
Impact of COVID-19 Outbreak on Influenza and Pneumococcal Vaccination Uptake: A Multi-Center Retrospective Study


Abstract
:1. Introduction
2. Materials and Methods
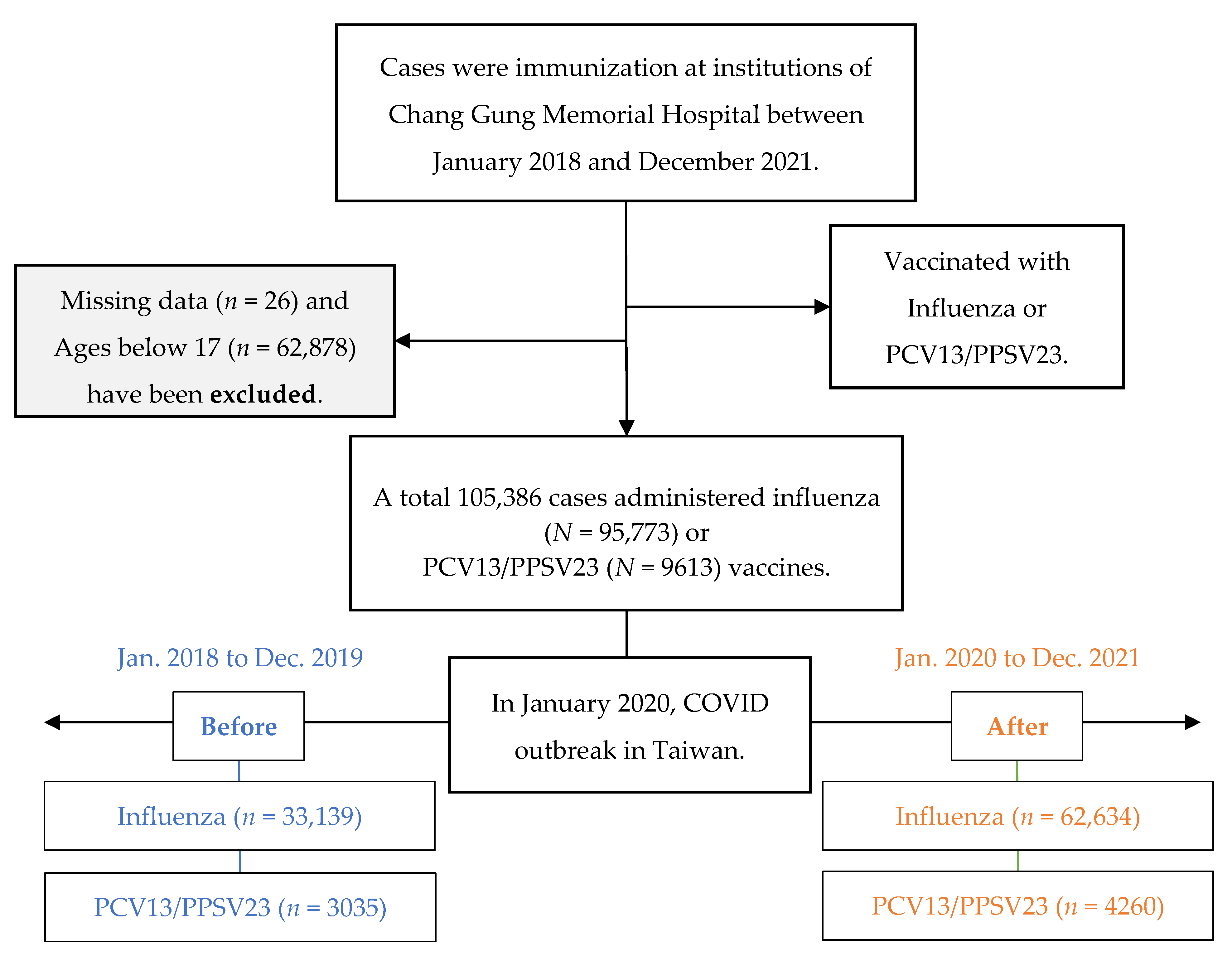
2.1. Participants
2.2. Data Collection
2.3. Outcomes Measure
2.4. Data Analysis
3. Results
3.1. Clinic Population and Duration
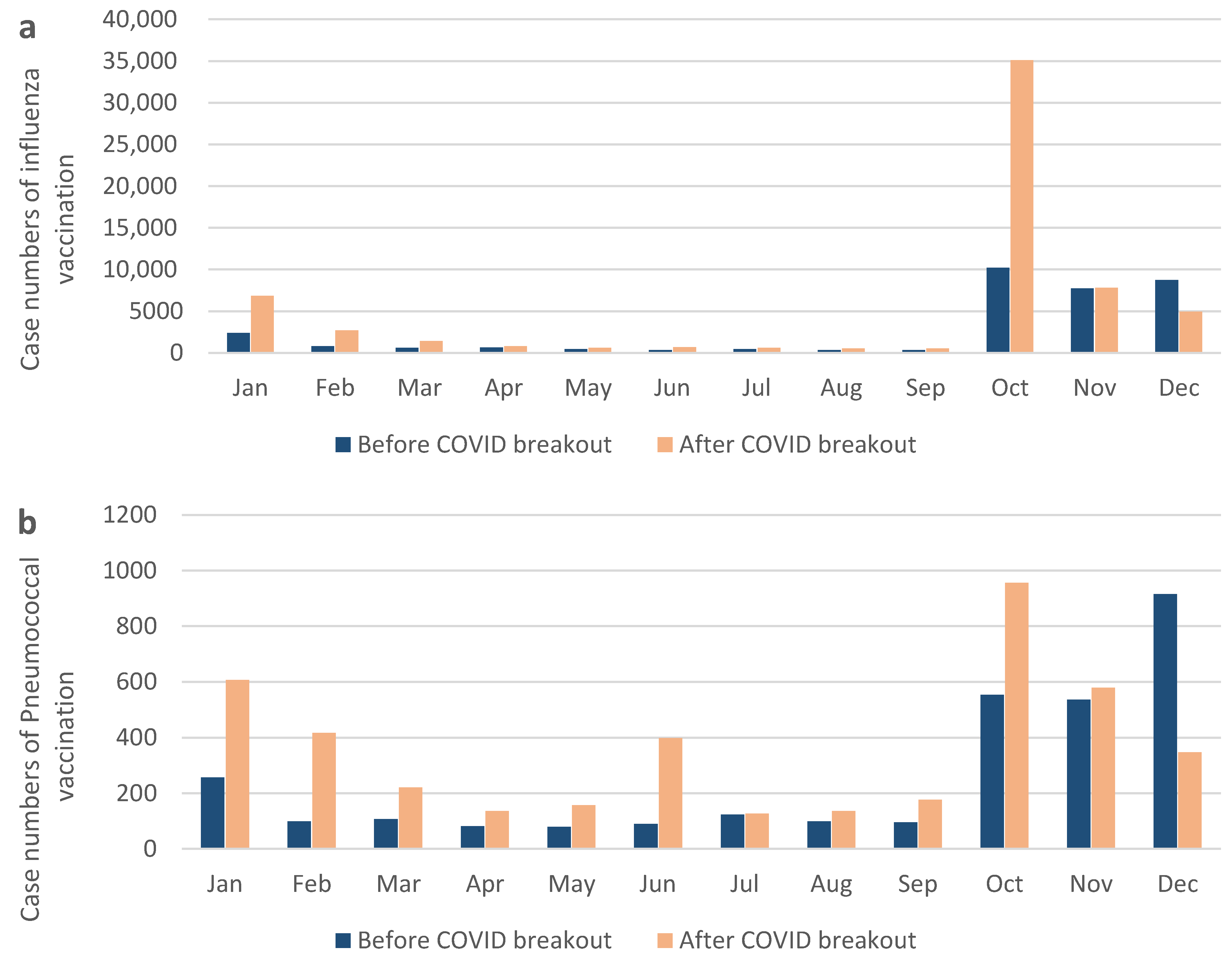
3.2. Influenza Vaccination Cases before and after COVID-19
3.3. Pneumococcal Vaccination Cases before and after COVID-19
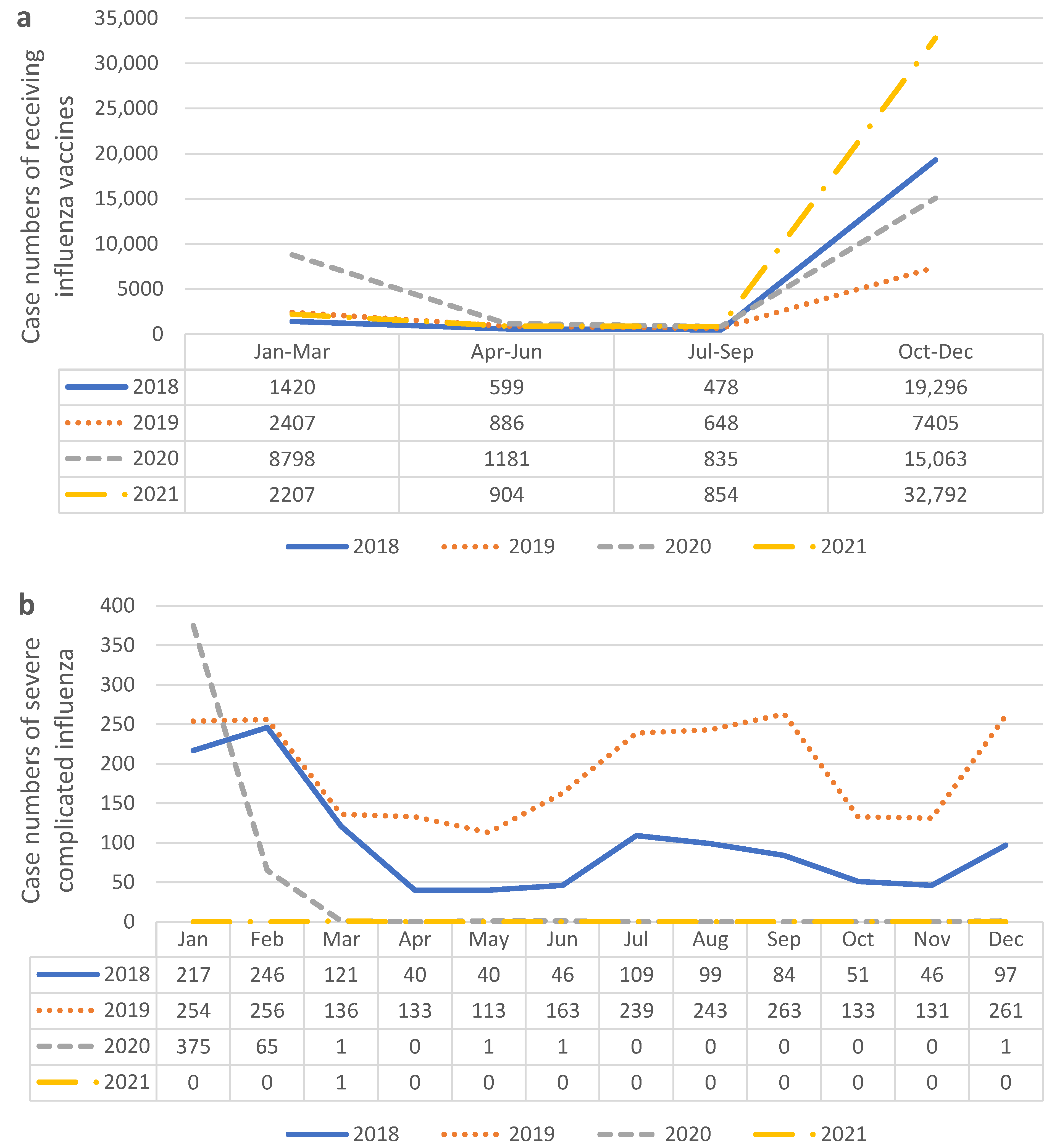
3.4. Influenza and Pneumococcal Vaccination around the COVID-19 Outbreak Point in Taiwan
4. Discussion
4.1. Increased Willingness for Pneumococcal Vaccination after the COVID-19 Pandemic
4.2. Increased Desire for Influenza Vaccination after the COVID-19 Pandemic
4.3. Underlying Diseases in Women after the COVID-19 Pandemic
4.4. Increasing Rate of Vaccination in Taiwan in Contrast to the Global Vaccination Disruption
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Guiding Principles for Immunization Activities During the COVID-19 Pandemic: Interim Guidance, 26 March 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Santoli, J.M. Effects of the COVID-19 pandemic on routine pediatric vaccine ordering and administration—United States, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 591–593. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, S.T.; Trefren, L.; Roth, H.; Moss, A.; Severson, R.; Kempe, A. Number of childhood and adolescent vaccinations administered before and after the COVID-19 outbreak in Colorado. JAMA Pediatr. 2021, 175, 305–307. [Google Scholar] [CrossRef] [PubMed]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Head, K.J.; Kasting, M.L.; Sturm, L.A.; Hartsock, J.A.; Zimet, G.D. A national survey assessing SARS-CoV-2 vaccination intentions: Implications for future public health communication efforts. Sci. Commun. 2020, 42, 698–723. [Google Scholar] [CrossRef]
- Bachtiger, P.; Adamson, A.; Chow, J.J.; Sisodia, R.; Quint, J.K.; Peters, N.S. The impact of the COVID-19 pandemic on the uptake of influenza vaccine: UK-wide observational study. JMIR Public Health Surveill. 2021, 7, e26734. [Google Scholar] [CrossRef]
- Marín-Hernández, D.; Schwartz, R.E.; Nixon, D.F. Epidemiological evidence for association between higher influenza vaccine uptake in the elderly and lower COVID-19 deaths in Italy. J. Med. Virol. 2020, 93, 64. [Google Scholar] [CrossRef]
- Iacobucci, G. Covid-19: Risk of death more than doubled in people who also had flu, English data show. Br. Med. J. Publ. Group 2020, 370, m3720. [Google Scholar] [CrossRef]
- Guo, L.; Wei, D.; Zhang, X.; Wu, Y.; Li, Q.; Zhou, M.; Qu, J. Clinical features predicting mortality risk in patients with viral pneumonia: The MuLBSTA score. Front. Microbiol. 2019, 10, 2752. [Google Scholar] [CrossRef]
- Bengoechea, J.A.; Bamford, C.G. SARS-CoV-2, bacterial co-infections, and AMR: The deadly trio in COVID-19? EMBO Mol. Med. 2020, 12, e12560. [Google Scholar] [CrossRef]
- Lai, C.-C.; Wang, C.-Y.; Hsueh, P.-R. Co-infections among patients with COVID-19: The need for combination therapy with non-anti-SARS-CoV-2 agents? J. Microbiol. Immunol. Infect. 2020, 53, 505–512. [Google Scholar] [CrossRef]
- Cox, M.J.; Loman, N.; Bogaert, D.; O'Grady, J. Co-infections: Potentially lethal and unexplored in COVID-19. Lancet Microbe 2020, 1, e11. [Google Scholar] [CrossRef]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef]
- Pawlowski, C.; Puranik, A.; Bandi, H.; Venkatakrishnan, A.J.; Agarwal, V.; Kennedy, R.; O’Horo, J.C.; Gores, G.J.; Williams, A.W.; Halamka, J.; et al. Exploratory analysis of immunization records highlights decreased SARS-CoV-2 rates in individuals with recent non-COVID-19 vaccinations. Sci. Rep. 2021, 11, 4741. [Google Scholar] [CrossRef]
- Tsai, M.S.; Lin, M.H.; Lee, C.P.; Yang, Y.H.; Chen, W.C.; Chang, G.H.; Tsai, Y.T.; Chen, P.C.; Tsai, Y.H. Chang Gung Research Database: A multi-institutional database consisting of original medical records. Biomed. J. 2017, 40, 263–269. [Google Scholar] [CrossRef]
- Invasive Pneumoccocal Disease. Taiwan Centers of Disease Control. Available online: https://www.cdc.gov.tw/En/Category/ListContent/bg0g_VU_Ysrgkes_KRUDgQ?uaid=lS42udX_s0u2fN0qLcdrnw (accessed on 30 April 2023).
- Liu, Y.C.; Liao, C.H.; Chang, C.F.; Chou, C.C.; Lin, Y.R. A Locally Transmitted Case of SARS-CoV-2 Infection in Taiwan. N. Engl. J. Med. 2020, 382, 1070–1072. [Google Scholar] [CrossRef]
- Liu, Y.C.; Kuo, R.L.; Shih, S.R. COVID-19: The first documented coronavirus pandemic in history. Biomed. J. 2020, 43, 328–333. [Google Scholar] [CrossRef]
- Kung, C.T.; Wu, K.H.; Wang, C.C.; Lin, M.C.; Lee, C.H.; Lien, M.H. Effective strategies to prevent in-hospital infection in the emergency department during the novel coronavirus disease 2019 pandemic. J. Microbiol. Immunol. Infect. 2021, 54, 120–122. [Google Scholar] [CrossRef]
- World Health Organization. Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease is suspected. Interim guidance. Paediatr. Fam. Med. 2020, 16, 9. [Google Scholar]
- Morris, D.E.; Cleary, D.W.; Clarke, S.C. Secondary bacterial infections associated with influenza pandemics. Front. Microbiol. 2017, 8, 1041. [Google Scholar] [CrossRef]
- Huijts, S.M.; Coenjaerts, F.E.J.; Bolkenbaas, M.; van Werkhoven, C.H.; Grobbee, D.E.; Bonten, M.J.M. CAPiTA Study Team The impact of 13-valent pneumococcal conjugate vaccination on virus-associated community-acquired pneumonia in elderly: Exploratory analysis of the CAPiTA trial. Clin. Microbiol. Infect. 2018, 24, 764–770. [Google Scholar] [CrossRef]
- Nunes, M.C.; Cutland, C.L.; Klugman, K.P.; Madhi, S.A. Pneumococcal conjugate vaccine protection against coronavirus-associated pneumonia hospitalization in children living with and without HIV. Mbio 2021, 12, e02347-20. [Google Scholar] [CrossRef] [PubMed]
- Palmu, A.A.; Jokinen, J.; Borys, D.; Nieminen, H.; Ruokokoski, E.; Siira, L.; Puumalainen, T.; Lommel, P.; Hezareh, M.; Moreira, M.; et al. Effectiveness of the ten-valent pneumococcal Haemophilus influenzae protein D conjugate vaccine (PHiD-CV10) against invasive pneumococcal disease: A cluster randomised trial. Lancet 2013, 381, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Loubet, P.; Sotto, A.; AVNIR Group. Covid-19 pandemic: An opportunity to seize to increase awareness and vaccine coverage in at-risk populations. Hum. Vaccines Immunother. 2021, 17, 3472–3473. [Google Scholar] [CrossRef] [PubMed]
- Fink, G.; Orlova-Fink, N.; Schindler, T.; Grisi, S.; Ferrer, A.P.S.; Daubenberger, C.; Brentani, A. Inactivated trivalent influenza vaccination is associated with lower mortality among patients with COVID-19 in Brazil. BMJ Evid. -Based Med. 2021, 26, 192–193. [Google Scholar] [CrossRef]
- Maor, Y.; Caspi, S. Attitudes towards influenza, and COVID-19 vaccines during the COVID-19 pandemic among a representative sample of the Jewish Israeli population. PLoS ONE 2022, 17, e0255495. [Google Scholar] [CrossRef]
- Conlon, A.; Ashur, C.; Washer, L.; Eagle, K.A.; Bowman, M.A.H. Impact of the influenza vaccine on COVID-19 infection rates and severity. Am. J. Infect. Control. 2021, 49, 694–700. [Google Scholar] [CrossRef]
- O’Connor, E.; Teh, J.; Kamat, A.M.; Lawrentschuk, N. Bacillus Calmette Guérin (BCG) vaccination use in the fight against COVID-19–what’s old is new again? Future Med. 2020, 16, 1323–1325. [Google Scholar] [CrossRef]
- Salem, M.L.; El-Hennawy, D. The possible beneficial adjuvant effect of influenza vaccine to minimize the severity of COVID-19. Med. Hypotheses 2020, 140, 109752. [Google Scholar] [CrossRef]
- Zanettini, C.; Omar, M.; Dinalankara, W.; Imada, E.L.; Colantuoni, E.; Parmigiani, G.; Marchionni, L. Influenza Vaccination and COVID19 Mortality in the USA: An Ecological Study. Vaccines 2021, 9, 427. [Google Scholar] [CrossRef]
- Ragni, P.; Marino, M.; Formisano, D.; Bisaccia, E.; Scaltriti, S.; Bedeschi, E.; Grilli, R. Association between exposure to influenza vaccination and COVID-19 diagnosis and outcomes. Vaccines 2020, 8, 675. [Google Scholar] [CrossRef]
- Jiang, B.; Huang, Q.; Jia, M.; Xue, X.; Wang, Q.; Yang, W.; Feng, L. Association between influenza vaccination and SARS-CoV-2 infection and its outcomes: Systematic review and meta-analysis. Chin. Med. J. 2022, 135, 2282–2293. [Google Scholar] [CrossRef]
- Kapoula, G.V.; Vennou, K.E.; Bagos, P.G. Influenza and Pneumococcal Vaccination and the Risk of COVID-19: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 3086. [Google Scholar] [CrossRef]
- Wang, R.; Liu, M.; Liu, J. The Association between Influenza Vaccination and COVID-19 and Its Outcomes: A Systematic Review and Meta-Analysis of Observational Studies. Vaccines 2021, 9, 529. [Google Scholar] [CrossRef]
- Interim Guidance for Routine and Influenza Immunization Services during the COVID-19 Pandemic. US Centers of Disease Control. Available online: https://www.cdc.gov/vaccines/pandemic-guidance/index.html#print (accessed on 30 April 2023).
- Influenza and COVID-19. Taiwan Centers of Disease Control. 19 September 2022. Available online: https://www.cdc.gov.tw/Category/QAPage/5iyc1MHv7KmUolKXhypPeQ (accessed on 30 April 2023).
- Rozbroj, T.; Lyons, A.; Lucke, J. Psychosocial and demographic characteristics relating to vaccine attitudes in Australia. Patient Educ. Couns. 2019, 102, 172–179. [Google Scholar] [CrossRef]
- Komada, M.T.; Lee, J.S.; Watanabe, E.; Nakazawa, E.; Mori, K.; Akabayashi, A. Factors of influenza vaccine inoculation and non-inoculation behavior of community-dwelling residents in Japan: Suggestions for vaccine policy and public health ethics after COVID-19. Vaccine X 2023, 13, 100245. [Google Scholar] [CrossRef]
- Redondo Margüello, E.; Trilla, A.; Munguira, I.L.; López-Herce, A.J.; Cotarelo Suárez, M. Knowledge, attitudes, beliefs and barriers of healthcare professionals and adults ≥65 years about vaccine-preventable diseases in Spain: The ADult Vaccination drIverS and barriErs (ADVISE) study. Hum. Vaccines Immunother. 2022, 18, 2025007. [Google Scholar] [CrossRef]
- Banach, D.B.; Ornstein, K.; Factor, S.H.; Soriano, T.A. Seasonal influenza vaccination among homebound elderly receiving home-based primary care in New York City. J. Community Health 2012, 37, 10–14. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Schneeberg, A.; Bettinger, J.A.; McNeil, S.; Ward, B.J.; Dionne, M.; Cooper, C.; Coleman, B.; Loeb, M.; Rubinstein, E.; McElhaney, J.; et al. Knowledge, attitudes, beliefs and behaviours of older adults about pneumococcal immunization, a Public Health Agency of Canada/Canadian Institutes of Health Research Influenza Research Network (PCIRN) investigation. BMC Public Health 2014, 14, 442. [Google Scholar] [CrossRef]
- MacDougall, D.M.; Halperin, B.A.; MacKinnon-Cameron, D.; Li, L.; McNeil, S.A.; Langley, J.M.; Halperin, S.A. The challenge of vaccinating adults: Attitudes and beliefs of the Canadian public and healthcare providers. BMJ Open 2015, 5, e009062. [Google Scholar] [CrossRef]
- Higuchi, M.; Narumoto, K.; Goto, T.; Inoue, M. Correlation between family physician’s direct advice and pneumococcal vaccination intention and behavior among the elderly in Japan: A cross-sectional study. BMC Fam. Pract. 2018, 19, 153. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, M.; Aoki, T.; Goto, R.; Ozone, S.; Haruta, J. Better patient experience is associated with better vaccine uptake in older adults: Multicentered cross-sectional study. J. Gen. Intern. Med. 2020, 35, 3485–3491. [Google Scholar] [CrossRef] [PubMed]
- Kizmaz, M.; Kumtepe Kurt, B.; Çetin Kargin, N.; Döner, E. Influenza, pneumococcal and herpes zoster vaccination rates among patients over 65 years of age, related factors, and their knowledge and attitudes. Aging Clin. Exp. Res. 2020, 32, 2383–2391. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.W.; Leng, C.H.; Chan, T.C. Determinants of personal vaccination hesitancy before and after the mid-2021 COVID-19 outbreak in Taiwan. PLoS ONE 2022, 17, e0270349. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Pulse Survey on Continuity of Essential Health Services during the COVID-19 Pandemic: Interim Report, 27 August 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Harris, R.C.; Chen, Y.; Côte, P.; Ardillon, A.; Nievera, M.C.; Ong-Lim, A.; Aiyamperumal, S.; Chong, C.P.; Kandasamy, K.V.; Mahenthiran, K.; et al. Impact of COVID-19 on routine immunisation in South-East Asia and Western Pacific: Disruptions and solutions. Lancet Reg. Health-West. Pac. 2021, 10, 100140. [Google Scholar] [CrossRef]
- McDonald, H.I.; Tessier, E.; White, J.M.; Woodruff, M.; Knowles, C.; Bates, C.; Parry, J.; Walker, J.L.; Scott, J.A.; Smeeth, L.; et al. Early impact of the coronavirus disease (COVID-19) pandemic and physical distancing measures on routine childhood vaccinations in England, January to April 2020. Eurosurveillance 2020, 25, 2000848. [Google Scholar] [CrossRef]
- Bramer, C.A.; Kimmins, L.M.; Swanson, R.; Kuo, J.; Vranesich, P.; Jacques-Carroll, L.A.; Shen, A.K. Decline in child vaccination coverage during the COVID-19 pandemic—Michigan Care Improvement Registry, May 2016–May 2020. Am. J. Transplant. 2020, 20, 1930. [Google Scholar] [CrossRef]
- Chandir, S.; Siddiqi, D.A.; Mehmood, M.; Setayesh, H.; Siddique, M.; Mirza, A.; Soundardjee, R.; Dharma, V.K.; Shah, M.T.; Abdullah, S.; et al. Impact of COVID-19 pandemic response on uptake of routine immunizations in Sindh, Pakistan: An analysis of provincial electronic immunization registry data. Vaccine 2020, 38, 7146–7155. [Google Scholar] [CrossRef]
- Chiu, N.C.; Lo, K.H.; Chen, C.C.; Huang, S.Y.; Weng, S.L.; Wang, C.J.; Kuo, H.H.; Chi, H.; Lien, C.H.; Tai, Y.L.; et al. The impact of COVID-19 on routine vaccinations in Taiwan and an unexpected surge of pneumococcal vaccination. Hum. Vaccines Immunother. 2022, 18, e2071079. [Google Scholar] [CrossRef]
- Lewnard, J.A.; Bruxvoort, K.J.; Fischer, H.; Hong, V.X.; Grant, L.R.; Jódar, L.; Gessner, B.D.; Tartof, S.Y. Prevention of Coronavirus Disease 2019 Among Older Adults Receiving Pneumococcal Conjugate Vaccine Suggests Interactions Between Streptococcus pneumoniae and Severe Acute Respiratory Syndrome Coronavirus 2 in the Respiratory Tract. J. Infect. Dis. 2021, 225, 1710–1720. [Google Scholar] [CrossRef]
- Wu, T.-Y.; Majeed, A.; Kuo, K.N. An overview of the healthcare system in Taiwan. Lond. J. Prim. Care 2010, 3, 115–119. [Google Scholar] [CrossRef]
- Taiwan Centers for Disease Control. Vaccine-Preventable Diseases Control. Available online: https://www.cdc.gov.tw/En/Category/ListPage/4TFK95zgsUb9k8XYFFj2Dw (accessed on 30 November 2022).
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A global map of COVID-19 vaccine acceptance rates per country: An updated concise narrative review. J. Multidiscip. Healthc. 2022, 15, 21–45. [Google Scholar] [CrossRef]
- Dyer, O. COVID-19: Variants are spreading in countries with low vaccination rates. BMJ 2021, 373, n1359. [Google Scholar] [CrossRef]
- Kuo, Y.J.; Chen, Y.P.; Wang, H.W.; Liu, C.H.; Strong, C.; Saffari, M.; Ko, N.Y.; Lin, C.Y.; Griffiths, M.D. Community outbreak moderates the association between COVID-19-related behaviors and COVID-19 fear among older people: A one-year longitudinal study in Taiwan. Front. Med. 2021, 8, 2609. [Google Scholar] [CrossRef]
- Lee, S.Y.D.; Tsai, T.I.; Tsai, Y.W.; Kuo, K.N. Health literacy, health status, and healthcare utilization of Taiwanese adults: Results from a national survey. BMC Public Health 2010, 10, 614. [Google Scholar] [CrossRef]
- Duong, V.T.; Lin, I.F.; Sorensen, K.; Pelikan, J.M.; Van Den Broucke, S.; Lin, Y.C.; Chang, P.W. Health Literacy in Taiwan: A Population-Based Study. Asia Pac. J. Public Health 2015, 27, 871–880. [Google Scholar] [CrossRef]
- World Health Organization. Guidance on Routine Immunization Services during COVID-19 Pandemic in the WHO European Region, 20 March 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Wang, C.W.; de Jong, E.P.; Faure, J.A.; Ellington, J.L.; Chen, C.H.S.; Chan, C.C. A matter of trust: A qualitative comparison of the determinants of COVID-19 vaccine hesitancy in Taiwan, the United States, the Netherlands, and Haiti. Hum. Vaccines Immunother. 2022, 18, e2050121. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Before Outbreak (n = 33,139) | After Outbreak (n = 62,634) | p-Value | |
|---|---|---|---|
| Age | 66 ± 13.8 | 54 ± 18.3 | <0.001 |
| Male sex | 16,471 (49.7%) | 25,319 (40.4%) | <0.001 |
| Location | |||
| Kaohsiung institution | 24,170 (72.9%) | 36,734 (58.6%) | <0.001 |
| Chiayi institution | 706 (2.1%) | 3465 (5.5%) | |
| Linkou institution | 5956 (18%) | 18,079 (28.9%) | |
| Keelung institution | 2307 (7%) | 4356 (7%) | |
| Without underlying diseases | 9298 (28.1%) | 31,554 (50.4%) | <0.001 |
| Underlying diseases | |||
| Hypertension | 16,725 (50.5%) | 21,143 (33.8%) | <0.001 |
| Diabetes mellitus | 11,485 (34.7%) | 14,342 (22.9%) | <0.001 |
| Liver cirrhosis | 1177 (3.6%) | 1266 (2%) | <0.001 |
| End stage renal disease | 971 (2.9%) | 1472 (2.4%) | <0.001 |
| Coronary artery disease | 4515 (13.6%) | 5191 (8.3%) | <0.001 |
| Heart failure | 1989 (6%) | 2140 (3.4%) | <0.001 |
| Cerebrovascular accident | 5135 (15.5%) | 6882 (11%) | <0.001 |
| Malignancy | 5770 (17.4%) | 7511 (12%) | <0.001 |
| Before Outbreak (n = 3035) | After Outbreak (n = 4260) | p-Value | |
|---|---|---|---|
| Age | 72 ± 12.1 | 68 ± 14.5 | <0.001 |
| Male sex | 1508 (49.7%) | 2011 (47.2%) | 0.037 |
| Location | |||
| Kaohsiung institution | 1953 (64.3%) | 2617 (61.4%) | 0.240 |
| Chiayi institution | 125 (4.1%) | 193 (4.5%) | |
| Linkou institution | 670 (22.1%) | 966 (22.7%) | |
| Keelung institution | 287 (9.5%) | 484 (11.4%) | |
| Vaccine type | |||
| PCV13 | 1366 (45.0%) | 2620 (61.5%) | <0.001 |
| PPSV23 | 1669 (55.0%) | 1640 (38.5%) | |
| Without underlying diseases | 807 (26.6%) | 1320 (31.0%) | <0.001 |
| Underlying diseases | |||
| Hypertension | 1675 (55.2%) | 2157 (50.6%) | <0.001 |
| Diabetes mellitus | 1181 (38.9%) | 1512 (35.5%) | 0.003 |
| Liver cirrhosis | 95 (3.1%) | 111 (2.6%) | 0.183 |
| End stage renal disease | 91 (3%) | 143 (3.4%) | 0.392 |
| Coronary artery disease | 379 (12.5%) | 534 (12.5%) | 0.952 |
| Heart failure | 199 (6.6%) | 263 (6.2%) | 0.508 |
| Cerebrovascular accident | 499 (16.4%) | 698 (16.4%) | 0.949 |
| Malignancy | 531 (17.5%) | 682 (16%) | 0.093 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lan, C.; Chen, Y.-C.; Chang, Y.-I.; Chuang, P.-C. Impact of COVID-19 Outbreak on Influenza and Pneumococcal Vaccination Uptake: A Multi-Center Retrospective Study. Vaccines 2023, 11, 986. https://doi.org/10.3390/vaccines11050986
Lan C, Chen Y-C, Chang Y-I, Chuang P-C. Impact of COVID-19 Outbreak on Influenza and Pneumococcal Vaccination Uptake: A Multi-Center Retrospective Study. Vaccines. 2023; 11(5):986. https://doi.org/10.3390/vaccines11050986
Chicago/Turabian StyleLan, Chieh, Yi-Chun Chen, Ye-In Chang, and Po-Chun Chuang. 2023. "Impact of COVID-19 Outbreak on Influenza and Pneumococcal Vaccination Uptake: A Multi-Center Retrospective Study" Vaccines 11, no. 5: 986. https://doi.org/10.3390/vaccines11050986