
The Influence of Recommendation of Medical and Non-Medical Authorities on the Decision to Vaccinate against Influenza from a Social Vaccinology Perspective: Cross-Sectional, Representative Study of Polish Society


Abstract
:1. Introduction
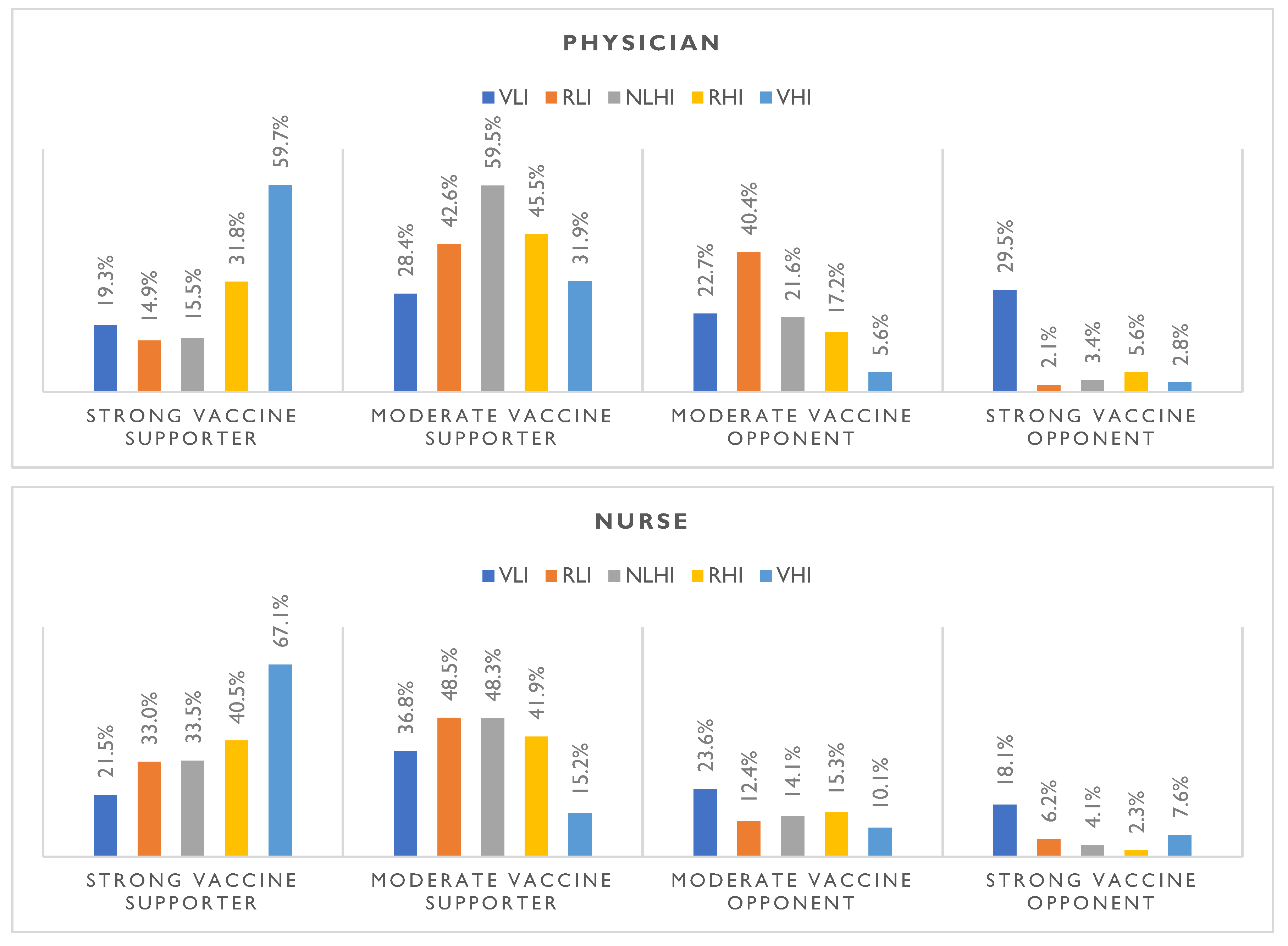
- To what extent would a physician’s or nurse’s opinion influence your decision to vaccinate against influenza?
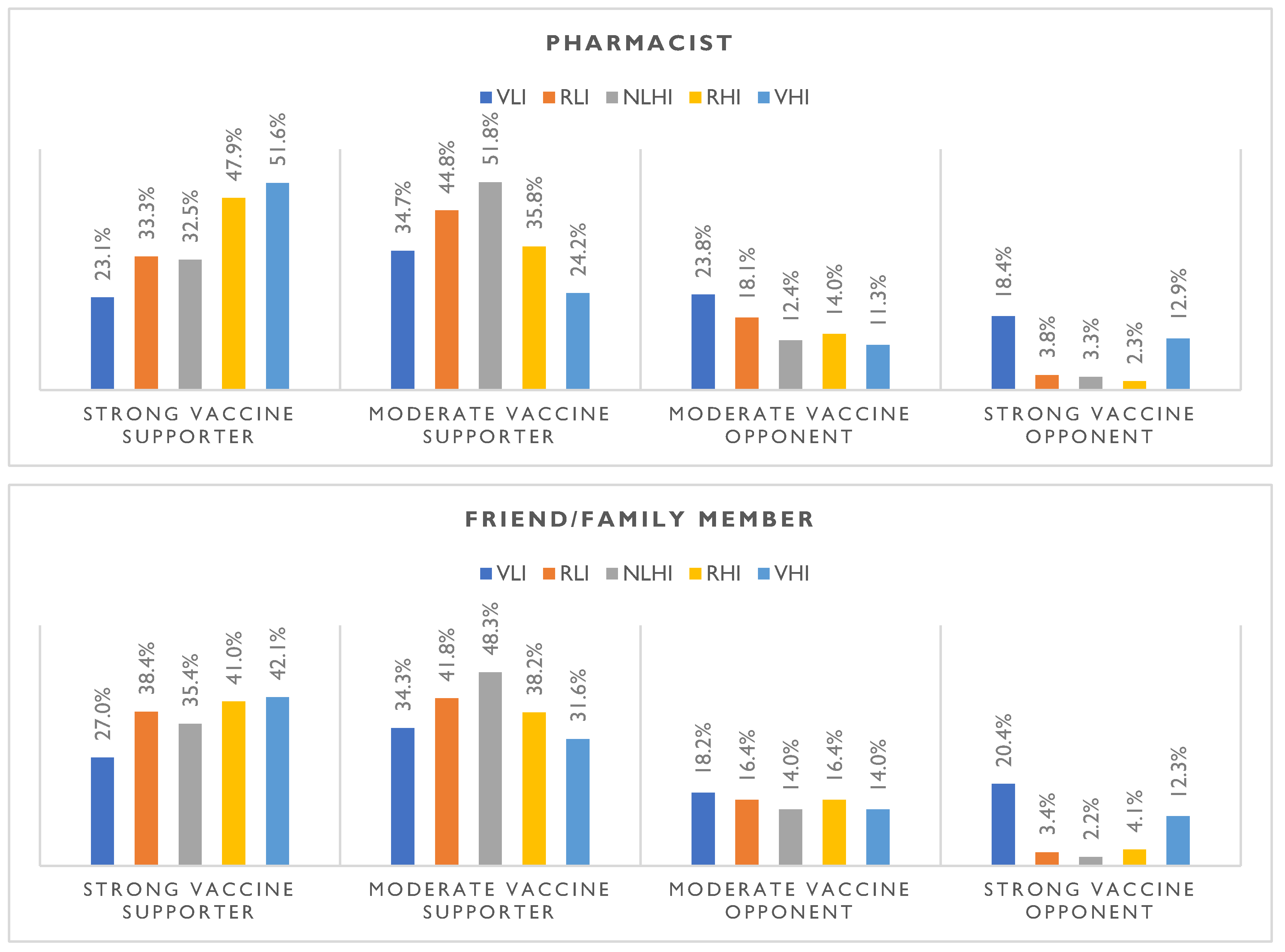
- To what extent a friend’s/family member’s opinion would influence a respondent’s decision to be vaccinated against influenza?
- To what extent would a pharmacist’s opinion influence flu vaccination?
- How does the respondent’s attitude toward vaccination correlate with trust in medical authority regarding influenza vaccination?
- Do sex and age affect the trust in medical authority regarding influenza vaccination?
2. Materials and Methods
2.1. Implementation of the Study and Sample Size
2.2. Operationalization of the Concept of Authority
2.3. Questionnaire Design
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Characteristics of Studied Participants
3.2. Attitudes toward Influenza Vaccination
3.3. The Influence of Medical and Personal Authority on Influenza Vaccination
3.4. Attitudes toward Vaccination Compared to Levels of Trust in Particular Authority Groups
4. Discussion
Limitations and Strengths of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hughes, M.M.; Reed, C.; Flannery, B.; Garg, S.; Singleton, J.A.; Fry, A.M.; Rolfes, M.A. Projected Population Benefit of Increased Effectiveness and Coverage of Influenza Vaccination on Influenza Burden in the United States. Clin. Infect. Dis. 2020, 70, 2496–2502. [Google Scholar] [CrossRef] [PubMed]
- Foppa, I.M.; Cheng, P.-Y.; Reynolds, S.B.; Shay, D.K.; Carias, C.; Bresee, J.S.; Kim, I.K.; Gambhir, M.; Fry, A.M. Deaths Averted by Influenza Vaccination in the U.S. during the Seasons 2005/06 through 2013/14. Vaccine 2015, 33, 3003–3009. [Google Scholar] [CrossRef] [PubMed]
- CDC. 2021–2022 Estimated Flu Illnesses, Medical Visits, Hospitalizations, and Deaths Prevented by Flu Vaccination. Available online: https://www.cdc.gov/flu/about/burden-averted/2021-2022.htm (accessed on 7 May 2023).
- de Figureido, A.; Eagan, R.L.; Hendrickx, G.; Karafillakis, E.; Van Damme, P.; Larson, H.J. State of Vaccine Confidence in the European Union. 2022. Available online: https://health.ec.europa.eu/system/files/2022-11/2022_confidence_rep_en.pdf (accessed on 7 May 2023).
- Narodowy Instytut Zdrowia Publicznego—Państwowy Zakład Higieny. Jaki Jest Poziom Zaszczepienia Przeciw Grypie w Polsce? Available online: https://szczepienia.pzh.gov.pl/faq/jaki-jest-poziom-zaszczepienia-przeciw-grypie-w-polsce/ (accessed on 7 May 2023).
- Jakie Czynniki Będą Determinowały Skalę i Dotkliwość Nadchodzącego Sezonu Grypowego? Available online: https://szczepienia.pzh.gov.pl/faq/jakie-czynniki-beda-determinowaly-skale-i-dotkliwosc-nadchodzacego-sezonu-grypowego (accessed on 7 May 2023).
- Nitsch-Osuch, A.; Gołębiak, I.; Wyszkowska, D.; Rosińska, R.; Kargul, L.; Szuba, B.; Tyszko, P.; Brydak, L.B. Influenza Vaccination Coverage among Polish Patients with Chronic Diseases. Adv. Exp. Med. Biol. 2017, 968, 19–34. [Google Scholar] [PubMed]
- Brydak, L.B.; Woźniak Kosek, A.; Nitsch-Osuch, A. Influenza Vaccines and Vaccinations in Poland—Past, Present and Future. Med. Sci. Monit. 2012, 18, RA166-71. [Google Scholar] [CrossRef]
- Su, W.; Wang, H.; Sun, C.; Li, N.; Guo, X.; Song, Q.; Liang, Q.; Liang, M.; Ding, X.; Sun, Y. The Association between Previous Influenza Vaccination and COVID-19 Infection Risk and Severity: A Systematic Review and Meta-Analysis. Am. J. Prev. Med. 2022, 63, 121–130. [Google Scholar] [CrossRef]
- Conlon, A.; Ashur, C.; Washer, L.; Eagle, K.A.; Hofmann Bowman, M.A. Impact of the Influenza Vaccine on COVID-19 Infection Rates and Severity. Am. J. Infect. Control 2021, 49, 694–700. [Google Scholar] [CrossRef]
- Poniedziałek, B.; Hallmann, E.; Sikora, D.; Szymański, K.; Kondratiuk, K.; Żurawski, J.; Rzymski, P.; Brydak, L. Relationship between Humoral Response in COVID-19 and Seasonal Influenza Vaccination. Vaccines 2022, 10, 1621. [Google Scholar] [CrossRef]
- Samel-Kowalik, P.; Jankowski, M.; Lisiecka-Biełanowicz, M.; Ostrowska, A.; Gujski, M.; Kobuszewski, B.; Pinkas, J.; Raciborski, F. Factors Associated with Attitudes towards Seasonal Influenza Vaccination in Poland: A Nationwide Cross-Sectional Survey in 2020. Vaccines 2021, 9, 1336. [Google Scholar] [CrossRef]
- Korn, L.; Böhm, R.; Meier, N.W.; Betsch, C. Vaccination as a Social Contract. Proc. Natl. Acad. Sci. USA 2020, 117, 14890–14899. [Google Scholar] [CrossRef]
- Bloom, D.E.; Cadarette, D.; Ferranna, M. The Societal Value of Vaccination in the Age of COVID-19. Am. J. Public Health 2021, 111, 1049–1054. [Google Scholar] [CrossRef]
- Sobierajski, T. Społeczny Kontekst Szczepień. In Wprowadzenie Do Wakcynologii Społecznej i Socjologii Szczepień; Alfa Medica: Rzeszów, Poland, 2017. [Google Scholar]
- Conti, A.A. Historical Evolution of the Concept of Health in Western Medicine. Acta Biomed. 2018, 89, 352–354. [Google Scholar]
- Larson, J.S. The World Health Organization’s Definition of Health: Social versus Spiritual Health. Soc. Indic. Res. 1996, 38, 181–192. [Google Scholar] [CrossRef]
- Mittelmark, M.B.; Bull, T.; Bouwman, L. Emerging Ideas Relevant to the Salutogenic Model of Health. In The Handbook of Salutogenesis; Springer International Publishing: Cham, Switzerland, 2017; pp. 45–56. ISBN 9783319045993. [Google Scholar]
- de Figueiredo, A.; Simas, C.; Larson, H.J. COVID-19 Vaccine Acceptance and Its Socio-Demographic and Emotional Determinants: A Multi-Country Cross-Sectional Study. Vaccine 2023, 41, 354–364. [Google Scholar] [CrossRef]
- Vet, R.; de Wit, J.B.; Das, E. Factors Associated with Hepatitis B Vaccination among Men Who Have Sex with Men: A Systematic Review of Published Research. Int. J. STD AIDS 2017, 28, 534–542. [Google Scholar] [CrossRef]
- Sheinfeld Gorin, S.N.; Glenn, B.A.; Perkins, R.B. The Human Papillomavirus (HPV) Vaccine and Cervical Cancer: Uptake and next Steps. Adv. Ther. 2011, 28, 615–639. [Google Scholar] [CrossRef]
- Prematunge, C.; Corace, K.; McCarthy, A.; Nair, R.C.; Pugsley, R.; Garber, G. Factors Influencing Pandemic Influenza Vaccination of Healthcare Workers—A Systematic Review. Vaccine 2012, 30, 4733–4743. [Google Scholar] [CrossRef]
- Nys, T. Autonomy, Trust, and Respect. J. Med. Philos. 2015, 41, 10–24. [Google Scholar] [CrossRef]
- Sofaer, S.; Kreling, B.; Kenney, E.; Swift, E.K.; Dewart, T. Family Members and Friends Who Help Beneficiaries Make Health Decisions. Health Care Financ. Rev. 2001, 23, 105–121. [Google Scholar]
- Watts, M.S. Physicians as Role Models in Society. West. J. Med. 1990, 152, 292. [Google Scholar]
- Waitzkin, H.; Waterman, B. Social Theory and Medicine. Int. J. Health Serv. 1976, 6, 9–23. [Google Scholar] [CrossRef]
- Fisher, K.A.; Nguyen, N.; Fouayzi, H.; Singh, S.; Crawford, S.; Mazor, K.M. Impact of a Physician Recommendation on COVID-19 Vaccination Intent among Vaccine Hesitant Individuals. Patient Educ. Couns. 2023, 106, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Hofstetter, A.M.; Robinson, J.D.; Lepere, K.; Cunningham, M.; Etsekson, N.; Opel, D.J. Clinician-Parent Discussions about Influenza Vaccination of Children and Their Association with Vaccine Acceptance. Vaccine 2017, 35, 2709–2715. [Google Scholar] [CrossRef] [PubMed]
- Shen, A.K.; Browne, S.; Srivastava, T.; Michel, J.J.; Tan, A.S.L.; Kornides, M.L. Factors Influencing Parental and Individual COVID-19 Vaccine Decision Making in a Pediatric Network. Vaccines 2022, 10, 1277. [Google Scholar] [CrossRef] [PubMed]
- Fenton, A.T.; Eun, T.J.; Clark, J.A.; Perkins, R.B. Indicated or Elective? The Association of Providers’ Words with HPV Vaccine Receipt. Hum. Vaccin. Immunother. 2018, 14, 2503–2509. [Google Scholar] [CrossRef]
- Steeb, D.R.; Ramaswamy, R. Recognizing and Engaging Pharmacists in Global Public Health in Limited Resource Settings. J. Glob. Health 2019, 9, 010318. [Google Scholar] [CrossRef]
- Bragazzi, N.; Mansour, M.; Bonsignore, A.; Ciliberti, R. The Role of Hospital and Community Pharmacists in the Management of COVID-19: Towards an Expanded Definition of the Roles, Responsibilities, and Duties of the Pharmacist. Pharmacy 2020, 8, 140. [Google Scholar] [CrossRef]
- Rogers, A.A.; Cook, R.E.; Button, J.A. Parent and Peer Norms Are Unique Correlates of COVID-19 Vaccine Intentions in a Diverse Sample of U.S. Adolescents. J. Adolesc. Health 2021, 69, 910–916. [Google Scholar] [CrossRef]
- Zarębska-Michaluk, D.; Rzymski, P.; Moniuszko-Malinowska, A.; Brzdęk, M.; Martonik, D.; Rorat, M.; Wielgat, J.; Kłos, K.; Musierowicz, W.; Wasilewski, P.; et al. Does Hospitalization Change the Perception of COVID-19 Vaccines among Unvaccinated Patients? Vaccines 2022, 10, 476. [Google Scholar] [CrossRef]
- Kan, T.; Zhang, J. Factors Influencing Seasonal Influenza Vaccination Behaviour among Elderly People: A Systematic Review. Public Health 2018, 156, 67–78. [Google Scholar] [CrossRef]
- Kong, K.L.; Chu, S.; Giles, M.L. Factors Influencing the Uptake of Influenza Vaccine Vary among Different Groups in the Hard-to-reach Population. Aust. N. Z. J. Public Health 2020, 44, 163–168. [Google Scholar] [CrossRef]
- Shaham, A.; Chodick, G.; Shalev, V.; Yamin, D. Personal and Social Patterns Predict Influenza Vaccination Decision. BMC Public Health 2020, 20, 222. [Google Scholar] [CrossRef]
- Stefanoff, P.; Sobierajski, T.; Bulinska-Stangrecka, H.; Augustynowicz, E. Exploring Factors Improving Support for Vaccinations among Polish Primary Care Physicians. PLoS ONE 2020, 15, e0232722. [Google Scholar] [CrossRef]
- Ustawa z Dni 17 Listopada 2021 r. o Zmianie Ustawy o Świadczeniach Opieki Zdrowotnej Finansowanych Ze Środków Publicznych Oraz Niektórych Innych Ustaw, Dz.U. 2021 Poz 2120. Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20210002120 (accessed on 7 May 2023).
- Syan, S.K.; Gohari, M.R.; Levitt, E.E.; Belisario, K.; Gillard, J.; DeJesus, J.; MacKillop, J. COVID-19 Vaccine Perceptions and Differences by Sex, Age, and Education in 1367 Community Adults in Ontario. Front. Public Health 2021, 9, 719665. [Google Scholar] [CrossRef]
- Nessler, K.; Krztoń-Królewiecka, A.; Chmielowiec, T.; Jarczewska, D.; Windak, A. Determinants of Influenza Vaccination Coverage Rates among Primary Care Patients in Krakow, Poland and the Surrounding Region. Vaccine 2014, 32, 7122–7127. [Google Scholar] [CrossRef]
- Kajikawa, N.; Kataoka, Y.; Goto, R.; Maeno, T.; Yokoya, S.; Umeyama, S.; Takahashi, S.; Maeno, T. Factors Associated with Influenza Vaccination in Japanese Elderly Outpatients. Infect. Dis. Health 2019, 24, 212–221. [Google Scholar] [CrossRef]
- Rzymski, P.; Poniedziałek, B.; Fal, A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines 2021, 9, 1286. [Google Scholar] [CrossRef]
- Zhang, M.; Chen, H.; Wu, F.; Li, Q.; Lin, Q.; Cao, H.; Zhou, X.; Gu, Z.; Chen, Q. Heightened Willingness toward Pneumococcal Vaccination in the Elderly Population in Shenzhen, China: A Cross-Sectional Study during the COVID-19 Pandemic. Vaccines 2021, 9, 212. [Google Scholar] [CrossRef]
- Baum, S.; Hitschold, T.; Becker, A.; Smola, S.; Solomayer, E.; Rody, A.; Rissland, J. Implementation of the Recommendation to Vaccinate Pregnant Women against Seasonal Influenza—Vaccination Rates and Acceptance. Geburtshilfe Frauenheilkd. 2017, 77, 340–351. [Google Scholar] [CrossRef]
- Ganczak, M.; Kalinowski, P.; Drozd-Dąbrowska, M.; Biesiada, D.; Dubiel, P.; Topczewska, K.; Molas-Biesiada, A.; Oszutowska-Mazurek, D.; Korzeń, M. School Life and Influenza Immunization: A Cross-Sectional Study on Vaccination Coverage and Influencing Determinants among Polish Teachers. Vaccine 2020, 38, 5548–5555. [Google Scholar] [CrossRef]
- Adadan Güvenç, I.; Parıldar, H.; Şahin, M.K.; Erbek, S.S. Better Knowledge and Regular Vaccination Practices Correlate Well with Higher Seasonal Influenza Vaccine Uptake in People at Risk: Promising Survey Results from a University Outpatient Clinic. Am. J. Infect. Control 2017, 45, 740–745. [Google Scholar] [CrossRef]
- Olatunbosun, O.D.; Esterhuizen, T.M.; Wiysonge, C.S. A Cross Sectional Survey to Evaluate Knowledge, Attitudes and Practices Regarding Seasonal Influenza and Influenza Vaccination among Diabetics in Pretoria, South Africa. Vaccine 2017, 35, 6375–6386. [Google Scholar] [CrossRef] [PubMed]
- van der Linden, S.; Roozenbeek, J.; Compton, J. Inoculating against Fake News about COVID-19. Front. Psychol. 2020, 11, 566790. [Google Scholar] [CrossRef] [PubMed]
- Rzymski, P.; Borkowski, L.; Drąg, M.; Flisiak, R.; Jemielity, J.; Krajewski, J.; Mastalerz-Migas, A.; Matyja, A.; Pyrć, K.; Simon, K.; et al. The Strategies to Support the COVID-19 Vaccination with Evidence-Based Communication and Tackling Misinformation. Vaccines 2021, 9, 109. [Google Scholar] [CrossRef] [PubMed]
- Nowak, B.M.; Miedziarek, C.; Pełczyński, S.; Rzymski, P. Misinformation, Fears and Adherence to Preventive Measures during the Early Phase of COVID-19 Pandemic: A Cross-Sectional Study in Poland. Int. J. Environ. Res. Public Health 2021, 18, 12266. [Google Scholar] [CrossRef]
- Skafle, I.; Nordahl-Hansen, A.; Quintana, D.S.; Wynn, R.; Gabarron, E. Misinformation about COVID-19 Vaccines on Social Media: Rapid Review. J. Med. Internet Res. 2022, 24, e37367. [Google Scholar] [CrossRef]
- Lee, S.K.; Sun, J.; Jang, S.; Connelly, S. Misinformation of COVID-19 Vaccines and Vaccine Hesitancy. Sci. Rep. 2022, 12, 13681. [Google Scholar] [CrossRef]
- Kraśnicka, J.; Krajewska-Kułak, E.; Klimaszewska, K.; Cybulski, M.; Guzowski, A.; Kowalewska, B.; Jankowiak, B.; Rolka, H.; Doroszkiewicz, H.; Kułak, W. Mandatory and Recommended Vaccinations in Poland in the Views of Parents. Hum. Vaccin. Immunother. 2018, 14, 2884–2893. [Google Scholar] [CrossRef]
- Narodowy Instytut Zdrowia Publicznego—Państwowy Zakład Higieny. Jaka jest Liczba Uchyleń Dotyczących Szczepień Obowiązkowych? Available online: https://szczepienia.pzh.gov.pl/faq/jaka-jest-liczba-uchylen-szczepien-obowiazkowych/ (accessed on 7 May 2023).
- Rusli, K.D.B.; Bryar, R. Maximising Influenza Vaccination Awareness and Uptake among Older Adults in Singapore. Br. J. Community Nurs. 2018, 23, 244–249. [Google Scholar] [CrossRef]
- Queeno, B.V. Evaluation of Inpatient Influenza and Pneumococcal Vaccination Acceptance Rates with Pharmacist Education. J. Pharm. Pract. 2017, 30, 202–208. [Google Scholar] [CrossRef]
- Pullagura, G.R.; Waite, N.M.; Houle, S.K.D.; Violette, R.; Wong, W.W.L. Cost-Utility Analysis of Offering a Novel Remunerated Community Pharmacist Consultation Service on Influenza Vaccination for Seniors in Ontario, Canada. J. Am. Pharm. Assoc. 2019, 59, 489–497.e1. [Google Scholar] [CrossRef]
- Kharroubi, G.; Cherif, I.; Bouabid, L.; Gharbi, A.; Boukthir, A.; Ben Alaya, N.; Ben Salah, A.; Bettaieb, J. Influenza Vaccination Knowledge, Attitudes, and Practices among Tunisian Elderly with Chronic Diseases. BMC Geriatr. 2021, 21, 700. [Google Scholar] [CrossRef]
- Quandelacy, T.M.; Viboud, C.; Charu, V.; Lipsitch, M.; Goldstein, E. Age- and Sex-Related Risk Factors for Influenza-Associated Mortality in the United States between 1997–2007. Am. J. Epidemiol. 2014, 179, 156–167. [Google Scholar] [CrossRef]
- Takahashi, O.; Noguchi, Y.; Rahman, M.; Shimbo, T.; Goto, M.; Matsui, K.; Asai, A.; Onishi, M.; Koyama, H.; Sawada, I.; et al. Influence of Family on Acceptance of Influenza Vaccination among Japanese Patients. Fam. Pract. 2003, 20, 162–166. [Google Scholar] [CrossRef]
- Quinn, S.C.; Hilyard, K.M.; Jamison, A.M.; An, J.; Hancock, G.R.; Musa, D.; Freimuth, V.S. The Influence of Social Norms on Flu Vaccination among African American and White Adults. Health Educ. Res. 2017, 32, 473–486. [Google Scholar] [CrossRef]
- Gorman, D.R.; Bielecki, K.; Willocks, L.J.; Pollock, K.G. A Qualitative Study of Vaccination Behaviour amongst Female Polish Migrants in Edinburgh, Scotland. Vaccine 2019, 37, 2741–2747. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Sex | ||
| Female | 428 | 53.1 |
| Male | 377 | 46.9 |
| Age | ||
| 18–24 | 100 | 12.4 |
| 25–34 | 153 | 19.0 |
| 35–49 | 195 | 24.3 |
| 50–64 | 231 | 28.7 |
| 65 and more | 126 | 15.7 |
| Education | ||
| Primary | 29 | 3.6 |
| Vocational | 59 | 7.3 |
| Secondary | 411 | 51.1 |
| Tertiary | 306 | 38.0 |
| Place of living | ||
| Rural area | 323 | 40.1 |
| City < 20 k | 94 | 11.7 |
| City 20–99 k | 154 | 19.1 |
| City 100–199 k | 66 | 8.2 |
| City 200–499 k | 73 | 9.0 |
| City > 500 k | 95 | 11.8 |
| Demographic Categories | Vaccination Supportes | Vaccination Opponents | p-Value | ||
|---|---|---|---|---|---|
| Strong | Moderate | Strong | Moderate | ||
| (n/%) | |||||
| Sex | |||||
| Female | 146/34.2 | 187/43.8 | 69/16.2 | 25/5.9 | 0.309 |
| Male | 146/38.6 | 145/38.4 | 58/15.3 | 29/7.7 | |
| Age | |||||
| 18–24 | 29/28.7 | 39/38.6 | 25/24.8 | 8/7.9 | <0.001 |
| 25–34 | 40/26.1 | 77/50.3 | 23/15.0 | 13/8.5 | |
| 35–49 | 61/31.3 | 78/40.0 | 40/20.5 | 16/8.2 | |
| 50–64 | 96/41.6 | 91/39.4 | 27/11.7 | 17/7.4 | |
| 65 and more | 67/53.2 | 47/37.3 | 11/8.7 | 1/0.8 | |
| Education | |||||
| Primary | 10/34.5 | 12/41.4 | 6/20.7 | 1/3.4 | 0.298 |
| Vocational | 24/40.7 | 21/35.6 | 9/15.3 | 5/8.5 | |
| Secondary | 135/32.8 | 171/41.5 | 75/18.2 | 31/7.5 | |
| Tertiary | 124/40.5 | 129/42.2 | 36/11.8 | 17/5.6 | |
| Place of living | |||||
| Country | 111/34.4 | 132/40.9 | 59/18.3 | 21/6.5 | 0.190 |
| City < 20 k | 35/37.2 | 36/38.3 | 14/14.9 | 9/9.6 | |
| City 20–99 k | 55/35.9 | 70/45.8 | 22/14.4 | 6/3.9 | |
| City 100–199 k | 23/34.2 | 28/41.8 | 15/22.4 | 1/1.5 | |
| City 200–499 k | 28/38.9 | 30/41.7 | 5/6.9 | 9/12.5 | |
| City > 500 k | 39/41.1 | 36/37.9 | 12/12.6 | 8/8.4 | |
| Influence | Median | Percentiles | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sex and Age of Respondents | Very Low | Rather Low | Neither Low nor High | Rather High | Very High | 25th | 50th | 75th | ||
| Physician | ||||||||||
| Sex | ||||||||||
| Female | 58/13.6 | 24/5.6 | 76/17.8 | 118/27.6 | 151/35.4 | 4.00 | 3.00 | 4.00 | 5.00 | 0.151 |
| Male | 30/7.9 | 22/5.8 | 73/19.3 | 115/30.4 | 138/36.5 | 4.00 | 3.00 | 4.00 | 5.00 | |
| Age | ||||||||||
| 18–24 | 8/8.0 | 8/8.0 | 17/17.0 | 30/30.0 | 37/37.0 | 4.00 | 3.00 | 4.00 | 5.00 | 0.003 |
| 25–34 | 14/9.1 | 10/6.5 | 38/24.7 | 49/31.8 | 43/27.9 | 4.00 | 3.00 | 4.00 | 5.00 | |
| 35–49 | 31/16.0 | 17/8.8 | 31/16.0 | 56/28.9 | 59/30.4 | 4.00 | 2.62 | 4.00 | 5.00 | |
| 50–64 | 28/12.1 | 9/3.9 | 41/17.7 | 66/28.6 | 87/37.7 | 4.00 | 3.00 | 4.00 | 5.00 | |
| 65 and more | 7/5.6 | 2/1.6 | 21/16.8 | 32/25.6 | 63/50.4 | 4.88 | 4.00 | 4.88 | 5.00 | |
| Nurse | ||||||||||
| Sex | ||||||||||
| Female | 84/19.6 | 55/12.9 | 145/33.9 | 108/25.2 | 36/8.4 | 3.00 | 2.00 | 3.00 | 4.00 | 0.314 |
| Male | 61/16.1 | 42/11.1 | 124/32.8 | 107/28.3 | 44/11.6 | 3.00 | 2.00 | 3.00 | 4.00 | |
| Age | ||||||||||
| 18–24 | 19/19.0 | 16/16.0 | 31/31.0 | 24/24.0 | 10/10.0 | 3.00 | 2.00 | 3.00 | 4.00 | 0.272 |
| 25–34 | 21/13.8 | 20/13.2 | 53/34.9 | 39/25.7 | 19/12.5 | 3.00 | 2.00 | 3.00 | 4.00 | |
| 35–49 | 45/23.1 | 22/11.3 | 55/28.2 | 54/27.7 | 19/9.7 | 3.00 | 2.00 | 3.00 | 4.00 | |
| 50–64 | 48/20.6 | 27/11.6 | 83/35.6 | 57/24.5 | 18/7.7 | 3.00 | 2.00 | 3.00 | 4.00 | |
| 65 and more | 13/10.3 | 12/9.5 | 47/37.3 | 41/32.5 | 13/10.3 | 3.00 | 3.00 | 3.00 | 4.00 | |
| Pharmacist | ||||||||||
| Sex | ||||||||||
| Female | 95/22.2 | 63/14.7 | 133/31.1 | 107/25.0 | 30/7.0 | 3.00 | 2.00 | 3.00 | 4.00 | 0.011 |
| Male | 53/14.0 | 43/11.4 | 141/37.3 | 109/28.8 | 32/8.5 | 3.00 | 2.00 | 3.00 | 4.00 | |
| Age | ||||||||||
| 18–24 | 18/18.0 | 14/14.0 | 37/37.0 | 25/25.0 | 6/6.0 | 3.00 | 2.00 | 3.00 | 4.00 | 0.033 |
| 25–34 | 21/13.8 | 25/16.4 | 58/38.2 | 32/21.1 | 16/10.5 | 3.00 | 2.00 | 3.00 | 4.00 | |
| 35–49 | 47/24.1 | 27/13.8 | 59/30.3 | 47/24.1 | 15/7.7 | 3.00 | 2.00 | 3.00 | 4.00 | |
| 50–64 | 49/21.2 | 30/13.0 | 74/32.0 | 63/27.3 | 15/6.5 | 3.00 | 2.00 | 3.00 | 4.00 | |
| 65 and more | 13/10.2 | 10/7.9 | 46/36.2 | 48/37.8 | 10/7.9 | 3.00 | 3.00 | 3.00 | 4.00 | |
| Friend/Family Member | ||||||||||
| Sex | ||||||||||
| Female | 81/19.0 | 79/18.5 | 137/32.1 | 97/22.7 | 33/7.7 | 3.00 | 2.00 | 3.00 | 4.00 | 0.378 |
| Male | 55/14.6 | 66/17.5 | 133/35.3 | 98/26.0 | 25/6.6 | 3.00 | 2.00 | 3.00 | 4.00 | |
| Age | ||||||||||
| 18–24 | 12/12.0 | 21/21.0 | 32/32/0 | 27/27.0 | 7/7.0 | 3.00 | 2.00 | 3.00 | 4.00 | 0.043 |
| 25–34 | 20/13.0 | 28/18.2 | 53/34.4 | 32/20.8 | 21/13.6 | 3.00 | 2.00 | 3.00 | 4.00 | |
| 35–49 | 43/22.1 | 34/17.4 | 59/30.3 | 46/23.6 | 13/6.7 | 3.00 | 2.00 | 3.00 | 4.00 | |
| 50–64 | 48/20.8 | 38/16.5 | 76/32.9 | 57/24.7 | 12/5.2 | 3.00 | 2.00 | 3.00 | 4.00 | |
| 65 and more | 14/11.1 | 24/19.0 | 50/39.7 | 33/26.2 | 5/4.0 | 3.00 | 2.00 | 3.00 | 4.00 | |
| Attitude towards Vaccination | Median | Percentiles | p-Value | ||
|---|---|---|---|---|---|
| 25th | 50th | 75th | |||
| Physician | |||||
| Strong vaccine supporter | 5.00 | 4.00 | 5.00 | 5.00 | <0.001 |
| Moderate vaccine supporter | 4.00 | 3.00 | 4.00 | 5.00 | |
| Moderate vaccine opponent | 3.00 | 2.00 | 3.00 | 4.00 | |
| Strong vaccine opponent | 2.44 | 1.00 | 2.44 | 4.00 | |
| Nurse | |||||
| Strong vaccine supporter | 3.00 | 3.00 | 3.00 | 4.00 | <0.001 |
| Moderate vaccine supporter | 3.00 | 2.00 | 3.00 | 4.00 | |
| Moderate vaccine opponent | 3.00 | 1.00 | 3.00 | 4.00 | |
| Strong vaccine opponent | 2.00 | 1.00 | 2.00 | 3.00 | |
| Pharmacist | |||||
| Strong vaccine supporter | 3.00 | 3.00 | 3.00 | 4.00 | <0.001 |
| Moderate vaccine supporter | 3.00 | 2.00 | 3.00 | 4.00 | |
| Moderate vaccine opponent | 3.00 | 1.00 | 3.00 | 4.00 | |
| Strong vaccine opponent | 1.64 | 1.00 | 1.64 | 3.41 | |
| Friend/Family Member | |||||
| Strong vaccine supporter | 3.00 | 2.00 | 3.00 | 4.00 | <0.001 |
| Moderate vaccine supporter | 3.00 | 2.00 | 3.00 | 4.00 | |
| Moderate vaccine opponent | 3.00 | 2.00 | 3.00 | 4.00 | |
| Strong vaccine opponent | 1.00 | 1.00 | 1.00 | 4.00 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sobierajski, T.; Rzymski, P.; Wanke-Rytt, M. The Influence of Recommendation of Medical and Non-Medical Authorities on the Decision to Vaccinate against Influenza from a Social Vaccinology Perspective: Cross-Sectional, Representative Study of Polish Society. Vaccines 2023, 11, 994. https://doi.org/10.3390/vaccines11050994
Sobierajski T, Rzymski P, Wanke-Rytt M. The Influence of Recommendation of Medical and Non-Medical Authorities on the Decision to Vaccinate against Influenza from a Social Vaccinology Perspective: Cross-Sectional, Representative Study of Polish Society. Vaccines. 2023; 11(5):994. https://doi.org/10.3390/vaccines11050994
Chicago/Turabian StyleSobierajski, Tomasz, Piotr Rzymski, and Monika Wanke-Rytt. 2023. "The Influence of Recommendation of Medical and Non-Medical Authorities on the Decision to Vaccinate against Influenza from a Social Vaccinology Perspective: Cross-Sectional, Representative Study of Polish Society" Vaccines 11, no. 5: 994. https://doi.org/10.3390/vaccines11050994