
Association between Overweight/Obesity and the Safety and Efficacy of COVID-19 Vaccination: A Systematic Review

Abstract
:1. Introduction
Research Hypotheses and Objectives
- To explore the effectiveness of the COVID-19 vaccine in obese people.
- To explore the safety of the COVID-19 vaccine in obese people.
2. Methods
2.1. Registration
2.2. Literature Search
2.3. Inclusion and Exclusion Criteria
2.4. Selection Process
2.5. Data Extraction
2.6. Assessment of Risk of Bias
3. Results
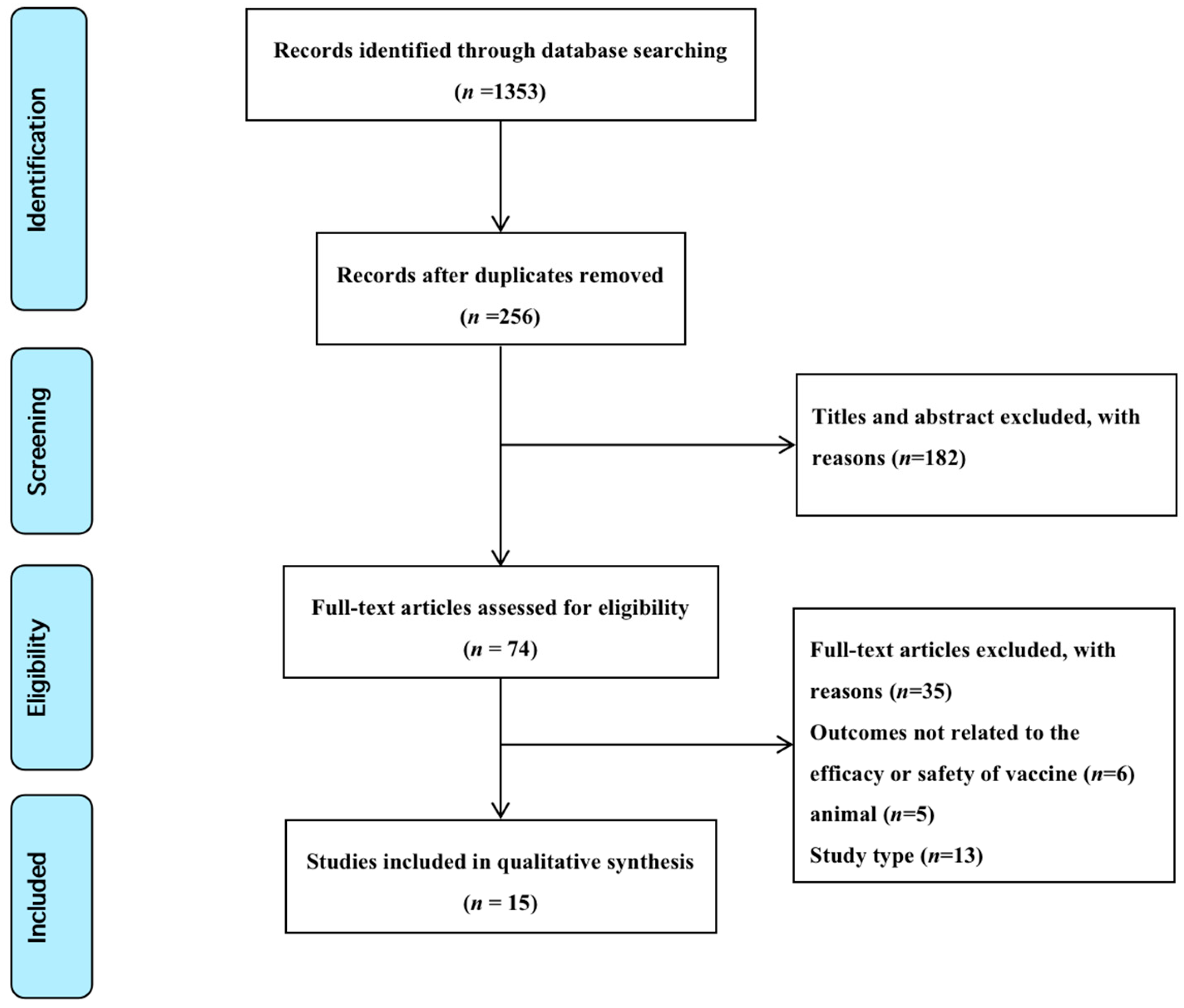
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Appraisal
3.4. Synthesis of Results
3.5. Overweight/Obesity and COVID-19 Vaccine Efficacy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coronavirus Disease (COVID-19) Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 9 January 2023).
- COVID-19 Vaccines. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines (accessed on 9 January 2023).
- Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants (accessed on 9 January 2023).
- Xing, K.; Tu, X.-Y.; Liu, M.; Liang, Z.-W.; Chen, J.-N.; Li, J.-J.; Jiang, L.-G.; Xing, F.-Q.; Jiang, Y. Efficacy and safety of COVID-19 vaccines: A systematic review. Zhongguo Dang Dai Er Ke Za Zhi 2021, 23, 221–228. [Google Scholar] [PubMed]
- COVID-19 Vaccine Tracker and Landscape. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 9 January 2023).
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 9 January 2023).
- Lv, M.; Luo, X.; Shen, Q.; Lei, R.; Liu, X.; Liu, E.; Li, Q.; Chen, Y. Safety, Immunogenicity, and Efficacy of COVID-19 Vaccines in Children and Adolescents: A Systematic Review. Vaccines 2021, 10, 1102. [Google Scholar] [CrossRef] [PubMed]
- Tian, D.; Nie, W.; Sun, Y.; Ye, Q. The Epidemiological Features of the SARS-CoV-2 Omicron Subvariant BA.5 and Its Evasion of the Neutralizing Activity of Vaccination and Prior Infection. Vaccines 2022, 10, 1699. [Google Scholar] [CrossRef] [PubMed]
- Obesity. Available online: https://www.who.int/health-topics/obesity (accessed on 9 January 2023).
- Butsch, W.S.; Hajduk, A.; Cardel, M.I.; Donahoo, W.T.; Kyle, T.K.; Stanford, F.C.; Zeltser, L.M.; Kotz, C.M.; Jastreboff, A.M. COVID-19 vaccines are effective in people with obesity: A position statement from The Obesity Society. Obesity 2021, 10, 1575–1579. [Google Scholar] [CrossRef] [PubMed]
- Malavazos, A.E.; Basilico, S.; Iacobellis, G.; Milani, V.; Cardani, R.; Boniardi, F.; Dubini, C.; Prandoni, I.; Capitanio, G.; Renna, L.V.; et al. Antibody responses to BNT162b2 mRNA vaccine: Infection-naïve individuals with abdominal obesity warrant attention. Obesity 2022, 3, 606–613. [Google Scholar] [CrossRef]
- Dicker, D.; Golan, R.; Baker, J.L.; Busetto, L.; Frühbeck, G.; Goossens, G.H.; Halford, J.C.; Holm, J.C.; Woodward, E.; Farpour-Lambert, N.J. Vaccinating People with Obesity for COVID-19: EASO Call for Action. Obes. Facts 2021, 3, 334–335. [Google Scholar] [CrossRef]
- Watanabe, M.; Balena, A.; Tuccinardi, D.; Tozzi, R.; Risi, R.; Masi, D.; Caputi, A.; Rossetti, R.; Spoltore, M.E.; Filippi, V.; et al. Central obesity, smoking habit, and hypertension are associated with lower antibody titres in response to COVID-19 mRNA vaccine. Diabetes Metab. Res. 2022, 38, e3465. [Google Scholar] [CrossRef]
- Tubjaroen, C.; Prachuapthunyachart, S.; Potjalongsilp, N.; Sodsai, P.; Hirankarn, N.; Jaru-Ampornpan, P.; Chongsrisawat, V. Immunogenicity of an mRNA-Based COVID-19 Vaccine among Adolescents with Obesity or Liver Transplants. Vaccines 2022, 10, 1867. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Institute, J.B. Checklist for Systematic Reviews and Research Syntheses; Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Moola, S. Chapter 7: Systematic reviews of etiology and risk. In Joanna Briggs Institute Reviewer’s Manual; Joanna Briggs Institute: Adelaide, Australia, 2017; p. 5. [Google Scholar]
- Gaborit, B.; Fernandes, S.; Loubet, P.; Ninove, L.; Dutour, A.; Cariou, B.; Coupaye, M.; Clement, K.; Czernichow, S.; Carette, C.; et al. Early humoral response to COVID-19 vaccination in patients living with obesity and diabetes in France. The COVPOP OBEDIAB study with results from the ANRS0001S COV-POPART cohort. Metabolism 2023, 142, 155412. [Google Scholar] [CrossRef]
- Zhu, Q.; Zhang, Y.; Kang, J.; Chen, Z.; Peng, M.; Chen, M.; Zhang, G.; Xiang, D.; Xiao, S.; Li, H.; et al. Weakened humoral and cellular immune response to the inactivated COVID-19 vaccines in Chinese individuals with obesity/overweight. Genes Dis. 2022, 10, 608–617. [Google Scholar] [CrossRef] [PubMed]
- Faizo, A.A.; Qashqari, F.S.; El-Kafrawy, S.A.; Barasheed, O.; Almashjary, M.N.; Alfelali, M.; Bawazir, A.A.; Albarakati, B.M.; Khayyat, S.A.; Hassan, A.M.; et al. A potential association between obesity and reduced effectiveness of COVID-19 vaccine-induced neutralizing humoral immunity. J. Med. Virol. 2023, 95, e28130. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Moon, J.Y.; Lee, S.K.; Lee, H.; Moon, S.; Chung, S.J.; Yeo, Y.; Park, T.S.; Park, D.W.; Kim, T.H.; et al. Anti-SARS-CoV-2 Spike Protein RBD Antibody Levels After Receiving a Second Dose of ChAdOx1 nCov-19 (AZD1222) Vaccine in Healthcare Workers: Lack of Association With Age, Sex, Obesity, and Adverse Reactions. Front. Immunol. 2021, 12, 779212. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Balena, A.; Masi, D.; Tozzi, R.; Risi, R.; Caputi, A.; Rossetti, R.; Spoltore, M.E.; Biagi, F.; Anastasi, E.; et al. Rapid Weight Loss, Central Obesity Improvement and Blood Glucose Reduction Are Associated with a Stronger Adaptive Immune Response Following COVID-19 mRNA Vaccine. Vaccines 2022, 5, 79. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Mizoue, T.; Tanaka, A.; Oshiro, Y.; Inamura, N.; Konishi, M.; Ozeki, M.; Miyo, K.; Sugiura, W.; Sugiyama, H.; et al. Sex-associated differences between BMI and SARS-CoV-2 antibody titers following the BNT162b2 vaccine. Obesity 2022, 30, 999–1003. [Google Scholar] [CrossRef] [PubMed]
- Kara, Z.; Akçin, R.; Demir, A.N.; Dinç, H.Ö.; Taşkın, H.E.; Kocazeybek, B.; Yumuk, V.D. Antibody Response to SARS-CoV-2 Vaccines in People with Severe Obesity. Obes. Surg. 2022, 32, 2987–2993. [Google Scholar] [CrossRef]
- Pellini, R.; Venuti, A.; Pimpinelli, F.; Abril, E.; Blandino, G.; Campo, F.; Conti, L.; De Virgilio, A.; De Marco, F.; Di Domenico, E.G.; et al. Initial observations on age, gender, BMI and hypertension in antibody responses to SARS-CoV-2 BNT162b2 vaccine. EClinicalMedicine 2021, 36, 100928. [Google Scholar] [CrossRef]
- Piernas, C.; Patone, M.; Astbury, N.M.; Gao, M.; Sheikh, A.; Khunti, K.; Shankar-Hari, M.; Dixon, S.; Coupland, C.; Aveyard, P.; et al. Associations of BMI with COVID-19 vaccine uptake, vaccine effectiveness, and risk of severe COVID-19 outcomes after vaccination in England: A population-based cohort study. Lancet Diabetes Endocrinol. 2022, 10, 571–580. [Google Scholar] [CrossRef]
- Iguacel, I.; Maldonado, A.L.; Ruiz-Cabello, A.L.; Casaus, M.; Moreno, L.A.; Martínez-Jarreta, B. Association between COVID-19 Vaccine Side Effects and Body Mass Index in Spain. Vaccines 2021, 15, 1321. [Google Scholar] [CrossRef]
- Yoshida, M.; Kobashi, Y.; Shimazu, Y.; Saito, H.; Yamamoto, C.; Kawamura, T.; Wakui, M.; Takahashi, K.; Ito, N.; Nishikawa, Y.; et al. Time course of adverse reactions following BNT162b2 vaccination in healthy and allergic disease individuals aged 5–11 years and comparison with individuals aged 12–15 years: An observational and historical cohort study. Eur. J. Pediatr. 2023, 182, 123–133. [Google Scholar] [CrossRef]
- Sutardi, A.Q.I.; Ramatillah, D.L. Eevaluation comparison between sinovac and pfizer vaccine among indonesian children and teenagers under 18 years old. Int. J. Appl. Pharm. 2022, 14, 22–30. [Google Scholar] [CrossRef]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef] [PubMed]
- Nasr, M.C.; Geerling, E.; Pinto, A.K. Impact of Obesity on Vaccination to SARS-CoV-2. Front. Endocrinol. 2022, 13, 898810. [Google Scholar] [CrossRef] [PubMed]
- Kipshidze, N.; Kipshidze, N.; Fried, M. COVID-19 Vaccines: Special Considerations for the Obese Population. Obes. Surg. 2021, 31, 3854–3856. [Google Scholar] [CrossRef] [PubMed]
- Westheim, A.J.F.; Bitorina, A.V.; Theys, J.; Shiri-Sverdlov, R. COVID-19 infection, progression, and vaccination: Focus on obesity and related metabolic disturbances. Obes. Rev. 2021, 22, e13313. [Google Scholar] [CrossRef]


{kind=link}
| No. | 1st Author (Year) | Study Objectives | Country | Study Design | Population | Follow-up Period | Vaccine Received | Outcomes | Conclusion |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Malavazos AE,2022 [11] | To evaluate how people with AO respond to mRNA vaccines against SARS-CoV-2 | Italy | cohort study | healthcare workers; AO = 492, NoAO = 568; Age: 41.42 ± 12.95 | (1) Baseline (2) 21 days after dose 1 (3) 1 month after dose 2 (4) 3 months after dose 2 | BNT162b2 | Vaccine Efficacy: Between the first and third month after vaccine dose 2, the drop in IgG-TrimericS levels was more remarkable in individuals with AO compared with those without AO | The waning antibody levels in individuals with AO |
| 2 | Gaborit B,2023 [18] | To investigate early humoral response to COVID-19 vaccination in patients with obesity | France | cohort study | patients with obesity (n = 357) healthy subjects (n = 573); Age: 47.2 ± 14.7 | 1, 6, 12, and 24 months after the first two doses of COVID-19 vaccines | (1) BNT162b2 (2) mRNA-1273 (3) ChAdOxnCov-2019 | Vaccine Efficacy: Patients with obesity were less likely to have positive antibodies after the first and second doses compared to the controls | The humoral response to the COVID-19 vaccine was lower in patients with obesity one month after the second dose |
| 3 | Zhu Q,2022 [19] | To evaluate the safety profile and provide new insights into inactivated COVID-19-vaccine-induced humoral and cellular immune responses | China | cohort study | obesity/overweight (n = 132) normal BMI (n = 82); Age: 18 to 75 years | 21−105 days after full-course COVID-19 vaccination | BBIBP-CorV/CoronaVac | Vaccine Safety: No serious vaccine-related adverse effects occurred. Vaccine Efficacy: Individuals with obesity/overweight had lower NAbs Anti-RBD-IgG | Inactivated COVID-19 vaccines were safe and well tolerated but induced poor humoral and cellular immune responses in individuals with obesity/overweight |
| 4 | Faizo AA,2023 [20] | To investigate the effectiveness of COVID-19 vaccines among individuals with obesity | Jeddah, Saudi Arabia | cross-sectional study | obese (n = 73) normal BMI (n = 46); Age: 18 to >60 years | (1) <90 days (2) 90–180 days (3) >180 days | (1) BNT162b2 (2) ChAdOx nCov-2019 (3) mRNA-1273 | Vaccine Efficacy: The observed reduction in COVID-19-vaccine-induced neutralizing humoral immunity among obese individuals occurred independently of gender, recovery from past infection, and time since the last vaccination. | The effectiveness of COVID-19 vaccines is potentially reduced among obese individuals |
| 5 | Lee SW, 2021 [21] | To assess the relationships of antibody level with BMI | Korea | cross-sectional study | healthcare workers; Obese (n = 88); Age: 40.6 ± 10.9 | (1) 7 days after each injection (2) 4 weeks after the second injection | ChAdOx1 nCoV-19 | Vaccine Efficacy: Anti-SARS-CoV-2 S protein RBD concentration showed no significant association of antibody concentration with BMI | Obesity was not associated with antibody responses after two doses of ChAdOx1 nCoV-19 vaccination |
| 6 | Watanabe M, 2022 [22] | To investigate the impact of rapid weight loss on the adaptive immune response in subjects with morbid obesity | Italy | cross-sectional study | 21 participants BMI ≥ 35 kg/m2 with at least one obesity-related complication or BMI ≥ 40 kg/m2 alone; Age: 51.50(41.50, 55.25) | 5 to 7 weeks between the two vaccine doses | BNT162b2 | Vaccine Efficacy: A high baseline BMI was correlated with a poor immune response | Obesity was associated with a reduced adaptive response to an mRNA COVID-19 vaccine |
| 7 | Tubjaroen, 2022 [14] | To evaluate immunogenicity among children with liver transplants and obesity following two doses of the BNT162b2 vaccine | Thailand | cohort study | n = 68 (Obese group: n = 24; LTRs group: n = 12; control group: n = 32); Age:14.9 ± 1.7 | 27.1 ± 3.2 days after the second dose | BNT162b2 | Vaccine Efficacy: SARS-CoV-2 antibody levels at approximately four weeks following the second dose of the BNT162b2 vaccine in obese adolescents were lower than those in the control participants with normal weight | Obese adolescents showed low antibody response to the BNT162b2 vaccine |
| 8 | Yamamoto S, 2022 [23] | To investigate the impact of obesity on antibody response to a COVID-19 vaccine | Japan | cohort study | healthcare workers (n = 2435); Age:36.6(27.6,47.6) | 2 months after the in-house vaccination program | BNT162b2 | Vaccine Efficacy: Spike IgG antibody titers tended to decrease with increasing BMI in men | Higher BMI was associated with lower titers of SARS-CoV-2 spike antibodies in men, but not in women |
| 9 | Kara Z, 2022 [24] | To investigate the spike-protein receptor-binding domain antibody titers against BNT162b2mRNA and inactivated SARS-CoV-2 (CoronaVac) vaccines in people with severe obesity | UK | cohort study | study group (BMI ≥ 40 kg/m2, n = 124) normal weight control group (BMI 18.5–24.9 kg/m2, n = 166) | 4th week and after 2nd dose of vaccination | (1) BNT162b2 (2) Corona Vac vaccines | Vaccine Efficacy: In 220 subjects (no prior infection) vaccinated with BNT162b2 or CoronaVac, the antibody titers against the SARS-CoV-2 spike antigen of patients with severe obesity were significantly lower than those of normal weight controls | Patients with severe obesity generated significantly reduced antibody titers against SARS-CoV-2 spike antigen after CoronaVac and BNT162b2 vaccines compared to people with normal weight |
| 10 | Pellini R, 2021 [25] | To analyze the antibody titer response 7 days after the second dose of a vaccine | Italy | cohort study | 248 healthcare workers; Age: 47 (range 23–69) | baseline and 7 days after BNT162b2 booster dose | BNT162b2 | Vaccine Efficacy: BMI had no statistically significant association with the geometric mean concentration of antibodies | BMI did not seem to be associated with a difference in immune response to the vaccine |
| 11 | Piernas C, 2022 [26] | To examine the association between BMI and COVID-19 vaccine uptake, vaccine effectiveness, and risk of severe COVID-19 outcomes after vaccination | UK | cohort study | 9,171,524 participants Age: 52 ± 19 | days from 8 December 2020 | (1) ChAdOx-nCov19 (2) BNT162b2 (3) mRNA1273 | Vaccine Efficacy: For COVID-19 test positivity, there was a linear association with BMI after the first dose, an exponential association after the second dose, and an inverse U-shaped association after the third dose, with significantly lower HRs at very low and very high BMI levels. Vaccine Safety: In the vaccinated cohort, there were significant linear associations of BMI with COVID-19 hospitalization and death after the first dose, and there were J-shaped associations after the second dose | In the vaccinated cohort, there were increased risks of severe COVID-19 outcomes for people with underweight or obesity compared with the vaccinated population with a healthy weight |
| 12 | Watanabe M, 2022 [13] | To explore variables associated with the serological response following an mRNA COVID-19 vaccine | Italy | cohort study | 86 healthcare workers; Central obesity (n = 53); Age:29 ± 17 | (1) Before the first inoculation (2) 1 and 4 weeks after the second inoculation | BNT162b2 | Vaccine Efficacy: Higher waist circumference was associated with lower antibody titers Vaccine Safety: Higher waist circumference, waist-to-hip ratio, BMI, and body fat were not associated with more adverse events | Central obesity was associated with lower antibody titers following COVID-19 vaccination |
| 13 | Iguacel I, 2021 [27] | To study the association between weight status and reported side-effects | Spain | cross-sectional study | 2136 adults | from 6 May to 9 June 2021 | Pfizer, Moderna, and AstraZeneca/Vaxzevria | Vaccine Safety: Most side-effects were reported at a higher percentage in those who were underweight or normal weight compared to overweight or obese | A nonoverweight status was associated with a higher risk of presenting fever ≥38°, vomiting, diarrhea, and chills compared to those who were overweight |
| 14 | Yoshida, 2022 [28] | To investigate the type and frequency of adverse reactions in healthy and allergic disease individuals aged 5–11 years over the first seven days following the first and second BNT162b2 vaccinations | Japan | cohort study | n = 421; Mean age: 8.8 ± 1.9; | Seven days after vaccination | BNT162b2 | Vaccine Safety: Compared to ‘normal’ individuals, ‘thin’ and ‘overweight’ individuals did not have higher odds of experiencing adverse systemic reactions | BMI was not associated with adverse systemic reactions |
| 15 | Sutardi, 2022 [29] | To evaluate a comparison between the Sinovac and Pfizer vaccines for children and teenagers under 18 y in Indonesia and other factors that influenced it | Indonesia | Cross-sectional study | n = 400 (Sinovac 200, Pfizer 200); Age: 12–17 years old | 1–6 months after vaccination | Sinovac vaccine and Pfizer vaccine | Vaccine Safety: BMI was related to side-effects after: 1st vaccination: fever, pain in the injection area, lost smell and taste; 2nd vaccination: sleepiness, fever; 1–3 months post-vaccination: menstrual problems; 4–6 months post-vaccination: menstrual problems (p < 0.05) | Vaccine recipients with a BMI of less than 25 had a higher risk of having side-effects from the COVID-19 vaccine |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, C.; Lin, N.; Zhu, J.; Ye, Q. Association between Overweight/Obesity and the Safety and Efficacy of COVID-19 Vaccination: A Systematic Review. Vaccines 2023, 11, 996. https://doi.org/10.3390/vaccines11050996
Fu C, Lin N, Zhu J, Ye Q. Association between Overweight/Obesity and the Safety and Efficacy of COVID-19 Vaccination: A Systematic Review. Vaccines. 2023; 11(5):996. https://doi.org/10.3390/vaccines11050996
Chicago/Turabian StyleFu, Cangcang, Nan Lin, Jihua Zhu, and Qing Ye. 2023. "Association between Overweight/Obesity and the Safety and Efficacy of COVID-19 Vaccination: A Systematic Review" Vaccines 11, no. 5: 996. https://doi.org/10.3390/vaccines11050996