
COVID-19 Prevention Behaviours and Vaccine Acceptability, and Their Association with a Behaviour Change Campaign in Somalia: Analysis of a Longitudinal Cohort
 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
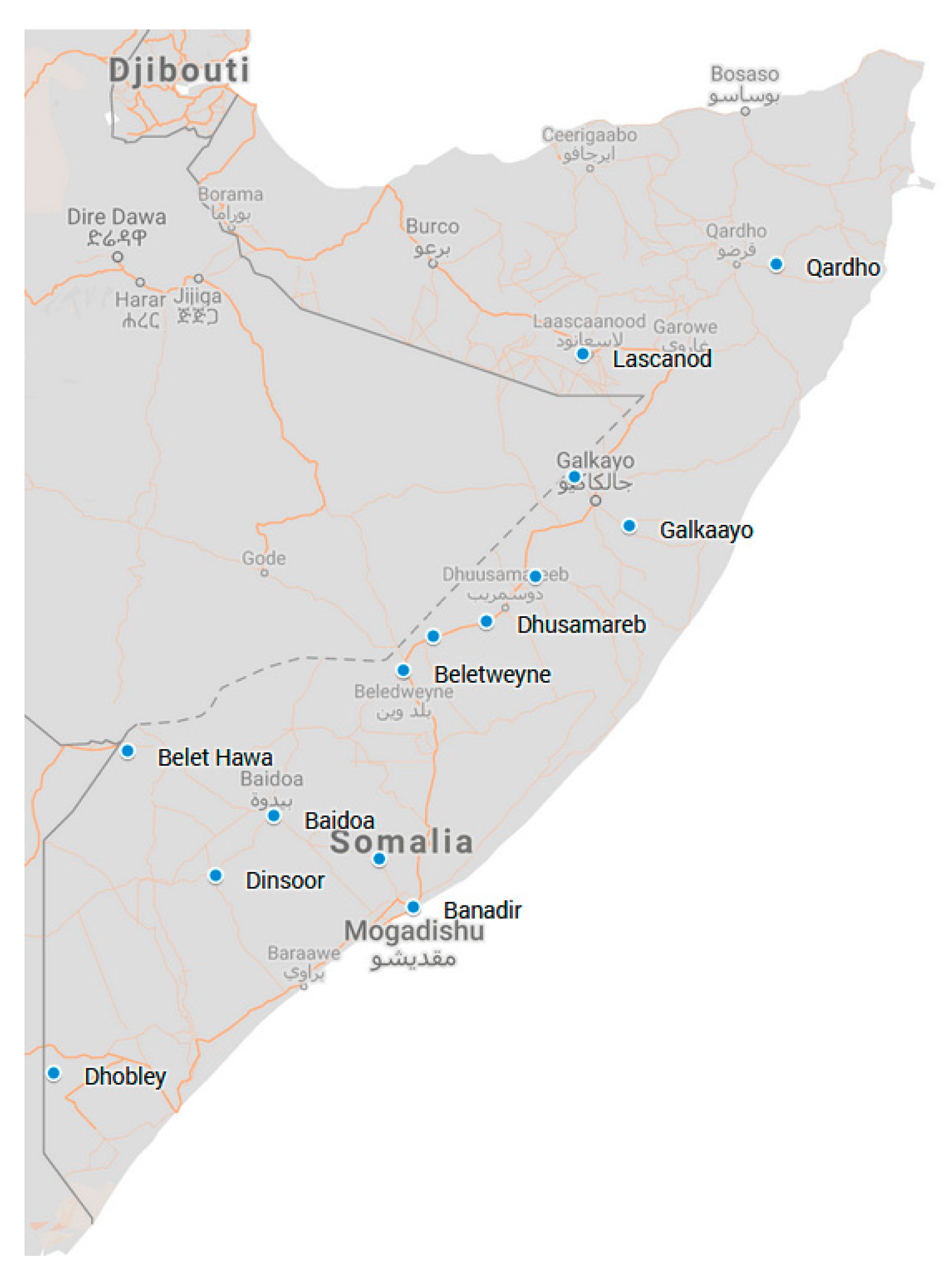
2.1. Setting
2.2. Study Design
2.3. Design of the SBCC Campaign
2.3.1. Content Design and Production
2.3.2. Influencers
2.3.3. Communication Channels
2.3.4. Targeting Hard to Reach Groups
2.3.5. Content Approval, Hosting, and Dissemination
2.4. Study Participants
2.5. Data Collection
2.6. Data Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Greenhalgh, T.; Griffin, S.; Gurdasani, D.; Hamdy, A.; Katzourakis, A.; McKee, M.; Michie, S.; Pagel, C.; Roberts, A.; Yates, K.; et al. Covid-19: An urgent call for global “vaccines-plus” action. BMJ 2022, 376, o1. [Google Scholar]
- Singanayagam, A.; Hakki, S.; Dunning, J.; Madon, K.J.; Crone, M.A.; Koycheva, A.; Derqui-Fernandez, N.; Barnett, J.L.; Whitfield, M.G.; Varro, R.; et al. Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: A prospective, longitudinal, cohort study. Lancet Infect. Dis. 2021, 22, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Razai, M.S.; Chaudhry, U.A.; Doerholt, K.; Bauld, L.; Majeed, A. COVID-19 vaccination hesitancy. BMJ 2021, 373, n1138. [Google Scholar] [CrossRef] [PubMed]
- Burke, P.F.; Masters, D.; Massey, G. Enablers and barriers to COVID-19 vaccine uptake: An international study of perceptions and intentions. Vaccine 2021, 39, 5116–5128. [Google Scholar] [CrossRef]
- Hassan, W.; Kazmi, S.K.; Tahir, M.J.; Ullah, I.; Royan, H.A.; Fahriani, M.; Nainu, F.; Rosa, S.G. Global acceptance and hesitancy of COVID-19 vaccination: A narrative review. Narra J. 2021, 1, 57–68. [Google Scholar] [CrossRef]
- Joshi, A.; Kaur, M.; Kaur, R.; Grover, A.; Nash, D.; El-Mohandes, A. Predictors of COVID-19 Vaccine Acceptance, Intention, and Hesitancy: A Scoping Review. Front. Public Health 2021, 9, 698111. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Moran, C.; Campbell, D.J.T.; Campbell, T.S.; Roach, P.; Bourassa, L.; Collins, Z.; Stasiewicz, M.; McLane, P. Predictors of attitudes and adherence to COVID-19 public health guidelines in Western countries: A rapid review of the emerging literature. J. Public Health 2021, 43, 739–753. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef]
- Limbu, Y.B.; Huhmann, B.A. Why Some People Are Hesitant to Receive COVID-19 Boosters: A Systematic Review. Trop. Med. Infect. Dis. 2023, 8, 159. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.; Wong, J.Y.; Cowling, B.J. Nonpharmaceutical interventions for managing SARS-CoV-2. Curr. Opin. Pulm. Med. 2023, 29, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Kairiza, T.; Kembo, G.; Chigusiwa, L. Herding behavior in COVID-19 vaccine hesitancy in rural Zimbabwe: The moderating role of health information under heterogeneous household risk perceptions. Soc. Sci. Med. 2023, 323, 115854. [Google Scholar] [CrossRef] [PubMed]
- Mutombo, P.N.; Fallah, M.P.; Munodawafa, D.; Kabel, A.; Houeto, D.; Goronga, T.; Mweemba, O.; Balance, G.; Onya, H.; Kamba, R.S.; et al. COVID-19 vaccine hesitancy in Africa: A call to action. Lancet Glob. Health 2021, 10, e320–e321. [Google Scholar] [CrossRef] [PubMed]
- Ackah, B.B.B.; Woo, M.; Stallwood, L.; Fazal, Z.A.; Okpani, A.; Ukah, U.V.; Adu, P.A. COVID-19 vaccine hesitancy in Africa: A scoping review. Glob. Health Res. Policy 2022, 7, 21. [Google Scholar] [CrossRef]
- Cooper, S.; van Rooyen, H.; Wiysonge, C.S. COVID-19 vaccine hesitancy in South Africa: How can we maximize uptake of COVID-19 vaccines? Expert Rev. Vaccines 2021, 20, 921–933. [Google Scholar] [CrossRef]
- Njoga, E.O.; Awoyomi, O.J.; Onwumere-Idolor, O.S.; Awoyomi, P.O.; Ugochukwu, I.C.; Ozioko, S.N. Persisting Vaccine Hesitancy in Africa: The Whys, Global Public Health Consequences and Ways-Out-COVID-19 Vaccination Acceptance Rates as Case-in-Point. Vaccines 2022, 10, 1934. [Google Scholar] [CrossRef]
- Siddiqui, A.; Priya; Adnan, A.; Abbas, S.; Qamar, K.; Islam, Z.; Rahmat, Z.S.; Essar, M.Y.; Farahat, R.A. COVID-19 vaccine hesitancy in conflict zones: A review of current literature. Front. Public Health 2022, 10, 1006271. [Google Scholar] [CrossRef]
- Van den Broucke, S. Why health promotion matters to the COVID-19 pandemic, and vice versa. Health Promot. Int. 2020, 35, 181–186. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Wood, C.E.; Kostkova, P. Vaccine hesitancy and behavior change theory-based social media interventions: A systematic review. Transl. Behav. Med. 2021, 12, 243–272. [Google Scholar] [CrossRef]
- OCHA. Ministry of Health M. COVID-19 Dashboard, Somalia 2020. Available online: https://covid19som-ochasom.hub.arcgis.com/ (accessed on 23 March 2021).
- Warsame, A.; Bashiir, F.; Freemantle, T.; Williams, C.; Vazquez, Y.; Reeve, C.; Aweis, A.; Ahmed, M.; Checchi, F.; Dalmar, A. Excess mortality during the COVID-19 pandemic: A geospatial and statistical analysis in Mogadishu, Somalia. Int. J. Infect. Dis. 2021, 113, 190–199. [Google Scholar] [CrossRef]
- Seal, A.; Jelle, M.; Nemeth, B.; Hassan, M.Y.; Farah, D.A.; Musili, F.M.; Asol, G.S.; Grijalva-Eternod, C.; Fottrell, E. Data innovation in response to COVID-19 in Somalia: Application of a syndromic case definition and rapid mortality assessment method. Global Health Action 2022, 14, 1983106. [Google Scholar] [CrossRef]
- Ahmed, M.A.M.; Fodjo, J.N.S.; Gele, A.A.; Farah, A.A.; Osman, S.; Guled, I.A.; Ali, A.M.; Colebunders, R. COVID-19 in Somalia: Adherence to Preventive Measures and Evolution of the Disease Burden. Pathogens 2020, 9, 735. [Google Scholar] [CrossRef] [PubMed]
- Gele, A.; Farah, A.A. COVID-19 response in Somalia: A comparative look. BMJ 2020, 386, m1090. [Google Scholar]
- BBC. Somalia Country Profile: BBC. 2018. Available online: https://www.bbc.co.uk/news/world-africa-14094503 (accessed on 1 June 2022).
- Risk Communication and Community Engagement (RCCE). OCHA Information Mangaement Unit and the Federal Government of Somalia. 2021. Available online: https://covid19som-ochasom.hub.arcgis.com/pages/rcce (accessed on 21 December 2021).
- NRC. BRCiS Consortium—Building Resilient Communities in Somalia: Norwegian Refugee Council. 2020. Available online: https://www.nrc.no/what-we-do/brcis-consortium---building-resilient-communities-in-somalia/ (accessed on 3 September 2021).
- Dhama, K.; Nainu, F.; Frediansyah, A.; Yatoo, M.I.; Mohapatra, R.K.; Chakraborty, S.; Zhou, H.; Islam, M.R.; Mamada, S.S.; Kusuma, H.I.; et al. Global emerging Omicron variant of SARS-CoV-2: Impacts, challenges and strategies. J. Infect. Public Health 2023, 16, 4–14. [Google Scholar] [CrossRef] [PubMed]
- State Funeral Held for ex-Somali President Ali Mahdi Mohamed. Africanews. 2021. Available online: https://www.africanews.com/2021/03/13/state-funeral-held-for-ex-somali-president-ali-mahdi-mohamed// (accessed on 1 June 2022).
- Ochola, E.A. Vaccine Hesitancy in Sub-Saharan Africa in the Context of COVID-19 Vaccination Exercise: A Systematic Review. Diseases 2023, 11, 32. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Behavior Frequency | Scores | ||
|---|---|---|---|
| Days/Week | Face Mask Use | Social Hugging | Social Handshaking |
| Everyday | 3 | 0 | 0 |
| Most of the days | 2 | 1 | 0 |
| Some days | 1 | 2 | 1 |
| Never | 0 | 3 | 2 |
| Times/day | Handwashing | ||
| 0 | 0 | ||
| 1–3 | 1 | ||
| 4–6 | 2 | ||
| >6 | 3 | ||
| Measurement Period | Round 4 | Round 5 | ||
|---|---|---|---|---|
| Data Collection | 30 November–20 December 2020 | 27 March–18 April 2021 | ||
| Households interviewed | 884 | 1403 | ||
| Household size (range, SD) | 8.4 | (1–22, 3.0) | 8.4 | (1–21, 3.1) |
| Respondent sex, % female (95% CI) | 62.9 | (59.7, 66.0) | 66.5 | (64.0, 68.9) |
| Respondent age, years (range, SD) | 43.1 | (13–95, 16.1) | 43.3 | (16–95, 15.9) |
| Livelihood type (%) | ||||
| Agricultural | 16.5 | (14.2, 19.1) | 23.1 | (21.0, 25.4) |
| Pastoral | 31.8 | (28.8, 34.9) | 26.5 | (24.3, 28.9) |
| Agropastoral | 5.4 | (4.1, 7.1) | 5.7 | (4.6, 7.0) |
| Riverine | 0.0 | - | 0.9 | (0.5, 1.6) |
| Urban | 46.3 | (43.0, 49.6) | 43.8 | (41.2, 46.4) |
| HH members with symptomatic COVID-19 | 12 | 81 | ||
| Period prevalence of symptomatic COVID-19 | 0.2% | 0.7% | ||
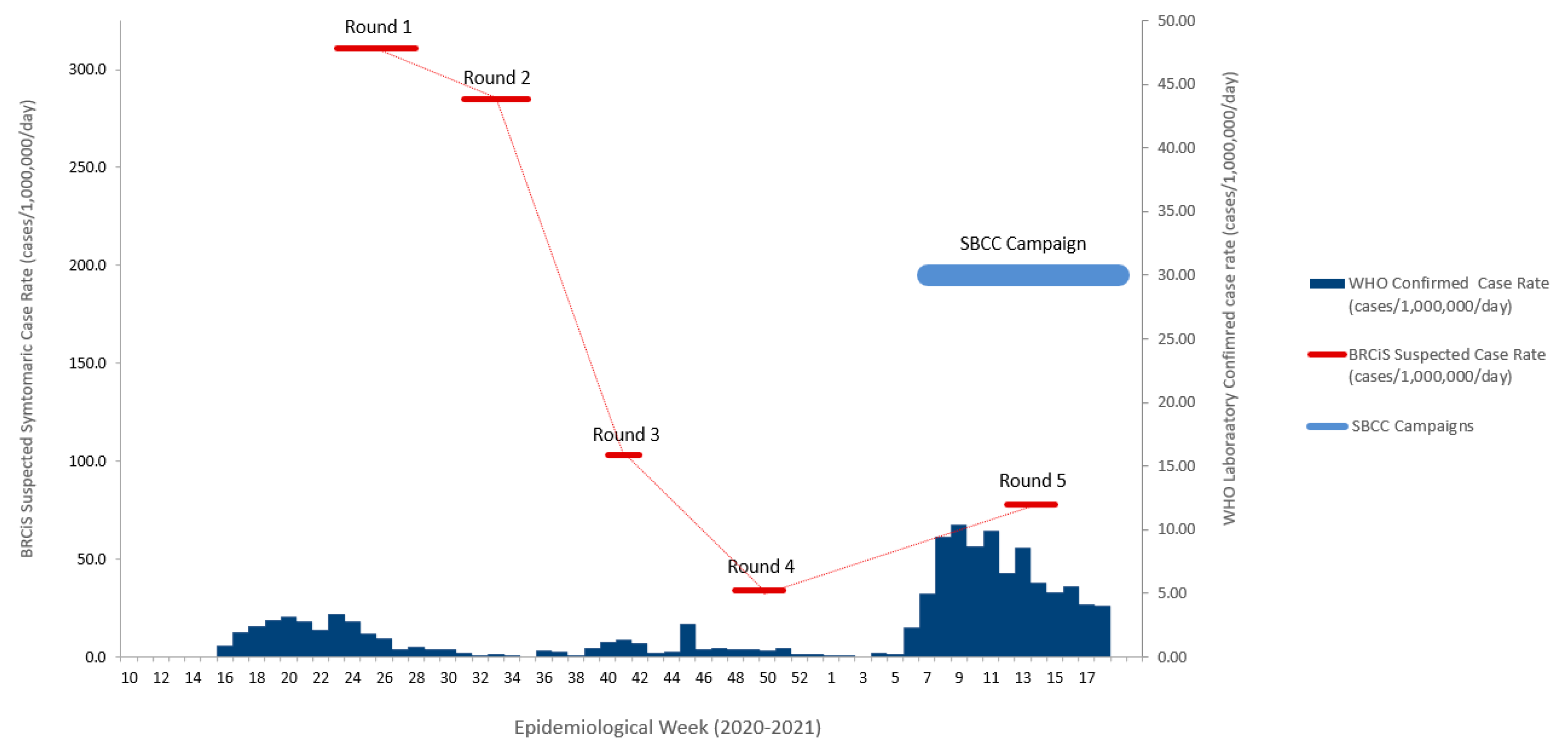
| Symptomatic COVID-19 infection rate (cases/1,000,000/day) 2 | 34 | 78 | ||
| Data Collection Round | Round 4 | Round 5 | Δ | (95% CI) | p-Value | ||
|---|---|---|---|---|---|---|---|
| N | 884 | 1403 | |||||
| How much of a threat, if any, is COVID-19 to your health and to the health of your family? %, (95%CI) | |||||||
| Not a threat | 7.9 | (4.4, 13.7) | 5.8 | (2.8, 11.4) | −2.1 | (−7.3, 3.0) | 0.462 |
| A minor threat | 45.9 | (33.0, 59.4) | 24.7 | (15.7, 36.6) | −21.3 | (−39.8, −2.7) | 0.023 |
| A major threat | 46.2 | (31.4, 61.6) | 69.6 | (56.9, 79.8) | 23.4 | (2.5, 44.3) | 0.021 |
| Do respondents who believed that COVID-19 is a disease that can affect only non-Muslims? %, (95% CI) | 6.2 | (3.8, 10.1) | 9.5 | (5.9, 14.8) | 3.3 | (−2.3, 8.8) | 0.241 |
| Proportion of respondents who had received news or information about COVID-19 in last 30 days. %, (95% CI) | 64.7 | (55.3, 73.1) | 87.9 | (75.4, 94.5) | 23.2 | (10.8, 35.6) | <0.0001 |
| Sources of information for respondents who had received news or information in last 30 days %, (95% CI) 1 | |||||||
| Religious Leaders/Mosque | 15.9 | (8.3, 28.2) | 36.8 | (24.5, 51.1) | 20.9 | (7.6, 34.2) | 0.003 |
| Phone | 67.3 | (53.3, 78.8) | 90.6 | (76.9, 96.5) | 23.3 | (7.4, 39.2) | 0.005 |
| Community health workers/NGO workers | 33.6 | (21.9, 47.6) | 38.8 | (28.3, 50.3) | 5.2 | (−9.1, 19.5) | 0.467 |
| Community Resilience Committees | 27.6 | (17.6, 40.5) | 30.7 | (21.8, 41.2) | 3.0 | (−11.8, 17.9) | 0.682 |
| Government sources | 10.0 | (5.2, 18.3) | 19.4 | (12.5, 28.9) | 9.4 | (−0.9, 19.7) | 0.072 |
| Radio | 71.3 | (56.3, 82.8) | 72.1 | (59.3, 82.1) | 0.8 | (−17.0, 18.6) | 0.931 |
| Women’s group | 20.8 | (12.0, 33.6) | 14.4 | (8.2, 23.9) | −6.4 | (−17.8, 4.9) | 0.256 |
| Social media or web sites | 8.0 | (4.0, 15.5) | 17.0 | (11.6, 24.4) | 9.0 | (0.4, 17.5) | 0.040 |
| Other | 38.5 | (25.4, 53.4) | 25.2 | (18.4, 33.5) | −13.2 | (−29.3, 2.8) | 0.104 |
| Data Collection Round | Round 4 | Round 5 | Δ | (95% CI) | p-Value | ||
|---|---|---|---|---|---|---|---|
| N | 884 | 1403 | |||||
| Number of times hands washed per day | 7.7 | (7.0, 8.4) | 8.2 | (7.6, 8.9) | 0.5 | (−0.3, 1.4) | 0.228 |
| Use of face masks when outside of their home (%): | |||||||
| Everyday | 4.1 | (2.0, 8.6) | 20.0 | (12.7, 30.1) | 15.8 | (7.1, 24.6) | 0.001 |
| Most of the days | 9.0 | (5.4, 13.8) | 26.3 | (20.6, 33.0) | 17.6 | (12.0, 23.2) | <0.0001 |
| Some days | 27.5 | (18.4, 39.0) | 18.3 | (14.8, 22.4) | −9.2 | (−19.9, 1.6) | 0.092 |
| Never | 59.6 | (14.8, 22.4) | 35.4 | (24.9, 47.4) | −24.3 | (−36.5, −12.1) | <0.0001 |
| Shaking hands with people outside of their household (%): | |||||||
| Everyday | 7.2 | (4.3, 11.9) | 3.4 | (1.5, 7.5) | −3.9 | (−8.8, 1.0) | 0.114 |
| Most of the days | 19.2 | (14.2, 25.5) | 9.8 | (6.8, 13.8) | −9.5 | (−15.8, −3.2) | 0.004 |
| Some days | 42.5 | (34.6, 50.9) | 32.6 | (25.2, 41.1) | −9.9 | (−19.4, −0.4) | 0.042 |
| Never | 31.0 | (22.1, 41.5) | 54.2 | (43.7, 64.4) | 23.2 | (9.8, 36.7) | 0.001 |
| Hugging someone from outside of their household (%): | |||||||
| Everyday | 0.2 | (0.1, 0.9) | 1.8 | (0.5, 6.3) | 1.6 | (−0.8, 3.9) | 0.185 |
| Most of the days | 5.9 | (3.6, 9.6) | 2.5 | (1.2, 5.3) | −3.4 | (−6.9, 0.2) | 0.061 |
| Some days | 24.5 | (18.5, 31.8) | 9.2 | (5.7, 14.4) | −15.4 | (−22.6, −8.1) | <0.0001 |
| Never | 69.3 | (60.0, 77.3) | 86.5 | (78.2, 92.0) | 17.2 | (6.2, 28.2) | 0.003 |
| Combined Prevention Score (PB-Score) (mean, 95% CI) | 6.9 | (6.6, 7.3) | 8.2 | (7.7, 8.7) | 1.3 | (0.7, 1.8) | <0.0001 |
| Campaign Component (N = 1403) | % | (95% CI) |
|---|---|---|
| Has heard the phrase ‘Hands face space’ (slogan 1) | 87.5 | (80.4, 92.2) |
| Has heard the phrase ‘I mask up’ (slogan 2) | 71.3 | (63.5, 78.3) |
| Has heard the phrase ‘I protect my family’ (slogan 3) | 67.8 | (59.9, 74.9) |
| Someone in household has made their own face mask | 52.9 | (39.9, 65.5) |
| SBCC Campaign Slogan | Target Behaviour/Attitude | Exposure to Slogan | Mean Behaviour Scoreor Adjusted Attitude Prevalence (%) | SD or 95% CI | Odds Ratio | (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|
| (1) ‘Hands face space’ | Social distancing: hugging 2 | − | 2.85 | 0.47 | Ref. | - | - |
| + | 2.79 | 0.57 | 0.75 | (0.18, 3.14) | 0.690 | ||
| Social distancing: hand shaking 2 | − | 2.63 | 0.67 | Ref. | - | - | |
| + | 2.34 | 0.80 | 0.41 | (0.11, 1.56) | 0.192 | ||
| Handwashing: daily frequency 2 | − | 2.40 | 0.72 | Ref. | - | - | |
| + | 2.71 | 0.53 | 0.76 | (0.35, 1.66) | 0.488 | ||
| Use of face covering 2 | − | 1.09 | 0.95 | Ref. | - | - | |
| + | 1.34 | 1.17 | 1.37 | (0.63, 2.95) | 0.426 | ||
| (2) ‘I mask up’ | Social distancing: hugging 2 | − | 2.86 | 0.47 | Ref. | - | - |
| + | 2.78 | 0.59 | 0.93 | (0.40, 2.18) | 0.872 | ||
| Social distancing: hand shaking 2 | − | 2.51 | 0.75 | Ref. | - | - | |
| + | 2.33 | 0.81 | 0.88 | (0.52, 1.49) | 0.627 | ||
| Handwashing: daily frequency 2 | − | 2.59 | 0.65 | Ref. | - | - | |
| + | 2.71 | 0.53 | 0.90 | (0.42, 1.92) | 0.781 | ||
| Use of face covering 2 | − | 0.94 | 1.00 | Ref. | - | - | |
| + | 1.46 | 1.46 | 2.31 | (1.52, 3.51) | <0.0001 | ||
| Vaccination acceptance 3 | − | 58.0% | 0.53, 0.63 | Ref. | - | - | |
| + | 76.4% | 0.69, 0.84 | 2.53 | (1.58, 4.06) | <0.0001 | ||
| (3) ‘I protect those I am responsible for’ | Vaccination acceptance 3 | − | 60.0% | 53.5, 66.4 | Ref. | - | - |
| + | 76.7% | 70.2, 83.2 | 2.36 | (1.60, 3.50) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seal, A.; Jelle, M.; Hassan, M.Y.; Farah, D.A.; Musili, F.M.; Micheni, J.; Asol, G.S.; Bhandari, M.; Nemeth, B. COVID-19 Prevention Behaviours and Vaccine Acceptability, and Their Association with a Behaviour Change Campaign in Somalia: Analysis of a Longitudinal Cohort. Vaccines 2023, 11, 972. https://doi.org/10.3390/vaccines11050972
Seal A, Jelle M, Hassan MY, Farah DA, Musili FM, Micheni J, Asol GS, Bhandari M, Nemeth B. COVID-19 Prevention Behaviours and Vaccine Acceptability, and Their Association with a Behaviour Change Campaign in Somalia: Analysis of a Longitudinal Cohort. Vaccines. 2023; 11(5):972. https://doi.org/10.3390/vaccines11050972
Chicago/Turabian StyleSeal, Andrew, Mohamed Jelle, Mohamed Yusuf Hassan, Dek Abdi Farah, Faith Mueni Musili, Janet Micheni, George Samuel Asol, Meena Bhandari, and Balint Nemeth. 2023. "COVID-19 Prevention Behaviours and Vaccine Acceptability, and Their Association with a Behaviour Change Campaign in Somalia: Analysis of a Longitudinal Cohort" Vaccines 11, no. 5: 972. https://doi.org/10.3390/vaccines11050972