
Previous Vaccination History and Psychological Factors as Significant Predictors of Willingness to Receive Mpox Vaccination and a Favorable Attitude towards Compulsory Vaccination

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Settings and Ethics Statement
2.2. Survey Instrument
2.2.1. Sociodemographic Variables
- Age as a scale ranging from 18 to 75 years, and later dichotomized based on the study sample median into two categories (≤32 years vs. >32 years);
- Sex as two categories (male vs. female);
- The highest educational level attained as two categories: (1) undergraduate including diploma, and Bachelor of Science (BSc) degrees; (2) postgraduate including Master in Science (MSc), higher specialization, fellowship and Doctor of Philosophy (PhD) degrees;
- Marital status as two categories: (1) married; (2) single, widow/widower and divorced;
- Subjective assessment of the current financial status as two categories: (1) poor or fair; (2) good or excellent;
- Current place of residence as two categories: (1) the Capital, Amman; (2) Outside the Capital;
- Occupational category (nurse vs. physician);
- Seniority level as two categories: (1) Less than 10 years of work experience; (2) 10 years or more of work experience;
- Nationality as two categories (Jordanian vs. non-Jordanian); and
- Self-reported history of chronic disease (e.g., hypertension (HTN), diabetes mellitus (DM), asthma, cardiovascular disease (CVD)), as two categories (yes vs. no).
2.2.2. Knowledge of Mpox
- Mpox is caused by bacteria (incorrect);
- There is a global outbreak of Mpox (correct);
- Mpox is endemic in Western and Central Africa (correct);
- Skin rash is a symptom of Mpox (correct);
- Mpox and smallpox symptoms are similar (correct);
- Mpox is easily transmitted in humans (incorrect);
- Mpox is spreading among male homosexuals to a large extent (correct);
- Mpox virus does not infect children or females (incorrect);
- Mpox can be treated with antibiotics (incorrect); and
- Currently, vaccination is available to prevent Mpox (correct).
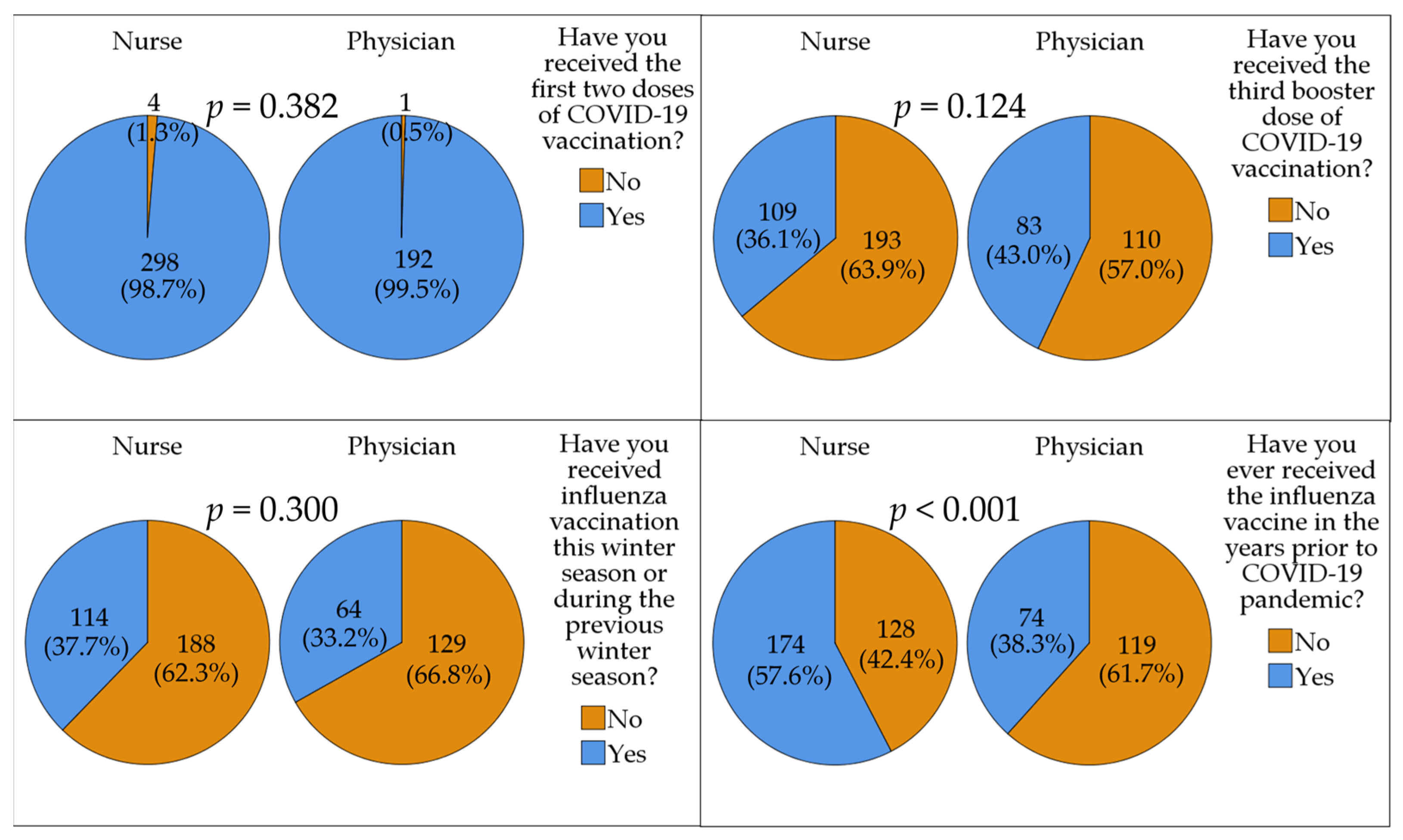
2.2.3. Vaccination Behavior
- Have you received the first two doses of COVID-19 vaccination?
- Have you received the third booster dose of COVID-19 vaccination?
- Have you received influenza vaccination this winter season or during the previous winter season? And
- Have you ever received the influenza vaccine in the years prior to the COVID-19 pandemic?
2.2.4. Intention to Receive Mpox Vaccination
- If a safe and effective Mpox vaccine is available free of charge, would you be willing to receive it?
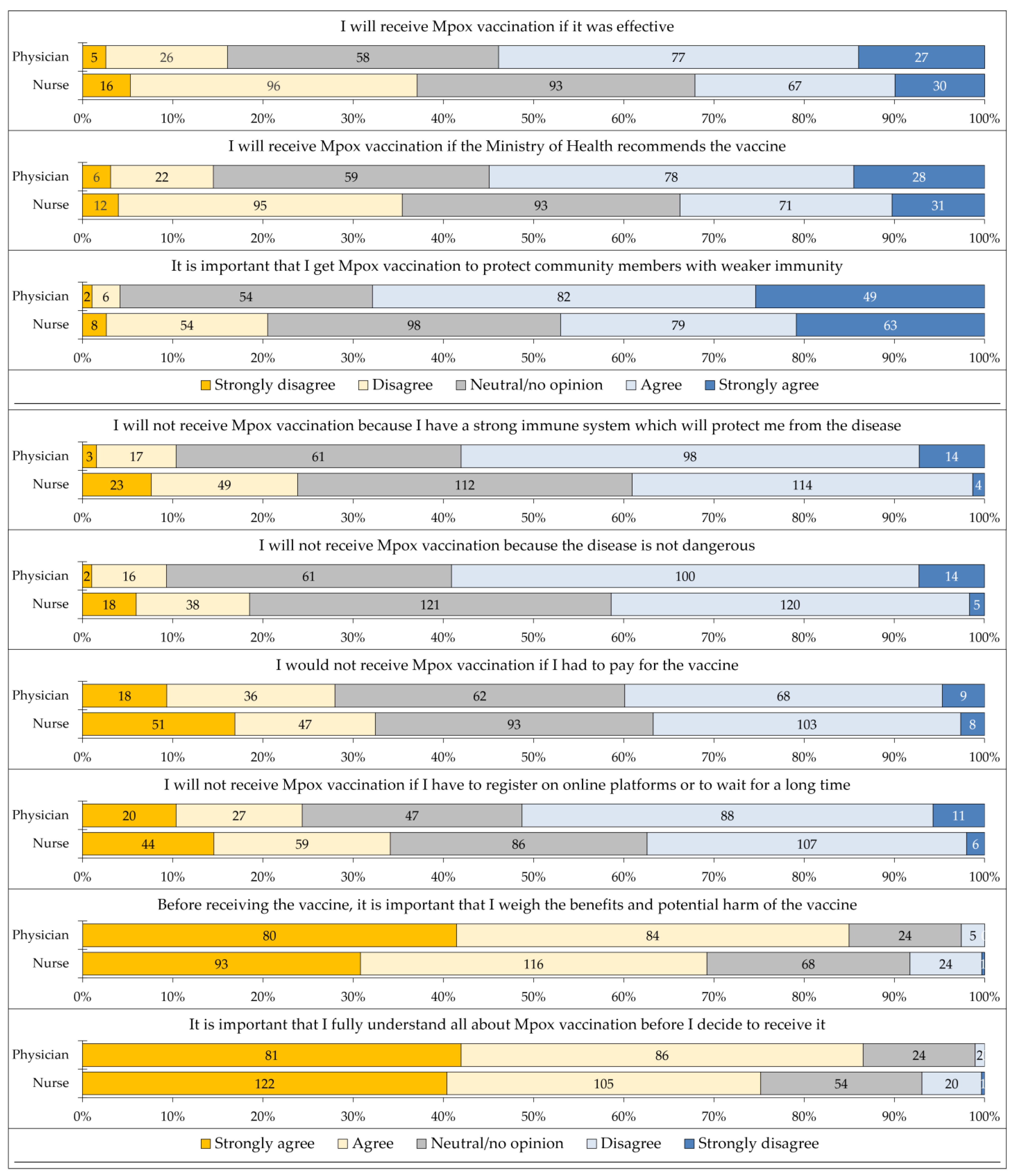
2.2.5. Psychological Determinants of Mpox Vaccination
- I will receive Mpox vaccination if it is effective;
- I will receive Mpox vaccination if the Ministry of Health recommends the vaccine;
- It is important that I get Mpox vaccination to protect community members with weaker immunity;
- I will not receive Mpox vaccination because I have a strong immune system which will protect me from the disease;
- I will not receive Mpox vaccination because the disease is not dangerous;
- I would not receive Mpox vaccination if I had to pay for the vaccine;
- I will not receive Mpox vaccination if I have to register on online platforms or wait for a long time;
- Before receiving the vaccine, it is important that I weigh the benefits and potential harm of the vaccine; and
- It is important that I fully understand all about Mpox vaccination before I decide to receive it.
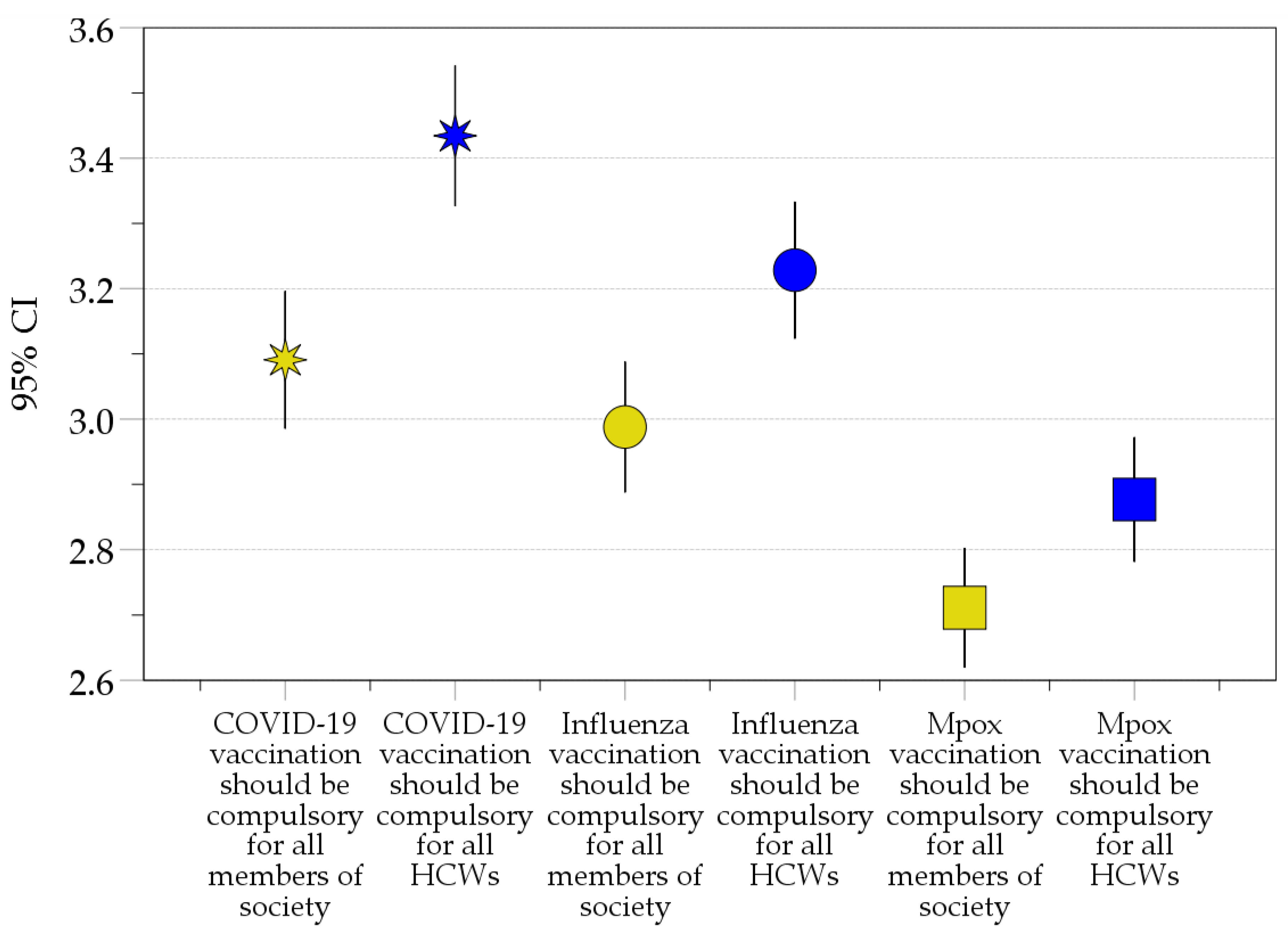
2.2.6. Attitude towards Compulsory COVID-19, Influenza, and Mpox Vaccination
- COVID-19 vaccination should be compulsory for all members of society;
- COVID-19 vaccination should be compulsory for all HCWs;
- Influenza vaccination should be compulsory for all members of society;
- Influenza vaccination should be compulsory for all HCWs;
- Mpox vaccination should be compulsory for all members of society; and
- Mpox vaccination should be compulsory for all HCWs.
2.3. Study Measures
2.3.1. Willingness to Get Mpox Vaccination
- Participants who answered “yes” were considered as the vaccine acceptance group;
- Participants who answered “maybe” were considered as the vaccine hesitancy group; and
- Participants who answered “no” were considered as the vaccine rejection group.
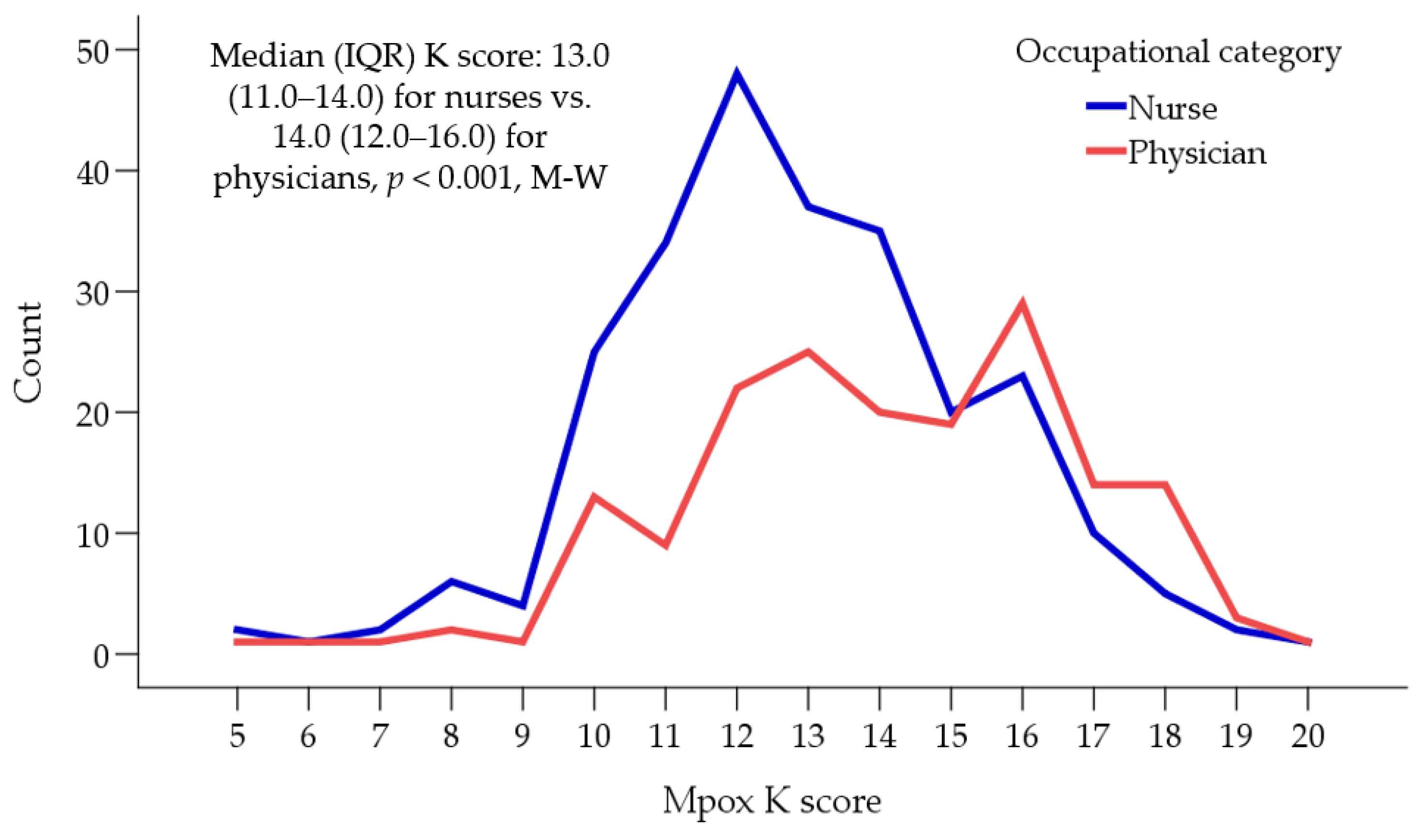
2.3.2. Mpox Knowledge Score (Mpox K Score)
- Participants with Mpox K score ≤12 were allocated to a “lower Mpox K score” group; and
- Participants with Mpox K score >12 were allocated to a “higher Mpox K score” group.
2.3.3. Previous Vaccination Behavior Score (VB Score)
- Participants with VB score ≤2 were allocated to a “lower VB score” group, indicating less active vaccine uptake behavior; and
- Participants with VB score >2 were allocated to “higher VB score” group, indicating more active vaccine uptake behavior.
2.3.4. 5C Scale for Psychological Determinants of Mpox Vaccination (5C Scale)
- Participants with 5C scale ≤ 26 were allocated to a “lower 5C scale” group; and
- Participants with 5C scale > 26 were allocated to a “higher 5C scale” group.
2.3.5. Attitude Scale towards Compulsory Vaccination
- Participants with a score ≤18 were considered as having a “lower compulsory vaccination scale” attitude, denoting a neutral or less favorable attitude towards compulsory vaccination; and
- Participants with a score >18 were considered as having a “higher compulsory vaccination scale” score, denoting a favorable attitude towards compulsory vaccination.
2.4. Statistical Analysis
3. Results
3.1. Study Sample
3.2. Unsatisfactory Level of Mpox Knowledge in the Study Sample
3.3. Previous Vaccination Behavior in the Study Sample
3.4. A Low Rate of Willingness to Get Mpox Vaccination Was Found in the Study Sample
3.5. Psychological Predictors for Willingness to Receive Mpox Vaccination in the Study Sample
3.6. Multivariate Analysis of the Factors Associated with Mpox Vaccine Acceptance
3.7. Attitude of the Participants towards Compulsory Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Larson, H.J.; Gakidou, E.; Murray, C.J.L. The Vaccine-Hesitant Moment. N. Engl. J. Med. 2022, 387, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.E.; Mahmud, A.S.; Miller, I.F.; Rajeev, M.; Rasambainarivo, F.; Rice, B.L.; Takahashi, S.; Tatem, A.J.; Wagner, C.E.; Wang, L.F.; et al. Infectious disease in an era of global change. Nat. Rev. Microbiol. 2022, 20, 193–205. [Google Scholar] [CrossRef] [PubMed]
- Rémy, V.; Zöllner, Y.; Heckmann, U. Vaccination: The cornerstone of an efficient healthcare system. J. Mark Access Health Policy 2015, 3, 27041. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Peretti-Watel, P.; Larson, H.J.; Ward, J.K.; Schulz, W.S.; Verger, P. Vaccine hesitancy: Clarifying a theoretical framework for an ambiguous notion. PLoS Curr. 2015, 7. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 27 January 2023).
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A Global Map of COVID-19 Vaccine Acceptance Rates per Country: An Updated Concise Narrative Review. J. Multidiscip. Healthc. 2022, 15, 21–45. [Google Scholar] [CrossRef]
- Rosenthal, S.; Cummings, C.L. Influence of rapid COVID-19 vaccine development on vaccine hesitancy. Vaccine 2021, 39, 7625–7632. [Google Scholar] [CrossRef]
- Lee, S.K.; Sun, J.; Jang, S.; Connelly, S. Misinformation of COVID-19 vaccines and vaccine hesitancy. Sci. Rep. 2022, 12, 13681. [Google Scholar] [CrossRef]
- Fajar, J.K.; Sallam, M.; Soegiarto, G.; Sugiri, Y.J.; Anshory, M.; Wulandari, L.; Kosasih, S.A.P.; Ilmawan, M.; Kusnaeni, K.; Fikri, M.; et al. Global Prevalence and Potential Influencing Factors of COVID-19 Vaccination Hesitancy: A Meta-Analysis. Vaccines 2022, 10, 1356. [Google Scholar] [CrossRef]
- Cataldi, J.R.; Kerns, M.E.; O’Leary, S.T. Evidence-based strategies to increase vaccination uptake: A review. Curr. Opin. Pediatr. 2020, 32, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J. Vaccine hesitancy: An overview. Hum. Vaccin. Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Cooper, L.Z.; Eskola, J.; Katz, S.L.; Ratzan, S. Addressing the vaccine confidence gap. Lancet 2011, 378, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Tuckerman, J.; Kaufman, J.; Danchin, M. Effective Approaches to Combat Vaccine Hesitancy. Pediatr. Infect. Dis. J. 2022, 41, e243–e245. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.; Chandra, R.; Mathur, M.; Samdariya, S.; Kapoor, N. Vaccine hesitancy: Understanding better to address better. Isr. J. Health Policy Res. 2016, 5, 2. [Google Scholar] [CrossRef]
- Larson, H.J. Defining and measuring vaccine hesitancy. Nat. Hum. Behav. 2022, 6, 1609–1610. [Google Scholar] [CrossRef]
- Neufeind, J.; Betsch, C.; Habersaat, K.B.; Eckardt, M.; Schmid, P.; Wichmann, O. Barriers and drivers to adult vaccination among family physicians-Insights for tailoring the immunization program in Germany. Vaccine 2020, 38, 4252–4262. [Google Scholar] [CrossRef]
- Larson, H.J.; Jarrett, C.; Schulz, W.S.; Chaudhuri, M.; Zhou, Y.; Dube, E.; Schuster, M.; MacDonald, N.E.; Wilson, R. Measuring vaccine hesitancy: The development of a survey tool. Vaccine 2015, 33, 4165–4175. [Google Scholar] [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef]
- Betsch, C.; Bach Habersaat, K.; Deshevoi, S.; Heinemeier, D.; Briko, N.; Kostenko, N.; Kocik, J.; Böhm, R.; Zettler, I.; Wiysonge, C.S.; et al. Sample study protocol for adapting and translating the 5C scale to assess the psychological antecedents of vaccination. BMJ Open 2020, 10, e034869. [Google Scholar] [CrossRef]
- Larson, H.J.; Clarke, R.M.; Jarrett, C.; Eckersberger, E.; Levine, Z.; Schulz, W.S.; Paterson, P. Measuring trust in vaccination: A systematic review. Hum. Vaccin. Immunother. 2018, 14, 1599–1609. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Böhm, R.; Korn, L. Inviting free-riders or appealing to prosocial behavior? game-theoretical reflections on communicating herd immunity in vaccine advocacy. Health Psychol. 2013, 32, 978–985. [Google Scholar] [CrossRef] [PubMed]
- Bussink-Voorend, D.; Hautvast, J.L.A.; Vandeberg, L.; Visser, O.; Hulscher, M.E.J.L. A systematic literature review to clarify the concept of vaccine hesitancy. Nat. Hum. Behav. 2022, 6, 1634–1648. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.-L. Barriers of Influenza Vaccination Intention and Behavior–A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef] [PubMed]
- Al-Tammemi, A.B.; Albakri, R.; Alabsi, S. The Outbreak of Human Monkeypox in 2022: A Changing Epidemiology or an Impending Aftereffect of Smallpox Eradication? Front. Trop. Dis. 2022, 3, 951380. [Google Scholar] [CrossRef]
- Al Awaidy, S.T.; Khamis, F.; Sallam, M.; Ghazy, R.M.; Zaraket, H. Monkeypox (Mpox) Outbreak: More queries posed as cases soar globally. Sultan. Qaboos. Univ. Med. J. 2023, 23, 1–4. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Kong, J.D.; Mahroum, N.; Tsigalou, C.; Khamisy-Farah, R.; Converti, M.; Wu, J. Epidemiological trends and clinical features of the ongoing monkeypox epidemic: A preliminary pooled data analysis and literature review. J. Med. Virol. 2023, 95, e27931. [Google Scholar] [CrossRef]
- Harapan, H.; Ophinni, Y.; Megawati, D.; Frediansyah, A.; Mamada, S.S.; Salampe, M.; Bin Emran, T.; Winardi, W.; Fathima, R.; Sirinam, S.; et al. Monkeypox: A Comprehensive Review. Viruses 2022, 14, 2155. [Google Scholar] [CrossRef]
- Lulli, L.G.; Baldassarre, A.; Mucci, N.; Arcangeli, G. Prevention, Risk Exposure, and Knowledge of Monkeypox in Occupational Settings: A Scoping Review. Trop. Med. Infect. Dis. 2022, 7, 276. [Google Scholar] [CrossRef]
- Ophinni, Y.; Frediansyah, A.; Sirinam, S.; Megawati, D.; Stoian, A.M.; Enitan, S.S.; Akele, R.Y.; Sah, R.; Pongpirul, K.; Abdeen, Z.; et al. Monkeypox: Immune response, vaccination and preventive efforts. Narra. J. 2022, 2, e90. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Vaccines and Immunization for Monkeypox: Interim Guidance, 16 November 2022. Available online: https://www.who.int/publications/i/item/WHO-MPX-Immunization (accessed on 4 February 2023).
- Lahariya, C.; Thakur, A.; Dudeja, N. Monkeypox Disease Outbreak (2022): Epidemiology, Challenges, and the Way Forward. Indian Pediatr. 2022, 59, 636–642. [Google Scholar] [CrossRef] [PubMed]
- McCollum, A.M.; Shelus, V.; Hill, A.; Traore, T.; Onoja, B.; Nakazawa, Y.; Doty, J.B.; Yinka-Ogunleye, A.; Petersen, B.W.; Hutson, C.L.; et al. Epidemiology of Human Mpox-Worldwide, 2018–2021. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 68–72. [Google Scholar] [CrossRef]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The changing epidemiology of human monkeypox-A potential threat? A systematic review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef] [PubMed]
- Center for Diseases Control and Prevention. 2022 Monkeypox Outbreak Global Map. Available online: https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html (accessed on 7 February 2023).
- Di Gennaro, F.; Veronese, N.; Marotta, C.; Shin, J.I.; Koyanagi, A.; Silenzi, A.; Antunes, M.; Saracino, A.; Bavaro, D.F.; Soysal, P.; et al. Human Monkeypox: A Comprehensive Narrative Review and Analysis of the Public Health Implications. Microorganisms 2022, 10, 1633. [Google Scholar] [CrossRef] [PubMed]
- McNeill, C.C.; Killian, T.S.; Moon, Z.; Way, K.A.; Betsy Garrison, M.E. The Relationship Between Perceptions of Emergency Preparedness, Disaster Experience, Health-Care Provider Education, and Emergency Preparedness Levels. Int. Q. Community Health Educ. 2018, 38, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Alsanafi, M.; Al-Mahzoum, K.; Sallam, M. Monkeypox Knowledge and Confidence in Diagnosis and Management with Evaluation of Emerging Virus Infection Conspiracies among Health Professionals in Kuwait. Pathogens 2022, 11, 994. [Google Scholar] [CrossRef]
- Alshahrani, N.Z.; Algethami, M.R.; Alarifi, A.M.; Alzahrani, F.; Alshehri, E.A.; Alshehri, A.M.; Sheerah, H.A.; Abdelaal, A.; Sah, R.; Rodriguez-Morales, A.J. Knowledge and Attitude Regarding Monkeypox Virus among Physicians in Saudi Arabia: A Cross-Sectional Study. Vaccines 2022, 10, 2099. [Google Scholar] [CrossRef]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Knowledge of human monkeypox viral infection among general practitioners: A cross-sectional study in Indonesia. Pathog. Glob. Health 2020, 114, 68–75. [Google Scholar] [CrossRef]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Confidence in managing human monkeypox cases in Asia: A cross-sectional survey among general practitioners in Indonesia. Acta Trop. 2020, 206, 105450. [Google Scholar] [CrossRef]
- Riccò, M.; Ferraro, P.; Camisa, V.; Satta, E.; Zaniboni, A.; Ranzieri, S.; Baldassarre, A.; Zaffina, S.; Marchesi, F. When a Neglected Tropical Disease Goes Global: Knowledge, Attitudes and Practices of Italian Physicians towards Monkeypox, Preliminary Results. Trop. Med. Infect. Dis. 2022, 7, 135. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Mahzoum, K.; Al-Tammemi, A.B.; Alkurtas, M.; Mirzaei, F.; Kareem, N.; Al-Naimat, H.; Jardaneh, L.; Al-Majali, L.; AlHadidi, A.; et al. Assessing Healthcare Workers’ Knowledge and Their Confidence in the Diagnosis and Management of Human Monkeypox: A Cross-Sectional Study in a Middle Eastern Country. Healthcare 2022, 10, 1722. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Eid, H.; Awamleh, N.; Al-Tammemi, A.B.; Barakat, M.; Athamneh, R.Y.; Hallit, S.; Harapan, H.; Mahafzah, A. Conspiratorial Attitude of the General Public in Jordan towards Emerging Virus Infections: A Cross-Sectional Study Amid the 2022 Monkeypox Outbreak. Trop. Med. Infect. Dis. 2022, 7, 411. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S.; Sarkar, T.; Khan, S.H.; Mostofa Kamal, A.H.; Hasan, S.M.M.; Kabir, A.; Yeasmin, D.; Islam, M.A.; Amin Chowdhury, K.I.; Anwar, K.S.; et al. COVID-19-Related Infodemic and Its Impact on Public Health: A Global Social Media Analysis. Am. J. Trop. Med. Hyg. 2020, 103, 1621–1629. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J. The biggest pandemic risk? Viral misinformation. Nature 2018, 562, 309. [Google Scholar] [CrossRef] [PubMed]
- National Vaccine Advisory Committee. Assessing the State of Vaccine Confidence in the United States: Recommendations from the National Vaccine Advisory Committee: Approved by the National Vaccine Advisory Committee on June 9, 2015. Public Health Rep. 2015, 130, 573–595. [Google Scholar] [CrossRef]
- Leask, J. Target the fence-sitters. Nature 2011, 473, 443–445. [Google Scholar] [CrossRef]
- Johnson, S.B.; Butcher, F. Doctors during the COVID-19 pandemic: What are their duties and what is owed to them? J. Med. Ethics 2021, 47, 12. [Google Scholar] [CrossRef]
- Bayerle, H.; Ike, J.D.; Logan, R.A.; Parker, R.M. Carrying a Community on Their Shoulders: Virgil’s Aeneas and the Duty of Healthcare Workers. J. Health Commun. 2021, 26, 312–316. [Google Scholar] [CrossRef]
- Ahmed, S.K.; Abdulqadir, S.O.; Omar, R.M.; Abdullah, A.J.; Rahman, H.A.; Hussein, S.H.; Mohammed Amin, H.I.; Chandran, D.; Sharma, A.K.; Dhama, K.; et al. Knowledge, Attitude and Worry in the Kurdistan Region of Iraq during the Mpox (Monkeypox) Outbreak in 2022: An Online Cross-Sectional Study. Vaccines 2023, 11, 610. [Google Scholar] [CrossRef]
- Abu-Farha, R.K.; Alzoubi, K.H.; Mukattash, T.L.; Alkhawaldeh, R.; Barakat, M.; Thiab, S. Public Knowledge and Perceptions about the Emerging Human Mpox in Jordan: A Cross-Sectional Study. Trop. Med. Infect. Dis. 2023, 8, 41. [Google Scholar] [CrossRef]
- Kumar, D.; Mathur, M.; Kumar, N.; Rana, R.K.; Tiwary, R.C.; Raghav, P.R.; Kumar, A.; Kapoor, N.; Mathur, M.; Tanu, T.; et al. Understanding the phases of vaccine hesitancy during the COVID-19 pandemic. Isr. J. Health Policy Res. 2022, 11, 16. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.; Sun, Y.; Li, Y.; Wang, B.; Yang, L.; Tian, T.; Wu, X.; Peng, X.; Liu, Q.; Chen, Y.; et al. Perception of and Vaccine Readiness towards Mpox among Men Who Have Sex with Men Living with HIV in China: A Cross-Sectional Study. Vaccines 2023, 11, 528. [Google Scholar] [CrossRef] [PubMed]
- Ulloque-Badaracco, J.R.; Alarcón-Braga, E.A.; Hernandez-Bustamante, E.A.; Al-Kassab-Córdova, A.; Benites-Zapata, V.A.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Acceptance towards Monkeypox Vaccination: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 1248. [Google Scholar] [CrossRef]
- Lounis, M.; Riad, A. Monkeypox (MPOX)-Related Knowledge and Vaccination Hesitancy in Non-Endemic Countries: Concise Literature Review. Vaccines 2023, 11, 229. [Google Scholar] [CrossRef] [PubMed]
- Saunders, B. How Mandatory Can We Make Vaccination? Public Health Ethics 2022, 15, 220–232. [Google Scholar] [CrossRef]
- Savulescu, J. Good reasons to vaccinate: Mandatory or payment for risk? J. Med. Ethics 2021, 47, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Galanakis, E.; Jansen, A.; Lopalco, P.L.; Giesecke, J. Ethics of mandatory vaccination for healthcare workers. Eurosurveillance 2013, 18, 20627. [Google Scholar] [CrossRef]
- Savulescu, J. Provide Vaccines, Not Require Immunity or Vaccination Passports … For Now. J. Law Med. Ethics 2021, 49, 303–306. [Google Scholar] [CrossRef]
- Giubilini, A.; Savulescu, J.; Pugh, J.; Wilkinson, D. Vaccine mandates for healthcare workers beyond COVID-19. J. Med. Ethics 2023, 49, 211. [Google Scholar] [CrossRef]
- World Health Organization; Regional Office for the Eastern Mediterranean. Health Workforce Snapshot Jordan. Available online: https://apps.who.int/iris/handle/10665/332429 (accessed on 30 December 2022).
- Epitools—Epidemiological Calculators. Sample Size to Estimate a Proportion or Apparent Prevalence with Specified Precision. Available online: https://epitools.ausvet.com.au/oneproportion (accessed on 30 December 2022).
- Sallam, M.; Al-Mahzoum, K.; Dardas, L.A.; Al-Tammemi, A.B.; Al-Majali, L.; Al-Naimat, H.; Jardaneh, L.; AlHadidi, F.; Al-Salahat, K.; Al-Ajlouni, E.; et al. Knowledge of Human Monkeypox and Its Relation to Conspiracy Beliefs among Students in Jordanian Health Schools: Filling the Knowledge Gap on Emerging Zoonotic Viruses. Medicina 2022, 58, 924. [Google Scholar] [CrossRef]
- Gualano, M.R.; Corradi, A.; Voglino, G.; Catozzi, D.; Olivero, E.; Corezzi, M.; Bert, F.; Siliquini, R. Healthcare Workers’ (HCWs) attitudes towards mandatory influenza vaccination: A systematic review and meta-analysis. Vaccine 2021, 39, 901–914. [Google Scholar] [CrossRef] [PubMed]
- Abd ElHafeez, S.; Elbarazi, I.; Shaaban, R.; ElMakhzangy, R.; Ossama Aly, M.; Alnagar, A.; Yacoub, M.; El Saeh, H.M.; Eltaweel, N.; Alqutub, S.T.; et al. Arabic validation and cross-cultural adaptation of the 5C scale for assessment of COVID-19 vaccines psychological antecedents. PLoS ONE 2021, 16, e0254595. [Google Scholar] [CrossRef] [PubMed]
- Al-Sanafi, M.; Sallam, M. Psychological Determinants of COVID-19 Vaccine Acceptance among Healthcare Workers in Kuwait: A Cross-Sectional Study Using the 5C and Vaccine Conspiracy Beliefs Scales. Vaccines 2021, 9, 701. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Ghazy, R.M.; Al-Salahat, K.; Al-Mahzoum, K.; AlHadidi, N.M.; Eid, H.; Kareem, N.; Al-Ajlouni, E.; Batarseh, R.; Ababneh, N.A.; et al. The Role of Psychological Factors and Vaccine Conspiracy Beliefs in Influenza Vaccine Hesitancy and Uptake among Jordanian Healthcare Workers during the COVID-19 Pandemic. Vaccines 2022, 10, 1355. [Google Scholar] [CrossRef] [PubMed]
- Globevnik Velikonja, V.; Verdenik, I.; Erjavec, K.; Kregar Velikonja, N. Influence of Psychological Factors on Vaccination Acceptance among Health Care Workers in Slovenia in Three Different Phases of the COVID-19 Pandemic. Vaccines 2022, 10, 1983. [Google Scholar] [CrossRef]
- Dasch, S.; Wachinger, J.; Bärnighausen, T.; Chen, S.; McMahon, S.A. Deliberation, context, emotion and trust–Understanding the dynamics of adults’ COVID-19 vaccination decisions in Germany. BMC Public Health 2023, 23, 136. [Google Scholar] [CrossRef]
- Cerda, A.A.; García, L.Y. Hesitation and Refusal Factors in Individuals’ Decision-Making Processes Regarding a Coronavirus Disease 2019 Vaccination. Front. Public Health 2021, 9, 626852. [Google Scholar] [CrossRef]
- Joshi, A.; Kaur, M.; Kaur, R.; Grover, A.; Nash, D.; El-Mohandes, A. Predictors of COVID-19 Vaccine Acceptance, Intention, and Hesitancy: A Scoping Review. Front. Public Health 2021, 9, 698111. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef]
- Goldman, R.D.; Yan, T.D.; Seiler, M.; Parra Cotanda, C.; Brown, J.C.; Klein, E.J.; Hoeffe, J.; Gelernter, R.; Hall, J.E.; Davis, A.L.; et al. Caregiver willingness to vaccinate their children against COVID-19: Cross sectional survey. Vaccine 2020, 38, 7668–7673. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Majid, U.; Ahmad, M.; Zain, S.; Akande, A.; Ikhlaq, F. COVID-19 vaccine hesitancy and acceptance: A comprehensive scoping review of global literature. Health Promot. Int. 2022, 37, daac078. [Google Scholar] [CrossRef] [PubMed]
- Ştefănuţ, A.M.; Vintilă, M.; Tomiţă, M.; Treglia, E.; Lungu, M.A.; Tomassoni, R. The Influence of Health Beliefs, of Resources, of Vaccination History, and of Health Anxiety on Intention to Accept COVID-19 Vaccination. Front. Psychol. 2021, 12, 729803. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Dauby, N.; Launay, O.; Botelho-Nevers, E. Intentions to get vaccinated against Monkeypox in Healthcare workers in France and Belgium correlates with attitudes toward COVID-19 vaccination. medRxiv 2022. preprint. [Google Scholar] [CrossRef]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Physicians’ willingness to be vaccinated with a smallpox vaccine to prevent monkeypox viral infection: A cross-sectional study in Indonesia. Clin. Epidemiol. Glob. Health 2020, 8, 1259–1263. [Google Scholar] [CrossRef] [PubMed]
- Salim, N.A.; Septadina, I.S.; Permata, M.; Hudari, H. Knowledge, attitude, and perception of anticipating 2022 global human monkeypox infection among internal medicine residents at palembang indonesia: An online survey. J. Kedokt. Dan Kesehat. Publ. Ilm. Fak. Kedokt. Univ. Sriwij. 2022, 9, 253–262. [Google Scholar] [CrossRef]
- Gonsalves, G.S.; Mayer, K.; Beyrer, C. Déjà vu All Over Again? Emergent Monkeypox, Delayed Responses, and Stigmatized Populations. J. Urban Health 2022, 99, 603–606. [Google Scholar] [CrossRef]
- Winters, M.; Malik, A.A.; Omer, S.B. Attitudes towards Monkeypox vaccination and predictors of vaccination intentions among the US general public. PLoS ONE 2022, 17, e0278622. [Google Scholar] [CrossRef]
- Kumar, N.; Ahmed, F.; Raza, M.S.; Rajpoot, P.L.; Rehman, W.; Khatri, S.A.; Mohammed, M.; Muhammad, S.; Ahmad, R. Monkeypox Cross-Sectional Survey of Knowledge, Attitudes, Practices, and Willingness to Vaccinate among University Students in Pakistan. Vaccines 2023, 11, 97. [Google Scholar] [CrossRef]
- Zucman, D.; Fourn, E.; Touche, P.; Majerholc, C.; Vallée, A. Monkeypox Vaccine Hesitancy in French Men Having Sex with Men with PrEP or Living with HIV in France. Vaccines 2022, 10, 1629. [Google Scholar] [CrossRef]
- Peng, X.; Wang, B.; Li, Y.; Chen, Y.; Wu, X.; Fu, L.; Sun, Y.; Liu, Q.; Lin, Y.-F.; Liang, B.; et al. Perceptions and worries about monkeypox, and attitudes towards monkeypox vaccination among medical workers in China: A cross-sectional survey. J. Infect. Public Health 2023, 16, 346–353. [Google Scholar] [CrossRef]
- Hong, J.; Pan, B.; Jiang, H.-J.; Zhang, Q.-M.; Xu, X.-W.; Jiang, H.; Ye, J.-E.; Cui, Y.; Yan, X.-J.; Zhai, X.-F.; et al. The willingness of Chinese healthcare workers to receive monkeypox vaccine and its independent predictors: A cross-sectional survey. J. Med. Virol. 2023, 95, e28294. [Google Scholar] [CrossRef] [PubMed]
- Lounis, M.; Bencherit, D.; Abdelhadi, S. Knowledge and awareness of Algerian healthcare workers about human monkeypox and their attitude toward its vaccination: An online cross-sectional survey. Vacunas 2023, 24, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Drobov, A.; Rozmarinová, J.; Drapáčová, P.; Klugarová, J.; Dušek, L.; Pokorná, A.; Klugar, M. Monkeypox Knowledge and Vaccine Hesitancy of Czech Healthcare Workers: A Health Belief Model (HBM)-Based Study. Vaccines 2022, 10, 2022. [Google Scholar] [CrossRef] [PubMed]
- Malaeb, D.; Sallam, M.; Salim, N.A.; Dabbous, M.; Younes, S.; Nasrallah, Y.; Iskandar, K.; Matta, M.; Obeid, S.; Hallit, S.; et al. Knowledge, Attitude and Conspiracy Beliefs of Healthcare Workers in Lebanon towards Monkeypox. Trop. Med. Infect. Dis. 2023, 8, 81. [Google Scholar] [CrossRef] [PubMed]
- BBC Arabic. Monkeypox: Conspiracy Theories Spread about Its Dispersal Amid Fears of a New Lockdown. Available online: https://www.bbc.com/arabic/trending-61553890 (accessed on 25 March 2023).
- Youssef, D.; Abboud, E.; Kawtharani, M.; Zheim, Z.; Abou Arrage, N.; Youssef, J. When a neglected tropical zoonotic disease emerges in non-endemic countries: Need to proactively fill the unveiled knowledge gaps towards human monkeypox among the Lebanese population. J. Pharm. Policy Pract. 2023, 16, 39. [Google Scholar] [CrossRef]
- Bardus, M.; Assaf, S.A.; Sakr, C.J. Using Social Marketing to Promote COVID-19 Vaccination Uptake: A Case Study from the “AUBe Vaccinated” Campaign. Vaccines 2023, 11, 459. [Google Scholar] [CrossRef]
- Moran, M.B.; Frank, L.B.; Chatterjee, J.S.; Murphy, S.T.; Baezconde-Garbanati, L. Information scanning and vaccine safety concerns among African American, Mexican American, and non-Hispanic White women. Patient Educ. Couns. 2016, 99, 147–153. [Google Scholar] [CrossRef]
- Shin, M.B.; Sloan, K.E.; Martinez, B.; Soto, C.; Baezconde-Garbanati, L.; Unger, J.B.; Kast, W.M.; Cockburn, M.; Tsui, J. Examining multilevel influences on parental HPV vaccine hesitancy among multiethnic communities in Los Angeles: A qualitative analysis. BMC Public Health 2023, 23, 545. [Google Scholar] [CrossRef]
- Rachiotis, G.; Mouchtouri, V.A.; Kremastinou, J.; Gourgoulianis, K.; Hadjichristodoulou, C. Low acceptance of vaccination against the 2009 pandemic influenza A(H1N1) among healthcare workers in Greece. Euro. Surveill. 2010, 15, 19486. Available online: https://www.eurosurveillance.org/content/10.2807/ese.15.06.19486-en (accessed on 4 February 2023). [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Navin, M.C.; Oberleitner, L.M.; Lucia, V.C.; Ozdych, M.; Afonso, N.; Kennedy, R.H.; Keil, H.; Wu, L.; Mathew, T.A. COVID-19 Vaccine Hesitancy Among Healthcare Personnel Who Generally Accept Vaccines. J. Community Health 2022, 47, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Alhasan, K.; Sallam, M.; Aljamaan, F.; Ali, T.; Al-jedai, A.; Nazmi, A.; Ajlan, A.; Aleid, H.; Karar, E.; Al-Awwami, M.; et al. Mpox Perceptions and Vaccine Advocacy among the Healthcare Workers of Solid Organ Transplant Centers: A Multicenter, Cross-Sectional Survey in Saudi Arabia. Healthcare 2023, 11, 603. [Google Scholar] [CrossRef] [PubMed]
- Beer, E.M.; Rao, V.B. A systematic review of the epidemiology of human monkeypox outbreaks and implications for outbreak strategy. PLoS Negl. Trop. Dis. 2019, 13, e0007791. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Dounias, G.; Rapisarda, V.; Ledda, C. Vaccination policies for healthcare personnel: Current challenges and future perspectives. Vaccine X 2022, 11, 100172. [Google Scholar] [CrossRef]
- Drees, M.; Wroten, K.; Smedley, M.; Mase, T.; Schwartz, J.S. Carrots and sticks: Achieving high healthcare personnel influenza vaccination rates without a mandate. Infect. Control Hosp. Epidemiol. 2015, 36, 717–724. [Google Scholar] [CrossRef]
- Peterson, C.J.; Lee, B.; Nugent, K. COVID-19 Vaccination Hesitancy among Healthcare Workers-A Review. Vaccines 2022, 10, 948. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Clinical Management and Infection Prevention and Control for Monkeypox: Interim Rapid Response Guidance. Available online: https://www.who.int/publications/i/item/WHO-MPX-Clinical-and-IPC-2022.1 (accessed on 25 March 2023).
- Ghazy, R.M.; Okeh, D.U.; Sallam, M.; Hussein, M.; Ismail, H.M.; Yazbek, S.; Mahboob, A.; Abd ElHafeez, S. Psychological Antecedents of Healthcare Workers towards Monkeypox Vaccination in Nigeria. Vaccines 2022, 10, 2151. [Google Scholar] [CrossRef]
- Abdelmoneim, S.A.; Sallam, M.; Hafez, D.M.; Elrewany, E.; Mousli, H.M.; Hammad, E.M.; Elkhadry, S.W.; Adam, M.F.; Ghobashy, A.A.; Naguib, M.; et al. COVID-19 Vaccine Booster Dose Acceptance: Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2022, 7, 298. [Google Scholar] [CrossRef]
- Roy, D.N.; Biswas, M.; Islam, E.; Azam, M.S. Potential factors influencing COVID-19 vaccine acceptance and hesitancy: A systematic review. PLoS ONE 2022, 17, e0265496. [Google Scholar] [CrossRef]
- Miraglia Del Giudice, G.; Della Polla, G.; Folcarelli, L.; Napoli, A.; Angelillo, I.F. Knowledge and attitudes of health care workers about monkeypox virus infection in Southern Italy. Front. Public Health 2023, 11, 1091267. [Google Scholar] [CrossRef]
- Gonzales-Zamora, J.A.; Soriano-Moreno, D.R.; Soriano-Moreno, A.N.; Ponce-Rosas, L.; Sangster-Carrasco, L.; De-Los-Rios-Pinto, A.; Benito-Vargas, R.M.; Murrieta-Ruiz, V.; Morocho-Alburqueque, N.; Caira-Chuquineyra, B.; et al. Level of Knowledge Regarding Mpox among Peruvian Physicians during the 2022 Outbreak: A Cross-Sectional Study. Vaccines 2023, 11, 167. [Google Scholar] [CrossRef] [PubMed]
- Sahin, T.K.; Erul, E.; Aksun, M.S.; Sonmezer, M.C.; Unal, S.; Akova, M. Knowledge and Attitudes of Turkish Physicians towards Human Monkeypox Disease and Related Vaccination: A Cross-Sectional Study. Vaccines 2022, 11, 19. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Böhm, R.; Chapman, G.B. Using behavioral insights to increase vaccination policy effectiveness. Policy Insights Behav. Brain Sci. 2015, 2, 61–73. [Google Scholar] [CrossRef]
- Betsch, C.; Korn, L.; Holtmann, C. Don’t try to convert the antivaccinators, instead target the fence-sitters. Proc. Natl. Acad. Sci. USA 2015, 112, E6725–E6726. [Google Scholar] [CrossRef]
- Slotte, P.; Karlsson, L.C.; Soveri, A. Attitudes towards mandatory vaccination and sanctions for vaccination refusal. Vaccine 2022, 40, 7378–7388. [Google Scholar] [CrossRef] [PubMed]
- Salmon, D.A.; Teret, S.P.; MacIntyre, C.R.; Salisbury, D.; Burgess, M.A.; Halsey, N.A. Compulsory vaccination and conscientious or philosophical exemptions: Past, present, and future. Lancet 2006, 367, 436–442. [Google Scholar] [CrossRef]
- Ritschl, V.; Eibensteiner, F.; Mosor, E.; Omara, M.; Sperl, L.; Nawaz, F.A.; Siva Sai, C.; Cenanovic, M.; Devkota, H.P.; Hribersek, M.; et al. Mandatory Vaccination Against COVID-19: Twitter Poll Analysis on Public Health Opinion. JMIR Form. Res. 2022, 6, e35754. [Google Scholar] [CrossRef]
- Sallam, M.; Salim, N.A.; Al-Tammemi, A.B.; Barakat, M.; Fayyad, D.; Hallit, S.; Harapan, H.; Hallit, R.; Mahafzah, A. ChatGPT Output Regarding Compulsory Vaccination and COVID-19 Vaccine Conspiracy: A Descriptive Study at the Outset of a Paradigm Shift in Online Search for Information. Cureus 2023, 15, e35029. [Google Scholar] [CrossRef]
- Greyson, D.; Vriesema-Magnuson, C.; Bettinger, J.A. Impact of school vaccination mandates on pediatric vaccination coverage: A systematic review. CMAJ Open 2019, 7, E524–E536. [Google Scholar] [CrossRef]
- Giubilini, A.; Savulescu, J. Vaccination, Risks, and Freedom: The Seat Belt Analogy. Public Health Ethics 2019, 12, 237–249. [Google Scholar] [CrossRef]
- Sprengholz, P.; Betsch, C.; Böhm, R. Reactance revisited: Consequences of mandatory and scarce vaccination in the case of COVID-19. Appl. Psychol. Health Well Being 2021, 13, 986–995. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.V.; Mohren, J.; Erren, T.C. COVID-19 and healthcare workers: A rapid systematic review into risks and preventive measures. BMJ Open 2021, 11, e042270. [Google Scholar] [CrossRef] [PubMed]
- Neufeind, J.; Schmid-Küpke, N.; Rehfuess, E.; Betsch, C.; Wichmann, O. How a generally well-accepted measles vaccine mandate may lead to inequities and decreased vaccine uptake: A preregistered survey study in Germany. BMC Public Health 2022, 22, 1846. [Google Scholar] [CrossRef] [PubMed]
- Bardosh, K.; de Figueiredo, A.; Gur-Arie, R.; Jamrozik, E.; Doidge, J.; Lemmens, T.; Keshavjee, S.; Graham, J.E.; Baral, S. The unintended consequences of COVID-19 vaccine policy: Why mandates, passports and restrictions may cause more harm than good. BMJ Glob. Health 2022, 7, e008684. [Google Scholar] [CrossRef]
- Sprengholz, P.; Korn, L.; Eitze, S.; Felgendreff, L.; Siegers, R.; Goldhahn, L.; De Bock, F.; Huebl, L.; Böhm, R.; Betsch, C. Attitude toward a mandatory COVID-19 vaccination policy and its determinants: Evidence from serial cross-sectional surveys conducted throughout the pandemic in Germany. Vaccine 2022, 40, 7370–7377. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Occupational Category | |
|---|---|---|---|
| Nurse N 2 (%) | Physician N (%) | ||
| Age | ≤32 years | 78 (25.8) | 167 (86.5) |
| >32 years | 224 (74.2) | 26 (13.5) | |
| Sex | Male | 107 (35.4) | 97 (50.3) |
| Female | 195 (64.6) | 96 (49.7) | |
| Highest educational level | Undergraduate | 283 (93.7) | 149 (77.2) |
| Postgraduate | 19 (6.3) | 44 (22.8) | |
| Marital status | Single, divorced, widow/widower | 62 (20.5) | 137 (71.0) |
| Married | 240 (79.5) | 56 (29.0) | |
| Self-reported financial status | Poor or fair | 163 (54.0) | 65 (33.7) |
| Good or excellent | 139 (46.0) | 128 (66.3) | |
| Residence | Amman | 143 (47.4) | 141 (73.1) |
| Outside the Capital | 159 (52.6) | 52 (26.9) | |
| Seniority level | 1–9 years | 109 (36.1) | 176 (91.2) |
| 10 years or more | 193 (63.9) | 17 (8.8) | |
| Nationality | Jordanian | 299 (99.0) | 179 (92.7) |
| Non-Jordanian | 3 (1.0) | 14 (7.3) | |
| Self-reported history of chronic disease (e.g., HTN, DM, asthma, CVD) 1 | Yes | 41 (13.6) | 10 (5.2) |
| No | 261 (86.4) | 183 (94.8) | |
| Mpox 1 Knowledge Item | Response | Occupational Category | p Value 3 | |
|---|---|---|---|---|
| Nurse N 2 (%) | Physician N (%) | |||
| Have you heard of Mpox prior to this study? | Yes | 255 (84.4) | 175 (90.7) | 0.045 |
| No | 47 (15.6) | 18 (9.3) | ||
| Mpox is caused by bacteria | Correct | 103 (40.4) | 125 (71.4) | <0.001 |
| I do not know | 75 (29.4) | 32 (18.3) | ||
| Incorrect | 77 (30.2) | 18 (10.3) | ||
| There is a global outbreak of Mpox | Correct | 118 (46.3) | 58 (33.1) | 0.022 |
| I do not know | 43 (16.9) | 40 (22.9) | ||
| Incorrect | 94 (36.9) | 77 (44.0) | ||
| Mpox is endemic in Western and Central Africa | Correct | 139 (54.5) | 75 (42.9) | 0.034 |
| I do not know | 87 (34.1) | 81 (46.3) | ||
| Incorrect | 29 (11.4) | 19 (10.9) | ||
| Skin rash is a symptom of Mpox | Correct | 227 (89.0) | 155 (88.6) | 0.125 |
| I do not know | 18 (7.1) | 18 (10.3) | ||
| Incorrect | 10 (3.9) | 2 (1.1) | ||
| Mpox and smallpox symptoms are similar | Correct | 193 (75.7) | 127 (72.6) | 0.021 |
| I do not know | 31 (12.2) | 36 (20.6) | ||
| Incorrect | 31 (12.2) | 12 (6.9) | ||
| Mpox is easily transmitted in humans | Correct | 86 (33.7) | 61 (34.9) | 0.017 |
| I do not know | 63 (24.7) | 62 (35.4) | ||
| Incorrect | 106 (41.6) | 52 (29.7) | ||
| Mpox is spreading among male homosexuals to a large extent | Correct | 110 (43.1) | 105 (60.0) | 0.002 |
| I do not know | 121 (47.5) | 62 (35.4) | ||
| Incorrect | 24 (9.4) | 8 (4.6) | ||
| Mpox virus does not infect children or females | Correct | 145 (56.9) | 113 (64.6) | 0.054 |
| I do not know | 85 (33.3) | 55 (31.4) | ||
| Incorrect | 25 (9.8) | 7 (4.0) | ||
| Mpox can be treated with antibiotics | Correct | 81 (31.8) | 106 (60.6) | <0.001 |
| I do not know | 95 (37.3) | 62 (35.4) | ||
| Incorrect | 79 (31.0) | 7 (4.0) | ||
| Currently, vaccination is available to prevent Mpox | Correct | 65 (25.5) | 32 (18.3) | 0.165 |
| I do not know | 119 (46.7) | 95 (54.3) | ||
| Incorrect | 71 (27.8) | 48 (27.4) | ||
| Variable | Category | Mpox K Score 1 | p Value 2 | |
|---|---|---|---|---|
| ≤12 N 2 (%) | >12 N (%) | |||
| Age | ≤32 years | 86 (39.3) | 133 (60.7) | 0.753 |
| >32 years | 86 (40.8) | 125 (59.2) | ||
| Sex | Male | 55 (31.6) | 119 (68.4) | 0.003 |
| Female | 117 (45.7) | 139 (54.3) | ||
| Highest educational level | Undergraduate | 157 (42.0) | 217 (58.0) | 0.030 |
| Postgraduate | 15 (26.8) | 41 (73.2) | ||
| Marital status | Single, divorced, widow/widower | 77 (41.6) | 108 (58.4) | 0.551 |
| Married | 95 (38.8) | 150 (61.2) | ||
| Self-reported financial status | Poor or fair | 79 (40.9) | 114 (59.1) | 0.722 |
| Good or excellent | 93 (39.2) | 144 (60.8) | ||
| Residence | Amman | 94 (37.2) | 159 (62.8) | 0.150 |
| Outside the Capital | 78 (44.1) | 99 (55.9) | ||
| Occupational category | Nurse | 122 (47.8) | 133 (52.2) | <0.001 |
| Physician | 50 (28.6) | 125 (71.4) | ||
| Seniority level | 1–9 years | 97 (38.3) | 156 (61.7) | 0.401 |
| 10 years or more | 75 (42.4) | 102 (57.6) | ||
| Nationality | Jordanian | 163 (39.5) | 250 (60.5) | 0.266 |
| Non-Jordanian | 9 (52.9) | 8 (47.1) | ||
| Self-reported history of chronic disease | Yes | 18 (41.9) | 25 (58.1) | 0.793 |
| No | 154 (39.8) | 233 (60.2) | ||
| Variable | Category | Have You Received the First Two Doses of COVID-19 2 Vaccination? | Have You Received the Third Booster Dose of COVID-19 Vaccination? | Have You Received Influenza Vaccination This Winter Season or during the Previous Winter Season? | Have You Ever Received the Influenza Vaccine in the Years Prior to COVID-19 Pandemic? | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Yes | p Value 3 | No | Yes | p Value | No | Yes | p Value | No | Yes | p Value | ||
| Age | ≤32 years | 4 (1.6) | 241 (98.4) | 0.170 | 155 (63.3) | 90 (36.7) | 0.353 | 162 (66.1) | 83 (33.9) | 0.339 | 148 (60.4) | 97 (39.6) | <0.001 |
| >32 years | 1 (0.4) | 249 (99.6) | 148 (59.2) | 102 (40.8) | 155 (62.0) | 95 (38.0) | 99 (39.6) | 151 (60.4) | |||||
| Sex | Male | 0 | 204 (100) | 0.060 | 115 (56.4) | 89 (43.6) | 0.064 | 132 (64.7) | 72 (35.3) | 0.796 | 98 (48.0) | 106 (52.0) | 0.488 |
| Female | 5 (1.7) | 286 (98.3) | 188 (64.6) | 103 (35.4) | 185 (63.6) | 106 (36.4) | 149 (51.2) | 142 (48.8) | |||||
| Highest educational level | Undergraduate | 4 (0.9) | 428 (99.1) | 0.624 | 265 (61.3) | 167 (38.7) | 0.876 | 278 (64.4) | 154 (35.6) | 0.705 | 218 (50.5) | 214 (49.5) | 0.511 |
| Postgraduate | 1 (1.6) | 62 (98.4) | 38 (60.3) | 25 (39.7) | 39 (61.9) | 24 (38.1) | 29 (46.0) | 34 (54.0) | |||||
| Marital status | Single, div/wid 1 | 2 (1.0) | 197 (99.0) | 0.993 | 123 (61.8) | 76 (38.2) | 0.823 | 135 (67.8) | 64 (32.2) | 0.149 | 126 (63.3) | 73 (36.7) | <0.001 |
| Married | 3 (1.0) | 293 (99.0) | 180 (60.8) | 116 (39.2) | 182 (61.5) | 114 (38.5) | 121 (40.9) | 175 (59.1) | |||||
| Self-reported financial status | Poor or fair | 3 (1.3) | 225 (98.7) | 0.530 | 142 (62.3) | 86 (37.7) | 0.652 | 153 (67.1) | 75 (32.9) | 0.189 | 117 (51.3) | 111 (48.7) | 0.560 |
| Good or excellent | 2 (0.7) | 265 (99.3) | 161 (60.3) | 106 (39.7) | 164 (61.4) | 103 (38.6) | 130 (48.7) | 137 (51.3) | |||||
| Residence | Amman | 3 (1.1) | 281 (98.9) | 0.905 | 161 (56.7) | 123 (43.3) | 0.017 | 170 (59.9) | 114 (40.1) | 0.025 | 138 (48.6) | 146 (51.4) | 0.500 |
| Outside the Capital | 2 (0.9) | 209 (99.1) | 142 (67.3) | 69 (32.7) | 147 (69.7) | 64 (30.3) | 109 (51.7) | 102 (48.3) | |||||
| Occupational category | Nurse | 4 (1.3) | 298 (98.7) | 0.382 | 193 (63.9) | 109 (36.1) | 0.124 | 188 (62.3) | 114 (37.7) | 0.300 | 128 (42.4) | 174 (57.6) | <0.001 |
| Physician | 1 (0.5) | 192 (99.5) | 110 (57.0) | 83 (43.0) | 129 (66.8) | 64 (33.2) | 119 (61.7) | 74 (38.3) | |||||
| Seniority level | 1–9 years | 4 (1.4) | 281 (98.6) | 0.308 | 180 (63.2) | 105 (36.8) | 0.301 | 198 (69.5) | 87 (30.5) | 0.003 | 173 (60.7) | 112 (39.3) | <0.001 |
| 10 years or more | 1 (0.5) | 209 (99.5) | 123 (58.6) | 87 (41.4) | 119 (56.7) | 91 (43.3) | 74 (35.2) | 136 (64.8) | |||||
| Nationality | Jordanian | 5 (1.0) | 473 (99.0) | 0.672 | 296 (61.9) | 182 (38.1) | 0.084 | 309 (64.6) | 169 (35.4) | 0.138 | 239 (50.0) | 239 (50.0) | 0.812 |
| Non-Jordanian | 0 | 17 (100) | 7 (41.2) | 10 (58.8) | 8 (47.1) | 9 (52.9) | 8 (47.1) | 9 (52.9) | |||||
| Self-reported history of chronic disease | Yes | 0 | 51 (100) | 0.446 | 26 (51.0) | 25 (49.0) | 0.113 | 28 (54.9) | 23 (45.1) | 0.151 | 19 (37.3) | 32 (62.7) | 0.057 |
| No | 5 (1.1) | 439 (98.9) | 277 (62.4) | 167 (37.6) | 289 (65.1) | 155 (34.9) | 228 (51.4) | 216 (48.6) | |||||
| Variable | Category | If a Safe and Effective Mpox Vaccine Is Available Free of Charge, Would You Be Willing to Receive It? | p Value 5 | ||
|---|---|---|---|---|---|
| Yes N 4 (%) | Maybe N (%) | No N (%) | |||
| Age | ≤32 years | 82 (33.5) | 91 (37.1) | 72 (29.4) | 0.001 |
| >32 years | 61 (24.4) | 74 (29.6) | 115 (46.0) | ||
| Sex | Male | 64 (31.4) | 65 (31.9) | 75 (36.8) | 0.588 |
| Female | 79 (27.1) | 100 (34.4) | 112 (38.5) | ||
| Highest educational level | Undergraduate | 121 (28.0) | 147 (34.0) | 164 (38.0) | 0.489 |
| Postgraduate | 22 (34.9) | 18 (28.6) | 23 (36.5) | ||
| Marital status | Single, divorced, widow/widower | 71 (35.7) | 80 (40.2) | 48 (24.1) | <0.001 |
| Married | 72 (24.3) | 85 (28.7) | 139 (47.0) | ||
| Self-reported financial status | Poor or fair | 61 (26.8) | 81 (35.5) | 86 (37.7) | 0.528 |
| Good or excellent | 82 (30.7) | 84 (31.5) | 101 (37.8) | ||
| Residence | Amman | 98 (34.5) | 95 (33.5) | 91 (32.0) | 0.001 |
| Outside the Capital | 45 (21.3) | 70 (33.2) | 96 (45.5) | ||
| Occupational category | Nurse | 70 (23.2) | 91 (30.1) | 141 (46.7) | <0.001 |
| Physician | 73 (37.8) | 74 (38.3) | 46 (23.8) | ||
| Seniority level | 1–9 years | 89 (31.2) | 111 (38.9) | 85 (29.8) | <0.001 |
| 10 years or more | 54 (25.7) | 54 (25.7) | 102 (48.6) | ||
| Nationality | Jordanian | 135 (28.2) | 159 (33.3) | 184 (38.5) | 0.141 |
| Non-Jordanian | 8 (47.1) | 6 (35.3) | 3 (17.6) | ||
| Self-reported history of chronic disease | Yes | 15 (29.4) | 13 (25.5) | 23 (45.1) | 0.394 |
| No | 128 (28.8) | 152 (34.2) | 164 (36.9) | ||
| Mpox K score 1 | ≤12 | 50 (29.1) | 52 (30.2) | 70 (40.7) | 0.142 |
| >12 | 80 (31.0) | 96 (37.2) | 82 (31.8) | ||
| VB score 2 | ≤2 | 64 (21.6) | 102 (34.5) | 130 (43.9) | <0.001 |
| >2 | 79 (39.7) | 63 (31.7) | 57 (28.6) | ||
| 5C scale 3 | ≤26 | 21 (9.5) | 58 (26.4) | 141 (64.1) | <0.001 |
| >26 | 122 (44.4) | 107 (38.9) | 46 (16.7) | ||
| Variable | Category | Confidence 1 Mean ± SD | Confidence 2 Mean ± SD | Collective Responsibility | Complacency 1 Mean ± SD | Complacency 2 Mean ± SD | Constraints 1 Mean ± SD | Constraints 2 Mean ± SD | Calculation 1 Mean ± SD | Calculation 2 Mean ± SD | 5C Mean ± SD |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | ≤32 years | 3.37 ± 1.00 | 3.41 ± 1.00 | 3.74 ± 0.90 | 3.40 ± 0.90 | 3.43 ± 0.87 | 3.06 ± 1.05 | 3.09 ± 1.09 | 1.87 ± 0.83 | 1.81 ± 0.80 | 27.18 ± 4.90 |
| >32 years | 3.01 ± 1.10 | 3.05 ± 1.07 | 3.50 ± 1.13 | 3.13 ± 0.93 | 3.23 ± 0.87 | 2.88 ± 1.14 | 2.97 ± 1.12 | 2.05 ± 0.94 | 1.87 ± 0.92 | 25.69 ± 4.76 | |
| p value 1 | <0.001 | <0.001 | 0.020 | 0.001 | 0.011 | 0.135 | 0.209 | 0.035 | 0.783 | <0.001 | |
| Sex | Male | 3.22 ± 1.09 | 3.27 ± 1.07 | 3.62 ± 1.07 | 3.22 ± 0.97 | 3.24 ± 0.90 | 2.87 ± 1.13 | 3.01 ± 1.12 | 1.96 ± 0.87 | 1.84 ± 0.85 | 26.25 ± 5.34 |
| Female | 3.17 ± 1.05 | 3.20 ± 1.04 | 3.61 ± 1.00 | 3.29 ± 0.89 | 3.40 ± 0.85 | 3.04 ± 1.07 | 3.04 ± 1.10 | 1.96 ± 0.90 | 1.84 ± 0.87 | 26.55 ± 4.54 | |
| p value | 0.578 | 0.444 | 0.712 | 0.437 | 0.039 | 0.094 | 0.731 | 0.887 | 0.870 | 0.669 | |
| Education | Undergraduate | 3.18 ± 1.08 | 3.22 ± 1.06 | 3.62 ± 1.05 | 3.27 ± 0.93 | 3.33 ± 0.88 | 2.99 ± 1.11 | 3.03 ± 1.12 | 1.98 ± 0.90 | 1.84 ± 0.87 | 26.46 ± 4.94 |
| Postgraduate | 3.24 ± 0.95 | 3.29 ± 0.99 | 3.59 ± 0.89 | 3.22 ± 0.89 | 3.37 ± 0.83 | 2.84 ± 1.03 | 3.00 ± 1.05 | 1.84 ± 0.79 | 1.86 ± 0.80 | 26.24 ± 4.43 | |
| p value | 0.702 | 0.691 | 0.562 | 0.677 | 0.796 | 0.208 | 0.660 | 0.361 | 0.673 | 0.571 | |
| Marital status | Single/div/wid 2 | 3.46 ± 1.02 | 3.47 ± 1.01 | 3.89 ± 0.90 | 3.46 ± 0.91 | 3.48 ± 0.86 | 3.06 ± 1.09 | 3.13 ± 1.13 | 1.80 ± 0.80 | 1.74 ± 0.75 | 27.49 ± 5.03 |
| Married | 3.01 ± 1.06 | 3.07 ± 1.05 | 3.43 ± 1.06 | 3.13 ± 0.91 | 3.23 ± 0.87 | 2.91 ± 1.10 | 2.96 ± 1.08 | 2.06 ± 0.93 | 1.91 ± 0.92 | 25.72 ± 4.65 | |
| p value | <0.001 | <0.001 | <0.001 | <0.001 | 0.002 | 0.113 | 0.044 | 0.002 | 0.086 | <0.001 | |
| Financial status | Poor/fair | 3.14 ± 1.05 | 3.19 ± 1.04 | 3.56 ± 1.02 | 3.17 ± 0.93 | 3.26 ± 0.87 | 2.91 ± 1.10 | 2.98 ± 1.10 | 2.00 ± 0.90 | 1.92 ± 0.88 | 26.11 ± 4.75 |
| Good/excellent | 3.24 ± 1.08 | 3.27 ± 1.07 | 3.66 ± 1.03 | 3.34 ± 0.91 | 3.39 ± 0.87 | 3.02 ± 1.09 | 3.07 ± 1.11 | 1.93 ± 0.88 | 1.78 ± 0.84 | 26.70 ± 4.98 | |
| p value | 0.292 | 0.386 | 0.258 | 0.011 | 0.022 | 0.194 | 0.209 | 0.398 | 0.076 | 0.193 | |
| Residence | Amman | 3.32 ± 1.03 | 3.37 ± 1.02 | 3.72 ± 0.95 | 3.41 ± 0.82 | 3.46 ± 0.78 | 3.10 ± 1.07 | 3.20 ± 1.06 | 1.91 ± 0.87 | 1.80 ± 0.82 | 27.29 ± 4.61 |
| Out. Amman 3 | 3.01 ± 1.08 | 3.04 ± 1.07 | 3.47 ± 1.11 | 3.06 ± 1.01 | 3.16 ± 0.96 | 2.79 ± 1.11 | 2.80 ± 1.13 | 2.02 ± 0.91 | 1.91 ± 0.92 | 25.27 ± 5.00 | |
| p value | 0.002 | 0.001 | 0.017 | <0.001 | 0.001 | 0.004 | <0.001 | 0.170 | 0.269 | <0.001 | |
| Occupation | Nurse | 3.00 ± 1.07 | 3.05 ± 1.06 | 3.45 ± 1.09 | 3.09 ± 0.94 | 3.19 ± 0.89 | 2.90 ± 1.13 | 2.91 ± 1.10 | 2.09 ± 0.94 | 1.92 ± 0.93 | 25.58 ± 4.70 |
| Physician | 3.49 ± 0.98 | 3.52 ± 0.98 | 3.88 ± 0.86 | 3.53 ± 0.82 | 3.56 ± 0.79 | 3.07 ± 1.05 | 3.22 ± 1.09 | 1.76 ± 0.77 | 1.73 ± 0.72 | 27.77 ± 4.87 | |
| p value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.153 | 0.001 | <0.001 | 0.082 | <0.001 | |
| Seniority | 1–9 years | 3.32 ± 1.01 | 3.39 ± 1.01 | 3.74 ± 0.92 | 3.39 ± 0.9 | 3.42 ± 0.84 | 2.99 ± 1.07 | 3.06 ± 1.10 | 1.86 ± 0.82 | 1.79 ± 0.80 | 26.94 ± 4.84 |
| ≥10 years | 3.02 ± 1.11 | 3.02 ± 1.08 | 3.45 ± 1.14 | 3.10 ± 0.93 | 3.20 ± 0.9 | 2.94 ± 1.14 | 3.00 ± 1.12 | 2.10 ± 0.96 | 1.92 ± 0.94 | 25.74 ± 4.85 | |
| p value | 0.002 | <0.001 | 0.004 | 0.001 | 0.011 | 0.930 | 0.606 | 0.007 | 0.224 | 0.006 | |
| Nationality | Jordanian | 3.17 ± 1.06 | 3.21 ± 1.05 | 3.60 ± 1.03 | 3.26 ± 0.91 | 3.32 ± 0.88 | 2.96 ± 1.10 | 3.03 ± 1.11 | 1.96 ± 0.89 | 1.84 ± 0.87 | 26.37 ± 4.86 |
| Non-Jordanian | 3.65 ± 1.06 | 3.82 ± 1.13 | 3.94 ± 1.03 | 3.24 ± 1.15 | 3.53 ± 0.72 | 3.06 ± 1.03 | 3.12 ± 1.05 | 1.88 ± 0.70 | 1.88 ± 0.70 | 28.12 ± 5.18 | |
| p value | 0.052 | 0.014 | 0.127 | 0.847 | 0.448 | 0.710 | 0.722 | 0.911 | 0.597 | 0.069 | |
| Chronic disease | Yes | 2.90 ± 1.08 | 3.00 ± 1.00 | 3.43 ± 1.08 | 3.10 ± 0.96 | 3.22 ± 0.88 | 2.98 ± 1.07 | 3.06 ± 1.01 | 2.27 ± 0.92 | 2.12 ± 0.95 | 26.08 ± 4.48 |
| No | 3.22 ± 1.06 | 3.26 ± 1.06 | 3.64 ± 1.02 | 3.28 ± 0.92 | 3.34 ± 0.87 | 2.97 ± 1.10 | 3.03 ± 1.12 | 1.92 ± 0.88 | 1.81 ± 0.84 | 26.47 ± 4.93 | |
| p value | 0.051 | 0.124 | 0.176 | 0.196 | 0.305 | 0.936 | 0.994 | 0.007 | 0.023 | 0.419 |
| 5C Item | Response | Willingness to Get Mpox Vaccination | p Value 1 | ||
|---|---|---|---|---|---|
| Acceptance Group | Hesitancy Group | Resistance Group | |||
| I will receive Mpox vaccination if it is effective | Agreement | 128 (89.5) | 61 (37.0) | 12 (6.4) | <0.001 |
| Neutral | 12 (8.4) | 92 (55.8) | 47 (25.1) | ||
| Disagreement | 3 (2.1) | 12 (7.3) | 128 (68.4) | ||
| I will receive Mpox vaccination if the Ministry of Health recommends the vaccine | Agreement | 120 (83.9) | 68 (41.2) | 20 (10.7) | <0.001 |
| Neutral | 18 (12.6) | 83 (50.3) | 51 (27.3) | ||
| Disagreement | 5 (3.5) | 14 (8.5) | 116 (62.0) | ||
| It is important that I get Mpox vaccination to protect community members with weaker immunity | Agreement | 121 (84.6) | 98 (59.4) | 54 (28.9) | <0.001 |
| Neutral | 19 (13.3) | 61 (37.0) | 72 (38.5) | ||
| Disagreement | 3 (2.1) | 6 (3.6) | 61 (32.6) | ||
| I will not receive Mpox vaccination because I have a strong immune system which will protect me from the disease | Disagreement | 99 (69.2) | 82 (49.7) | 49 (26.2) | <0.001 |
| Neutral | 29 (20.3) | 68 (41.2) | 76 (40.6) | ||
| Agreement | 15 (10.5) | 15 (9.1) | 62 (33.2) | ||
| I will not receive Mpox vaccination because the disease is not dangerous | Disagreement | 104 (72.7) | 80 (48.5) | 55 (29.4) | <0.001 |
| Neutral | 25 (17.5) | 76 (46.1) | 81 (43.3) | ||
| Agreement | 14 (9.8) | 9 (5.5) | 51 (27.3) | ||
| I would not receive Mpox vaccination if I had to pay for the vaccine | Disagreement | 70 (49.0) | 62 (37.6) | 56 (29.9) | <0.001 |
| Neutral | 35 (24.5) | 66 (40) | 54 (28.9) | ||
| Agreement | 38 (26.6) | 37 (22.4) | 77 (41.2) | ||
| I will not receive Mpox vaccination if I have to register on online platforms or wait for a long time | Disagreement | 83 (58.0) | 70 (42.4) | 59 (31.6) | <0.001 |
| Neutral | 24 (16.8) | 60 (36.4) | 49 (26.2) | ||
| Agreement | 36 (25.2) | 35 (21.2) | 79 (42.2) | ||
| Before receiving the vaccine, it is important that I weigh the benefits and potential harm of the vaccine | Disagreement | 5 (3.5) | 4 (2.4) | 21 (11.2) | <0.001 |
| Neutral | 18 (12.6) | 33 (20.0) | 41 (21.9) | ||
| Agreement | 120 (83.9) | 128 (77.6) | 125 (66.8) | ||
| It is important that I fully understand all about Mpox vaccination before I decide to receive it | Disagreement | 2 (1.4) | 4 (2.4) | 17 (9.1) | 0.001 |
| Neutral | 16 (11.2) | 30 (18.2) | 32 (17.1) | ||
| Agreement | 125 (87.4) | 131 (79.4) | 138 (73.8) | ||
| Mpox Vaccine Acceptance vs. Mpox Vaccine Hesitancy | OR (95% CI) 3 | p Value |
|---|---|---|
| Age: >32 years vs. ≤32 years | 0.845 (0.382–1.870) | 0.678 |
| Marital status: Married vs. single, divorced, widow/widower | 0.987 (0.555–1.755) | 0.964 |
| Residence: Outside the Capital vs. Amman | 0.731 (0.442–1.211) | 0.224 |
| Occupational category: Physician vs. nurse | 1.326 (0.708–2.484) | 0.378 |
| Seniority level: 10 years or more vs. 1–9 years | 1.406 (0.643–3.075) | 0.742 |
| VB score 1: >2 vs. ≤2 | 1.980 (1.208–3.244) | 0.007 |
| 5C scale 2: >26 vs. ≤26 | 2.972 (1.675–5.272) | <0.001 |
| Mpox Vaccine Acceptance vs. Mpox Vaccine Rejection | OR (95% CI) | p Value |
| Age: >32 years vs. ≤32 years | 1.638 (0.689–3.891) | 0.264 |
| Marital status: Married vs. single, divorced, widow/widower | 0.429 (0.221–0.834) | 0.013 |
| Residence: Outside the Capital vs. Amman | 0.610 (0.349–1.065) | 0.082 |
| Occupational category: Physician vs. nurse | 1.688 (0.827–3.442) | 0.150 |
| Seniority level: 10 years or more vs. 1–9 years | 0.514 (0.221–1.193) | 0.121 |
| VB score: >2 vs. ≤2 | 3.860 (2.180–6.835) | <0.001 |
| 5C scale: >26 vs. ≤26 | 16.129 (8.868–29.336) | <0.001 |
| Item | Response | Nurse N 4 (%) | Physician N (%) | p Value 5 |
|---|---|---|---|---|
| COVID-19 1 vaccination should be compulsory for all members of society | Strongly agree | 43 (14.2) | 35 (18.1) | 0.305 |
| Agree | 68 (22.5) | 43 (22.3) | ||
| Neutral/no opinion | 65 (21.5) | 51 (26.4) | ||
| Disagree | 106 (35.1) | 52 (26.9) | ||
| Strongly disagree | 20 (6.6) | 12 (6.2) | ||
| COVID-19 vaccination should be compulsory for all HCWs 2 | Strongly agree | 62 (20.5) | 56 (29.0) | 0.017 |
| Agree | 81 (26.8) | 62 (32.1) | ||
| Neutral/no opinion | 60 (19.9) | 36 (18.7) | ||
| Disagree | 82 (27.2) | 30 (15.5) | ||
| Strongly disagree | 17 (5.6) | 9 (4.7) | ||
| Influenza vaccination should be compulsory for all members of society | Strongly agree | 35 (11.6) | 27 (14.0) | 0.253 |
| Agree | 70 (23.2) | 29 (15.0) | ||
| Neutral/no opinion | 78 (25.8) | 57 (29.5) | ||
| Disagree | 100 (33.1) | 69 (35.8) | ||
| Strongly disagree | 19 (6.3) | 11 (5.7) | ||
| Influenza vaccination should be compulsory for all HCWs | Strongly agree | 48 (15.9) | 43 (22.3) | 0.347 |
| Agree | 74 (24.5) | 47 (24.4) | ||
| Neutral/no opinion | 71 (23.5) | 47 (24.4) | ||
| Disagree | 92 (30.5) | 48 (24.9) | ||
| Strongly disagree | 17 (5.6) | 8 (4.1) | ||
| Mpox 3 vaccination should be compulsory for all members of society | Strongly agree | 20 (6.6) | 19 (9.8) | 0.001 |
| Agree | 45 (14.9) | 12 (6.2) | ||
| Neutral/no opinion | 83 (27.5) | 78 (40.4) | ||
| Disagree | 133 (44.0) | 65 (33.7) | ||
| Strongly disagree | 21 (7.0) | 19 (9.8) | ||
| Mpox vaccination should be compulsory for all HCWs | Strongly agree | 27 (8.9) | 23 (11.9) | 0.047 |
| Agree | 52 (17.2) | 28 (14.5) | ||
| Neutral/no opinion | 84 (27.8) | 73 (37.8) | ||
| Disagree | 120 (39.7) | 55 (28.5) | ||
| Strongly disagree | 19 (6.3) | 14 (7.3) |
| Variable | Category | Attitude to Compulsory Vaccination | p Value 5 | |
|---|---|---|---|---|
| ≤18 N 4 (%) | >18 N (%) | |||
| Age | ≤32 years | 130 (53.1) | 115 (46.9) | 0.198 |
| >32 years | 147 (58.8) | 103 (41.2) | ||
| Sex | Male | 114 (55.9) | 90 (44.1) | 0.977 |
| Female | 163 (56.0) | 128 (44.0) | ||
| Highest educational level | Undergraduate | 236 (54.6) | 196 (45.4) | 0.119 |
| Postgraduate | 41 (65.1) | 22 (34.9) | ||
| Marital status | Single, divorced, widow/widower | 108 (54.3) | 91 (45.7) | 0.535 |
| Married | 169 (57.1) | 127 (42.9) | ||
| Self-reported financial status | Poor or fair | 128 (56.1) | 100 (43.9) | 0.940 |
| Good or excellent | 149 (55.8) | 118 (44.2) | ||
| Residence | Amman | 149 (52.5) | 135 (47.5) | 0.069 |
| Outside the Capital | 128 (60.7) | 83 (39.3) | ||
| Occupational category | Nurse | 176 (58.3) | 126 (41.7) | 0.194 |
| Physician | 101 (52.3) | 92 (47.7) | ||
| Seniority level | 1–9 years | 150 (52.6) | 135 (47.4) | 0.082 |
| 10 years or more | 127 (60.5) | 83 (39.5) | ||
| Nationality | Jordanian | 268 (56.1) | 210 (43.9) | 0.799 |
| Non-Jordanian | 9 (52.9) | 8 (47.1) | ||
| Self-reported history of chronic disease | Yes | 35 (68.6) | 16 (31.4) | 0.054 |
| No | 242 (54.5) | 202 (45.5) | ||
| Mpox K score 1 | ≤12 | 91 (52.9) | 81 (47.1) | 0.406 |
| >12 | 147 (57.0) | 111 (43.0) | ||
| VB score 2 | ≤2 | 184 (62.2) | 112 (37.8) | 0.001 |
| >2 | 93 (46.7) | 106 (53.3) | ||
| 5C score 3 | ≤26 | 152 (69.1) | 68 (30.9) | <0.001 |
| >26 | 125 (45.5) | 150 (54.5) | ||
| Agreement vs. Neutral/Disagreement towards Compulsory Vaccination | OR (95% CI) 3 | p Value |
|---|---|---|
| Residence: Outside the Capital vs. Amman | 0.821 (0.563–1.198) | 0.307 |
| Seniority level: 10 years or more vs. 1–9 years | 0.681 (0.460–1.009) | 0.056 |
| VB score 1: >2 vs. ≤2 | 1.930 (1.306–2.853) | 0.001 |
| 5C scale 2: >26 vs. ≤26 | 2.430 (1.662–3.554) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahameed, H.; Al-Mahzoum, K.; AlRaie, L.A.; Aburumman, R.; Al-Naimat, H.; Alhiary, S.; Barakat, M.; Al-Tammemi, A.B.; Salim, N.A.; Sallam, M. Previous Vaccination History and Psychological Factors as Significant Predictors of Willingness to Receive Mpox Vaccination and a Favorable Attitude towards Compulsory Vaccination. Vaccines 2023, 11, 897. https://doi.org/10.3390/vaccines11050897
Mahameed H, Al-Mahzoum K, AlRaie LA, Aburumman R, Al-Naimat H, Alhiary S, Barakat M, Al-Tammemi AB, Salim NA, Sallam M. Previous Vaccination History and Psychological Factors as Significant Predictors of Willingness to Receive Mpox Vaccination and a Favorable Attitude towards Compulsory Vaccination. Vaccines. 2023; 11(5):897. https://doi.org/10.3390/vaccines11050897
Chicago/Turabian StyleMahameed, Haneen, Kholoud Al-Mahzoum, Lana A. AlRaie, Razan Aburumman, Hala Al-Naimat, Sakher Alhiary, Muna Barakat, Ala’a B. Al-Tammemi, Nesreen A. Salim, and Malik Sallam. 2023. "Previous Vaccination History and Psychological Factors as Significant Predictors of Willingness to Receive Mpox Vaccination and a Favorable Attitude towards Compulsory Vaccination" Vaccines 11, no. 5: 897. https://doi.org/10.3390/vaccines11050897