

Correlation between CD4 T-Cell Counts and Seroconversion among COVID-19 Vaccinated Patients with HIV: A Meta-Analysis
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Quality Assessment
2.4. Definitions of Vaccines
2.5. Statistical Analysis
3. Results
3.1. Study Selection, Characteristics and Quality Assessment
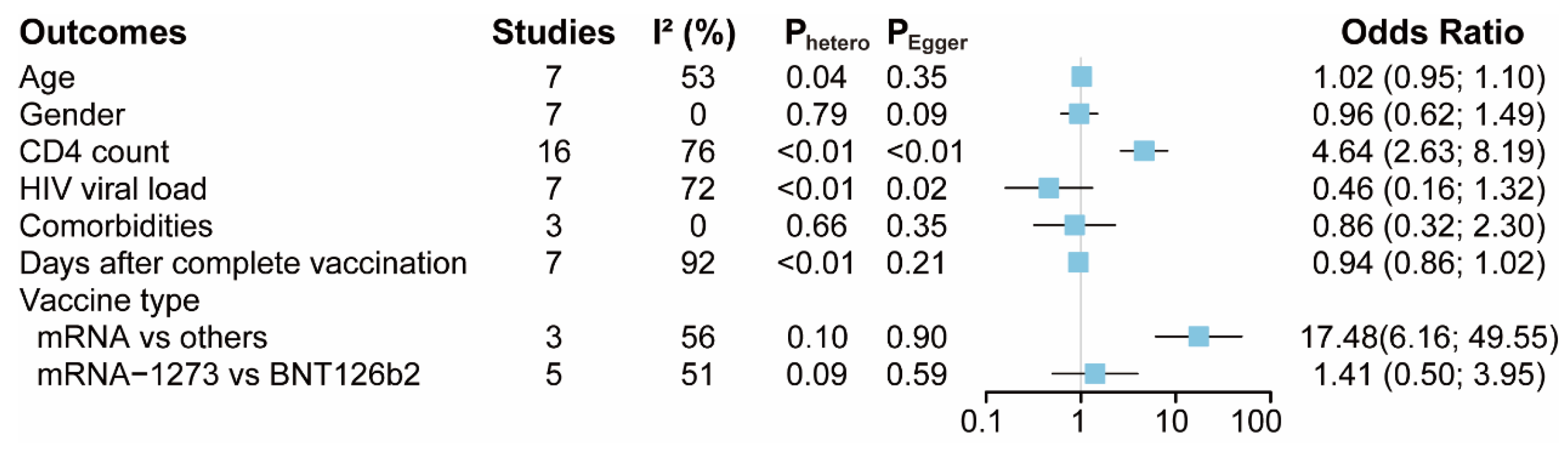
3.2. Risk Factors for Seroconversion Rate in PLWH
3.3. Publication Bias
3.4. Meta-Regression and Subgroup Analysis
3.5. Sensitivity Analysis
3.6. Grading the Quality of Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Geretti, A.M.; Stockdale, A.J.; Kelly, S.H.; Cevik, M.; Collins, S.; Waters, L.; Villa, G.; Docherty, A.; Harrison, E.M.; Turtle, L.; et al. Outcomes of Coronavirus Disease 2019 (COVID-19) Related Hospitalization Among People With Human Immunodeficiency Virus (HIV) in the ISARIC World Health Organization (WHO) Clinical Characterization Protocol (UK): A Prospective Observational Study. Clin. Infect. Dis. 2021, 73, e2095–e2106. [Google Scholar] [CrossRef] [PubMed]
- Western Cape Department of Health in collaboration with the National Institute for Communicable Diseases, South Africa. Risk Factors for Coronavirus Disease 2019 (COVID-19) Death in a Population Cohort Study from the Western Cape Province, South Africa. Clin. Infect. Dis. 2021, 73, e2005–e2015. [Google Scholar] [CrossRef] [PubMed]
- Bhaskaran, K.; Rentsch, C.T.; MacKenna, B.; Schultze, A.; Mehrkar, A.; Bates, C.J.; Eggo, R.M.; Morton, C.E.; Bacon, S.C.J.; Inglesby, P.; et al. HIV infection and COVID-19 death: A population-based cohort analysis of UK primary care data and linked national death registrations within the OpenSAFELY platform. Lancet HIV 2021, 8, e24–e32. [Google Scholar] [CrossRef]
- Tesoriero, J.M.; Swain, C.-A.E.; Pierce, J.L.; Zamboni, L.; Wu, M.; Holtgrave, D.R.; Gonzalez, C.J.; Udo, T.; Morne, J.E.; Hart-Malloy, R.; et al. COVID-19 Outcomes Among Persons Living With or Without Diagnosed HIV Infection in New York State. JAMA Netw. Open 2021, 4, e2037069. [Google Scholar] [CrossRef]
- Balcells, M.E.; Le Corre, N.; Durán, J.; Ceballos, M.E.; Vizcaya, C.; Mondaca, S.; Dib, M.; Rabagliati, R.; Sarmiento, M.; Burgos, P.I.; et al. Reduced Immune Response to Inactivated Severe Acute Respiratory Syndrome Coronavirus 2 Vaccine in a Cohort of Immunocompromised Patients in Chile. Clin. Infect. Dis. 2022, 75, e594–e602. [Google Scholar] [CrossRef]
- Huang, X.; Yan, Y.; Su, B.; Xiao, D.; Yu, M.; Jin, X.; Duan, J.; Zhang, X.; Zheng, S.; Fang, Y.; et al. Comparing Immune Responses to Inactivated Vaccines against SARS-CoV-2 between People Living with HIV and HIV-Negative Individuals: A Cross-Sectional Study in China. Viruses 2022, 14, 277. [Google Scholar] [CrossRef]
- Yan, Y.; Davgadorj, C.; Lyu, C.; Zhang, S.; Qiu, Y. Immunogenicity of a third dose of inactivated COVID-19 vaccine in people living with HIV-1, HBV, and tuberculosis during the Omicron variant epidemic: A cross-sectional study. J. Infect. 2022, 85, e109–e111. [Google Scholar] [CrossRef]
- Chan, D.P.C.; Wong, N.S.; Wong, B.C.; Chan, J.M.; Lee, S.S. Three-Dose Primary Series of Inactivated COVID-19 Vaccine for Persons Living with HIV, Hong Kong. Emerg. Infect. Dis. 2022, 28, 2130–2132. [Google Scholar] [CrossRef]
- Hafiz, I.; Illian, D.N.; Meila, O.; Utomo, A.R.H.; Susilowati, A.; Susetya, I.E.; Desrita, D.; Siregar, G.A.; Basyuni, M. Effectiveness and Efficacy of Vaccine on Mutated SARS-CoV-2 Virus and Post Vaccination Surveillance: A Narrative Review. Vaccines 2022, 10, 82. [Google Scholar] [CrossRef]
- Hasan, T.; Beardsley, J.; Marais, B.; Nguyen, T.; Fox, G. The Implementation of Mass-Vaccination against SARS-CoV-2: A Systematic Review of Existing Strategies and Guidelines. Vaccines 2021, 9, 326. [Google Scholar] [CrossRef]
- Petráš, M.; Máčalík, R.; Janovská, D.; Čelko, A.M.; Dáňová, J.; Selinger, E.; Doleček, J.; Neradová, S.; Franklová, M.; Dlouhý, P.; et al. Risk factors affecting COVID-19 vaccine effectiveness identified from 290 cross-country observational studies until February 2022: A meta-analysis and meta-regression. BMC Med. 2022, 20, 461. [Google Scholar] [CrossRef]
- Corma-Gómez, A.; Fernández-Fuertes, M.; García, E.; Fuentes-López, A.; Gómez-Ayerbe, C.; Rivero-Juárez, A.; Domínguez, C.; Santos, M.; Viñuela, L.; Palacios, R.; et al. Severe immunosuppression is related to poorer immunogenicity to SARS-CoV-2 vaccines among people living with HIV. Clin. Microbiol. Infect. 2022, 28, 1492–1498. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Dekkers, O.M.; Egger, M.; Altman, D.G.; Vandenbroucke, J.P. Distinguishing Case Series From Cohort Studies. Ann. Intern. Med. 2012, 156, 37–40. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Ziff, M.; Lane, D.A.; Samra, M.; Griffith, M.; Kirchhof, P.; Lip, G.Y.H.; Steeds, R.; Townend, J.; Kotecha, D. Safety and efficacy of digoxin: Systematic review and meta-analysis of observational and controlled trial data. BMJ 2015, 351, h4451. [Google Scholar] [CrossRef] [Green Version]
- Antinori, A.; Cicalini, S.; Meschi, S.; Bordoni, V.; Lorenzini, P.; Vergori, A.; Lanini, S.; De Pascale, L.; Matusali, G.; Mariotti, D.; et al. Humoral and Cellular Immune Response Elicited by mRNA Vaccination Against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in People Living With Human Immunodeficiency Virus Receiving Antiretroviral Therapy Based on Current CD4 T-Lymphocyte Count. Clin. Infect. Dis. 2022, 75, e552–e563. [Google Scholar] [CrossRef]
- Ao, L.; Lu, T.; Cao, Y.; Chen, Z.; Wang, Y.; Li, Z.; Ren, X.; Xu, P.; Peng, M.; Chen, M.; et al. Safety and immunogenicity of inactivated SARS-CoV-2 vaccines in people living with HIV. Emerg. Microbes Infect. 2022, 11, 1126–1134. [Google Scholar] [CrossRef]
- Bergman, P.; Blennow, O.; Hansson, L.; Mielke, S.; Nowak, P.; Chen, P.; Söderdahl, G.; Österborg, A.; Smith, C.I.E.; Wullimann, D.; et al. Safety and efficacy of the mRNA BNT162b2 vaccine against SARS-CoV-2 in five groups of immunocompromised patients and healthy controls in a prospective open-label clinical trial. Ebiomedicine 2021, 74, 103705. [Google Scholar] [CrossRef] [PubMed]
- Brumme, Z.L.; Mwimanzi, F.; Lapointe, H.R.; Cheung, P.K.; Sang, Y.; Duncan, M.C.; Yaseen, F.; Agafitei, O.; Ennis, S.; Ng, K.; et al. Humoral immune responses to COVID-19 vaccination in people living with HIV receiving suppressive antiretroviral therapy. Npj Vaccines 2022, 7, 28. [Google Scholar] [CrossRef] [PubMed]
- Gianserra, L.; Donà, M.G.; Giuliani, E.; Stingone, C.; Pontone, M.; Buonomini, A.R.; Giuliani, M.; Pimpinelli, F.; Morrone, A.; Latini, A. Immunogenicity and Safety of BNT162b2 Homologous Booster Vaccination in People Living with HIV under Effective cART. Vaccines 2022, 10, 1243. [Google Scholar] [CrossRef] [PubMed]
- Haidar, G.; Agha, M.; Bilderback, A.; Lukanski, A.; Linstrum, K.; Troyan, R.; Rothenberger, S.; McMahon, D.K.; Crandall, M.D.; Sobolewksi, M.D.; et al. Prospective Evaluation of Coronavirus Disease 2019 (COVID-19) Vaccine Responses Across a Broad Spectrum of Immunocompromising Conditions: The COVID-19 Vaccination in the Immunocompromised Study (COVICS). Clin. Infect. Dis. 2022, 75, e630–e644. [Google Scholar] [CrossRef]
- Han, X.; Yu, X.; Han, Y.; Fang, Q.; Shen, C.; Liu, H.; Wang, P.; Wang, Y.; Li, X. Safety and Immunogenicity of Inactivated COVID-19 Vaccines Among People Living with HIV in China. Infect. Drug Resist. 2022, 15, 2091–2100. [Google Scholar] [CrossRef]
- Hassold, N.; Brichler, S.; Ouedraogo, E.; Leclerc, D.; Carroue, S.; Gater, Y.; Alloui, C.; Carbonnelle, E.; Bouchaud, O.; Mechai, F.; et al. Impaired antibody response to COVID-19 vaccination in advanced HIV infection. AIDS 2022, 36, F1–F5. [Google Scholar] [CrossRef]
- Hensley, K.S.; Jongkees, M.J.; Geers, D.; GeurtsvanKessel, C.H.; Mueller, Y.M.; Dalm, V.A.S.H.; Papageorgiou, G.; Steggink, H.; Gorska, A.; Bogers, S.; et al. Immunogenicity and reactogenicity of SARS-CoV-2 vaccines in people living with HIV in The Netherlands: A nationwide prospective cohort study. PLoS Med. 2023, 20, e1004159. [Google Scholar] [CrossRef]
- Khan, K.; Lustig, G.; Bernstein, M.; Archary, D.; Cele, S.; Karim, F.; Smith, M.; Ganga, Y.; Jule, Z.; Reedoy, K.; et al. Immunogenicity of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection and Ad26.CoV2.S Vaccination in People Living With Human Immunodeficiency Virus (HIV). Clin. Infect. Dis. 2022, 75, e857–e864. [Google Scholar] [CrossRef]
- Milano, E.; Ricciardi, A.; Casciaro, R.; Pallara, E.; De Vita, E.; Bavaro, D.F.; Larocca, A.M.V.; Stefanizzi, P.; Tafuri, S.; Saracino, A. Immunogenicity and safety of the BNT162b2 COVID-19 mRNA vaccine in PLWH: A monocentric study in Bari, Italy. J. Med. Virol. 2022, 94, 2230–2236. [Google Scholar] [CrossRef]
- Nault, L.; Marchitto, L.; Goyette, G.; Tremblay-Sher, D.; Fortin, C.; Martel-Laferrière, V.; Trottier, B.; Richard, J.; Durand, M.; Kaufmann, D.; et al. Covid-19 vaccine immunogenicity in people living with HIV-1. Vaccine 2022, 40, 3633–3637. [Google Scholar] [CrossRef]
- Netto, L.C.; Ibrahim, K.Y.; Picone, C.M.; Alves, A.P.P.S.; Aniceto, E.V.; Santiago, M.R.; Parmejani, P.S.S.; Aikawa, N.E.; Medeiros-Ribeiro, A.C.; Pasoto, S.G.; et al. Safety and immunogenicity of CoronaVac in people living with HIV: A prospective cohort study. Lancet HIV 2022, 9, e323–e331. [Google Scholar] [CrossRef]
- Polvere, J.; Fabbiani, M.; Pastore, G.; Rancan, I.; Rossetti, B.; Durante, M.; Zirpoli, S.; Morelli, E.; Pettini, E.; Lucchesi, S.; et al. B cell response six months after SARS-CoV-2 mRNA vaccination in people living with HIV. Commun. Med. 2022, 3, 13. [Google Scholar] [CrossRef]
- Speich, B.; Chammartin, F.; Abela, I.A.; Amico, P.; Stoeckle, M.P.; Eichenberger, A.L.; Hasse, B.; Braun, D.L.; Schuurmans, M.M.; Müller, T.F.; et al. Antibody Response in Immunocompromised Patients After the Administration of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccine BNT162b2 or mRNA-1273: A Randomized Controlled Trial. Clin. Infect. Dis. 2022, 75, e585–e593. [Google Scholar] [CrossRef]
- Spinelli, M.A.; Peluso, M.J.; Lynch, K.L.; Yun, C.; Glidden, D.V.; Henrich, T.J.; Deeks, S.G.; Gandhi, M. Differences in Post-mRNA Vaccination Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Immunoglobulin G (IgG) Concentrations and Surrogate Virus Neutralization Test Response by Human Immunodeficiency Virus (HIV) Status and Type of Vaccine: A Matched Case-Control Observational Study. Clin. Infect. Dis. 2022, 75, e916–e919. [Google Scholar] [CrossRef]
- Tuan, J.J.; Zapata, H.; Critch-Gilfillan, T.; Ryall, L.; Turcotte, B.; Mutic, S.; Andrews, L.; Roh, M.E.; Friedland, G.; Barakat, L.; et al. Qualitative assessment of anti-SARS-CoV-2 spike protein immunogenicity (QUASI) after COVID-19 vaccination in older people living with HIV. HIV Med. 2022, 23, 178–185. [Google Scholar] [CrossRef]
- Vergori, A.; Cozzi-Lepri, A.; Matusali, G.; Colavita, F.; Cicalini, S.; Gallì, P.; Garbuglia, A.R.; Fusto, M.; Puro, V.; Maggi, F.; et al. SARS-CoV-2 Omicron Variant Neutralization after Third Dose Vaccination in PLWH. Viruses 2022, 14, 1710. [Google Scholar] [CrossRef]
- Wong, N.S.; Wong, B.C.K.; Chan, J.M.C.; Wong, K.H.; Tsang, O.T.Y.; Mok, C.K.P.; Hui, D.S.C.; Lee, S.S.; Chan, D.P.C. Surrogate neutralization responses following severe acute respiratory syndrome coronavirus 2 vaccination in people with HIV: Comparison between inactivated and mRNA vaccine. AIDS 2022, 36, 1255–1264. [Google Scholar] [CrossRef]
- Xu, X.; Vesterbacka, J.; Aleman, S.; Nowak, P. High seroconversion rate after vaccination with mRNA BNT162b2 vaccine against SARS-CoV-2 among people with HIV-but HIV viremia matters? AIDS 2022, 36, 479–481. [Google Scholar] [CrossRef]
- Zeng, G.; Xu, L.; Feng, S.; Tang, J.; Wang, X.; Li, G.; Gan, Y.; Zheng, C.; Zhao, J.; Yang, Z. IgG Antibody Responses and Immune Persistence of Two Doses of BBIBP-CorV Vaccine or CoronaVac Vaccine in People Living with HIV (PLWH) in Shenzhen, China. Vaccines 2022, 10, 880. [Google Scholar] [CrossRef]
- Zou, S.; Wu, M.; Ming, F.; Wu, S.; Guo, W.; Marley, G.; Xing, Z.; Zhang, Z.; Zeng, M.; Sun, C.; et al. Immune response and safety to inactivated COVID-19 vaccine: A comparison between people living with HIV and HIV-naive individuals. AIDS Res. Ther. 2022, 19, 33. [Google Scholar] [CrossRef]
- Catherine, F.-X.; Piroth, L. Hepatitis B virus vaccination in HIV-infected people: A review. Hum. Vaccines Immunother. 2017, 13, 1304–1313. [Google Scholar] [CrossRef] [PubMed]
- Pallikkuth, S.; De Armas, L.R.; Pahwa, R.; Rinaldi, S.; George, V.K.; Sanchez, C.M.; Pan, L.; Dickinson, G.; Rodriguez, A.; Fischl, M.; et al. Impact of aging and HIV infection on serologic response to seasonal influenza vaccination. AIDS 2018, 32, 1085–1094. [Google Scholar] [CrossRef] [PubMed]
- Grohskopf, L.A.; Alyanak, E.; Broder, K.R.; Walter, E.B.; Fry, A.M.; Jernigan, D.B. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices—United States, 2019–2020 Influenza Season. MMWR. Recomm. Rep. 2019, 68, 1–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nejad, M.-M.M.; Shobeiri, P.; Dehghanbanadaki, H.; Tabary, M.; Aryannejad, A.; Ghadery, A.H.; Shabani, M.; Moosaie, F.; SeyedAlinaghi, S.; Rezaei, N. Seroconversion following the first, second, and third dose of SARS-CoV-2 vaccines in immunocompromised population: A systematic review and meta-analysis. Virol. J. 2022, 19, 132. [Google Scholar] [CrossRef]
- Yin, J.; Chen, Y.; Li, Y.; Wang, C.; Zhang, X. Immunogenicity and efficacy of COVID-19 vaccines in people living with HIV: A systematic review and meta-analysis. Int. J. Infect. Dis. 2022, 124, 212–223. [Google Scholar] [CrossRef]
- Kang, L.; Shang, W.; Gao, P.; Wang, Y.; Liu, J.; Liu, M. Immunogenicity and Safety of COVID-19 Vaccines among People Living with HIV: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1569. [Google Scholar] [CrossRef]
- Zotos, D.; Coquet, J.M.; Zhang, Y.; Light, A.; D’Costa, K.; Kallies, A.; Corcoran, L.M.; Godfrey, D.I.; Toellner, K.-M.; Smyth, M.J.; et al. IL-21 regulates germinal center B cell differentiation and proliferation through a B cell–intrinsic mechanism. J. Exp. Med. 2010, 207, 365–378. [Google Scholar] [CrossRef] [Green Version]
- Ruddy, J.A.; Boyarsky, B.J.; Werbel, W.A.; Bailey, J.R.; Karaba, A.H.; Garonzik-Wang, J.M.; Segev, D.L.; Durand, C.M. Safety and antibody response to the first dose of severe acute respiratory syndrome coronavirus 2 messenger RNA vaccine in persons with HIV. AIDS 2021, 35, 1872–1874. [Google Scholar] [CrossRef]
- Avelino-Silva, V.I.; Miyaji, K.T.; Hunt, P.W.; Huang, Y.; Simoes, M.; Lima, S.B.; Freire, M.S.; Caiaffa-Filho, H.H.; Hong, M.A.; Costa, D.A.; et al. CD4/CD8 Ratio and KT Ratio Predict Yellow Fever Vaccine Immunogenicity in HIV-Infected Patients. PLoS Negl. Trop. Dis. 2016, 10, e0005219. [Google Scholar] [CrossRef] [Green Version]
- Parmigiani, A.; Alcaide, M.L.; Freguja, R.; Pallikkuth, S.; Frasca, D.; Fischl, M.A.; Pahwa, S. Impaired Antibody Response to Influenza Vaccine in HIV-Infected and Uninfected Aging Women Is Associated with Immune Activation and Inflammation. PLoS ONE 2013, 8, e79816. [Google Scholar] [CrossRef]
- Heftdal, L.D.; Knudsen, A.D.; Hamm, S.R.; Hansen, C.B.; Møller, D.L.; Pries-Heje, M.; Fogh, K.; Hasselbalch, R.B.; Jarlhelt, I.; Pérez-Alós, L.; et al. Humoral response to two doses of BNT162b2 vaccination in people with HIV. J. Intern. Med. 2022, 291, 513–518. [Google Scholar] [CrossRef]
- Fedele, G.; Trentini, F.; Schiavoni, I.; Abrignani, S.; Antonelli, G.; Baldo, V.; Baldovin, T.; Bandera, A.; Bonura, F.; Clerici, P.; et al. Evaluation of humoral and cellular response to four vaccines against COVID-19 in different age groups: A longitudinal study. Front. Immunol. 2022, 13, 1021396. [Google Scholar] [CrossRef]
- Maringer, Y.; Nelde, A.; Schroeder, S.M.; Schuhmacher, J.; Hörber, S.; Peter, A.; Karbach, J.; Jäger, E.; Walz, J.S. Durable spike-specific T cell responses after different COVID-19 vaccination regimens are not further enhanced by booster vaccination. Sci. Immunol. 2022, 7, 78. [Google Scholar] [CrossRef]
- Kwok, S.L.; Cheng, S.M.; Leung, J.N.; Leung, K.; Lee, C.-K.; Peiris, J.M.; Wu, J.T. Waning antibody levels after COVID-19 vaccination with mRNA Comirnaty and inactivated CoronaVac vaccines in blood donors, Hong Kong, April 2020 to October 2021. Eurosurveillance 2022, 27, 2101197. [Google Scholar] [CrossRef]
- Peng, Q.; Zhou, R.; Wang, Y.; Zhao, M.; Liu, N.; Li, S.; Huang, H.; Yang, D.; Au, K.-K.; Wang, H.; et al. Waning immune responses against SARS-CoV-2 variants of concern among vaccinees in Hong Kong. Ebiomedicine 2022, 77, 103904. [Google Scholar] [CrossRef]
- Lim, W.W.; Mak, L.; Leung, G.M.; Cowling, B.J.; Peiris, M. Comparative immunogenicity of mRNA and inactivated vaccines against COVID-19. Lancet Microbe 2021, 2, e423. [Google Scholar] [CrossRef]
- Chen, Y.; Shen, H.; Huang, R.; Tong, X.; Wu, C. Serum neutralising activity against SARS-CoV-2 variants elicited by CoronaVac. Lancet Infect. Dis. 2021, 21, 1071–1072. [Google Scholar] [CrossRef]
- Ben Ahmed, M.; Bellali, H.; Gdoura, M.; Zamali, I.; Kallala, O.; Ben Hmid, A.; Hamdi, W.; Ayari, H.; Fares, H.; Mechri, K.; et al. Humoral and Cellular Immunogenicity of Six Different Vaccines against SARS-CoV-2 in Adults: A Comparative Study in Tunisia (North Africa). Vaccines 2022, 10, 1189. [Google Scholar] [CrossRef]
- Wei, J.; Zhang, W.; Doherty, M.; Wallace, Z.S.; Sparks, J.A.; Lu, N.; Li, X.; Zeng, C.; Lei, G. Comparative effectiveness of BNT162b2 and ChAdOx1 nCoV-19 vaccines against COVID-19. BMC Med. 2023, 21, 78. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Source | Country | Design | Data Source | Cases | Vaccine Type | Vaccine Dose | COVID-19 History | Outcomes | Multivariable Analysis | Impact Factors | Adjust |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Anais 2022 [13] | Spain | Pro | Three university hospitals in Southern Spain | 420 | BNT162b2, mRNA-1273, ChAdOx1 nCoV-19, or Ad26.COV2.S | Complete | NO | anti-S IgG | YES | Age, gender, HIV infection way, CDC clinical category nadir CD4 T-cell counts, Charlson index, cirrhosis, chronic kidney disease, immunosuppressive therapy, CD4 T-cell counts (cutoff = 200 cell/mm3), HIV viral load, vaccine | - |
| Antinori 2022 [19] | Italy | Pro | National Institute for Infectious Diseases Lazzaro Spallanzani | 153 | BNT162b2 or mRNA-1273 | Complete | NO | nAbs | NO | CD4 T-cell counts (cutoff = 200 cell/mm3) | - |
| Ao 2022 [20] | China | Pro | People’s Hospital of Tongliang District | 139 | BBIBP-CorV or Corona Vac | Complete | NO | anti-RBD IgG | YES | Age, gender, days after 2nd vaccination, CD4 T-cell counts (cutoff = 500 cell/mm3), HIV viral load, white blood cell count, lymphocyte count, platelet count, alanine aminotransferase, aspartate aminotransferase, B cells, RBD-specific B cells, RBD-specific MBCs, RBD+ rMBCs, RBD+ actMBCs, RBD+ atyMBCs, RBD+ intMBCs | - |
| Bergman 2021 [21] | Sweden | Pro | Karolinska University Hospital | 79 | BNT162b2 | Complete | NO | anti-RBD IgG | NO | CD4 T-cell counts (cutoff = 300 cell/mm3) | Age (partially) |
| Brumme 2022 [22] | Canada | Retro | Three HIV care clinics in | 100 | BNT162b2, mRNA-1273 or ChAdOx1 | Complete | YES | anti-RBD IgG | NO | Days after 2nd vaccination | Age, chronic health conditions |
| Gianserra 2022 [23] | Italy | Pro | HIV/AIDS Unit of the San Gallicano Dermatological Institute | 42 | BNT162b2 | Complete | NO | SARS-CoV-2 S1/S2 IgG | NO | Days after second vaccination | - |
| Haidar 2022 [24] | USA | Pro | Unive University of Pittsburgh Medical Center Health System | 94 | BNT162b2, mRNA-1273 or Adenovirus | Complete | NO | anti-RBD IgG | NO, except for days after 2nd dose | Age, gender, race, vaccine, days after second dose | - |
| Han 2022 [25] | China | Retro | Beijing Ditan Hospital | 47 | CoronaVac or Sinopharm | Complete | NO | nAbs | NO | CD4 T-cell counts (cutoff = 350 cell/mm3) | Age, sex, and interval length |
| Hassold 2022 [26] | France | Retro | Department of Infectious Diseases of Hospital Avicenne | 105 | BNT162b2, mRNA-1273 or ChAdOx1-nCoV-19 | Complete | NO | Anti-spike IgG | NO | CD4 T-cell counts (cutoff = 200 cell/mm3) | - |
| Hensley 2022 [27] | Netherlands | Pro | 22 HIV treatment centers | 1154 | BNT162b2, mRNA-1273, ChAdOx1-S or Ad26.COV2.S | Complete | NO | Anti-spike IgG | YES, except for vaccine type | Vaccine type, age, gender, HIV viral load, CD4 T-cell counts (cutoff = 250 cell/mm3), CD4 nadir cell counts | - |
| Khan 2022 [28] | South African | Pro | Biomedical Research of the University of KwaZulu–Natal | 26 | Ad26.CoV2.S | Complete | YES | Neutralization capacity | NO | HIV viral load | - |
| Milano 2022 [29] | Italy | Pro | University of Bari | 578 | BNT162b2 | Complete | NO | Anti-RBD IgG | NO | Days after complete vaccination | - |
| Nault 2022 [30] | Canada | Retro | HIV clinics in Montreal | 106 | mRNA-1273 | Uncomplete | YES | Anti-RBD IgG | NO | CD4 T-cell counts (cutoff = 250 cell/mm3) | - |
| Netto 2022 [31] | Brazil | Pro | University of Sao Paulo HIV/AIDS outpatient clinic | 215 | CoronaVac | Complete | NO | nAbs | NO | CD4 T-cell counts (cutoff = 500 cell/mm3) | - |
| Polvere 2022 [32] | Italy | Retro | Azienda Ospedaliera Universitaria Senese | 84 | BNT162b2 or mRNA-1273 | Complete | NO | nAbs | NO | Age, gender, vaccine type, BMI, IDU, years from HIV infection, CDC stage, HBV or HCV coinfection, zenith HIV-RNA, CD4 T-cell counts at nadir, years from first ART, type of ART, HIV viral load, time from last HIV-RNA >50 copies/mL, CD4 T-cell counts at baseline (cutoff = 350 cell/mm3), CD4%, CD4/CD8 ratio | - |
| Speich 2022 [33] | Switzerland | RCT | University Hospital Basel, University Hospital Bern and University Hospital Zurich | 341 | BNT162b2 or mRNA-1273 | Complete | YES | nAbs | NO | Vaccine type | RCT |
| Spinelli 2022 [34] | USA | Retro | A large outpatient HIV clinic | 100 | BNT162b2 or mRNA-1273 | Complete | NO | nAbs | YES | CD4 T-cell counts (cutoff = NA), HIV viral load, vaccine type | Care for chronic medical conditions on days since completion of second vaccination (minimum 10), sex, age and mRNA vaccine type |
| Tuan 2022 [35] | USA | Retro | Two HIV clinics of the Yale New Haven Health System | 78 | BNT162b2 | Uncomplete | NO | IgG | NO, except for CD4 T-cell counts | Age, gender, days after second vaccination, BMI, self-reported substance use, time since HIV diagnosis, HIV ART regimen, CD4 T-cell counts (cutoff = 500 cell/mm3), HIV viral load, comorbidities | - |
| Vergori 2022 [36] | Italy | Retro | Infectious Diseases Lazzaro Spallanzani in Rome | 106 | BNT162b2 or Mrna-1273 | Booster | NO | nAbs | NO | CD4 T-cell counts (cutoff = 200 cell/mm3), CD4 T-cell counts at nadir | - |
| Wong 2022 [37] | China | Pro | The Integrated Treatment Centre or Princess Margaret Hospital HIV Service | 213 | CoronaVac or Comirnaty | Complete | NO | nAbs | NO | Vaccine type | age, sex, CD4 T-cell counts, and suppressed viral load (SVL) at the time point nearest to vaccination. |
| Xu 2022 [38] | Sweden | Pro | Karolinska University Hospital | 79 | BNT162b2 | Complete | NO | anti-spike-IgG | NO | CD4 T-cell counts (cutoff = 200 cell/mm3) | - |
| Zeng 2022 [39] | China | Retro | The Third People’s Hospital of Shenzhen | 126 | BBIBP-CorV or CoronaVac | Complete | NO | anti-RBD IgG | NO | CD4 T-cell counts (cutoff = 350 cell/mm3), days after complete vaccination, vaccine type | - |
| Zou 2022 [40] | China | Pro | Wuchang district of Wuhan city | 46 | Sinopharm WIBP-CorV | Complete | NO | nAbs and IgG | YES, except for days after 2nd dose | Age, gender, CD4 T-cell counts (cutoff = NA), days after second dose | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, Q.; Liu, Y.; Zeng, F.; Meng, Y.; Liu, H.; Deng, G. Correlation between CD4 T-Cell Counts and Seroconversion among COVID-19 Vaccinated Patients with HIV: A Meta-Analysis. Vaccines 2023, 11, 789. https://doi.org/10.3390/vaccines11040789
Zhou Q, Liu Y, Zeng F, Meng Y, Liu H, Deng G. Correlation between CD4 T-Cell Counts and Seroconversion among COVID-19 Vaccinated Patients with HIV: A Meta-Analysis. Vaccines. 2023; 11(4):789. https://doi.org/10.3390/vaccines11040789
Chicago/Turabian StyleZhou, Qian, Yihuang Liu, Furong Zeng, Yu Meng, Hong Liu, and Guangtong Deng. 2023. "Correlation between CD4 T-Cell Counts and Seroconversion among COVID-19 Vaccinated Patients with HIV: A Meta-Analysis" Vaccines 11, no. 4: 789. https://doi.org/10.3390/vaccines11040789