Zaccardi, F.; Watkinson, P.; Shankar-Hari, M.; Doidge, J.; et al. Risk of thrombocytopenia and thromboembolism after COVID-19 vaccination and SARS-CoV-2 positive testing: Self-controlled case series study. BMJ 2021, 374, n1931. [Google Scholar] [CrossRef]
- Gorenflo, M.P.; Davis, P.B.; Kaelber, D.C.; Xu, R. Ischemic stroke after COVID-19 bivalent vaccine administration in patients aged 65 years and older: Analysis of nation-wide patient electronic health records in the United States. medRxiv 2023. [Google Scholar] [CrossRef]
- Ye, X.; Huang, C.; Yan, V.K.C.; Kang, W.; Fan, M.; Tsang, G.K.C.; Ho, C.M.Y.; Lip, G.Y.H.; Yiu, K.H.; Tse, H.F.; et al. Sex-based differences in risk of ischemic stroke or systemic embolism after BNT162b2 or CoronaVac COVID-19 vaccination in patients with atrial fibrillation: A self-controlled case series and nested case-control study. Eur. Heart J. Cardiovasc. Pharmacother. 2023; in press. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, S.J.; Sa, S.; Bae, J.H.; Song, G.; Lee, C.W.; Kim, J.H.; Shim, S.R.; Hong, M.; Han, H.W. Safety of COVID-19 Vaccines among Patients with Type 2 Diabetes Mellitus: Real-World Data Analysis. Diabetes Metab. J. 2023, 47, 356–365. [Google Scholar] [CrossRef]
- Stamenković, M.; Radmilo, L.; Jovićević, M.; Rabi-Žikić, T.; Žarkov, M.; Ružička-Kaloci, S.; Simić, S.; Stamenković, A.; Dangić, J.; Knezović, G.; et al. Clinical Characteristics of Patients with Acute Ischemic Stroke Previously Vaccinated Against COVID-19. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2022, 31, 106483. [Google Scholar] [CrossRef] [PubMed]
- Kolahchi, Z.; Khanmirzaei, M.; Mowla, A. Acute ischemic stroke and vaccine-induced immune thrombotic thrombocytopenia post COVID-19 vaccination; a systematic review. J. Neurol. Sci. 2022, 439, 120327. [Google Scholar] [CrossRef] [PubMed]
- Cascio Rizzo, A.; Giussani, G.; Agostoni, E.C. Ischemic Stroke and Vaccine-Induced Immune Thrombotic Thrombocytopenia following COVID-19 Vaccine: A Case Report with Systematic Review of the Literature. Cerebrovasc. Dis. 2022, 51, 722–734. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2018, 49, e46–e110. [Google Scholar] [CrossRef]
- Mowla, A.; Razavi, S.M.; Lail, N.S.; Mohammadi, P.; Shirani, P.; Kavak, K.S.; Sawyer, R.N.; Kamal, H. Hyperdense middle cerebral artery sign and response to combination of mechanical Thrombectomy plus intravenous thrombolysis in acute stroke patients. J. Neurol. Sci. 2021, 429, 117618. [Google Scholar] [CrossRef] [PubMed]
- Kenda, J.; Lovrič, D.; Škerget, M.; Milivojević, N. Treatment of ChAdOx1 nCoV-19 Vaccine-Induced Immune Thrombotic Thrombocytopenia Related Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2021, 30, 106072. [Google Scholar] [CrossRef]
- Patone, M.; Handunnetthi, L.; Saatci, D.; Pan, J.; Katikireddi, S.V.; Razvi, S.; Hunt, D.; Mei, X.W.; Dixon, S.; Zaccardi, F.; et al. Neurological complications after first dose of COVID-19 vaccines and SARS-CoV-2 infection. Nat. Med. 2021, 27, 2144–2153. [Google Scholar] [CrossRef]
- Moll, K.; Lufkin, B.; Fingar, K.R.; Ke Zhou, C.; Tworkoski, E.; Shi, C.; Hobbi, S.; Hu, M.; Sheng, M.; McCarty, J.; et al. Background rates of adverse events of special interest for COVID-19 vaccine safety monitoring in the United States, 2019–2020. Vaccine 2023, 41, 333–353. [Google Scholar] [CrossRef]
- Chui, C.S.L.; Fan, M.; Wan, E.Y.F.; Leung, M.T.Y.; Cheung, E.; Yan, V.K.C.; Gao, L.; Ghebremichael-Weldeselassie, Y.; Man, K.K.C.; Lau, K.K.; et al. Thromboembolic events and hemorrhagic stroke after mRNA (BNT162b2) and inactivated (CoronaVac) COVID-19 vaccination: A self-controlled case series study. EClinicalMedicine 2022, 50, 101504. [Google Scholar] [CrossRef]
- Lazcano, U.; Cuadrado-Godia, E.; Grau, M.; Subirana, I.; Martínez-Carbonell, E.; Boher-Massaguer, M.; Rodríguez-Campello, A.; Giralt-Steinhauer, E.; Fernández-Pérez, I.; Jiménez-Conde, J.; et al. Increased COVID-19 Mortality in People With Previous Cerebrovascular Disease: A Population-Based Cohort Study. Stroke 2022, 53, 1276–1284. [Google Scholar] [CrossRef]
- Nachamkin, I.; Shadomy, S.V.; Moran, A.P.; Cox, N.; Fitzgerald, C.; Ung, H.; Corcoran, A.T.; Iskander, J.K.; Schonberger, L.B.; Chen, R.T. Anti-ganglioside antibody induction by swine (A/NJ/1976/H1N1) and other influenza vaccines: Insights into vaccine-associated Guillain-Barré syndrome. J. Infect. Dis. 2008, 198, 226–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keddie, S.; Pakpoor, J.; Mousele, C.; Pipis, M.; Machado, P.M.; Foster, M.; Record, C.J.; Keh, R.Y.S.; Fehmi, J.; Paterson, R.W.; et al. Epidemiological and cohort study finds no association between COVID-19 and Guillain-Barré syndrome. Brain A J. Neurol. 2021, 144, 682–693. [Google Scholar] [CrossRef] [PubMed]
- Messina, N.L.; Zimmermann, P.; Curtis, N. The impact of vaccines on heterologous adaptive immunity. Clin. Microbiol. Infect. 2019, 25, 1484–1493. [Google Scholar] [CrossRef] [PubMed]
- van Aalst, S.; Ludwig, I.S.; van der Zee, R.; van Eden, W.; Broere, F. Bystander activation of irrelevant CD4+ T cells following antigen-specific vaccination occurs in the presence and absence of adjuvant. PLoS ONE 2017, 12, e0177365. [Google Scholar] [CrossRef]
- Wraith, D.C.; Goldman, M.; Lambert, P.H. Vaccination and autoimmune disease: What is the evidence? Lancet 2003, 362, 1659–1666. [Google Scholar] [CrossRef]
- Teijaro, J.R.; Farber, D.L. COVID-19 vaccines: Modes of immune activation and future challenges. Nat. Rev. Immunol. 2021, 21, 195–197. [Google Scholar] [CrossRef]
- Soeiro, T.; Salvo, F.; Pariente, A.; Grandvuillemin, A.; Jonville-Béra, A.P.; Micallef, J. Type I interferons as the potential mechanism linking mRNA COVID-19 vaccines to Bell’s palsy. Therapie 2021, 76, 365–367. [Google Scholar] [CrossRef]
- Alonso Castillo, R.; Martínez Castrillo, J.C. Neurological manifestations associated with COVID-19 vaccine. Neurologia, 2022; in press. [Google Scholar] [CrossRef]
- Wan, E.Y.F.; Chui, C.S.L.; Lai, F.T.T.; Chan, E.W.Y.; Li, X.; Yan, V.K.C.; Gao, L.; Yu, Q.; Lam, I.C.H.; Chun, R.K.C.; et al. Bell’s palsy following vaccination with mRNA (BNT162b2) and inactivated (CoronaVac) SARS-CoV-2 vaccines: A case series and nested case-control study. Lancet Infect. Dis. 2022, 22, 64–72. [Google Scholar] [CrossRef]
- Ozonoff, A.; Nanishi, E.; Levy, O. Bell’s palsy and SARS-CoV-2 vaccines. Lancet Infect. Dis. 2021, 21, 450–452. [Google Scholar] [CrossRef]
- Bertin, B.; Grenet, G.; Pizzoglio-Billaudaz, V.; Lepelley, M.; Atzenhoffer, M.; Vial, T. Vaccines and Bell’s palsy: A narrative review. Therapie 2022, 78, 279–292. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, M.; Ansari, I.; Ahmad, H.; Ghaffar, H.; Khurshid, A.; Shahid, A.; Essar, M.Y.; Ullah, I.; Cheema, H.A. Development of facial palsy following COVID-19 vaccination: A systematic review. Ann. Med. Surg. 2022, 82, 104758. [Google Scholar] [CrossRef] [PubMed]
- Shibli, R.; Barnett, O.; Abu-Full, Z.; Gronich, N.; Najjar-Debbiny, R.; Doweck, I.; Rennert, G.; Saliba, W. Association between vaccination with the BNT162b2 mRNA COVID-19 vaccine and Bell’s palsy: A population-based study. Lancet Reg. Health. Eur. 2021, 11, 100236. [Google Scholar] [CrossRef] [PubMed]
- Shahsavarinia, K.; Mahmoodpoor, A.; Sadeghi-Ghyassi, F.; Nedayi, A.; Razzaghi, A.; Zehi Saadat, M.; Salehi-Pourmehr, H. Bell’s Palsy and COVID-19 Vaccination: A Systematic Review. Med. J. Islam. Repub. Iran 2022, 36, 85. [Google Scholar] [CrossRef]
- Shemer, A.; Pras, E.; Hecht, I. Peripheral Facial Nerve Palsy Following BNT162b2 (COVID-19) Vaccination. Isr. Med. Assoc. J. IMAJ 2021, 23, 143–144. [Google Scholar]
- Renoud, L.; Khouri, C.; Revol, B.; Lepelley, M.; Perez, J.; Roustit, M.; Cracowski, J.L. Association of Facial Paralysis With mRNA COVID-19 Vaccines: A Disproportionality Analysis Using the World Health Organization Pharmacovigilance Database. JAMA Intern. Med. 2021, 181, 1243–1245. [Google Scholar] [CrossRef]
- Albakri, K.; Khaity, A.; Atwan, H.; Saleh, O.; Al-Hajali, M.; Cadri, S.; Diab, R.A.; Albazee, E.; Negida, A. Bell’s Palsy and COVID-19 Vaccines: A Systematic Review and Meta-Analysis. Vaccines 2023, 11, 236. [Google Scholar] [CrossRef]
- Sato, K.; Mano, T.; Niimi, Y.; Toda, T.; Iwata, A.; Iwatsubo, T. Facial nerve palsy following the administration of COVID-19 mRNA vaccines: Analysis of a self-reporting database. Int. J. Infect. Dis. 2021, 111, 310–312. [Google Scholar] [CrossRef]
- Shemer, A.; Pras, E.; Einan-Lifshitz, A.; Dubinsky-Pertzov, B.; Hecht, I. Association of COVID-19 Vaccination and Facial Nerve Palsy: A Case-Control Study. JAMA Otolaryngol.-Head Neck Surg. 2021, 147, 739–743. [Google Scholar] [CrossRef]
- Alkhalifah, J.M.; Al Seraihi, A.; Al-Tawfiq, J.A.; Alshehri, B.F.; Alhaluli, A.H.; Alsulais, N.M.; Alessa, M.M.; Seddiq, W.; Aljeri, T.; Qahtani, M.H.; et al. Pattern of self-reported adverse events related to COVID-19 vaccines in Saudi Arabia: A nationwide study. Front. Public Health 2023, 11, 1043696. [Google Scholar] [CrossRef]
- Lahoz Fernandez, P.E.; Miranda Pereira, J.; Fonseca Risso, I.; Baleeiro Rodrigues Silva, P.; Freitas Barboza, I.C.; Vieira Silveira, C.G.; Diogo Silva, G.; Marzorati Kuntz Puglia, P.; Genaro Mutarelli, E. Guillain-Barre syndrome following COVID-19 vaccines: A scoping review. Acta Neurol. Scand. 2022, 145, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Abolmaali, M.; Rezania, F.; Behnagh, A.K.; Hamidabad, N.M.; Gorji, A.; Mirzaasgari, Z. Guillain-Barré syndrome in association with COVID-19 vaccination: A systematic review. Immunol. Res. 2022, 70, 752–764. [Google Scholar] [CrossRef] [PubMed]
- Finsterer, J.; Scorza, F.A.; Scorza, C.A. Post SARS-CoV-2 vaccination Guillain-Barre syndrome in 19 patients. Clinics 2021, 76, e3286. [Google Scholar] [CrossRef] [PubMed]
- García-Grimshaw, M.; Michel-Chávez, A.; Vera-Zertuche, J.M.; Galnares-Olalde, J.A.; Hernández-Vanegas, L.E.; Figueroa-Cucurachi, M.; Paredes-Ceballos, O.; Reyes-Terán, G.; Carbajal-Sandoval, G.; Ceballos-Liceaga, S.E.; et al. Guillain-Barré syndrome is infrequent among recipients of the BNT162b2 mRNA COVID-19 vaccine. Clin. Immunol. 2021, 230, 108818. [Google Scholar] [CrossRef]
- Tondo, G.; Virgilio, E.; Naldi, A.; Bianchi, A.; Comi, C. Safety of COVID-19 Vaccines: Spotlight on Neurological Complications. Life 2022, 12, 1338. [Google Scholar] [CrossRef]
- Germano, F.; Bellucci, M.; Grisanti, S.; Beronio, A.; Grazzini, M.; Coco, E.; Tassinari, T.; Della Cava, F.; De Michelis, C.; Baldi, O.; et al. COVID-19 vaccine-related Guillain-Barré syndrome in the Liguria region of Italy: A multicenter case series. J. Neurol. Sci. 2022, 440, 120330. [Google Scholar] [CrossRef]
- Ha, J.; Park, S.; Kang, H.; Kyung, T.; Kim, N.; Kim, D.K.; Kim, H.; Bae, K.; Song, M.C.; Lee, K.J.; et al. Real-world data on the incidence and risk of Guillain-Barré syndrome following SARS-CoV-2 vaccination: A prospective surveillance study. Sci. Rep. 2023, 13, 3773. [Google Scholar] [CrossRef]
- Yu, M.; Nie, S.; Qiao, Y.; Ma, Y. Guillain-Barre syndrome following COVID-19 vaccines: A review of literature. Front. Immunol. 2023, 14, 1078197. [Google Scholar] [CrossRef]
- Li, X.; Ostropolets, A.; Makadia, R.; Shoaibi, A.; Rao, G.; Sena, A.G.; Martinez-Hernandez, E.; Delmestri, A.; Verhamme, K.; Rijnbeek, P.R.; et al. Characterising the background incidence rates of adverse events of special interest for COVID-19 vaccines in eight countries: Multinational network cohort study. BMJ 2021, 373, n1435. [Google Scholar] [CrossRef]
- Hanson, K.E.; Goddard, K.; Lewis, N.; Fireman, B.; Myers, T.R.; Bakshi, N.; Weintraub, E.; Donahue, J.G.; Nelson, J.C.; Xu, S.; et al. Incidence of Guillain-Barré Syndrome After COVID-19 Vaccination in the Vaccine Safety Datalink. JAMA Netw. Open 2022, 5, e228879. [Google Scholar] [CrossRef]
- Atzenhoffer, M.; Auffret, M.; Pegat, A.; Masmoudi, K.; Khouri, C.; Bertin, B.; Vial, T. Guillain-Barré Syndrome Associated with COVID-19 Vaccines: A Perspective From Spontaneous Report Data. Clin. Drug Investig. 2022, 42, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Shao, S.C.; Wang, C.H.; Chang, K.C.; Hung, M.J.; Chen, H.Y.; Liao, S.C. Guillain-Barré Syndrome Associated with COVID-19 Vaccination. Emerg. Infect. Dis. 2021, 27, 3175–3178. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Kim, J.E.; Yoon, B.A.; Kim, J.K.; Bae, J.S. Bilateral Facial Weakness with Distal Paresthesia Following COVID-19 Vaccination: A Scoping Review for an Atypical Variant of Guillain-Barré Syndrome. Brain Sci. 2022, 12, 1046. [Google Scholar] [CrossRef] [PubMed]
- Chua, S.K.K.; Soh, Q.Y.; Saffari, S.E.; Tan, E.K. Prognosis of Guillain-Barré Syndrome Linked to COVID-19 Vaccination. Brain Sci. 2022, 12, 711. [Google Scholar] [CrossRef]
- Gupta, A.; Ranga, A.; Prakash, N.B.; Khanna, M. Rehabilitation outcomes in patients with post-COVID-19 vaccine-associated Guillain-Barre syndrome. J. Neurosci. Rural Pract. 2022, 13, 684–690. [Google Scholar] [CrossRef]
- Pritchard, J.; Mukherjee, R.; Hughes, R.A. Risk of relapse of Guillain-Barré syndrome or chronic inflammatory demyelinating polyradiculoneuropathy following immunisation. J. Neurol. Neurosurg. Psychiatry 2002, 73, 348–349. [Google Scholar] [CrossRef] [Green Version]
- Baars, A.E.; Kuitwaard, K.; de Koning, L.C.; Luijten, L.W.G.; Kok, W.M.; Eftimov, F.; Wieske, L.; Goedee, H.S.; van der Pol, W.L.; Blomkwist-Markens, P.H.; et al. SARS-CoV-2 Vaccination Safety in Guillain-Barré Syndrome, Chronic Inflammatory Demyelinating Polyneuropathy, and Multifocal Motor Neuropathy. Neurology 2023, 100, e182–e191. [Google Scholar] [CrossRef]
- Kim, J.E.; Yoon, B.A.; Kim, Y.H.; Kim, J.K.; Bae, J.S. Miller Fisher syndrome following COVID-19 vaccines: A scoping review. Acta Neurol. Scand. 2022, 146, 604–609. [Google Scholar] [CrossRef]
- Nishiguchi, Y.; Matsuyama, H.; Maeda, K.; Shindo, A.; Tomimoto, H. Miller Fisher syndrome following BNT162b2 mRNA coronavirus 2019 vaccination. BMC Neurol. 2021, 21, 452. [Google Scholar] [CrossRef]
- Siddiqi, A.R.; Khan, T.; Tahir, M.J.; Asghar, M.S.; Islam, M.S.; Yousaf, Z. Miller Fisher syndrome after COVID-19 vaccination: Case report and review of literature. Medicine 2022, 101, e29333. [Google Scholar] [CrossRef]
- Doron, A.; Piura, Y.; Vigiser, I.; Kolb, H.; Regev, K.; Nesher, N.; Karni, A. BNT162b2 mRNA COVID-19 vaccine three-dose safety and risk of COVID-19 in patients with myasthenia gravis during the alpha, delta, and omicron waves. J. Neurol. 2022, 269, 6193–6201. [Google Scholar] [CrossRef]
- Mirmosayyeb, O.; Moases Ghaffary, E.; Mazdak, M.; Bagheri, Z.; Bagherieh, S.; Shaygannejad, V. Is Myasthenia Gravis a Real Complication of the COVID-19 Vaccine? A Case Report-Based Systematic Review. Can. J. Infect. Dis. Med. Microbiol. J. Can. Mal. Infect. Microbiol. Med. 2022, 2022, 5009450. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Z.; Tang, Y.; Li, C.; Sun, C.; Zhu, Y.; Li, Z.; Chang, T. COVID-19 Vaccination in Patients with Myasthenia Gravis: A Single-Center Case Series. Vaccines 2021, 9, 1112. [Google Scholar] [CrossRef] [PubMed]
- Maher, D.I.; Hogarty, D.; Ben Artsi, E. Acute onset ocular myasthenia gravis after vaccination with the Oxford-AstraZeneca COVID-19 vaccine. Orbit 2022, 1–5. [Google Scholar] [CrossRef]
- Ishizuchi, K.; Takizawa, T.; Sekiguchi, K.; Motegi, H.; Oyama, M.; Nakahara, J.; Suzuki, S. Flare of myasthenia gravis induced by COVID-19 vaccines. J. Neurol. Sci. 2022, 436, 120225. [Google Scholar] [CrossRef]
- Lotan, I.; Hellmann, M.A.; Friedman, Y.; Stiebel-Kalish, H.; Steiner, I.; Wilf-Yarkoni, A. Early safety and tolerability profile of the BNT162b2 COVID-19 vaccine in myasthenia gravis. Neuromuscul. Disord. NMD 2022, 32, 230–235. [Google Scholar] [CrossRef]
- Lee, M.A.; Lee, C.; Park, J.H.; Lee, J.H. Early-Onset Myasthenia Gravis Following COVID-19 Vaccination. J. Korean Med. Sci. 2022, 37, e50. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.S.; Hoe, R.H.M.; Chen, G.J.; Goh, Y.; Tan, B.Y.Q.; Yong, M.H.; Hui, A.C.; Tu, T.M.; Yong, K.P.; Angon, J.; et al. Low incidence of neurological recurrent side-effects following COVID-19 reimmunization. QJM Mon. J. Assoc. Physicians 2023, 116, 221–226. [Google Scholar] [CrossRef]
- Tagliaferri, A.R.; Narvaneni, S.; Azzam, M.H.; Grist, W. A Case of COVID-19 Vaccine Causing a Myasthenia Gravis Crisis. Cureus 2021, 13, e15581. [Google Scholar] [CrossRef]
- Sonigra, K.J.; Sarna, K.; Vaghela, V.P.; Guthua, S. An Interesting Case of Fatal Myasthenic Crisis Probably Induced by the COVID-19 Vaccine. Cureus 2022, 14, e23251. [Google Scholar] [CrossRef]
- Camelo-Filho, A.E.; Silva, A.M.S.; Estephan, E.P.; Zambon, A.A.; Mendonça, R.H.; Souza, P.V.S.; Pinto, W.; Oliveira, A.S.B.; Dangoni-Filho, I.; Pouza, A.F.P.; et al. Myasthenia Gravis and COVID-19: Clinical Characteristics and Outcomes. Front. Neurol. 2020, 11, 1053. [Google Scholar] [CrossRef] [PubMed]
- Elnahry, A.G.; Asal, Z.B.; Shaikh, N.; Dennett, K.; Abd Elmohsen, M.N.; Elnahry, G.A.; Shehab, A.; Vytopil, M.; Ghaffari, L.; Athappilly, G.K.; et al. Optic neuropathy after COVID-19 vaccination: A report of two cases. Int. J. Neurosci. 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Huang, S.; Yu, Z.; Zhang, S.; Hou, G.; Xu, S. Unilateral optic neuritis after vaccination against the coronavirus disease: Two case reports. Doc. Ophthalmol. Adv. Ophthalmol. 2022, 145, 65–70. [Google Scholar] [CrossRef] [PubMed]
- García-Estrada, C.; Gómez-Figueroa, E.; Alban, L.; Arias-Cárdenas, A. Optic neuritis after COVID-19 vaccine application. Clin. Exp. Neuroimmunol. 2022, 13, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Motegi, S.; Kanda, T.; Takeuchi, M. A Case of Atypical Unilateral Optic Neuritis Following BNT162b2 mRNA COVID-19 Vaccination. Vaccines 2022, 10, 1574. [Google Scholar] [CrossRef]
- Lee, G.W.; Park, H.S.; Lee, D. Silent progressive bilateral papillitis after COVID-19 vaccination: A case report. Medicine 2022, 101, e31112. [Google Scholar] [CrossRef]
- Shah, P.P.; Gelnick, S.; Zhu, D.; Wong, A.; Verma, R. Optic neuritis secondary to the Pfizer-BioNTech-162b2 COVID-19 vaccine managed with plasmapheresis: A case report and review. Oman J. Ophthalmol. 2022, 15, 397–402. [Google Scholar]
- Kim, J.E.; Park, J.; Song, T.J. A disproportionality analysis for the association of central nervous system demyelinating diseases with COVID-19 vaccination using the World Health Organization pharmacovigilance database. Mult. Scler. 2022, 28, 2112–2123. [Google Scholar] [CrossRef]
- Gao, J.J.; Tseng, H.P.; Lin, C.L.; Shiu, J.S.; Lee, M.H.; Liu, C.H. Acute Transverse Myelitis Following COVID-19 Vaccination. Vaccines 2021, 9, 1008. [Google Scholar] [CrossRef]
- Ostovan, V.R.; Sahraian, M.A.; Karazhian, N.; Rostamihosseinkhani, M.; Salimi, M.; Marbooti, H. Clinical characteristics, radiological features and prognostic factors of transverse myelitis following COVID-19 vaccination: A systematic review. Mult. Scler. Relat. Disord. 2022, 66, 104032. [Google Scholar] [CrossRef]
- Ismail, I.I.; Salama, S. A systematic review of cases of CNS demyelination following COVID-19 vaccination. J. Neuroimmunol. 2022, 362, 577765. [Google Scholar] [CrossRef] [PubMed]
- Erdem, N.; Demirci, S.; Özel, T.; Mamadova, K.; Karaali, K.; Çelik, H.T.; Uslu, F.I.; Özkaynak, S.S. Acute transverse myelitis after inactivated COVID-19 vaccine. Ideggyogy. Szle. 2021, 74, 273–276. [Google Scholar] [CrossRef] [PubMed]
- Román, G.C.; Gracia, F.; Torres, A.; Palacios, A.; Gracia, K.; Harris, D. Acute Transverse Myelitis (ATM):Clinical Review of 43 Patients With COVID-19-Associated ATM and 3 Post-Vaccination ATM Serious Adverse Events With the ChAdOx1 nCoV-19 Vaccine (AZD1222). Front. Immunol. 2021, 12, 653786. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.K.; Paliwal, V.K. Spectrum of neurological complications following COVID-19 vaccination. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2022, 43, 3–40. [Google Scholar] [CrossRef]
- Khan, E.; Shrestha, A.K.; Colantonio, M.A.; Liberio, R.N.; Sriwastava, S. Acute transverse myelitis following SARS-CoV-2 vaccination: A case report and review of literature. J. Neurol. 2022, 269, 1121–1132. [Google Scholar] [CrossRef]
- Maramattom, B.V.; Lotlikar, R.S.; Sukumaran, S. Central nervous system adverse events after ChAdOx1 vaccination. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2022, 43, 3503–3507. [Google Scholar] [CrossRef]
- Gustavsen, S.; Nordling, M.M.; Weglewski, A. Acute disseminated encephalomyelitis following the COVID-19 vaccine Ad26.COV2.S, a case report. Bull. Natl. Res. Cent. 2023, 47, 5. [Google Scholar] [CrossRef]
- Rinaldi, V.; Bellucci, G.; Buscarinu, M.C.; Reniè, R.; Marrone, A.; Nasello, M.; Zancan, V.; Nistri, R.; Palumbo, R.; Salerno, A.; et al. CNS inflammatory demyelinating events after COVID-19 vaccines: A case series and systematic review. Front. Neurol. 2022, 13, 1018785. [Google Scholar] [CrossRef]
- Permezel, F.; Borojevic, B.; Lau, S.; de Boer, H.H. Acute disseminated encephalomyelitis (ADEM) following recent Oxford/AstraZeneca COVID-19 vaccination. Forensic Sci. Med. Pathol. 2022, 18, 74–79. [Google Scholar] [CrossRef]
- Netravathi, M.; Dhamija, K.; Gupta, M.; Tamborska, A.; Nalini, A.; Holla, V.V.; Nitish, L.K.; Menon, D.; Pal, P.K.; Seena, V.; et al. COVID-19 vaccine associated demyelination & its association with MOG antibody. Mult. Scler. Relat. Disord. 2022, 60, 103739. [Google Scholar] [CrossRef]
- Poli, K.; Poli, S.; Ziemann, U. Multiple Autoimmune Syndromes Including Acute Disseminated Encephalomyelitis, Myasthenia Gravis, and Thyroiditis Following Messenger Ribonucleic Acid-Based COVID-19 Vaccination: A Case Report. Front. Neurol. 2022, 13, 913515. [Google Scholar] [CrossRef]
- Bastide, L.; Perrotta, G.; Lolli, V.; Mathey, C.; Vierasu, O.I.; Goldman, S.; Vandergheynst, F. Atypical acute disseminated encephalomyelitis with systemic inflammation after a first dose of AztraZaneca COVID-19 vaccine. A case report. Front. Neurol. 2022, 13, 995875. [Google Scholar] [CrossRef] [PubMed]
- Hada, M.; Mosholder, A.D.; Leishear, K.; Perez-Vilar, S. Systematic review of risk of SARS-CoV-2 infection and severity of COVID-19 with therapies approved to treat multiple sclerosis. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2022, 43, 1557–1567. [Google Scholar] [CrossRef] [PubMed]
- Nojszewska, M.; Kalinowska, A.; Adamczyk-Sowa, M.; Kułakowska, A.; Bartosik-Psujek, H. COVID-19 mRNA vaccines (Pfizer-BioNTech and Moderna) in patients with multiple sclerosis: A statement by a working group convened by the Section of Multiple Sclerosis and Neuroimmunology of the Polish Neurological Society. Neurol. I Neurochir. Pol. 2021, 55, 8–11. [Google Scholar] [CrossRef]
- Yamout, B.I.; Zakaria, M.; Inshasi, J.; Al-Jumah, M.; Zeineddine, M.; Dahdaleh, M.; Bohlega, S.; Gouider, R.; Alroughani, R. MENACTRIMS practice guideline for COVID-19 vaccination in patients with multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 56, 103225. [Google Scholar] [CrossRef]
- Fujimori, J.; Miyazawa, K.; Nakashima, I. Initial clinical manifestation of multiple sclerosis after immunization with the Pfizer-BioNTech COVID-19 vaccine. J. Neuroimmunol. 2021, 361, 577755. [Google Scholar] [CrossRef]
- Nabizadeh, F.; Ramezannezhad, E.; Kazemzadeh, K.; Khalili, E.; Ghaffary, E.M.; Mirmosayyeb, O. Multiple sclerosis relapse after COVID-19 vaccination: A case report-based systematic review. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2022, 104, 118–125. [Google Scholar] [CrossRef]
- Koch-Henriksen, N.; Thygesen, L.C.; Stenager, E.; Laursen, B.; Magyari, M. Incidence of MS has increased markedly over six decades in Denmark particularly with late onset and in women. Neurology 2018, 90, e1954–e1963. [Google Scholar] [CrossRef]
- Murtonen, A.; Sumelahti, M.L. Multiple sclerosis prevalence in 2000 and 2010 in Western Finland. Acta Neurol. Scand. 2020, 141, 311–318. [Google Scholar] [CrossRef]
- Magyari, M.; Sorensen, P.S. The changing course of multiple sclerosis: Rising incidence, change in geographic distribution, disease course, and prognosis. Curr. Opin. Neurol. 2019, 32, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Khayat-Khoei, M.; Bhattacharyya, S.; Katz, J.; Harrison, D.; Tauhid, S.; Bruso, P.; Houtchens, M.K.; Edwards, K.R.; Bakshi, R. COVID-19 mRNA vaccination leading to CNS inflammation: A case series. J. Neurol. 2022, 269, 1093–1106. [Google Scholar] [CrossRef]
- Toljan, K.; Amin, M.; Kunchok, A.; Ontaneda, D. New diagnosis of multiple sclerosis in the setting of mRNA COVID-19 vaccine exposure. J. Neuroimmunol. 2022, 362, 577785. [Google Scholar] [CrossRef] [PubMed]
- Achiron, A.; Dolev, M.; Menascu, S.; Zohar, D.N.; Dreyer-Alster, S.; Miron, S.; Shirbint, E.; Magalashvili, D.; Flechter, S.; Givon, U.; et al. COVID-19 vaccination in patients with multiple sclerosis: What we have learnt by February 2021. Mult. Scler. 2021, 27, 864–870. [Google Scholar] [CrossRef]
- Kavosh, A.; Ashtari, F.; Naghavi, S.; Adibi, I.; Shaygannejad, V.; Karimi, Z.; Arabi, S.; Rahimi, M.; Mazaheri, S. Safety of Sinopharm vaccine for people with Multiple Sclerosis: Study of adverse reactions and disease activity. Mult. Scler. Relat. Disord. 2022, 61, 103708. [Google Scholar] [CrossRef] [PubMed]
- Paybast, S.; Emami, A.; Baghalha, F.; Naser Moghadasi, A. Watch out for neuromyelitis optica spectrum disorder onset or clinical relapse after COVID-19 vaccination: What neurologists need to know? Mult. Scler. Relat. Disord. 2022, 65, 103960. [Google Scholar] [CrossRef]
- Shirah, B.; Mulla, I.; Aladdin, Y. Optic Neuritis Following the BNT162b2 mRNA COVID-19 Vaccine in a Patient with Systemic Lupus Erythematosus Uncovering the Diagnosis of Neuromyelitis Optica Spectrum Disorders. Ocul. Immunol. Inflamm. 2022, 1–3. [Google Scholar] [CrossRef]
- Motahharynia, A.; Naghavi, S.; Shaygannejad, V.; Adibi, I. Fulminant neuromyelitis optica spectrum disorder (NMOSD) following COVID-19 vaccination: A need for reconsideration? Mult. Scler. Relat. Disord. 2022, 66, 104035. [Google Scholar] [CrossRef]
- Mealy, M.A.; Cook, L.J.; Pache, F.; Velez, D.L.; Borisow, N.; Becker, D.; Arango, J.A.J.; Paul, F.; Levy, M. Vaccines and the association with relapses in patients with neuromyelitis optica spectrum disorder. Mult. Scler. Relat. Disord. 2018, 23, 78–82. [Google Scholar] [CrossRef] [Green Version]
- Samim, M.M.; Dhar, D.; Goyal, S.; Dey, T.; Parvin, N.; Shah, R.D.; Singh, V.; Chowdhury, S.; Lal, B.M.; Varghese, N.; et al. AI-CoV Study: Autoimmune Encephalitis Associated with COVID-19 and Its Vaccines—A Systematic Review. J. Clin. Neurol. 2022, 18, 692–710. [Google Scholar] [CrossRef]
- Zlotnik, Y.; Gadoth, A.; Abu-Salameh, I.; Horev, A.; Novoa, R.; Ifergane, G. Case Report: Anti-LGI1 Encephalitis Following COVID-19 Vaccination. Front. Immunol. 2021, 12, 813487. [Google Scholar] [CrossRef] [PubMed]
- Abu-Abaa, M.; Dawood, G.; Arshad, H.; Jumaah, O.; Landau, D. A Possible Case of Autoimmune Encephalitis After mRNA COVID-19 Booster Vaccine: A Case Report. Cureus 2022, 14, e31118. [Google Scholar] [CrossRef]
- Huang, Y.F.; Ho, T.C.; Chang, C.C.; Shen, D.H.; Chan, H.P.; Chuang, K.P.; Tyan, Y.C.; Yang, M.H. A Rare Adverse Effect of the COVID-19 Vaccine on Autoimmune Encephalitis. Vaccines 2022, 10, 1114. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Guo, K.; Lu, L.; Luo, R.; Liu, J.; Zhou, D.; Hong, Z. Safety of inactivated COVID-19 vaccines in autoimmune encephalitis: A real-world cross-sectional survey. Mult. Scler. Relat. Disord. 2022, 70, 104495. [Google Scholar] [CrossRef]
- Mastropaolo, M.; Hasbani, M.J. Small Fiber Neuropathy Triggered by COVID-19 Vaccination: Association with FGFR3 Autoantibodies and Improvement during Intravenous Immunoglobulin Treatment. Case Rep. Neurol. 2023, 15, 6–10. [Google Scholar] [CrossRef]
- Schelke, M.W.; Barcavage, S.; Lampshire, E.; Brannagan, T.H., 3rd. Post-COVID-19 vaccine small-fiber neuropathy and tinnitus treated with plasma exchange. Muscle Nerve 2022, 66, E21–E23. [Google Scholar] [CrossRef]
- Trevino, J.A.; Novak, P. TS-HDS and FGFR3 antibodies in small fiber neuropathy and Dysautonomia. Muscle Nerve 2021, 64, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; De Marco, G.; Mahajna, H.; Druyan, A.; Eltity, M.; Hijazi, N.; Haddad, A.; Elias, M.; Zisman, D.; Naffaa, M.E.; et al. Immune-Mediated Disease Flares or New-Onset Disease in 27 Subjects Following mRNA/DNA SARS-CoV-2 Vaccination. Vaccines 2021, 9, 435. [Google Scholar] [CrossRef]
- Waheed, W.; Carey, M.E.; Tandan, S.R.; Tandan, R. Post COVID-19 vaccine small fiber neuropathy. Muscle Nerve 2021, 64, E1–E2. [Google Scholar] [CrossRef]
- Fathy, R.A.; McMahon, D.E.; Lee, C.; Chamberlin, G.C.; Rosenbach, M.; Lipoff, J.B.; Tyagi, A.; Desai, S.R.; French, L.E.; Lim, H.W.; et al. Varicella-zoster and herpes simplex virus reactivation post-COVID-19 vaccination: A review of 40 cases in an International Dermatology Registry. J. Eur. Acad. Dermatol. Venereol. JEADV 2022, 36, e6–e9. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Psichogiou, M.; Samarkos, M.; Mikos, N.; Hatzakis, A. Reactivation of Varicella Zoster Virus after Vaccination for SARS-CoV-2. Vaccines 2021, 9, 572. [Google Scholar] [CrossRef] [PubMed]
- Hertel, M.; Heiland, M.; Nahles, S.; von Laffert, M.; Mura, C.; Bourne, P.E.; Preissner, R.; Preissner, S. Real-world evidence from over one million COVID-19 vaccinations is consistent with reactivation of the varicella-zoster virus. J. Eur. Acad. Dermatol. Venereol. JEADV 2022, 36, 1342–1348. [Google Scholar] [CrossRef]
- Rodríguez-Jiménez, P.; Chicharro, P.; Cabrera, L.M.; Seguí, M.; Morales-Caballero, Á.; Llamas-Velasco, M.; Sánchez-Pérez, J. Varicella-zoster virus reactivation after SARS-CoV-2 BNT162b2 mRNA vaccination: Report of 5 cases. JAAD Case Rep. 2021, 12, 58–59. [Google Scholar] [CrossRef] [PubMed]
- Katsikas Triantafyllidis, K.; Giannos, P.; Mian, I.T.; Kyrtsonis, G.; Kechagias, K.S. Varicella Zoster Virus Reactivation Following COVID-19 Vaccination: A Systematic Review of Case Reports. Vaccines 2021, 9, 1013. [Google Scholar] [CrossRef]
- Wan, E.Y.F.; Chui, C.S.L.; Wang, Y.; Ng, V.W.S.; Yan, V.K.C.; Lai, F.T.T.; Li, X.; Wong, C.K.H.; Chan, E.W.Y.; Wong, C.S.M.; et al. Herpes zoster related hospitalization after inactivated (CoronaVac) and mRNA (BNT162b2) SARS-CoV-2 vaccination: A self-controlled case series and nested case-control study. Lancet Reg. Health West. Pac. 2022, 21, 100393. [Google Scholar] [CrossRef]
- Shahrudin, M.S.; Mohamed-Yassin, M.S.; Nik Mohd Nasir, N.M. Herpes Zoster Following COVID-19 Vaccine Booster. Am. J. Case Rep. 2023, 24, e938667. [Google Scholar] [CrossRef]
- Préta, L.H.; Contejean, A.; Salvo, F.; Treluyer, J.M.; Charlier, C.; Chouchana, L. Association study between herpes zoster reporting and mRNA COVID-19 vaccines (BNT162b2 and mRNA-1273). Br. J. Clin. Pharmacol. 2022, 88, 3529–3534. [Google Scholar] [CrossRef]
- Chen, J.; Li, F.; Tian, J.; Xie, X.; Tang, Q.; Chen, Y.; Ge, Y. Varicella zoster virus reactivation following COVID-19 vaccination in patients with autoimmune inflammatory rheumatic diseases: A cross-sectional Chinese study of 318 cases. J. Med. Virol. 2023, 95, e28307. [Google Scholar] [CrossRef] [PubMed]
- May Lee, M.; Macchi, S.; Mora, E.; Feliciani, C. Potential risk factors for Varicella-zoster virus reactivation after COVID-19 vaccination. J. Cosmet. Dermatol. 2022, 21, 1347–1349. [Google Scholar] [CrossRef]
- Butler, M.; Coebergh, J.; Safavi, F.; Carson, A.; Hallett, M.; Michael, B.; Pollak, T.A.; Solomon, T.; Stone, J.; Nicholson, T.R. Functional Neurological Disorder After SARS-CoV-2 Vaccines: Two Case Reports and Discussion of Potential Public Health Implications. J. Neuropsychiatry Clin. Neurosci. 2021, 33, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Ercoli, T.; Lutzoni, L.; Orofino, G.; Muroni, A.; Defazio, G. Functional neurological disorder after COVID-19 vaccination. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2021, 42, 3989–3990. [Google Scholar] [CrossRef]
- Espay, A.J.; Aybek, S.; Carson, A.; Edwards, M.J.; Goldstein, L.H.; Hallett, M.; LaFaver, K.; LaFrance, W.C., Jr.; Lang, A.E.; Nicholson, T.; et al. Current Concepts in Diagnosis and Treatment of Functional Neurological Disorders. JAMA Neurol. 2018, 75, 1132–1141. [Google Scholar] [CrossRef]
- Fasano, A.; Daniele, A. Functional disorders after COVID-19 vaccine fuel vaccination hesitancy. J. Neurol. Neurosurg. Psychiatry 2022, 93, 339–340. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, O.; Sakakibara, R.; Sawai, S.; Ogata, T. Functional neurological disorders after COVID-19 vaccination: Case series and literature review. Psychiatry Clin. Neurosci. 2022, 76, 529–531. [Google Scholar] [CrossRef] [PubMed]
- de Souza, A.; Jacques, R.; Mohan, S. Vaccine-Induced Functional Neurological Disorders in the COVID-19 Era. Can. J. Neurol. Sci. J. Can. Sci. Neurol. 2022, 50, 346–350. [Google Scholar] [CrossRef]
- Alonso-Canovas, A.; Kurtis, M.M.; Gomez-Mayordomo, V.; Macías-García, D.; Gutiérrez Viedma, Á.; Mondragón Rezola, E.; Pagonabarraga, J.; Aranzabal Orgaz, L.; Masjuan, J.; Martinez-Castrillo, J.C.; et al. Functional neurological disorders after COVID-19 and SARS-CoV-2 vaccines: A national multicentre observational study. J. Neurol. Neurosurg. Psychiatry, 2023; online first. [Google Scholar] [CrossRef]
- Linden, S.C.; Carson, A.J.; Wessely, S. Functional neurological disorder after vaccination: A balanced approach informed by history. J. R. Coll. Physicians Edinb. 2021, 51, 330–331. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Neurological disorders following COVID-19 vaccination: CVST cranial venous sinus thrombosis; IS ischemic stroke; HS hemorrhagic stroke; ADEM acute disseminated encephalomyelitis; ATM acute transverse myelitis; MS multiple sclerosis; GBS Guillain–Barre syndrome; MFS Miller–Fisher syndrome; NMOSD neuromyelitis optica spectrum disorder; ON optic neuritis; AE autoimmune encephalitis; MG myasthenia gravis; SFN small fiber neuropathy; BP Bell’s palsy; HVR herpes virus reactivation; FND functional neurological disorder.
Figure 1.
Neurological disorders following COVID-19 vaccination: CVST cranial venous sinus thrombosis; IS ischemic stroke; HS hemorrhagic stroke; ADEM acute disseminated encephalomyelitis; ATM acute transverse myelitis; MS multiple sclerosis; GBS Guillain–Barre syndrome; MFS Miller–Fisher syndrome; NMOSD neuromyelitis optica spectrum disorder; ON optic neuritis; AE autoimmune encephalitis; MG myasthenia gravis; SFN small fiber neuropathy; BP Bell’s palsy; HVR herpes virus reactivation; FND functional neurological disorder.


{kind=link}
Table 1.
Clinical characteristics of VITT-CVST and non-VITT-CVST following COVID-19 vaccination.
| VITT-CVST | Non-VITT-CVST | |
|---|---|---|
| Age | Younger | Older |
| Vaccine type | Adenoviral vector-based vaccines | Non-vector-based vaccines |
| Onset time | Shorter interval | Longer interval |
| Thrombocytopenia | Yes | Usually no |
| PF4 antibodies assay | Usually positive | Negative |
| D-dimer | Higher than 2000 μg/L | Lower than 2000 μg/L |
| Other risk factors for thromboses | Usually absent | Usually present |
| Intracerebral hemorrhage | More common | Less common |
| Thromboses in other sites | More common | Less common |
| Mortality | Higher | Lower |
| Treatment | Non-heparin anticoagulants and IVIG | Heparin anticoagulants |
Table 2.
Clinical characteristics of Guillain–Barre syndrome and Miller–Fisher syndrome following COVID-19 vaccination.
Table 2.
Clinical characteristics of Guillain–Barre syndrome and Miller–Fisher syndrome following COVID-19 vaccination.
| Guillain–Barre Syndrome | Miller–Fisher Syndrome | |
|---|---|---|
| Vaccine type | Most adenoviral vector-based vaccines | Various kinds of vaccines |
| Anti-ganglioside antibodies | Usually absent | Usually present |
| Respiratory muscle involvement | More frequent | Less frequent |
| Treatment | IVIG, plasma exchange | Usually IVIG only |
| Prognosis | Various | Good |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Yang, Y.; Huang, L. Neurological Disorders following COVID-19 Vaccination. Vaccines 2023, 11, 1114. https://doi.org/10.3390/vaccines11061114
AMA Style
Yang Y, Huang L. Neurological Disorders following COVID-19 Vaccination. Vaccines. 2023; 11(6):1114. https://doi.org/10.3390/vaccines11061114
Chicago/Turabian StyleYang, Ying, and Lisu Huang. 2023. "Neurological Disorders following COVID-19 Vaccination" Vaccines 11, no. 6: 1114. https://doi.org/10.3390/vaccines11061114
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.