


Impact of Influenza Vaccination on the Burden of Severe Influenza in the Elderly: Spain, 2017–2020

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Study Settings and Study Population
2.2. Influenza Hospitalization and ICU rates
2.3. Impact of the Influenza Vaccination Program in the Elderly
2.4. Input Data for the Estimation of Vaccination Impact
3. Results
3.1. Burden of Severe Influenza in Spain
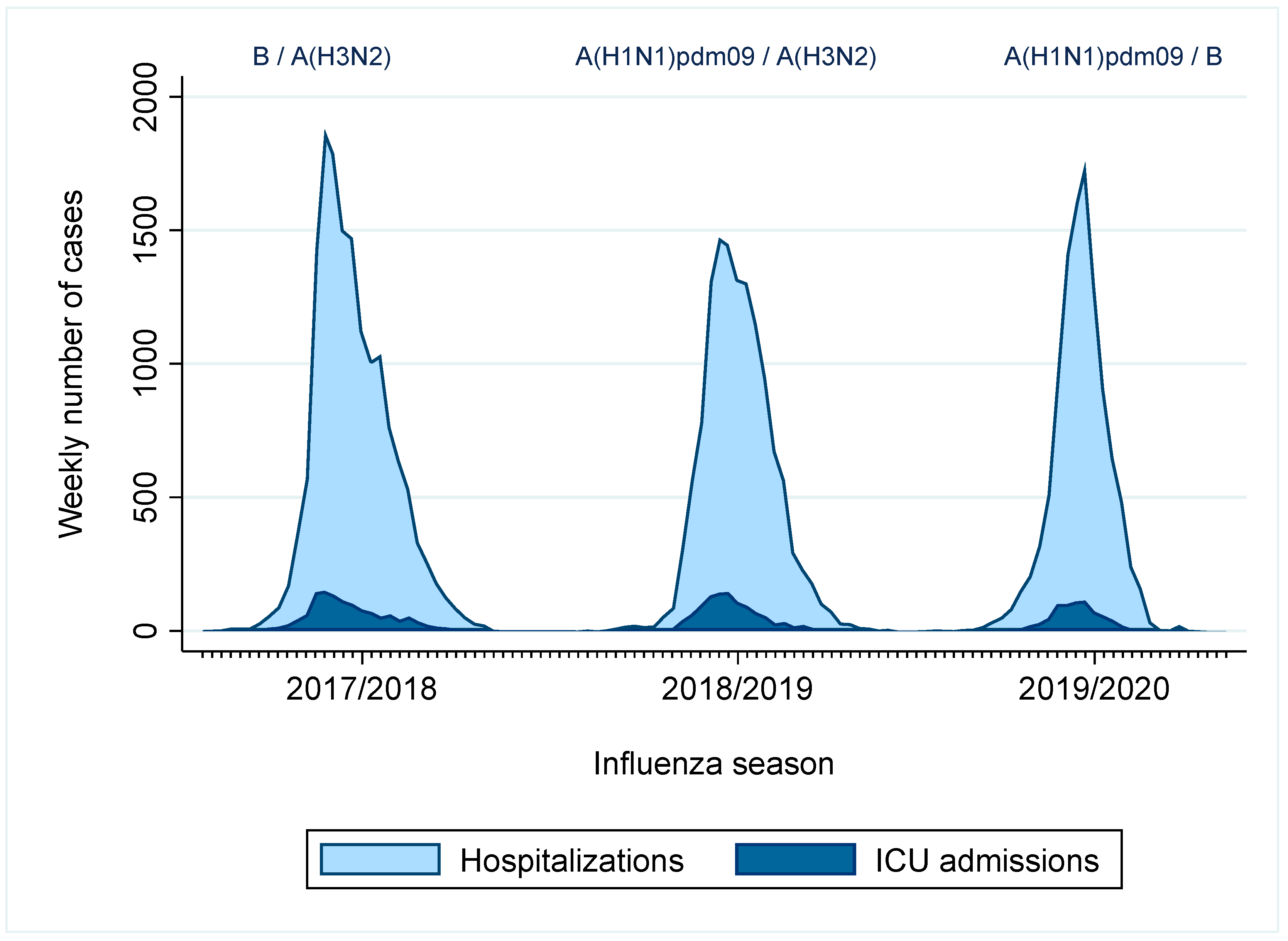
3.1.1. Cases Reported to the Spanish Influenza Hospitalization Surveillance System
3.1.2. Estimated Burden of Influenza Hospitalizations and ICU Admissions in the Spanish Population
3.1.3. Estimated Number of Influenza Hospitalizations and ICU Admissions, IVE Estimates and Influenza VC in the Elderly
3.2. Impact of Influenza Vaccination in the Elderly
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lafond, K.E.; Porter, R.M.; Whaley, M.J.; Suizan, Z.; Ran, Z.; Aleem, M.A.; Thapa, B.; Sar, B.; Proschle, V.S.; Peng, Z.; et al. Global Burden of Influenza-Associated Lower Respiratory Tract Infections and Hospitalizations among Adults: A Systematic Review and Meta-Analysis. PLoS Med. 2021, 18, e1003550. [Google Scholar] [CrossRef] [PubMed]
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of Global Seasonal Influenza-Associated Respiratory Mortality: A Modelling Study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef]
- Ministerio de Sanidad. Gobierno de España Recomendaciones de Vacunación Frente a La Gripe. Temporada 2022–2023. Available online: https://www.sanidad.gob.es/areas/promocionPrevencion/vacunaciones/programasDeVacunacion/docs/Recomendaciones_vacunacion_gripe.pdf (accessed on 9 May 2023).
- Ministerio de Sanidad. Gobierno de España Evolución de Cobertura de Vacunación Antigripal En Población ≥65 Años. España, Temporadas 2011–2012 a 2020–2021. Available online: https://www.sanidad.gob.es/areas/promocionPrevencion/vacunaciones/calendario-y-coberturas/coberturas/docs/Tabla4.pdf (accessed on 8 May 2022).
- Jorgensen, P.; Mereckiene, J.; Cotter, S.; Johansen, K.; Tsolova, S.; Brown, C. How Close Are Countries of the WHO European Region to Achieving the Goal of Vaccinating 75% of Key Risk Groups against Influenza? Results from National Surveys on Seasonal Influenza Vaccination Programmes, 2008/2009 to 2014/2015. Vaccine 2018, 36, 442–452. [Google Scholar] [CrossRef] [PubMed]
- World Health Assembly, 56. Prevention and Control of Influenza Pandemics and Annual Epidemics; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Palekar, R.S.; Rolfes, M.A.; Arriola, C.S.; Acosta, B.O.; Guidos, P.A.; Vargas, X.B.; Bancej, C.; Ramirez, J.B.; Baumeister, E.; Bruno, A.; et al. Burden of Influenza-Associated Respiratory Hospitalizations in the Americas, 2010–2015. PLoS ONE 2019, 14, e0221479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, A.; Kislaya, I.; Larrauri, A.; Matias Dias, C.; Nunes, B. Impact of National Influenza Vaccination Strategy in Severe Influenza Outcomes among the High-Risk Portuguese Population. BMC Public Health 2019, 19, 1690. [Google Scholar] [CrossRef]
- Rolfes, M.A.; Foppa, I.M.; Garg, S.; Flannery, B.; Brammer, L.; Singleton, J.A.; Burns, E.; Jernigan, D.; Olsen, S.J.; Bresee, J.; et al. Annual Estimates of the Burden of Seasonal Influenza in the United States: A Tool for Strengthening Influenza Surveillance and Preparedness. Influenza Other Respir. Viruses 2018, 12, 132–137. [Google Scholar] [CrossRef] [Green Version]
- MOVE+ Generic Protocol for Measuring the Impact of Influenza Vaccination Programmes among the Elderly Population in the European Union and European Economic Area Member States. Available online: https://www.imoveflu.org/wp-content/uploads/2019/12/I-MOVE-GEneric-influenza-Vaccine-Impact-protocol.pdf (accessed on 18 May 2023).
- Tokars, J.I.; Rolfes, M.A.; Foppa, I.M.; Reed, C. An Evaluation and Update of Methods for Estimating the Number of Influenza Cases Averted by Vaccination in the United States. Vaccine 2018, 36, 7331–7337. [Google Scholar] [CrossRef]
- Sistema de Vigilancia de la Gripe en España. Guía de Procedimientos Para La Vigilancia de Gripe En España. Octubre 2019. Available online: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/GRIPE/GUIAS/Guia_procedimientos_vigilancia_gripe_Octubre2019.pdf (accessed on 19 July 2022).
- Oliva, J.; Delgado-Sanz, C.; Larrauri, A. The Spanish Influenza Surveillance System Estimating the Burden of Seasonal Influenza in Spain from Surveillance of Mild and Severe Influenza Disease, 2010–2016. Influenza Other Respir. Viruses 2015, 12, 161–170. [Google Scholar] [CrossRef]
- Kissling, E.; Valenciano, M.; Pozo, F.; Vilcu, A.-M.; Reuss, A.; Rizzo, C.; Larrauri, A.; Horváth, J.K.; Brytting, M.; Domegan, L.; et al. 2015/16 I-MOVE/I-MOVE+ Multicentre Case-Control Study in Europe: Moderate Vaccine Effectiveness Estimates against Influenza A(H1N1)Pdm09 and Low Estimates against Lineage-Mismatched Influenza B among Children. Influenza Other Respir. Viruses 2017, 12, 423–437. [Google Scholar] [CrossRef]
- Rose, A.M.C.; Kissling, E.; Gherasim, A.; Casado, I.; Bella, A.; Launay, O.; Lazăr, M.; Marbus, S.; Kuliese, M.; Syrjänen, R.; et al. Vaccine Effectiveness against Influenza A(H3N2) and B among Laboratory-Confirmed, Hospitalised Older Adults, Europe, 2017-18: A Season of B Lineage Mismatched to the Trivalent Vaccine. Influenza Other Respir. Viruses 2020, 14, 302–310. [Google Scholar] [CrossRef]
- Kissling, E.; Rose, A.; Emborg, H.-D.; Gherasim, A.; Pebody, R.; Pozo, F.; Trebbien, R.; Mazagatos, C.; Whitaker, H.; Valenciano, M.; et al. Interim 2018/19 Influenza Vaccine Effectiveness: Six European Studies, October 2018 to January 2019. Eurosurveillance 2019, 24, 1900121. [Google Scholar] [CrossRef]
- Rose, A.; Kissling, E.; Emborg, H.-D.; Larrauri, A.; McMenamin, J.; Pozo, F.; Trebbien, R.; Mazagatos, C.; Whitaker, H.; Valenciano, M.; et al. Interim 2019/20 Influenza Vaccine Effectiveness: Six European Studies, September 2019 to January 2020. Eurosurveillance 2020, 25, 2000153. [Google Scholar] [CrossRef] [Green Version]
- Machado, A.; Mazagatos, C.; Dijkstra, F.; Kislaya, I.; Gherasim, A.; McDonald, S.A.; Kissling, E.; Valenciano, M.; Meijer, A.; Hooiveld, M.; et al. Impact of Influenza Vaccination Programmes among the Elderly Population on Primary Care, Portugal, Spain and the Netherlands: 2015/16 to 2017/18 Influenza Seasons. Eurosurveillance 2019, 24, 1900268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reed, C.; Chaves, S.S.; Kirley, P.D.; Emerson, R.; Aragon, D.; Hancock, E.B.; Butler, L.; Baumbach, J.; Hollick, G.; Bennett, N.M.; et al. Estimating Influenza Disease Burden from Population-Based Surveillance Data in the United States. PLoS ONE 2015, 10, e0118369. [Google Scholar] [CrossRef]
- Machado, A. Measuring the Impact of Influenza Vaccination National Strategy among the at Risk Portuguese Population. Ph.D. Thesis, Universidade Nova de Lisboa, Lisbon, Portugal, 2020. [Google Scholar]
- Casado, I.; Domínguez, Á.; Toledo, D.; Chamorro, J.; Astray, J.; Egurrola, M.; Fernández-Sierra, M.A.; Martín, V.; Morales-Suárez-Varela, M.; Godoy, P.; et al. Repeated Influenza Vaccination for Preventing Severe and Fatal Influenza Infection in Older Adults: A Multicentre Case-Control Study. CMAJ 2018, 190, E3–E12. [Google Scholar] [CrossRef] [Green Version]
- Caini, S.; Spreeuwenberg, P.; Kusznierz, G.F.; Rudi, J.M.; Owen, R.; Pennington, K.; Wangchuk, S.; Gyeltshen, S.; Ferreira de Almeida, W.A.; Pessanha Henriques, C.M.; et al. Distribution of Influenza Virus Types by Age Using Case-Based Global Surveillance Data from Twenty-Nine Countries, 1999–2014. BMC Infect. Dis. 2018, 18, 269. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.; Presanis, A.M.; Bond, H.S.; Lau, E.H.Y.; Fang, V.J.; Cowling, B.J. A Joint Analysis of Influenza-Associated Hospitalizations and Mortality in Hong Kong, 1998–2013. Sci. Rep. 2017, 7, 929. [Google Scholar] [CrossRef] [Green Version]
- Zhou, H.; Thompson, W.W.; Viboud, C.G.; Ringholz, C.M.; Cheng, P.-Y.; Steiner, C.; Abedi, G.R.; Anderson, L.J.; Brammer, L.; Shay, D.K. Hospitalizations Associated with Influenza and Respiratory Syncytial Virus in the United States, 1993–2008. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2012, 54, 1427–1436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgado-Sanz, C.; Mazagatos-Ateca, C.; Oliva, J.; Gherasim, A.; Larrauri, A. Illness Severity in Hospitalized Influenza Patients by Virus Type and Subtype, Spain, 2010–2017. Emerg. Infect. Dis. 2020, 26, 220–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rondy, M.; Gherasim, A.; Casado, I.; Launay, O.; Rizzo, C.; Pitigoi, D.; Mickiene, A.; Marbus, S.D.; Machado, A.; Syrjänen, R.K.; et al. Low 2016/17 Season Vaccine Effectiveness against Hospitalised Influenza A(H3N2) among Elderly: Awareness Warranted for 2017/18 Season. Eurosurveillance 2017, 22, 17-00645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kissling, E. Low Vaccine Effectiveness against Influenza A(H3N2) in Europe: Estimates from the I-MOVE Multicentre Case Control Study. In Proceedings of the European Scientific Conference on Applied Infectious Disease Epidemiology (ESCAIDE), Stockholm, Sweden, 6–8 November 2017. [Google Scholar]
- Kissling, E.; Pozo, F.; Buda, S.; Vilcu, A.-M.; Gherasim, A.; Brytting, M.; Domegan, L.; Gómez, V.; Meijer, A.; Lazar, M.; et al. Low 2018/19 Vaccine Effectiveness against Influenza A(H3N2) among 15–64-Year-Olds in Europe: Exploration by Birth Cohort. Eurosurveillance 2019, 24, 1900604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagaria, J.; Jansen, T.; Marques, D.F.; Hooiveld, M.; McMenamin, J.; de Lusignan, S.; Vilcu, A.-M.; Meijer, A.; Rodrigues, A.-P.; Brytting, M.; et al. Rapidly Adapting Primary Care Sentinel Surveillance across Seven Countries in Europe for COVID-19 in the First Half of 2020: Strengths, Challenges, and Lessons Learned. Eurosurveillance 2022, 27, 2100864. [Google Scholar] [CrossRef] [PubMed]
- Larrauri, A.; Trilar, K.P. Preparing for an Influenza Season 2021/22 with a Likely Co-Circulation of Influenza Virus and SARS-CoV-2. Eurosurveillance 2021, 26, 2100975. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control Seasonal Influenza—Annual Epidemiological Report for 2020–2021. Available online: https://www.ecdc.europa.eu/en/publications-data/seasonal-influenza-annual-epidemiological-report-2020-2021 (accessed on 18 August 2022).
- Adlhoch, C.; Sneiderman, M.; Martinuka, O.; Melidou, A.; Bundle, N.; Fielding, J.; Olsen, S.J.; Penttinen, P.; Pastore, L.; Pebody, R.; et al. Spotlight Influenza: The 2019/20 Influenza Season and the Impact of COVID-19 on Influenza Surveillance in the WHO European Region. Eurosurveillance 2021, 26, 2100077. [Google Scholar] [CrossRef]
- Uyeki, T.M.; Wentworth, D.E.; Jernigan, D.B. Influenza Activity in the US during the 2020–2021 Season. JAMA 2021, 325, 2247–2248. [Google Scholar] [CrossRef]
- Instituto de Salud Carlos III. Sistema de Vigilancia de Infección Respiratoria Aguda en España (SiVIRA). Informe Anual de Vigilancia de Gripe, COVID-19 y VRS España, SiVIRA, Temporada 2021–2022. Available online: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/GRIPE/INFORMES%20ANUALES/Informe%20SiVIRA%20de%20Vigilancia%20de%20gripe%2c%20COVID-19%20y%20VRS_temporada%202021-22_v14112022.pdf (accessed on 8 May 2023).
- Reed, C.; Kim, I.K.; Singleton, J.A.; Chaves, S.S.; Flannery, B.; Finelli, L.; Fry, A.; Burns, E.; Gargiullo, P.; Jernigan, D.; et al. Estimated Influenza Illnesses and Hospitalizations Averted by Vaccination—United States, 2013–14 Influenza Season. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 1151–1154. [Google Scholar]
- Centers for Disease Control and Prevention Estimated Flu-Related Illnesses, Medical Visits, Hospitalizations, and Deaths in the United States—2019–2020 Flu Season|CDC. Available online: https://www.cdc.gov/flu/about/burden/2019-2020.html (accessed on 18 August 2022).
- Yin, J.K.; Heywood, A.E.; Georgousakis, M.; King, C.; Chiu, C.; Isaacs, D.; Macartney, K.K. Systematic Review and Meta-Analysis of Indirect Protection Afforded by Vaccinating Children Against Seasonal Influenza: Implications for Policy. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2017, 65, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Eichner, M.; Schwehm, M.; Eichner, L.; Gerlier, L. Direct and Indirect Effects of Influenza Vaccination. BMC Infect. Dis. 2017, 17, 308. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad. Ministerio de Sanidad, Gobierno de España Recomendaciones de Vacunación Frente a La Gripe En Población Infantil de 6 a 59 Meses. Ponencia de Programa y Registro de Vacunaciones 2022. Octubre de 2022. Available online: https://www.sanidad.gob.es/areas/promocionPrevencion/vacunaciones/programasDeVacunacion/docs/Recomendaciones_vacunacion_gripe_PoblacionInfantil.pdf (accessed on 18 May 2023).


{kind=link}
| Distribution of Influenza Viruses Circulating in Spain (%) | Pooled IVE Weighted by Influenza Subtype Distribution in Spain | |||
|---|---|---|---|---|
| Season | A(H1N1)pdm09 | A(H3N2) | B | VE (95% CI) |
| 2017–18 | 7.6 | 25.3 | 64.9 | 30 (22; 38) |
| 2018–19 | 36.3 | 61.2 | 20 (6; −36) | |
| 2019–20 | 59.5 | 19.0 | 21.5 | 49 (24; 66) |
| Influenza Hospitalizations | |||||||
|---|---|---|---|---|---|---|---|
| Season | Age Group | Number | 95% CI | Rate 1 | 95% CI | ||
| 2017–18 | All ages | 49,752 | 34,163 | 72,455 | 107.4 | 73.8 | 156.5 |
| <5 years | 4893 | 2989 | 8009 | 237.2 | 144.9 | 388.3 | |
| 5–14 years | 2398 | 1350 | 4258 | 49.6 | 27.9 | 88.1 | |
| 15–64 years | 13,594 | 9117 | 20,270 | 44.5 | 29.8 | 66.3 | |
| >64 years | 28,173 | 20,463 | 38,789 | 318.7 | 231.5 | 438.8 | |
| 2018–19 | All ages | 35,344 | 26,704 | 46,780 | 76.4 | 57.8 | 101.2 |
| <5 years | 3266 | 2261 | 4717 | 164.8 | 114.1 | 238.0 | |
| 5–14 years | 1815 | 1102 | 2990 | 37.6 | 22.8 | 61.9 | |
| 15–64 years | 9635 | 6579 | 14,111 | 31.7 | 21.6 | 46.4 | |
| >64 years | 20,510 | 15,947 | 26,378 | 228.0 | 177.3 | 293.2 | |
| 2019–20 | All ages | 27,657 | 21,212 | 36,060 | 59.9 | 45.9 | 78.1 |
| <5 years | 4558 | 3152 | 6590 | 237.6 | 164.3 | 343.5 | |
| 5–14 years | 1870 | 1233 | 2836 | 39.1 | 25.8 | 59.4 | |
| 15–64 years | 9890 | 7481 | 13,075 | 32.6 | 24.7 | 43.1 | |
| >64 years | 11,703 | 8787 | 15,585 | 127.9 | 96.0 | 170.3 | |
| ICU admissions | |||||||
| Season | Age group | Number | 95% CI | Rate 1 | 95% CI | ||
| 2017–18 | All ages | 2881 | 2348 | 3535 | 6.2 | 5.1 | 7.6 |
| <5 years | 321 | 210 | 490 | 15.6 | 10.2 | 23.8 | |
| 5–14 years | 121 | 62 | 237 | 2.5 | 1.3 | 4.9 | |
| 15–64 years | 1203 | 989 | 1463 | 3.9 | 3.2 | 4.8 | |
| >64 years | 1330 | 1087 | 1626 | 15.0 | 12.3 | 18.4 | |
| 2018–19 | All ages | 2532 | 2211 | 2899 | 5.5 | 4.8 | 6.3 |
| <5 years | 238 | 136 | 416 | 12.0 | 6.9 | 21.0 | |
| 5–14 years | 93 | 59 | 147 | 1.9 | 1.2 | 3.0 | |
| 15–64 years | 1186 | 1021 | 1379 | 3.9 | 3.4 | 4.5 | |
| >64 years | 1028 | 856 | 1234 | 11.4 | 9.5 | 13.7 | |
| 2019–20 | All ages | 1763 | 1406 | 2213 | 3.8 | 3.0 | 4.8 |
| <5 years | 197 | 124 | 314 | 10.3 | 6.5 | 16.4 | |
| 5–14 years | 103 | 54 | 195 | 2.2 | 1.1 | 4.1 | |
| 15–64 years | 1021 | 783 | 1332 | 3.4 | 2.6 | 4.1 | |
| >64 years | 453 | 357 | 575 | 5.0 | 3.9 | 6.3 | |
| Season | Number Reported to SISSS | % Swabbing | Estimated Burden | VE 1; 95% IC (%) | VC 2 (%) |
|---|---|---|---|---|---|
| Influenza hospitalizations | |||||
| 2017–18 | 28,173 | 40.5 | 69,563 | 30; 22–38 | 55.7 |
| 2018–19 | 20,510 | 42.3 | 48,487 | 20; 6–36 | 54.4 |
| 2019–20 | 11,703 | 42.7 | 27,407 | 49; 24–66 | 53.5 |
| ICU admissions | |||||
| 2017–18 | 1330 | 40.5 | 3284 | 74; 42–88 | 55.7 |
| 2018–19 | 1028 | 42.3 | 2430 | 74; 42–88 | 54.4 |
| 2019–20 | 453 | 42.7 | 1061 | 74; 42–88 | 53.5 |
| Season | 2017–18 | 2018–19 | 2019–20 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | 95% CI | n | 95% CI | n | 95% CI | ||||
| Influenza hospitalizations | |||||||||
| Number averted | 13,985 | 9444 | 18,399 | 5892 | 817 | 11,173 | 9823 | 4078 | 14,924 |
| Rate (per 100,000 pop) | 158.2 | 106.8 | 208.1 | 65.5 | 9.1 | 124.2 | 107.4 | 44.6 | 163.1 |
| Prevented fraction (%) | 16.7 | 12.0 | 20.9 | 10.8 | 1.7 | 18.8 | 26.4 | 13.0 | 35.3 |
| ICU admissions | |||||||||
| Number averted | 2299 | 1033 | 3196 | 1628 | 736 | 2241 | 695 | 324 | 949 |
| Rate (per 100,000 pop) | 26.0 | 11.7 | 36.2 | 18.1 | 8.2 | 24.9 | 7.6 | 3.5 | 10.4 |
| Prevented fraction (%) | 41.2 | 23.9 | 49.2 | 40.1 | 23.4 | 47.9 | 39.6 | 23.3 | 47.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazagatos, C.; Delgado-Sanz, C.; Milagro, A.; Liébana-Rodríguez, M.; Larrauri, A. Impact of Influenza Vaccination on the Burden of Severe Influenza in the Elderly: Spain, 2017–2020. Vaccines 2023, 11, 1110. https://doi.org/10.3390/vaccines11061110
Mazagatos C, Delgado-Sanz C, Milagro A, Liébana-Rodríguez M, Larrauri A. Impact of Influenza Vaccination on the Burden of Severe Influenza in the Elderly: Spain, 2017–2020. Vaccines. 2023; 11(6):1110. https://doi.org/10.3390/vaccines11061110
Chicago/Turabian StyleMazagatos, Clara, Concepción Delgado-Sanz, Ana Milagro, María Liébana-Rodríguez, and Amparo Larrauri. 2023. "Impact of Influenza Vaccination on the Burden of Severe Influenza in the Elderly: Spain, 2017–2020" Vaccines 11, no. 6: 1110. https://doi.org/10.3390/vaccines11061110