
How Well the Constructs of Health Belief Model Predict Vaccination Intention: A Systematic Review on COVID-19 Primary Series and Booster Vaccines

Abstract
:1. Introduction
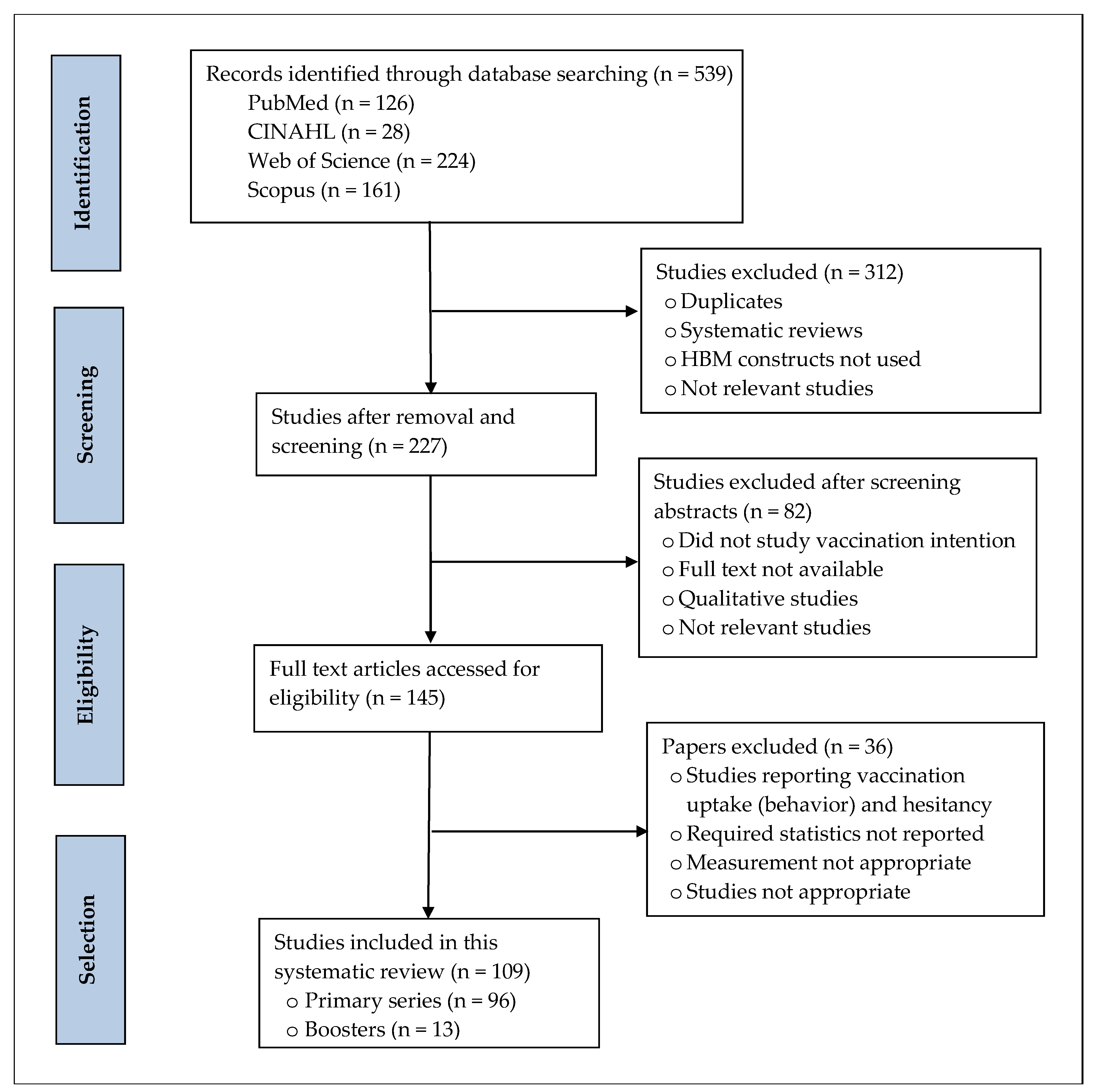
2. Methodology
2.1. Eligibility
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
2.2. Search Strategy
2.3. Data Extraction and Analysis
2.4. Risk of Bias
3. Results
3.1. Characteristics of the Included Studies
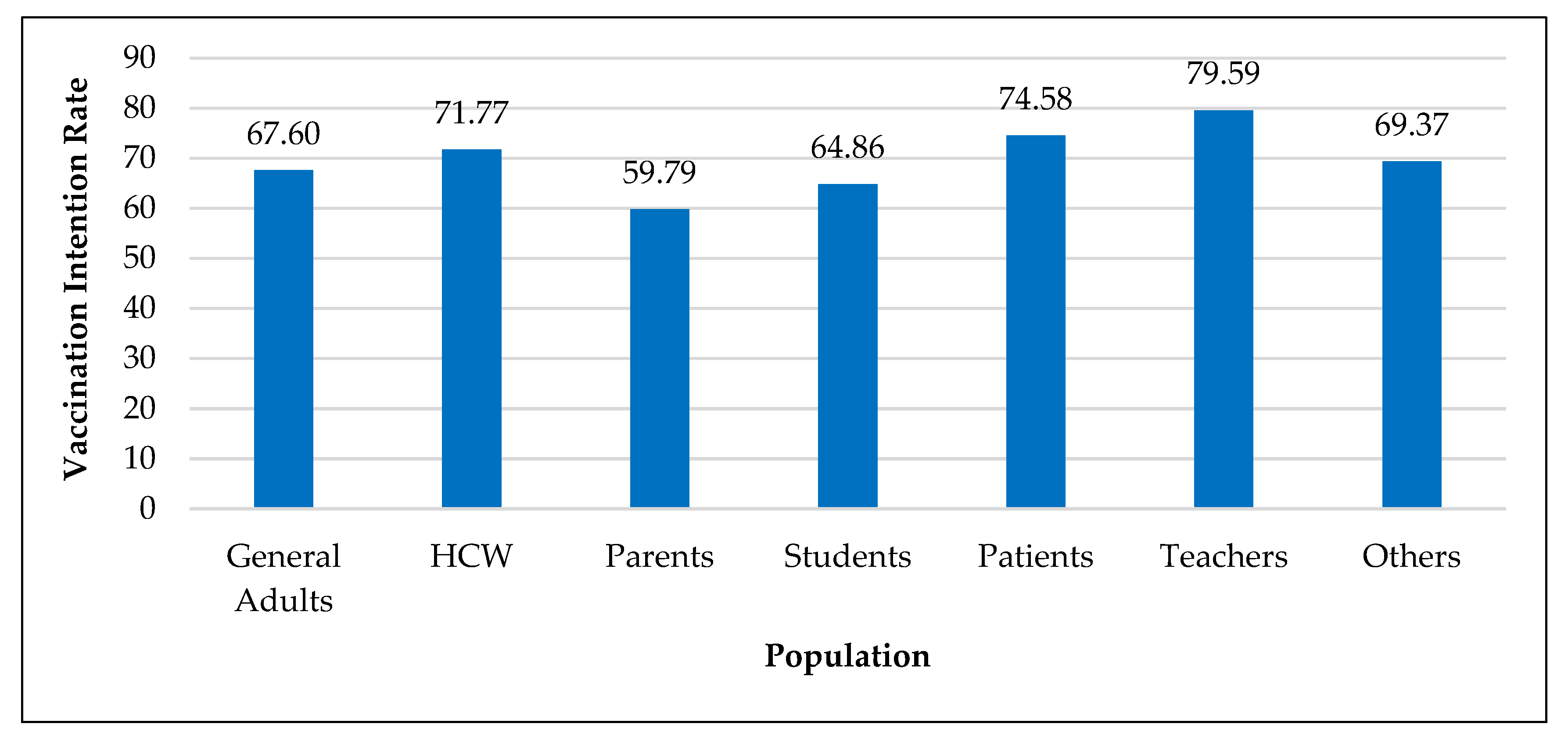
3.2. Vaccination Intention Rate by Country, Population, and Year
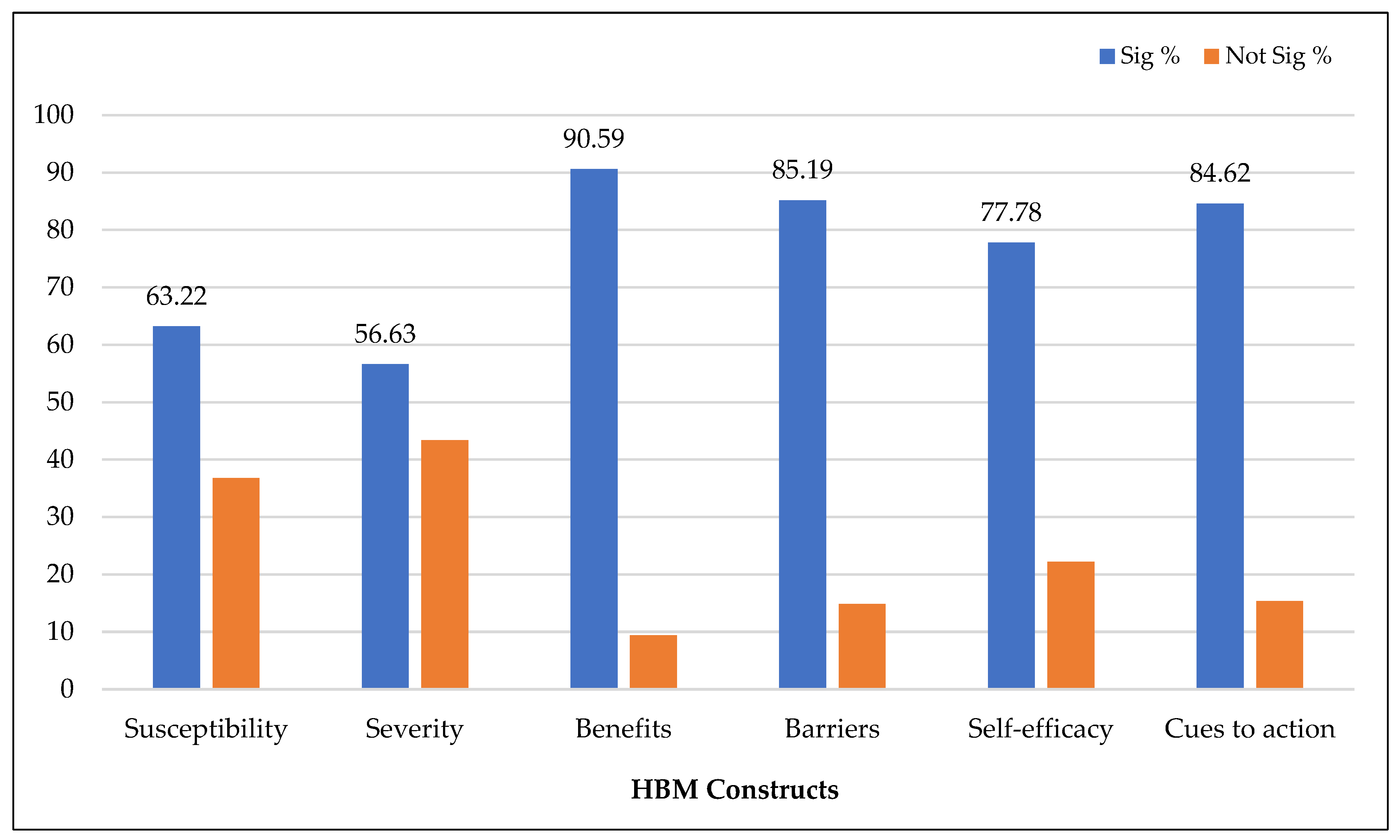
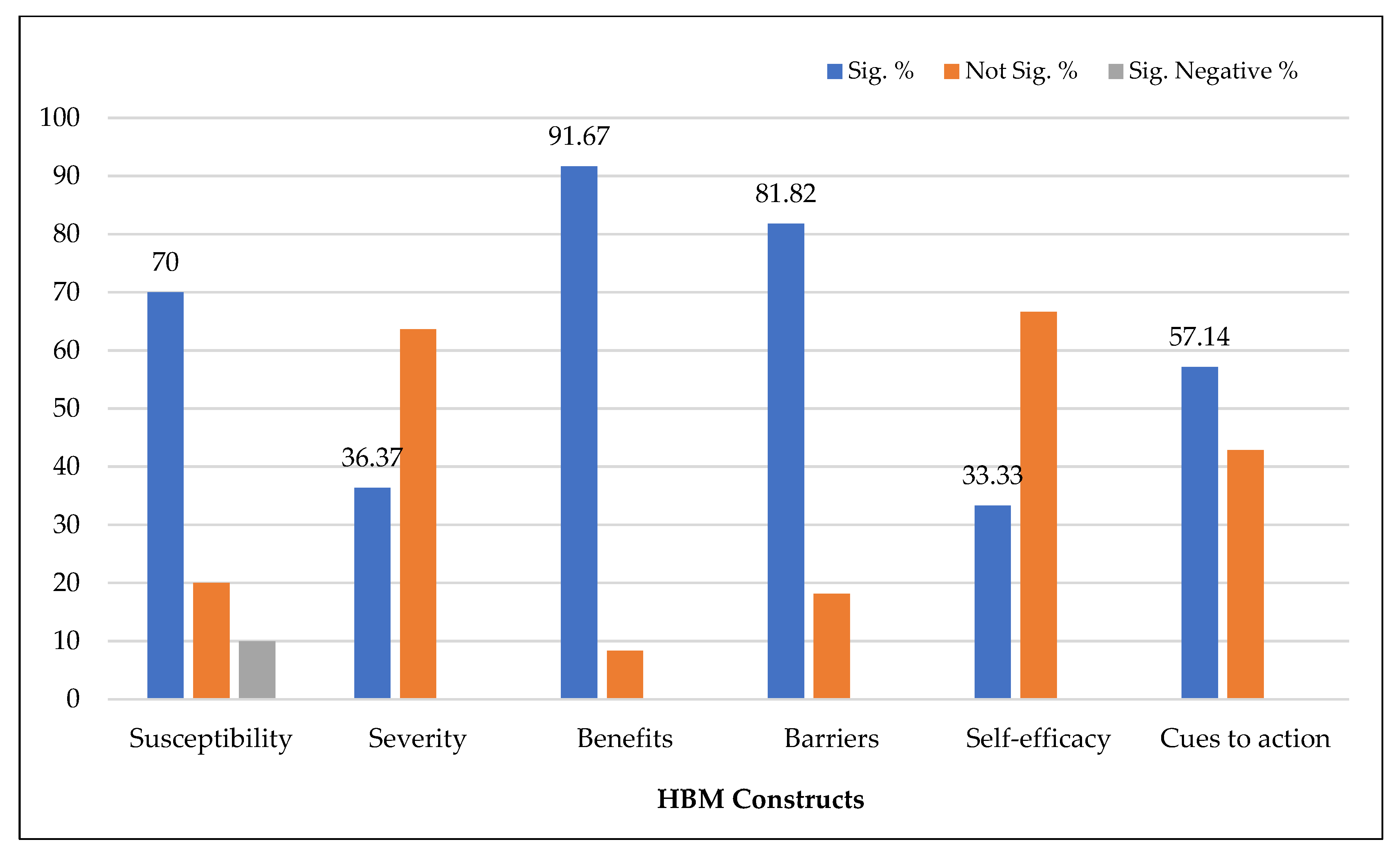
3.3. HBM Constructs Associated with Vaccination Intention
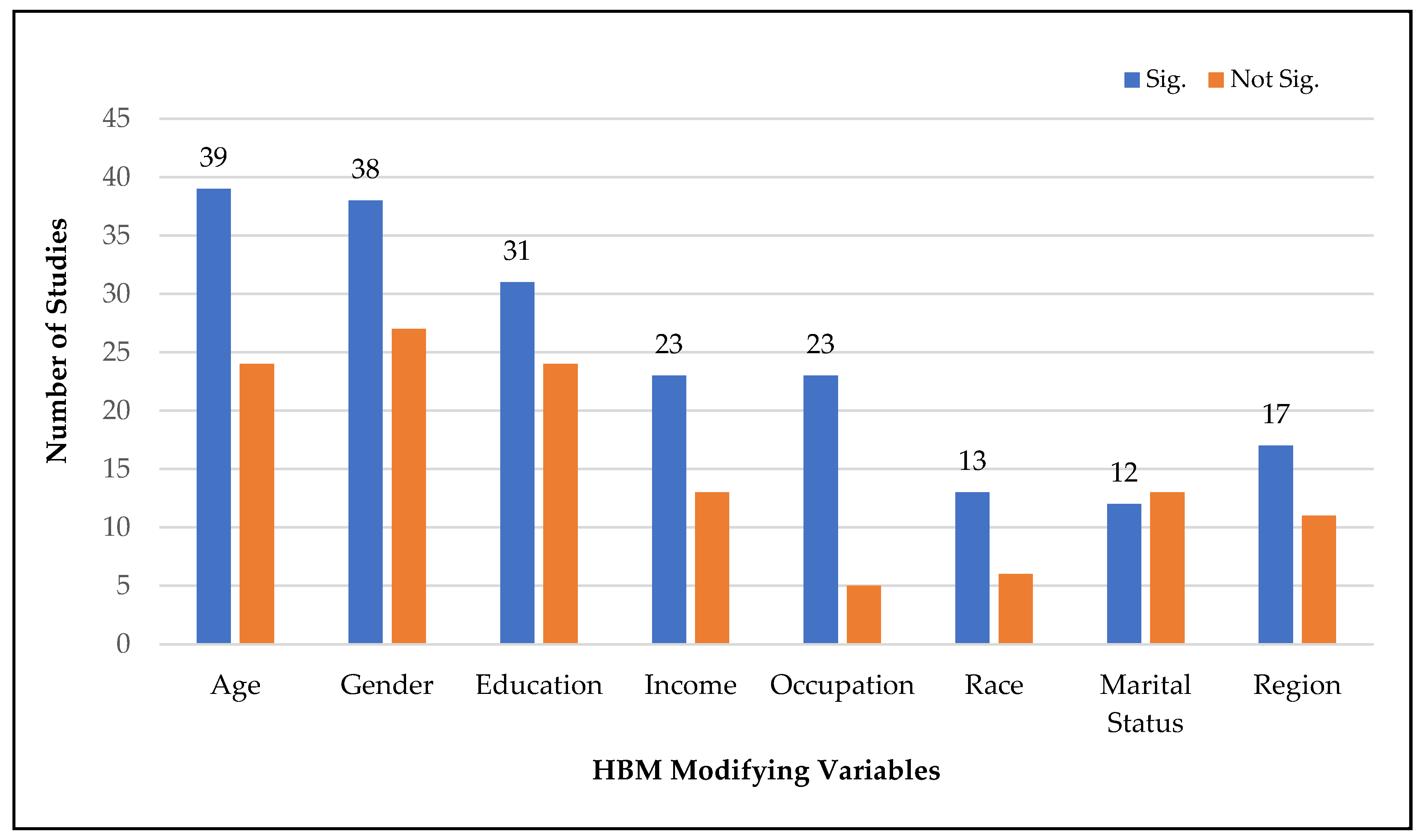
3.4. Modifying HBM Constructs Associated with Vaccination Intention
3.5. HBM Constructs Associated with Vaccination Intention by Data Collection Year, Country, Continent, and Sample
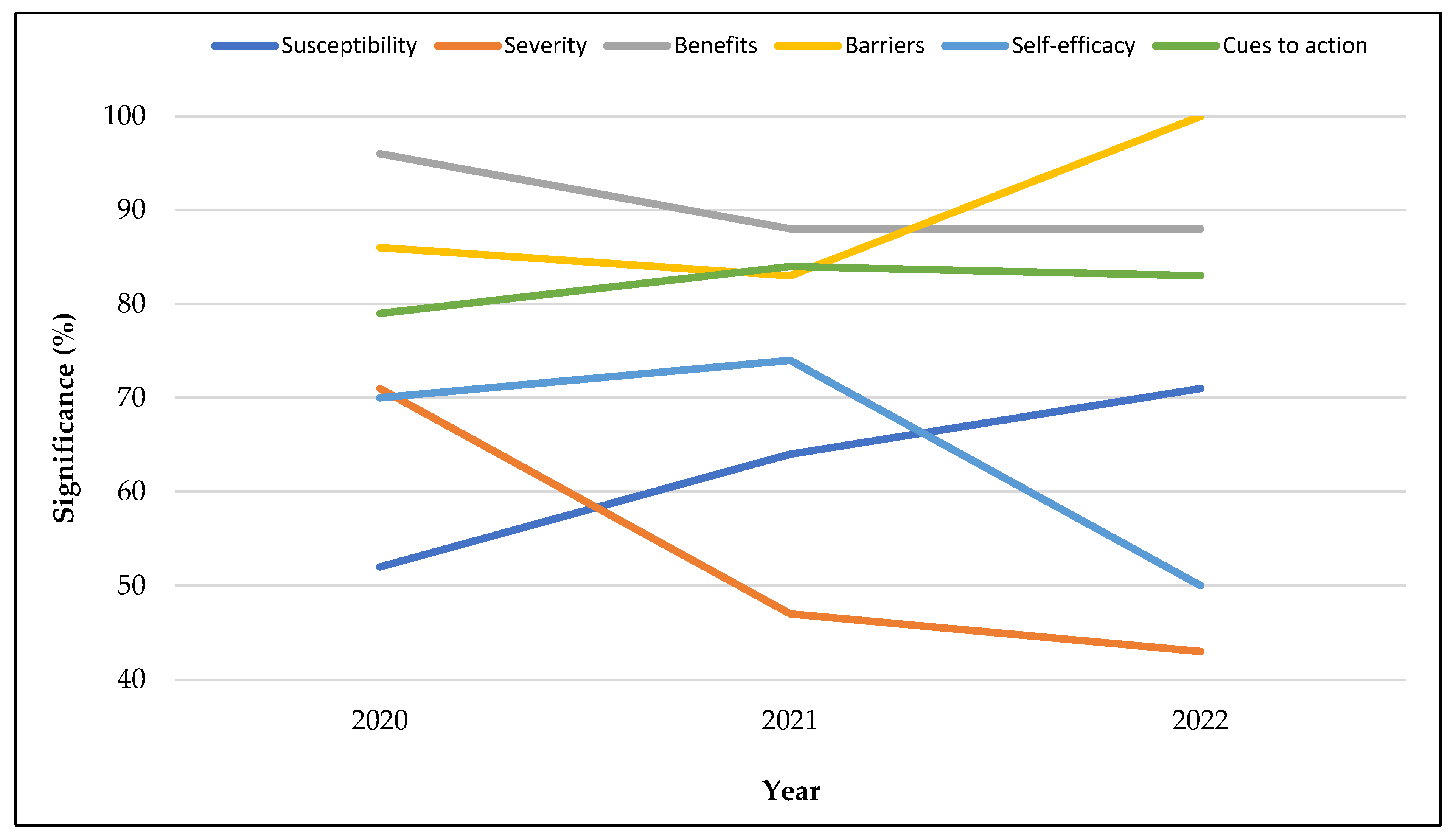
3.5.1. Data Collection Year
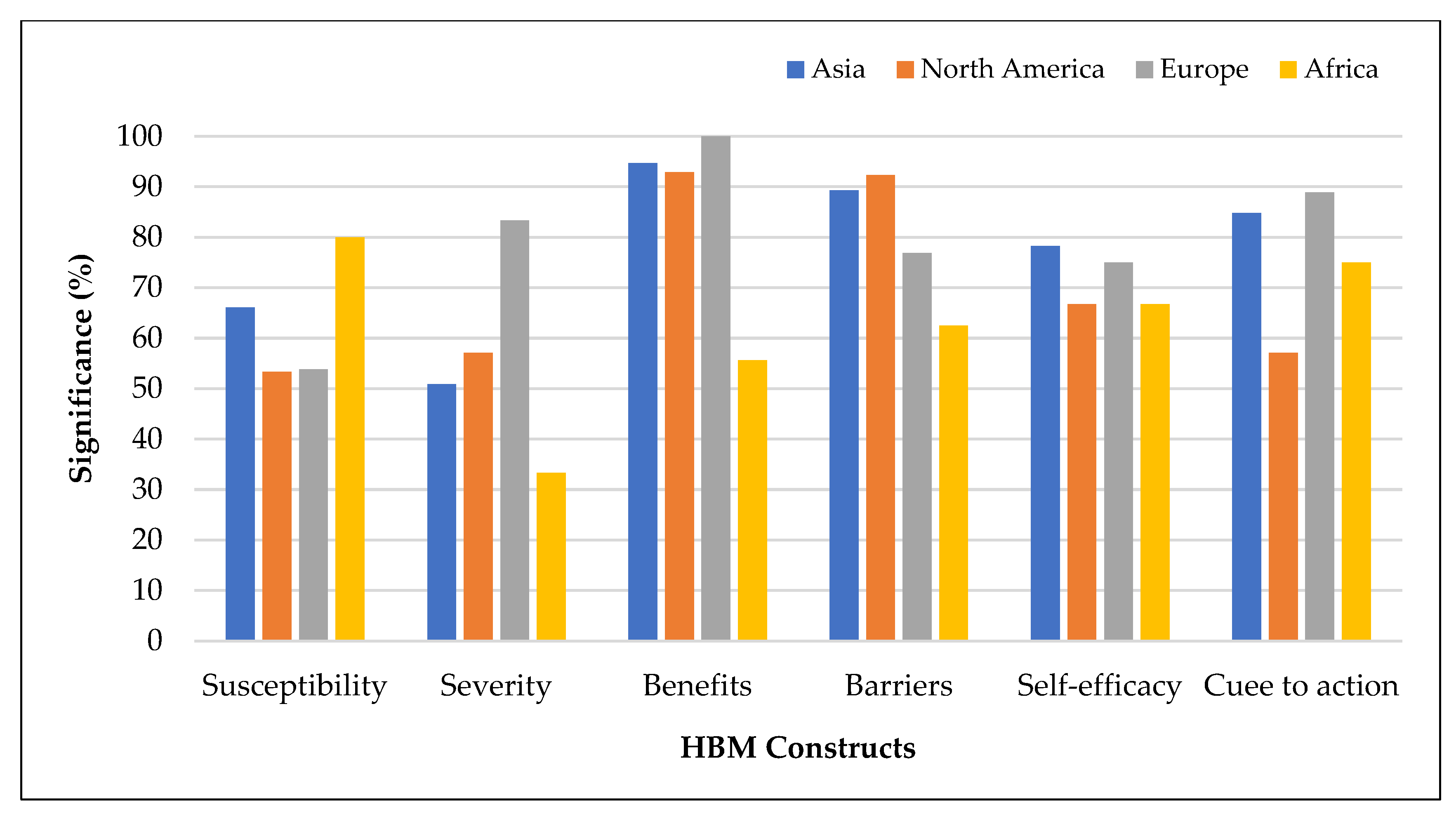
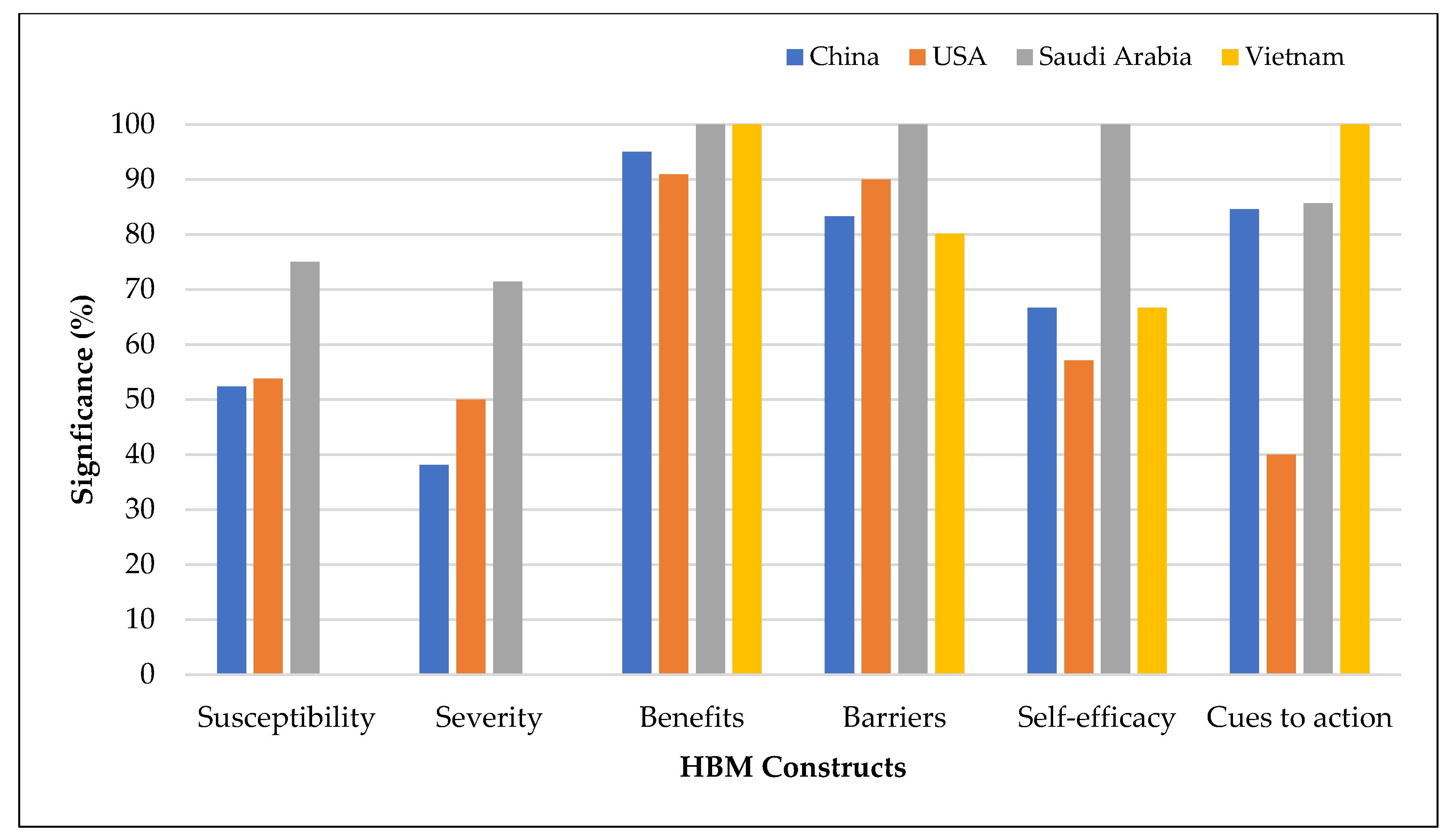
3.5.2. Geographic Location
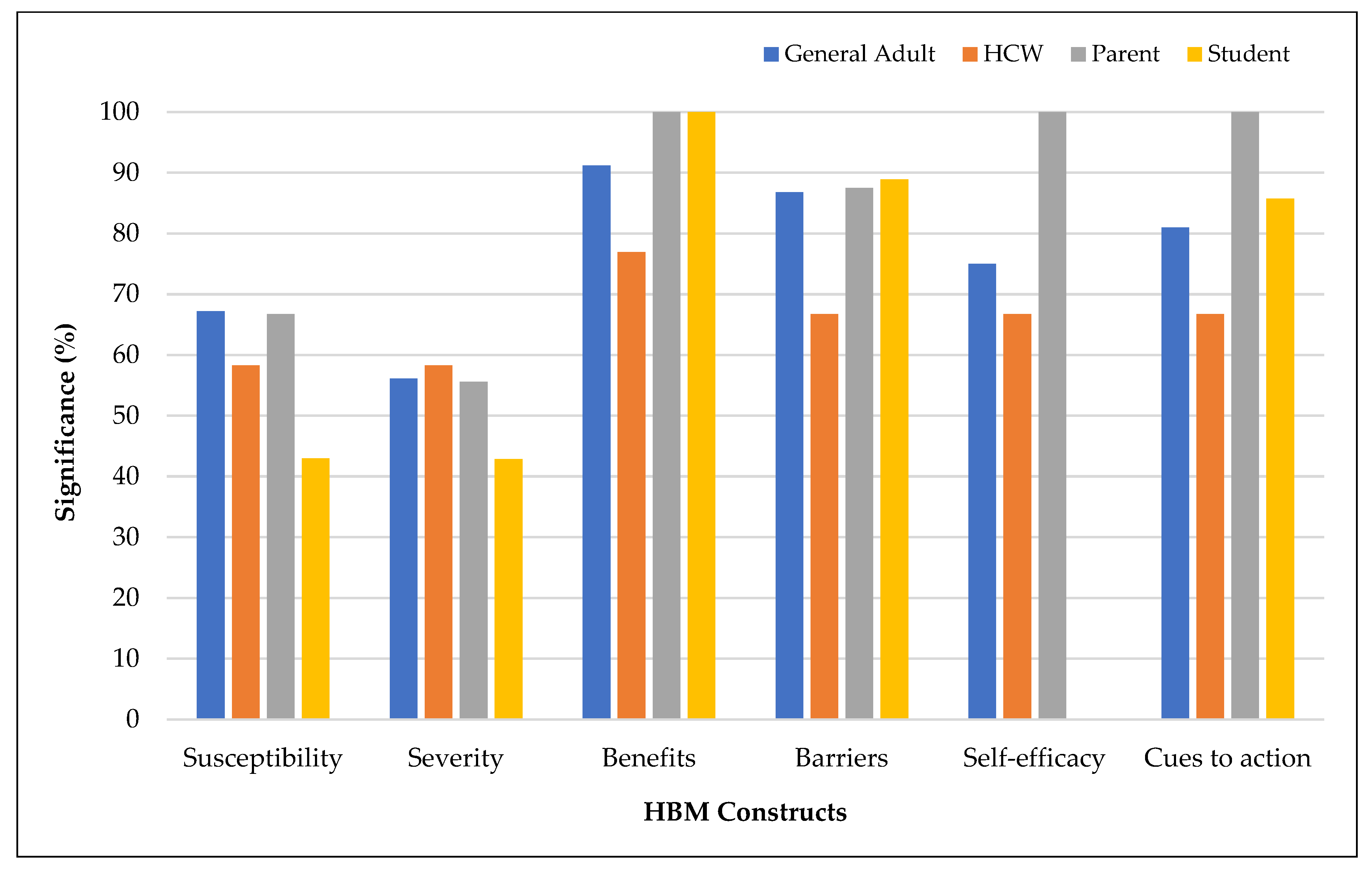
3.5.3. Study Population
4. Discussion and Implications
5. Directions for Future Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 12 March 2023).
- Zintel, S.; Flock, C.; Arbogast, A.L.; Forster, A.; Von Wagner, C.; Sieverding, M. Gender differences in the intention to get vaccinated against COVID-19: A systematic review and meta-analysis. J. Public Health 2022, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Intention of healthcare workers to accept COVID-19 vaccination and related factors: A systematic review and meta-analysis. Asian Pac. J. Trop. Med. 2021, 14, 543. [Google Scholar] [CrossRef]
- Al-Amer, R.; Maneze, D.; Everett, B.; Montayre, J.; Villarosa, A.R.; Dwekat, E.; Salamonson, Y. COVID-19 Vaccination Intention in the First Year of the Pandemic: A Systematic Review. J. Clin. Nurs. 2022, 31, 62–86. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Chinese Parents’ Intentions to Vaccinate Their Children against SARS-CoV-2 Infection and Vaccine Preferences. Hum. Vaccines Immunother. 2021, 17, 4806–4815. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, Y. Multilevel Determinants of COVID-19 Vaccination Hesitancy in the United States: A Rapid Systematic Review. Prev. Med. Rep. 2022, 25, 101673. [Google Scholar] [CrossRef]
- AlShurman, B.A.; Khan, A.F.; Mac, C.; Majeed, M.; Butt, Z.A. What demographic, social, and contextual factors influence the intention to use COVID-19 vaccines: A scoping review. Int. J. Environ. Res. Public Health 2021, 18, 9342. [Google Scholar] [CrossRef]
- Biswas, M.; Alzubaidi, M.S.; Shah, U.; Abd-Alrazaq, A.A.; Shah, Z. A scoping review to find out worldwide COVID-19 vaccine hesitancy and its underlying determinants. Vaccines 2021, 9, 1243. [Google Scholar] [CrossRef]
- Wang, Q.; Yang, L.; Jin, H.; Lin, L. Vaccination against COVID-19: A Systematic Review and Meta-Analysis of Acceptability and Its Predictors. Prev. Med. 2021, 150, 106694. [Google Scholar] [CrossRef]
- Chen, H.; Li, X.; Gao, J.; Liu, X.; Mao, Y.; Wang, R.; Zheng, P.; Xiao, Q.; Jia, Y.; Fu, H.; et al. Health Belief Model Perspective on the Control of COVID-19 Vaccine Hesitancy and the Promotion of Vaccination in China: Web-Based Cross-sectional Study. J. Med. Internet Res. 2021, 23, e29329. [Google Scholar] [CrossRef]
- Limbu, Y.B.; Gautam, R.K.; Pham, L. The Health Belief Model Applied to COVID-19 Vaccine Hesitancy: A Systematic Review. Vaccines 2022, 10, 973. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Whiting, P.; Savović, J.; Higgins, J.P.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R.; ROBIS Group. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Hasan, A.; Khuntia, J.; Yim, D. Does Seeing What Others Do Through Social Media Influence Vaccine Uptake and Help in the Herd Immunity Through Vaccination? A Cross-Sectional Analysis. Front. Public Health 2021, 9, 715931. [Google Scholar] [CrossRef] [PubMed]
- Al-Metwali, B.Z.; Al-Jumaili, A.A.; Al-Alag, Z.A.; Sorofman, B. Exploring the Acceptance of COVID -19 Vaccine among Healthcare Workers and General Population Using Health Belief Model. J. Eval. Clin. Pract. 2021, 27, 1112–1122. [Google Scholar] [CrossRef] [PubMed]
- Almalki, O.S.; Alfayez, O.M.; Al Yami, M.S.; Asiri, Y.A.; Almohammed, O.A. Parents’ Hesitancy to Vaccinate Their 5–11-Year-Old Children Against COVID-19 in Saudi Arabia: Predictors From the Health Belief Model. Front. Public Health 2022, 10, 842862. [Google Scholar] [CrossRef]
- Alobaidi, S. Predictors of Intent to Receive the COVID-19 Vaccination Among the Population in the Kingdom of Saudi Arabia: A Survey Study. JMDH 2021, 14, 1119–1128. [Google Scholar] [CrossRef]
- Alobaidi, S.; Hashim, A. Predictors of the Third (Booster) Dose of COVID-19 Vaccine Intention among the Healthcare Workers in Saudi Arabia: An Online Cross-Sectional Survey. Vaccines 2022, 10, 987. [Google Scholar] [CrossRef]
- Alobaidi, S.; Alsolami, E.; Sherif, A.; Almahdy, M.; Elmonier, R.; Alobaidi, W.Y.; Akl, A. COVID-19 Booster Vaccine Hesitancy among Hemodialysis Patients in Saudi Arabia Using the Health Belief Model: A Multi-Centre Experience. Vaccines 2023, 11, 95. [Google Scholar] [CrossRef]
- An, P.L.; Nguyen, H.T.N.; Dang, H.T.B.; Huynh, Q.N.H.; Pham, B.D.U.; Huynh, G. Integrating Health Behavior Theories to Predict Intention to Get a COVID-19 Vaccine. Health Serv. Insights 2021, 14, 117863292110601. [Google Scholar] [CrossRef]
- Ao, Q.; Egolet, R.O.; Yin, H.; Cui, F. Acceptance of COVID-19 Vaccines among Adults in Lilongwe, Malawi: A Cross-Sectional Study Based on the Health Belief Model. Vaccines 2022, 10, 760. [Google Scholar] [CrossRef] [PubMed]
- Apuke, O.D.; Asude Tunca, E. Modelling the Factors That Predict the Intention to Take COVID-19 Vaccine in Nigeria. J. Asian Afr. Stud. 2022. [Google Scholar] [CrossRef]
- Arabyat, R.M.; Nusair, M.B.; Al-Azzam, S.I.; Amawi, H.A.; El-Hajji, F.D. Willingness to Pay for COVID-19 Vaccines: Applying the Health Belief Model. Res. Soc. Adm. Pharm. 2023, 19, 95–101. [Google Scholar] [CrossRef]
- Banik, R.; Islam, M.S.; Pranta, M.U.R.; Rahman, Q.M.; Rahman, M.; Pardhan, S.; Driscoll, R.; Hossain, S.; Sikder, M.T. Understanding the Determinants of COVID-19 Vaccination Intention and Willingness to Pay: Findings from a Population-Based Survey in Bangladesh. BMC Infect. Dis. 2021, 21, 892. [Google Scholar] [CrossRef] [PubMed]
- Barattucci, M.; Pagliaro, S.; Ballone, C.; Teresi, M.; Consoli, C.; Garofalo, A.; De Giorgio, A.; Ramaci, T. Trust in Science as a Possible Mediator between Different Antecedents and COVID-19 Booster Vaccination Intention: An Integration of Health Belief Model (HBM) and Theory of Planned Behavior (TPB). Vaccines 2022, 10, 1099. [Google Scholar] [CrossRef] [PubMed]
- Berg, M.B.; Lin, L. Predictors of COVID-19 Vaccine Intentions in the United States: The Role of Psychosocial Health Constructs and Demographic Factors. Transl. Behav. Med. 2021, 11, 1782–1788. [Google Scholar] [CrossRef]
- Berni, I.; Menouni, A.; Filali Zegzouti, Y.; Kestemont, M.-P.; Godderis, L.; El Jaafari, S. Factors Associated with COVID-19 Vaccine Acceptance in Morocco: Applying the Health Belief Model. Vaccines 2022, 10, 784. [Google Scholar] [CrossRef]
- Burke, P.F.; Masters, D.; Massey, G. Enablers and Barriers to COVID-19 Vaccine Uptake: An International Study of Perceptions and Intentions. Vaccine 2021, 39, 5116–5128. [Google Scholar] [CrossRef]
- Cahapay, M.B. To Get or Not to Get: Examining the Intentions of Philippine Teachers to Vaccinate against COVID-19. J. Hum. Behav. Soc. Environ. 2022, 32, 325–335. [Google Scholar] [CrossRef]
- Caple, A.; Dimaano, A.; Sagolili, M.M.; Uy, A.A.; Aguirre, P.M.; Alano, D.L.; Camaya, G.S.; Ciriaco, B.J.; Clavo, P.J.M.; Cuyugan, D.; et al. Interrogating COVID-19 Vaccine Intent in the Philippines with a Nationwide Open-Access Online Survey. PeerJ 2022, 10, e12887. [Google Scholar] [CrossRef]
- Chu, H.; Liu, S. Integrating Health Behavior Theories to Predict American’s Intention to Receive a COVID-19 Vaccine. Patient Educ. Couns. 2021, 104, 1878–1886. [Google Scholar] [CrossRef] [PubMed]
- Coe, A.B.; Elliott, M.H.; Gatewood, S.B.S.; Goode, J.-V.R.; Moczygemba, L.R. Perceptions and Predictors of Intention to Receive the COVID-19 Vaccine. Res. Soc. Adm. Pharm. 2022, 18, 2593–2599. [Google Scholar] [CrossRef]
- Duan, L.; Wang, Y.; Dong, H.; Song, C.; Zheng, J.; Li, J.; Li, M.; Wang, J.; Yang, J.; Xu, J. The COVID-19 Vaccination Behavior and Correlates in Diabetic Patients: A Health Belief Model Theory-Based Cross-Sectional Study in China, 2021. Vaccines 2022, 10, 659. [Google Scholar] [CrossRef] [PubMed]
- Dziedzic, A.; Issa, J.; Hussain, S.; Tanasiewicz, M.; Wojtyczka, R.; Kubina, R.; Konwinska, M.D.; Riad, A. COVID-19 Vaccine Booster Hesitancy (VBH) of Healthcare Professionals and Students in Poland: Cross-Sectional Survey-Based Study. Front. Public Health 2022, 10, 938067. [Google Scholar] [CrossRef] [PubMed]
- Ellithorpe, M.E.; Aladé, F.; Adams, R.B.; Nowak, G.J. Looking Ahead: Caregivers’ COVID-19 Vaccination Intention for Children 5 Years Old and Younger Using the Health Belief Model. Vaccine 2022, 40, 1404–1412. [Google Scholar] [CrossRef]
- Enea, V.; Eisenbeck, N.; Carreno, D.F.; Douglas, K.M.; Sutton, R.M.; Agostini, M.; Bélanger, J.J.; Gützkow, B.; Kreienkamp, J.; Abakoumkin, G.; et al. Intentions to Be Vaccinated Against COVID-19: The Role of Prosociality and Conspiracy Beliefs across 20 Countries. Health Commun. 2022, 1–10. [Google Scholar] [CrossRef]
- Getachew, T.; Lami, M.; Eyeberu, A.; Balis, B.; Debella, A.; Eshetu, B.; Degefa, M.; Mesfin, S.; Negash, A.; Bekele, H.; et al. Acceptance of COVID-19 Vaccine and Associated Factors among Health Care Workers at Public Hospitals in Eastern Ethiopia Using the Health Belief Model. Front. Public Health 2022, 10, 957721. [Google Scholar] [CrossRef]
- Getachew, T.; Negash, A.; Degefa, M.; Lami, M.; Balis, B.; Debela, A.; Gemechu, K.; Shiferaw, K.; Nigussie, K.; Bekele, H.; et al. COVID-19 Vaccine Acceptance and Associated Factors among Adult Clients at Public Hospitals in Eastern Ethiopia Using the Health Belief Model: Multicentre Cross-Sectional Study. BMJ Open 2023, 13, e070551. [Google Scholar] [CrossRef]
- Ghazy, R.M.; Abdou, M.S.; Awaidy, S.; Sallam, M.; Elbarazi, I.; Youssef, N.; Fiidow, O.A.; Mehdad, S.; Hussein, M.F.; Adam, M.F.; et al. Acceptance of COVID-19 Vaccine Booster Doses Using the Health Belief Model: A Cross-Sectional Study in Low-Middle- and High-Income Countries of the East Mediterranean Region. Int. J. Environ. Res. Public Health 2022, 19, 12136. [Google Scholar] [CrossRef]
- Goffe, L.; Antonopoulou, V.; Meyer, C.J.; Graham, F.; Tang, M.Y.; Lecouturier, J.; Grimani, A.; Bambra, C.; Kelly, M.P.; Sniehotta, F.F. Factors Associated with Vaccine Intention in Adults Living in England Who Either Did Not Want or Had Not yet Decided to Be Vaccinated against COVID-19. Hum. Vaccines Immunother. 2021, 17, 5242–5254. [Google Scholar] [CrossRef]
- Goruntla, N.; Chintamani, S.; Bhanu, P.; Samyuktha, S.; Veerabhadrappa, K.; Bhupalam, P.; Ramaiah, J. Predictors of Acceptance and Willingness to Pay for the COVID-19 Vaccine in the General Public of India: A Health Belief Model Approach. Asian Pac. J. Trop. Med. 2021, 14, 165. [Google Scholar] [CrossRef]
- Guidry, J.P.D.; Laestadius, L.I.; Vraga, E.K.; Miller, C.A.; Perrin, P.B.; Burton, C.W.; Ryan, M.; Fuemmeler, B.F.; Carlyle, K.E. Willingness to Get the COVID-19 Vaccine with and without Emergency Use Authorization. Am. J. Infect. Control 2021, 49, 137–142. [Google Scholar] [CrossRef]
- Guidry, J.P.D.; Miller, C.A.; Perrin, P.B.; Laestadius, L.I.; Zurlo, G.; Savage, M.W.; Stevens, M.; Fuemmeler, B.F.; Burton, C.W.; Gültzow, T.; et al. Between Healthcare Practitioners and Clergy: Evangelicals and COVID-19 Vaccine Hesitancy. Int. J. Environ. Res. Public Health 2022, 19, 11120. [Google Scholar] [CrossRef] [PubMed]
- Guillon, M.; Kergall, P. Factors Associated with COVID-19 Vaccination Intentions and Attitudes in France. Public Health 2021, 198, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Handebo, S.; Wolde, M.; Shitu, K.; Kassie, A. Determinant of Intention to Receive COVID-19 Vaccine among School Teachers in Gondar City, Northwest Ethiopia. PLoS ONE 2021, 16, e0253499. [Google Scholar] [CrossRef] [PubMed]
- Hawlader, M.D.H.; Rahman, M.L.; Nazir, A.; Ara, T.; Haque, M.M.A.; Saha, S.; Barsha, S.Y.; Hossian, M.; Matin, K.F.; Siddiquea, S.R.; et al. COVID-19 Vaccine Acceptance in South Asia: A Multi-Country Study. Int. J. Infect. Dis. 2022, 114, 1–10. [Google Scholar] [CrossRef]
- Hossian, M.; Khan, M.A.S.; Nazir, A.; Nabi, M.H.; Hasan, M.; Maliha, R.; Hossain, M.A.; Rashid, M.U.; Itrat, N.; Hawlader, M.D.H. Factors Affecting Intention to Take COVID-19 Vaccine among Pakistani University Students. PLoS ONE 2022, 17, e0262305. [Google Scholar] [CrossRef]
- Hu, D.; Liu, Z.; Gong, L.; Kong, Y.; Liu, H.; Wei, C.; Wu, X.; Zhu, Q.; Guo, Y. Exploring the Willingness of the COVID-19 Vaccine Booster Shots in China Using the Health Belief Model: Web-Based Online Cross-Sectional Study. Vaccines 2022, 10, 1336. [Google Scholar] [CrossRef]
- Huang, C.; Yan, D.; Liang, S. The Relationship between Information Dissemination Channels, Health Belief, and COVID-19 Vaccination Intention: Evidence from China. J. Environ. Public Health 2023, 2023, 6915125. [Google Scholar] [CrossRef]
- Huynh, G.; Tran, T.; Nguyen, H.N.; Pham, L. COVID-19 Vaccination Intention among Healthcare Workers in Vietnam. Asian Pac. J. Trop. Med. 2021, 14, 159. [Google Scholar] [CrossRef]
- Iacob, C.I.; Ionescu, D.; Avram, E.; Cojocaru, D. COVID-19 Pandemic Worry and Vaccination Intention: The Mediating Role of the Health Belief Model Components. Front. Psychol. 2021, 12, 674018. [Google Scholar] [CrossRef] [PubMed]
- Jahanshahi-Amjazi, R.; Rezaeian, M.; Abdolkarimi, M.; Nasirzadeh, M. Predictors of the Intention to Receive the COVID 19 Vaccine by Iranians 18–70 Year Old: Application of Health Belief Model. J. Edu. Health Promot. 2022, 11, 175. [Google Scholar] [CrossRef]
- Jiang, T.; Zhou, X.; Wang, H.; Dong, S.; Wang, M.; Akezhuoli, H.; Zhu, H. COVID-19 Vaccination Intention and Influencing Factors among Different Occupational Risk Groups: A Cross-Sectional Study. Hum. Vaccines Immunother. 2021, 17, 3433–3440. [Google Scholar] [CrossRef] [PubMed]
- Jin, Q.; Raza, S.H.; Yousaf, M.; Zaman, U.; Siang, J.M.L.D. Can Communication Strategies Combat COVID-19 Vaccine Hesitancy with Trade-Off between Public Service Messages and Public Skepticism? Experimental Evidence from Pakistan. Vaccines 2021, 9, 757. [Google Scholar] [CrossRef]
- Kasting, M.L.; Macy, J.T.; Grannis, S.J.; Wiensch, A.J.; Lavista Ferres, J.M.; Dixon, B.E. Factors Associated With the Intention to Receive the COVID-19 Vaccine: Cross-Sectional National Study. JMIR Public Health Surveill. 2022, 8, e37203. [Google Scholar] [CrossRef]
- Khalafalla, H.E.; Tumambeng, M.Z.; Halawi, M.H.A.; Masmali, E.M.A.; Tashari, T.B.M.; Arishi, F.H.A.; Shadad, R.H.M.; Alfaraj, S.Z.A.; Fathi, S.M.A.; Mahfouz, M.S. COVID-19 Vaccine Hesitancy Prevalence and Predictors among the Students of Jazan University, Saudi Arabia Using the Health Belief Model: A Cross-Sectional Study. Vaccines 2022, 10, 289. [Google Scholar] [CrossRef]
- Kabir, R.; Mahmud, I.; Chowdhury, M.T.H.; Vinnakota, D.; Jahan, S.S.; Siddika, N.; Isha, S.N.; Nath, S.K.; Hoque Apu, E. COVID-19 Vaccination Intent and Willingness to Pay in Bangladesh: A Cross-Sectional Study. Vaccines 2021, 9, 416. [Google Scholar] [CrossRef]
- Lai, X.; Zhu, H.; Wang, J.; Huang, Y.; Jing, R.; Lyu, Y.; Zhang, H.; Feng, H.; Guo, J.; Fang, H. Public Perceptions and Acceptance of COVID-19 Booster Vaccination in China: A Cross-Sectional Study. Vaccines 2021, 9, 1461. [Google Scholar] [CrossRef]
- Le An, P.; Nguyen, H.T.N.; Nguyen, D.D.; Vo, L.Y.; Huynh, G. The Intention to Get a COVID-19 Vaccine among the Students of Health Science in Vietnam. Hum. Vaccines Immunother. 2021, 17, 4823–4828. [Google Scholar] [CrossRef]
- Le, C.N.; Nguyen, U.T.T.; Do, D.T.H. Predictors of COVID-19 vaccine acceptability among health professions students in Vietnam. BMC Public Health 2022, 22, 854. [Google Scholar] [CrossRef]
- Lee, L.Y.; Chu, K.; Chan, M.H.; Wong, C.T.; Leung, H.P.; Chan, I.C.; Ng, C.K.; Wong, R.Y.; Pun, A.L.; Ng, Y.H.; et al. Living in a Region With a Low Level of COVID-19 Infection: Health Belief Toward COVID-19 Vaccination and Intention to Receive a COVID-19 Vaccine in Hong Kong Individuals. INQUIRY 2022, 59, 004695802210827. [Google Scholar] [CrossRef]
- Li, J.-B.; Lau, E.Y.H.; Chan, D.K.C. Why Do Hong Kong Parents Have Low Intention to Vaccinate Their Children against COVID-19? Testing Health Belief Model and Theory of Planned Behavior in a Large-Scale Survey. Vaccine 2022, 40, 2772–2780. [Google Scholar] [CrossRef]
- Li, G.; Zhong, Y.; Htet, H.; Luo, Y.; Xie, X.; Wichaidit, W. COVID-19 Vaccine Acceptance and Associated Factors among Unvaccinated Workers at a Tertiary Hospital in Southern Thailand. Health Serv. Res. Manag. Epidemiol. 2022, 9, 233339282210830. [Google Scholar] [CrossRef]
- Liao, Q.; Cowling, B.J.; Xiao, J.; Yuan, J.; Dong, M.; Ni, M.Y.; Fielding, R.; Lam, W.W.T. Priming with social benefit information of vaccination to increase acceptance of COVID-19 vaccines. Vaccine 2022, 40, 1074–1081. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 Vaccine Demand and Hesitancy: A Nationwide Online Survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Liu, R.; Huang, Y.-H.C.; Sun, J.; Lau, J.; Cai, Q. A Shot in the Arm for Vaccination Intention: The Media and the Health Belief Model in Three Chinese Societies. Int. J. Environ. Res. Public Health 2022, 19, 3705. [Google Scholar] [CrossRef]
- López-Cepero, A.; Cameron, S.; Negrón, L.E.; Colón-López, V.; Colón-Ramos, U.; Mattei, J.; Fernández-Repollet, E.; Pérez, C.M. Uncertainty and Unwillingness to Receive a COVID-19 Vaccine in Adults Residing in Puerto Rico: Assessment of Perceptions, Attitudes, and Behaviors. Hum. Vaccines Immunother. 2021, 17, 3441–3449. [Google Scholar] [CrossRef]
- Lyons, N.; Bhagwandeen, B.; Edwards, J. Factors Affecting COVID-19 Vaccination Intentions among Patients Attending a Large HIV Treatment Clinic in Trinidad Using Constructs of the Health Belief Model. Vaccines 2022, 11, 4. [Google Scholar] [CrossRef]
- Mahmud, I.; Kabir, R.; Rahman, M.A.; Alradie-Mohamed, A.; Vinnakota, D.; Al-Mohaimeed, A. The Health Belief Model Predicts Intention to Receive the COVID-19 Vaccine in Saudi Arabia: Results from a Cross-Sectional Survey. Vaccines 2021, 9, 864. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, I.; Al Imam, M.H.; Vinnakota, D.; Kheirallah, K.A.; Jaber, M.F.; Abalkhail, A.; Alasqah, I.; Alslamah, T.; Kabir, R. Vaccination Intention against COVID-19 among the Unvaccinated in Jordan during the Early Phase of the Vaccination Drive: A Cross-Sectional Survey. Vaccines 2022, 10, 1159. [Google Scholar] [CrossRef] [PubMed]
- Maria, S.; Pelupessy, D.C.; Koesnoe, S.; Yunihastuti, E.; Handayani, D.O.T.L.; Siddiq, T.H.; Mulyantini, A.; Halim, A.R.V.; Wahyuningsih, E.S.; Widhani, A.; et al. COVID-19 Booster Vaccine Intention by Health Care Workers in Jakarta, Indonesia: Using the Extended Model of Health Behavior Theories. Trop. Med. 2022, 7, 323. [Google Scholar] [CrossRef]
- Mercadante, A.R.; Law, A.V. Will they, or Won’t they? Examining patients’ vaccine intention for flu and COVID-19 using the Health Belief Model. Res. Soc. Adm. Pharm. 2021, 17, 1596–1605. [Google Scholar] [CrossRef] [PubMed]
- Miyachi, T.; Sugano, Y.; Tanaka, S.; Hirayama, J.; Yamamoto, F.; Nomura, K. COVID-19 Vaccine Intention and Knowledge, Literacy, and Health Beliefs among Japanese University Students. Vaccines 2022, 10, 893. [Google Scholar] [CrossRef]
- Mohammed, A.H.; Hassan, B.A.R.; Wayyes, A.M.; Gadhban, A.Q.; Blebil, A.; Alhija, S.A.; Darwish, R.M.; Al-Zaabi, A.T.; Othman, G.; Jaber, A.A.S.; et al. Parental Health Beliefs, Intention, and Strategies about COVID-19 Vaccine for Their Children: A Cross-Sectional Analysis from Five Arab Countries in the Middle East. Vaccine 2022, 40, 6549–6557. [Google Scholar] [CrossRef]
- Morar, C.; Tiba, A.; Jovanovic, T.; Valjarević, A.; Ripp, M.; Vujičić, M.D.; Stankov, U.; Basarin, B.; Ratković, R.; Popović, M.; et al. Supporting Tourism by Assessing the Predictors of COVID-19 Vaccination for Travel Reasons. Int. J. Environ. Res. Public Health 2022, 19, 918. [Google Scholar] [CrossRef]
- Nguyen, V.T.; Nguyen, M.Q.; Le, N.T.; Nguyen, T.N.H.; Huynh, G. Predictors of Intention to Get a COVID-19 Vaccine of Health Science Students: A Cross-Sectional Study. RMHP 2021, 14, 4023–4030. [Google Scholar] [CrossRef]
- Okai, G.A.; Abekah-Nkrumah, G. The Level and Determinants of COVID-19 Vaccine Acceptance in Ghana. PLoS ONE 2022, 17, e0270768. [Google Scholar] [CrossRef]
- Okmi, E.A.; Almohammadi, E.; Alaamri, O.; Alfawaz, R.; Alomari, N.; Saleh, M.; Alsuwailem, S.; Moafa, N.J. Determinants of COVID-19 Vaccine Acceptance Among the General Adult Population in Saudi Arabia Based on the Health Belief Model: A Web-Based Cross-Sectional Study. Cureus 2022, 14, 28326. [Google Scholar] [CrossRef] [PubMed]
- Okuyan, B.; Bektay, M.Y.; Demirci, M.Y.; Ay, P.; Sancar, M. Factors Associated with Turkish Pharmacists’ Intention to Receive COVID-19 Vaccine: An Observational Study. Int. J. Clin. Pharm. 2022, 44, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Otiti-Sengeri, J.; Andrew, O.B.; Lusobya, R.C.; Atukunda, I.; Nalukenge, C.; Kalinaki, A.; Mukisa, J.; Nakanjako, D.; Colebunders, R. High COVID-19 Vaccine Acceptance among Eye Healthcare Workers in Uganda. Vaccines 2022, 10, 609. [Google Scholar] [CrossRef]
- Patwary, M.M.; Bardhan, M.; Disha, A.S.; Hasan, M.; Haque, M.Z.; Sultana, R.; Hossain, M.R.; Browning, M.H.E.M.; Alam, M.A.; Sallam, M. Determinants of COVID-19 Vaccine Acceptance among the Adult Population of Bangladesh Using the Health Belief Model and the Theory of Planned Behavior Model. Vaccines 2021, 9, 1393. [Google Scholar] [CrossRef]
- Qin, C.; Yan, W.; Du, M.; Liu, Q.; Tao, L.; Liu, M.; Liu, J. Acceptance of the COVID-19 Vaccine Booster Dose and Associated Factors among the Elderly in China Based on the Health Belief Model (HBM): A National Cross-Sectional Study. Front. Public Health 2022, 10, 986916. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Wang, R.; Tao, L.; Liu, M.; Liu, J. Acceptance of a Third Dose of COVID-19 Vaccine and Associated Factors in China Based on Health Belief Model: A National Cross-Sectional Study. Vaccines 2022, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Wang, R.; Tao, L.; Liu, M.; Liu, J. Association Between Risk Perception and Acceptance for a Booster Dose of COVID-19 Vaccine to Children Among Child Caregivers in China. Front. Public Health 2022, 10, 834572. [Google Scholar] [CrossRef]
- Qin, C.; Du, M.; Wang, Y.; Liu, Q.; Yan, W.; Tao, L.; Liu, M.; Liu, J. Assessing acceptability of the fourth dose against COVID-19 among Chinese adults: A population-based survey. Hum. Vaccines Immunother. 2023, 19, 2186108. [Google Scholar] [CrossRef] [PubMed]
- Quinto, J.C.D.; Balderrama, A.N.C.; Hocson, F.N.Z.; Salanguit, M.B.; Palatino, M.C.; Gregorio, E.R., Jr. Association of knowledge and risk perceptions of Manila City school teachers with COVID-19 vaccine acceptance. Philipp. J. Health Res. Dev. 2022, 25, 8–18. [Google Scholar]
- Rabin, C.; Dutra, S. Predicting Engagement in Behaviors to Reduce the Spread of COVID-19: The Roles of the Health Belief Model and Political Party Affiliation. Psychol. Health Med. 2022, 27, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Reindl, D.; Catma, S. A Pre-Vaccine Analysis Using the Health Belief Model to Explain Parents’ Willingness to Vaccinate (WTV) Their Children in the United States: Implications for Vaccination Programs. Expert Rev. Pharm. Outcomes Res. 2022, 22, 753–761. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Rosental, H.; Shmueli, L. Integrating Health Behavior Theories to Predict COVID-19 Vaccine Acceptance: Differences between Medical Students and Nursing Students. Vaccines 2021, 9, 783. [Google Scholar] [CrossRef]
- Rountree, C.; Prentice, G. Segmentation of Intentions towards COVID-19 Vaccine Acceptance through Political and Health Behaviour Explanatory Models. Ir. J. Med. Sci. 2022, 191, 2369–2383. [Google Scholar] [CrossRef]
- Seangpraw, K.; Pothisa, T.; Boonyathee, S.; Ong-Artborirak, P.; Tonchoy, P.; Kantow, S.; Auttama, N.; Choowanthanapakorn, M. Using the Health Belief Model to Predict Vaccination Intention Among COVID-19 Unvaccinated People in Thai Communities. Front. Med. 2022, 9, 890503. [Google Scholar] [CrossRef] [PubMed]
- Seboka, B.T.; Yehualashet, D.E.; Belay, M.M.; Kabthymer, R.H.; Ali, H.; Hailegebreal, S.; Demeke, A.D.; Amede, E.S.; Tesfa, G.A. Factors influencing COVID-19 vaccination demand and intent in resource-limited settings: Based on health belief model. Risk Manag. Healthc. Policy 2021, 14, 2743–2756. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Gui, H.; Chua, P.E.Y.; Tan, J.-Y.; Suen, L.K.; Chan, S.W.; Pang, J. Factors Associated with COVID-19 Vaccination Intent in Singapore, Australia and Hong Kong. Vaccine 2022, 40, 2949–2959. [Google Scholar] [CrossRef] [PubMed]
- Shmueli, L. Predicting Intention to Receive COVID-19 Vaccine among the General Population Using the Health Belief Model and the Theory of Planned Behavior Model. BMC Public Health 2021, 21, 804. [Google Scholar] [CrossRef]
- Shmueli, L. The Role of Incentives in Deciding to Receive the Available COVID-19 Vaccine in Israel. Vaccines 2022, 10, 77. [Google Scholar] [CrossRef]
- Short, M.B.; Marek, R.J.; Knight, C.F.; Kusters, I.S. Understanding factors associated with intent to receive the COVID-19 vaccine. Fam. Syst. Health 2022, 40, 160. [Google Scholar] [CrossRef]
- Sieverding, M.; Zintel, S.; Schmidt, L.; Arbogast, A.L.; von Wagner, C. Explaining the Intention to Get Vaccinated against COVID-19: General Attitudes towards Vaccination and Predictors from Health Behavior Theories. Psychol. Health Med. 2023, 28, 161–170. [Google Scholar] [CrossRef]
- Spinewine, A.; Pétein, C.; Evrard, P.; Vastrade, C.; Laurent, C.; Delaere, B.; Henrard, S. Attitudes towards COVID-19 Vaccination among Hospital Staff—Understanding What Matters to Hesitant People. Vaccines 2021, 9, 469. [Google Scholar] [CrossRef]
- Ştefănuţ, A.M.; Vintilă, M.; Tomiţă, M.; Treglia, E.; Lungu, M.A.; Tomassoni, R. The Influence of Health Beliefs, of Resources, of Vaccination History, and of Health Anxiety on Intention to Accept COVID-19 Vaccination. Front. Psychol. 2021, 12, 729803. [Google Scholar] [CrossRef]
- Su, L.; Du, J.; Du, Z. Government Communication, Perceptions of COVID-19, and Vaccination Intention: A Multi-Group Comparison in China. Front. Psychol. 2022, 12, 783374. [Google Scholar] [CrossRef]
- Suess, C.; Maddock, J.E.; Dogru, T.; Mody, M.; Lee, S. Using the Health Belief Model to Examine Travelers’ Willingness to Vaccinate and Support for Vaccination Requirements Prior to Travel. Tour. Manag. 2022, 88, 104405. [Google Scholar] [CrossRef]
- Tran, V.D.; Pak, T.V.; Gribkova, E.I.; Galkina, G.A.; Loskutova, E.E.; Dorofeeva, V.V.; Dewey, R.S.; Nguyen, K.T.; Pham, D.T. Determinants of COVID-19 Vaccine Acceptance in a High Infection-Rate Country: A Cross-Sectional Study in Russia. Pharm. Pract. 2021, 19, 2276. [Google Scholar] [CrossRef] [PubMed]
- Ung, C.O.L.; Hu, Y.; Hu, H.; Bian, Y. Investigating the Intention to Receive the COVID-19 Vaccination in Macao: Implications for Vaccination Strategies. BMC Infect. Dis. 2022, 22, 218. [Google Scholar] [CrossRef] [PubMed]
- Vatcharavongvan, P.; Boonyanitchayakul, N.; Khampachuea, P.; Sinturong, I.; Prasert, V. Health Belief Model and Parents’ Acceptance of the Pfizer-BioNTech and Sinopharm COVID-19 Vaccine for Children Aged 5–18 Years Old: A National Survey. Vaccine 2023, 41, 1480–1489. [Google Scholar] [CrossRef]
- Wagner, A.L.; Wileden, L.; Shanks, T.R.; Goold, S.D.; Morenoff, J.D.; Sheinfeld Gorin, S.N. Mediators of Racial Differences in COVID-19 Vaccine Acceptance and Uptake: A Cohort Study in Detroit, MI. Vaccines 2021, 10, 36. [Google Scholar] [CrossRef]
- Walker, A.N.; Zhang, T.; Peng, X.-Q.; Ge, J.-J.; Gu, H.; You, H. Vaccine Acceptance and Its Influencing Factors: An Online Cross-Sectional Study among International College Students Studying in China. Vaccines 2021, 9, 585. [Google Scholar] [CrossRef]
- Wang, X. Putting Emotions in the Health Belief Model: The Role of Hope and Anticipated Guilt on the Chinese’s Intentions to Get COVID-19 Vaccination. Health Commun. 2022, 1–10. [Google Scholar] [CrossRef]
- Wang, H.; Zhou, X.; Jiang, T.; Wang, X.; Lu, J.; Li, J. Factors Influencing COVID-19 Vaccination Intention among Overseas and Domestic Chinese University Students: A Cross-Sectional Survey. Hum. Vaccines Immunother. 2021, 17, 4829–4837. [Google Scholar] [CrossRef]
- Wijesinghe, M.S.D.; Weerasinghe, W.M.P.C.; Gunawardana, I.; Perera, S.N.S.; Karunapema, R.P.P. Acceptance of COVID-19 Vaccine in Sri Lanka: Applying the Health Belief Model to an Online Survey. Asia Pac. J. Public Health 2021, 33, 598–602. [Google Scholar] [CrossRef]
- Wirawan, G.B.S.; Harjana, N.P.A.; Nugrahani, N.W.; Januraga, P.P. Health Beliefs and Socioeconomic Determinants of COVID-19 Booster Vaccine Acceptance: An Indonesian Cross-Sectional Study. Vaccines 2022, 10, 724. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.-F.; Lee, H.Y.; AbuBakar, S. The Use of the Health Belief Model to Assess Predictors of Intent to Receive the COVID-19 Vaccine and Willingness to Pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Xiao, Q.; Liu, X.; Wang, R.; Mao, Y.; Chen, H.; Li, X.; Liu, X.; Dai, J.; Gao, J.; Fu, H.; et al. Predictors of Willingness to Receive the COVID-19 Vaccine after Emergency Use Authorization: The Role of Coping Appraisal. Vaccines 2021, 9, 967. [Google Scholar] [CrossRef] [PubMed]
- Yan, E.; Lai, D.W.L.; Lee, V.W.P. Predictors of Intention to Vaccinate against COVID-19 in the General Public in Hong Kong: Findings from a Population-Based, Cross-Sectional Survey. Vaccines 2021, 9, 696. [Google Scholar] [CrossRef]
- Yang, X.; Wei, L.; Liu, Z. Promoting COVID-19 Vaccination Using the Health Belief Model: Does Information Acquisition from Divergent Sources Make a Difference? Int. J. Environ. Res. Public Health 2022, 19, 3887. [Google Scholar] [CrossRef] [PubMed]
- Youssef, D.; Abou-Abbas, L.; Berry, A.; Youssef, J.; Hassan, H. Determinants of acceptance of Coronavirus disease-2019 (COVID-19) vaccine among Lebanese health care workers using health belief model. PLoS ONE 2022, 17, e0264128. [Google Scholar] [CrossRef]
- Yu, Y.; Ling, R.H.Y.; Ip, T.K.M.; Luo, S.; Lau, J.T.F. Factors of COVID-19 Vaccination among Hong Kong Chinese Men Who Have Sex with Men during Months 5–8 since the Vaccine Rollout—General Factors and Factors Specific to This Population. Vaccines 2022, 10, 1763. [Google Scholar] [CrossRef] [PubMed]
- Zakeri, M.; Li, J.; Sadeghi, S.D.; Essien, E.J.; Sansgiry, S.S. Strategies to Decrease COVID-19 Vaccine Hesitancy for Children. J. Pharm. Health Serv. Res. 2021, 12, 539–544. [Google Scholar] [CrossRef]
- Zampetakis, L.A.; Melas, C. The Health Belief Model Predicts Vaccination Intentions against COVID-19: A Survey Experiment Approach. Appl. Psychol. Health Well 2021, 13, 469–484. [Google Scholar] [CrossRef]
- Zhang, R.; Yan, J.; Jia, H.; Luo, X.; Liu, Q.; Lin, J. Policy Endorsement and Booster Shot: Exploring Politicized Determinants for Acceptance of a Third Dose of COVID-19 Vaccine in China. Vaccines 2023, 11, 421. [Google Scholar] [CrossRef]
- Zhelyazkova, A.; Kim, S.; Klein, M.; Prueckner, S.; Horster, S.; Kressirer, P.; Choukér, A.; Coenen, M.; Adorjan, K. COVID-19 Vaccination Intent, Barriers and Facilitators in Healthcare Workers: Insights from a Cross-Sectional Study on 2500 Employees at LMU University Hospital in Munich, Germany. Vaccines 2022, 10, 1231. [Google Scholar] [CrossRef] [PubMed]
- Brewer, N.T.; Chapman, G.B.; Gibbons, F.X.; Gerrard, M.; McCaul, K.D.; Weinstein, N. D Meta-analysis of the relationship between risk perception and health behavior: The example of vaccination. Health Psychol. 2007, 26, 136–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsutsui, Y.; Benzion, U.; Shahrabani, S. Economic and behavioral factors in an individual’s decision to take the influenza vaccination in Japan. J. Socio Econ. 2012, 4, 594–602. [Google Scholar] [CrossRef] [Green Version]
- Shahrabani, S.; Benzion, U. Workplace vaccination and other factors impacting influenza vaccination decision among employees in Israel. Int. J. Environ. Res. Public Health 2010, 7, 853–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griva, K.; Tan, K.Y.K.; Chan, F.H.F.; Periakaruppan, R.; Ong, B.W.L.; Soh, A.S.E.; Chen, M.I. Evaluating Rates and Determinants of COVID-19 Vaccine Hesitancy for Adults and Children in the Singapore Population: Strengthening Our Community’s Resilience against Threats from Emerging Infections (SOCRATEs) Cohort. Vaccines 2021, 9, 1415. [Google Scholar] [CrossRef]
- Limbu, Y.B.; Gautam, R.K.; Zhou, W. Predicting Vaccination Intention against COVID-19 Using Theory of Planned Behavior: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 2026. [Google Scholar] [CrossRef]
- Limbu, Y.B.; Huhmann, B.A. Why Some People Are Hesitant to Receive COVID-19 Boosters: A Systematic Review. Trop. Med. Infect. Dis. 2023, 8, 159. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author(s) | Year of Publication | Journal | Country | Vaccine Intention % | Population | Sample Size |
|---|---|---|---|---|---|---|
| Al-Hasan et al. [15] | 2021 | Frontiers in Public Health | NR* | 75 | General population | 372 |
| Al-Metwali et al. [16] | 2021 | Journal of Evaluation in Clinical Practice | Iraq | 62 | HCW | 1680 |
| Almalki et al. [17] | 2022 | Frontier in Public Health | Saudi Arabia | 38 | Parents | 4135 |
| Alobaidi [18] | 2021 | Journal of Multidisciplinary Healthcare | Saudi Arabia | 72 | General population | 1333 |
| Alobaidi and Hashim [19] | 2022 | Vaccines | Saudi Arabia | 71 | HCW | 2059 |
| Alobaidi et al. [20] | 2023 | Vaccines | Saudi Arabia | 78 | Patients | 179 |
| An et al. [21] | 2021 | Health Services Insights | Vietnam | 81 | Patients | 462 |
| Ao et al. [22] | 2022 | Vaccines | Malawi | 61 | General population | 758 |
| Apuke and Tunca [23] | 2022 | Journal of Asian and African Studies | Nigeria | 55 | General population | 385 |
| Arabyat et al. [24] | 2023 | Research in Social and Administrative Pharmacy | Jordan | - | General population | 3116 |
| Banik et al. [25] | 2021 | BMC Infectious Diseases | Bangladesh | 66 | General population | 682 |
| Barattucci et al. [26] | 2022 | Vaccines | Italy | 84 | General population | 1095 |
| Berg and Lin [27] | 2021 | Translational Behavioral Medicine | USA | 71 | General population | 350 |
| Berni et al. [28] | 2022 | Vaccines | Morocco | 71 | General population | 3800 |
| Burke et al. [29] | 2021 | Vaccine | Australia, Canada, England, New Zealand, USA | 73 | General population | 4303 |
| Cahapay [30] | 2022 | Journal of Human Behavior in the Social Environment | Philippine | - | Teachers | 1070 |
| Caple et al. [31] | 2022 | PeerJ | Philippines | 63 | General population | 7193 |
| Chu and Liu [32] | 2021 | Patient Education and Counseling | USA | 80 | General population | 934 |
| Coe et al. [33] | 2022 | Research in Social and Administrative Pharmacy | USA | 63 | General population | 1047 |
| Duan et al. [34] | 2022 | Vaccines | China | 80 | Patients | 645 |
| Dziedzic et al. [35] | 2022 | Frontiers in Public Health | Poland | 75 | HCW | 443 |
| Ellithorpe et al. [36] | 2022 | Vaccine | USA | 60 | Parents | 682 |
| Enea et al. [37] | 2022 | Health Communication | Argentina, Australia, Brazil, Canada, Croatia, France, Germany, Greece, Hungary, Italy, Malaysia, Netherlands, Romania, Russia, South Africa, Spain, Turkey, Ukraine, UK, USA | 73 | General population | 6697 |
| Getachew et al. [38] | 2022 | Frontier in Public Health | Ethiopia | 36 | HCW | 417 |
| Getachew et al. [39] | 2023 | BMJ Open | Ethiopia | 55 | Patient | 412 |
| Ghazy et al. [40] | 2022 | IJERPH | EMR | 75 | General population | 2327 |
| Goffe et al. [41] | 2021 | HVI | UK | 62 | General population | 1660 |
| Goruntla et al. [42] | 2022 | Asian Pacific Journal of Tropical Medicine | India | 89 | General population | 2451 |
| Guidry et al. [43] | 2021 | American Journal of Infection Control | USA | 60 | General population | 788 |
| Guidry et al. [44] | 2022 | International Journal of Environmental Research and Public Health | USA | 80 | Evangelicals | 531 |
| Guillon and Kergall [45] | 2021 | Public Health | France | 31 | General population | 1146 |
| Handebo et al. [46] | 2021 | PLOS ONE | Ethiopia | 67 | Teachers | 301 |
| Hawlader et al. [47] | 2022 | International Journal of Infectious Diseases | Bangladesh, India, Pakistan, Nepal | 68 | General population | 18,201 |
| Hossian et al. [48] | 2022 | PLOS ONE | Pakistan | 73 | Students | 2865 |
| Hu et al. [49] | 2022 | Vaccines | China | 84 | General population | 898 |
| Huang et al. [50] | 2023 | Journal of Environmental and Public Health | China | 92 | General population | 525 |
| Huynh et al. [51] | 2022 | Asian Pacific Journal of Tropical Medicine | Vietnam | 76 | HCW | 410 |
| Iacob et al. [52] | 2021 | Frontiers in Psychology | Romania | 45 | General population | 864 |
| Jahanshahi-Amjazi et al. [53] | 2022 | JEHP | Iran | 72 | General population | 2365 |
| Jiang et al. [54] | 2021 | HVI | China | 72 | HCW | 1039 |
| Jin et al. [55] | 2021 | Vaccines | Pakistan | General population | 320 | |
| Kasting et al. [56] | 2022 | JMIR Public Health and Surveillance | USA | 80 | General population | 1643 |
| Khalafalla et al. [57] | 2022 | Vaccines | Saudi Arabia | 84 | General population | 1039 |
| Kabir et al. [58] | 2021 | Vaccines | Bangladesh | 69 | General population | 697 |
| Lai et al. [59] | 2021 | Vaccines | China | 85 | General population | 1145 |
| Le An et al. [60] | 2021 | HVI | Vietnam | 77 | Students | 854 |
| Le et al. [61] | 2022 | BMC Public Health | Vietnam | 58 | HCW | 911 |
| Lee et al. [62] | 2022 | JHCPF | Hong Kong | 29 | General population | 800 |
| Li, J.-B. et al. [63] | 2022 | Vaccine | Hong Kong | - | Parents | 11,141 |
| Li, G. et al. [64] | 2022 | Health Services Research and Managerial Epidemiology | Thailand | 67 | HCW | 226 |
| Liao et al. [65] | 2022 | Vaccine | Hong Kong | 61 | General population | 4055 |
| Lin et al. [66] | 2020 | PLOS Neglected Tropical Diseases | China | 83 | General population | 3541 |
| Lin et al. [5] | 2021 | HVI | China | 78 | Parents | 2026 |
| Liu et al. [67] | 2022 | IJERPH | China | 63 | General population | 3389 |
| Lopez-Cepero et al. [68] | 2021 | HVI | Puerto Rico | 83 | General population | 1911 |
| Lyons et al. [69] | 2023 | Vaccines | Trinidad | 60 | Patients | 272 |
| Mahmud et al. [70] | 2021 | Vaccines | Saudi Arabia | 58 | General population | 1387 |
| Mahmud et al. [71] | 2022 | Vaccines | Jordan | 84 | General population | 2307 |
| Maria et al. [72] | 2022 | Vaccines | Indonesia | 89 | HCW | 1684 |
| Mercadante and Law [73] | 2021 | Research in Social and Administrative Pharmacy | USA | 67 | General population | 525 |
| Miyachi et al. [74] | 2022 | Vaccines | Japan | 91 | Students | 1776 |
| Mohammed et al. [75] | 2022 | Vaccine | Iraq, Jordan, UAE, Oman, Yemen | 56 | Parents | 1154 |
| Morar et al. [76] | 2022 | IJERPH | Romania | 51 | General population | 110 |
| Nguyen et al. [77] | 2021 | Risk Management and Healthcare Policy | Vietnam | 78 | Students | 412 |
| Okai and Abekah-Nkrumah [78] | 2022 | PLOS ONE | Ghana | 63 | General population | 362 |
| Okmi et al. [79] | 2022 | Cureus | Saudi Arabia | 73 | General population | 1939 |
| Okuyan et al. [80] | 2021 | International Journal of Clinical Pharmacy | Turkey | 75 | HCW | 961 |
| Otiti-Sengeri et al. [81] | 2022 | Vaccines | Uganda | 98 | HCW | 300 |
| Patwary et al. [82] | 2021 | Vaccines | Bangladesh | 85 | General population | 543 |
| Qin et al. [83] | 2022a | Vaccines | China | 94 | General population | 3119 |
| Qin et al. [84] | 2022b | Frontiers in Public Health | China | 88 | Parents | 1724 |
| Qin et al. [85] | 2022c | Frontiers in Public Health | China | 83 | 60 or older | 3321 |
| Qin et al. [86] | 2023 | HVI | China | 81 | General population | 3224 |
| Quinto et al. [87] | 2021 | Philippine Journal of Health Research and Development | Philippine | 93 | Teachers | 707 |
| Rabin and Durta [88] | 2021 | Psychology, Health & Medicine | USA | 76 | General population | 186 |
| Reindl and Catma [89] | 2022 | Expert Review of Pharmacoeconomics & Outcomes Research | USA | 66 | Parents | 30 |
| Reiter et al. [90] | 2020 | Vaccine | USA | 69 | General population | 2006 |
| Rosental and Shmueli [91] | 2021 | Vaccines | Israel | 82 | Students | 628 |
| Rountree and Prentice [92] | 2022 | Irish Journal of Medical Science | Ireland | 32 | General population | 1995 |
| Seangpraw et al. [93] | 2022 | Frontiers in Medicine | Thailand | General population | 1024 | |
| Seboka et al. [94] | 2021 | Risk Management and Healthcare Policy | Ethiopia | 65 | General population | 1160 |
| Shah et al. [95] | 2022 | Vaccine | Singapore | - | General population | 1009 |
| Shmueli [96] | 2021 | BMC Public Health | Israel | 80 | General population | 398 |
| Shmueli [97] | 2022 | Vaccines | Israel | 65 | General population | 461 |
| Short et al. [98] | 2022 | Families, Systems and Health | USA | 37 | Students | 526 |
| Sieverding et al. [99] | 2023 | Psychology, Health & Medicine | UK and Germany | 88 | General population | 1425 |
| Spinewine et al. [100] | 2021 | Vaccines | Belgium | 58 | General population | 1132 |
| Ştefănuţ et al. [101] | 2021 | Frontiers in Psychology | Romania | 45 | Students | 432 |
| Su et al. [102] | 2022 | Frontiers in Psychology | China | 73 | General population | 557 |
| Suess et al. [103] | 2022 | Tourism Management | USA | 71 | Travelers | 1478 |
| Tran et al. [104] | 2021 | Pharmacy Practice | Russia | 42 | General population | 876 |
| Ung et al. [105] | 2022 | BMC Infectious Diseases | Macao | 62 | General population | 552 |
| Vatcharavongvan et al. [106] | 2023 | Vaccine | Thailand | 90 | Parents | 1056 |
| Wagner et al. [107] | 2022 | Vaccines | USA | 38 | General population | 1012 |
| Walker et al. [108] | 2021 | Vaccines | China | 36 | Students | 330 |
| Wang [109] | 2022 | Health Communication | China | 80 | General population | 460 |
| Wang et al. [110] | 2021 | HVI | China | 64 | Students | 833 |
| Wijesinghe et al. [111] | 2021 | Asia Pacific Journal of Public Health | Sri Lanka | 54 | General population | 895 |
| Wirawan et al. [112] | 2022 | Vaccines | Indonesia | 56 | General population | 2674 |
| Wong et al. [113] | 2020 | HVI | Malaysia | 94 | General population | 1159 |
| Xiao et al. [114] | 2021 | Vaccines | China | 56 | General population | 2528 |
| Yan et al. [115] | 2021 | Vaccines | Hong Kong | 42 | General population | 1255 |
| Yang et al. [116] | 2022 | IJERPH | China | 82 | General population | 621 |
| Youssef et al. [117] | 2022 | PLOS ONE | Lebanon | 58 | HCW | 1800 |
| Yu et al. [118] | 2021 | HVI | China | 72 | HCW | 2254 |
| Zakeri et al. [119] | 2021 | Journal of Pharmaceutical Health Services Research | USA | 62 | Parents | 595 |
| Zampetakis and Melas [120] | 2021 | Appl Psychol Health Well-Being | Greece | 44 | Employees | 1165 |
| Zhang et al. [121] | 2023 | Vaccines | China | 86 | General population | 1472 |
| Zhelyazkova et al. [122] | 2022 | Vaccines | Germany | 84 | HCW | 2555 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Limbu, Y.B.; Gautam, R.K. How Well the Constructs of Health Belief Model Predict Vaccination Intention: A Systematic Review on COVID-19 Primary Series and Booster Vaccines. Vaccines 2023, 11, 816. https://doi.org/10.3390/vaccines11040816
Limbu YB, Gautam RK. How Well the Constructs of Health Belief Model Predict Vaccination Intention: A Systematic Review on COVID-19 Primary Series and Booster Vaccines. Vaccines. 2023; 11(4):816. https://doi.org/10.3390/vaccines11040816
Chicago/Turabian StyleLimbu, Yam B., and Rajesh K. Gautam. 2023. "How Well the Constructs of Health Belief Model Predict Vaccination Intention: A Systematic Review on COVID-19 Primary Series and Booster Vaccines" Vaccines 11, no. 4: 816. https://doi.org/10.3390/vaccines11040816