

Effects of Vaccine Literacy, Health Beliefs, and Flu Vaccination on Perceived Physical Health Status among Under/Graduate Students

Abstract
:1. Introduction
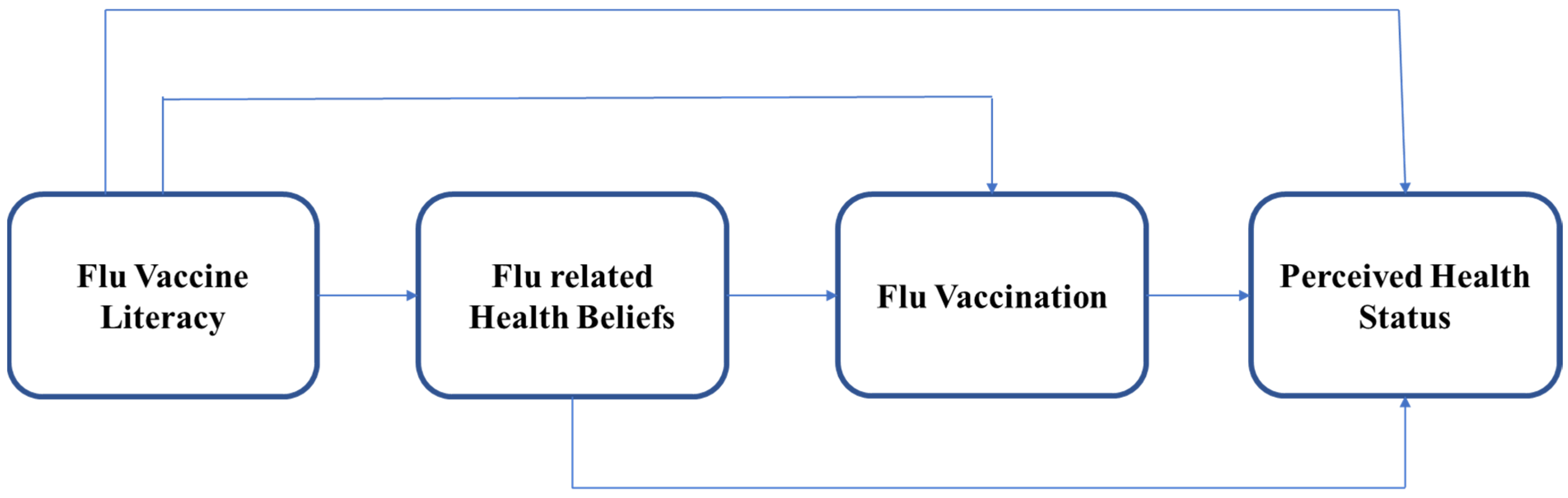
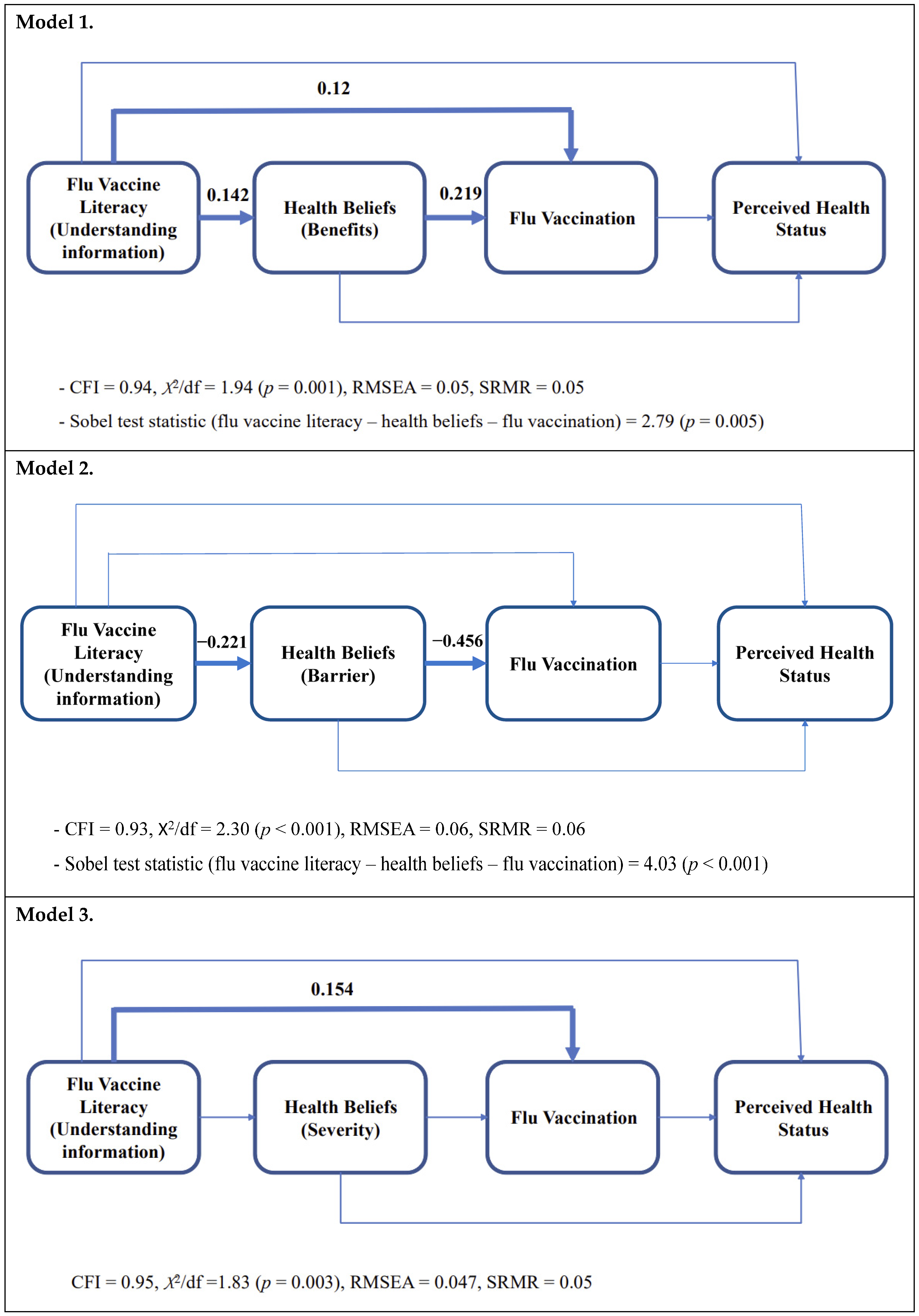
- Hypothesis 1.Flu vaccine literacy influences perceived benefits and flu vaccination influences perceived health status, controlling for socioeconomic factors.
- Hypothesis 2.Flu vaccine literacy influences perceived barriers and flu vaccination influences perceived health status, controlling for socioeconomic factors.
- Hypothesis 3.Flu vaccine literacy influences perceived severity and flu vaccination influences perceived health status, controlling for socioeconomic factors.
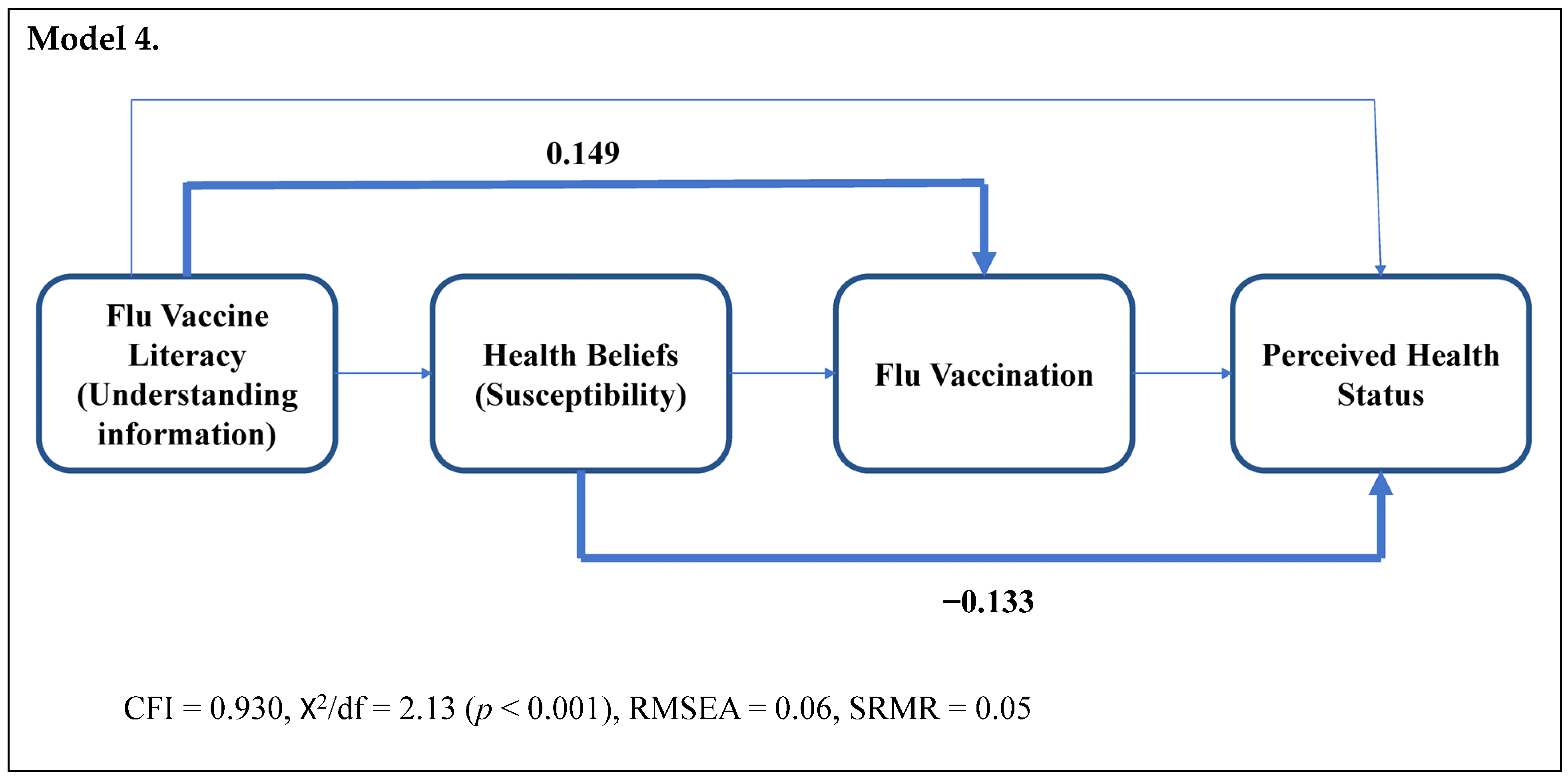
- Hypothesis 4.Flu vaccine literacy influences perceived susceptibility and flu vaccination influences perceived health status, controlling for socioeconomic factors.
2. Materials and Methods
2.1. Data Collection Procedure
2.2. Measures
2.3. Analyses Strategies
3. Results
3.1. Sample Characteristics
3.2. Hypothesis Testing
4. Discussions
4.1. Vaccine Literacy, Health Beliefs, and Flu Vaccination
4.2. Health Beliefs and Perceived Health Status
4.3. Implications
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roman, P.C.; Kirtland, K.; Zell, E.R.; Jones-Jack, N.; Shaw, L.; Shrader, L.; Sprague, C.; Schultz, J.; Le, Q.; Nalla, A.; et al. Influenza Vaccinations During the COVID-19 Pandemic—11 U.S. Jurisdictions, September–December 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 1575–1578. [Google Scholar] [CrossRef] [PubMed]
- Marsa, L. Is a ‘Twindemic’ of Flu and COVID-19 about to Hit the U.S.? National Geographic Society: Washington, DC, USA, 2021. [Google Scholar]
- Siena, L.M.; Isonne, C.; Sciurti, A.; De Blasiis, M.R.; Migliara, G.; Marzuillo, C.; De Vito, C.; Villari, P.; Baccolini, V. The Association of Health Literacy with Intention to Vaccinate and Vaccination Status: A Systematic Review. Vaccines 2022, 10, 1832. [Google Scholar] [CrossRef] [PubMed]
- Shon, E.J.; Wells, A. Effects of Patient-Centered Communication on Influenza Vaccination and Self-Reported General Health Status among Asian Americans: A Comparison Model for Young/Middle-Aged and Older Adults. J. Aging Health 2020, 32, 1409–1418. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Flu Vaccination Coverage, United States, 2021–2022 Influenza Season; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2022. [Google Scholar]
- Grohskopf, L.A.; Blanton, L.H.; Ferdinands, J.M.; Chung, J.R.; Broder, K.R.; Talbot, H.K.; Morgan, R.L.; Fry, A.M. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices—United States, 2022–2023 Influenza Season. MMWR Recomm. Rep. 2022, 71, 1–28. [Google Scholar] [CrossRef]
- Zhang, F.; Or, P.P.-L.; Chung, J.W.-Y. The effects of health literacy in influenza vaccination competencies among community-dwelling older adults in Hong Kong. BMC Geriatr. 2020, 20, 103. [Google Scholar] [CrossRef]
- Biasio, L.R.; Corbellini, G.; D’Alessandro, D. An Italian validation of “meter”, an easy-to-use Health Literacy (hl) screener. Ann. Di Ig. Med. Prev. E Di Comunità 2017, 29, 171–178. [Google Scholar] [CrossRef]
- Benjamin, S.M.; Bahr, K.O. Barriers Associated with Seasonal Influenza Vaccination among College Students. Influenza Res. Treat. 2016, 2016, 4248071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramsey, M.A.; Marczinski, C.A. College students’ perceptions of H1N1 flu risk and attitudes toward vaccination. Vaccine 2011, 29, 7599–7601. [Google Scholar] [CrossRef] [Green Version]
- Nichol, K.L.; D’Heilly, S.; Ehlinger, E.P. Influenza vaccination among college and university students: Impact on influenzalike illness, health care use, and impaired school performance. Arch. Pediatr. Adolesc. Med. 2008, 162, 1113–1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nichol, K.L.; D’Heilly, S.; Ehlinger, E. Colds and influenza-like illnesses in university students: Impact on health, academic and work performance, and health care use. Clin. Infect. Dis. 2005, 40, 1263–1270. [Google Scholar] [CrossRef]
- Santana, S.; Brach, C.; Harris, L.; Ochiai, E.; Blakey, C.; Bevington, F.; Kleinman, D.; Pronk, N. Updating Health Literacy for Healthy People 2030: Defining Its Importance for a New Decade in Public Health. J. Public Health Manag. Pract. 2021, 27, S258–S264. [Google Scholar] [CrossRef]
- Baker, D.W.; Gazmararian, J.A.; Williams, M.V.; Scott, T.; Parker, R.M.; Green, D.; Ren, J.; Peel, J. Health literacy and use of outpatient physician services by Medicare managed care enrollees. J. Gen. Intern. Med. 2004, 19, 215–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, Y.I.; Lee, S.Y.; Arozullah, A.M.; Crittenden, K.S. Effects of health literacy on health status and health service utilization amongst the elderly. Soc. Sci. Med. 2008, 66, 1809–1816. [Google Scholar] [CrossRef]
- Sudore, R.L.; Yaffe, K.; Satterfield, S.; Harris, T.B.; Mehta, K.M.; Simonsick, E.M.; Newman, A.B.; Rosano, C.; Rooks, R.; Rubin, S.M.; et al. Limited literacy and mortality in the elderly: The health, aging, and body composition study. J. Gen. Intern. Med. 2006, 21, 806–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, D.W.; Wolf, M.S.; Feinglass, J.; Thompson, J.A. Health literacy, cognitive abilities, and mortality among elderly persons. J. Gen. Intern. Med. 2008, 23, 723–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hope, C.; Wu, J.; Tu, W.; Young, J.; Murray, M. Association of medication adherence, knowledge, and skills with emergency department visits by adults 50 years or older with congestive heart failure. Am. J. Health Syst. Pharm. 2004, 61, 2043–2049. [Google Scholar] [CrossRef]
- Bennett, I.M.; Chen, J.; Soroui, J.S.; White, S. The contribution of health literacy to disparities in self-rated health status and preventive health behaviors in older adults. Ann. Fam. Med. 2009, 7, 204–211. [Google Scholar] [CrossRef] [Green Version]
- Andre, F.E.; Booy, R.; Bock, H.L.; Clemens, J.; Datta, S.K.; John, T.J.; Lee, B.W.; Lolekha, S.; Peltola, H.; Ruff, T.A.; et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull. World Health Organ. 2008, 86, 140–146. [Google Scholar] [CrossRef]
- Zhang, H.; Chen, L.; Zhang, F. Revisit the Effects of Health Literacy on Health Behaviors in the Context of COVID-19: The Mediation Pathways Based on the Health Belief Model. Front. Public Health 2022, 10, 917022. [Google Scholar] [CrossRef]
- Brega, A.G.; Johnson, R.L.; Schmiege, S.J.; Wilson, A.R.; Jiang, L.; Albino, J. Pathways Through Which Health Literacy Is Linked to Parental Oral Health Behavior in an American Indian Tribe. Ann. Behav. Med. 2021, 55, 1144–1155. [Google Scholar] [CrossRef]
- Ghorbani-Dehbalaei, M.; Loripoor, M.; Nasirzadeh, M. The role of health beliefs and health literacy in women’s health promoting behaviours based on the health belief model: A descriptive study. BMC Women’s Health 2021, 21, 421. [Google Scholar] [CrossRef] [PubMed]
- Jadhav, E.D.; Winkler, D.L.; Anderson, B.S. Vaccination Perceptions of College Students: With and without Vaccination Waiver. Front. Public Health 2018, 6, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratnapradipa, K.L.; Norrenberns, R.; Turner, J.A.; Kunerth, A. Freshman Flu Vaccination Behavior and Intention During a Nonpandemic Season. Health Promot. Pract. 2017, 18, 662–671. [Google Scholar] [CrossRef]
- Yang, Z.J. Predicting young adults’ intentions to get the H1N1 vaccine: An integrated model. J. Health Commun. 2015, 20, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, V. A/H1N1 vaccine intentions in college students: An application of the theory of planned behavior. J. Am. Coll. Health 2014, 62, 416–424. [Google Scholar] [CrossRef] [PubMed]
- Kamimura, A.; Trinh, H.N.; Weaver, S.; Chernenko, A.; Nourian, M.M.; Assasnik, N.; Nguyen, H. Knowledge and Perceptions of Influenza Vaccinations Among College Students in Vietnam and the United States. J. Prev. Med. Public Health 2017, 50, 268–273. [Google Scholar] [CrossRef]
- Palache, A.M. Influenza vaccines. A reappraisal of their use. Drugs 1997, 54, 841–856. [Google Scholar] [CrossRef]
- Nordin, J.; Mullooly, J.; Poblete, S.; Strikas, R.; Petrucci, R.; Wei, F.; Rush, B.; Safirstein, B.; Wheeler, D.; Nichol, K.L. Influenza Vaccine Effectiveness in Preventing Hospitalizations and Deaths in Persons 65 Years or Older in Minnesota, New York, and Oregon: Data from 3 Health Plans. J. Infect. Dis. 2001, 184, 665–670. [Google Scholar] [CrossRef]
- Ohmit, S.E.; Monto, A.S. Influenza vaccine effectiveness in preventing hospitalization among the elderly during influenza type A and type B seasons. Int. J. Epidemiol. 1995, 24, 1240–1248. [Google Scholar] [CrossRef]
- Gross, P.A.; Hermogenes, A.W.; Sacks, H.S.; Lau, J.; Levandowski, R.A. The efficacy of influenza vaccine in elderly persons. A meta-analysis and review of the literature. Ann. Intern. Med. 1995, 123, 518–527. [Google Scholar] [CrossRef]
- Demicheli, V.; Jefferson, T.; Rivetti, D.; Deeks, J. Prevention and early treatment of influenza in healthy adults. Vaccine 2000, 18, 957–1030. [Google Scholar] [CrossRef]
- Glanz, K.; Rimer, B.K.; Viswanath, K. Health Behavior: Theory, Research, and Practice; Wiley: New York, NY, USA, 2015. [Google Scholar]
- Squiers, L.; Peinado, S.; Berkman, N.; Boudewyns, V.; McCormack, L. The health literacy skills framework. J. Health Commun. 2012, 17 (Suppl. 3), 30–54. [Google Scholar] [CrossRef]
- Légaré, F.; Kearing, S.; Clay, K.; Gagnon, S.; D’Amours, D.; Rousseau, M.; O’Connor, A. Are you SURE?: Assessing patient decisional conflict with a 4-item screening test. Can. Fam. Physician 2010, 56, e308–e314. [Google Scholar]
- Montano, D.E. Predicting and Understanding Influenza Vaccination Behavior: Alternatives to the Health Belief Model. Med. Care 1986, 24, 438–453. [Google Scholar] [CrossRef]
- Nexøe, J.; Kragstrup, J.; Søgaard, J. Decision on influenza vaccination among the elderly. A questionnaire study based on the Health Belief Model and the Multidimensional Locus of Control Theory. Scand. J. Prim. Health Care 1999, 17, 105–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coe, A.B.; Gatewood, S.B.; Moczygemba, L.R.; Goode, J.V.; Beckner, J.O. The use of the health belief model to assess predictors of intent to receive the novel (2009) H1N1 influenza vaccine. Innov. Pharm. 2012, 3, 1–11. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Curran, P.J.; West, S.G.; Finch, J.F. The robustness of test statistics to nonnormality and specification error in confirmatory factor analysis. Psychol. Methods 1996, 1, 16–29. [Google Scholar] [CrossRef]
- Fabrigar, L.R.; Wegener, D.T.; MacCallum, R.C.; Strahan, E.J. Evaluating the use of exploratory factor analysis in psychological research. Psychol. Methods 1999, 4, 272–299. [Google Scholar] [CrossRef]
- Abbas, K.M.; Kang, G.J.; Chen, D.; Werre, S.R.; Marathe, A. Demographics, perceptions, and socioeconomic factors affecting influenza vaccination among adults in the United States. PeerJ 2018, 6, e5171. [Google Scholar] [CrossRef] [PubMed]
- Ryan, K.A.; Filipp, S.L.; Gurka, M.J.; Zirulnik, A.; Thompson, L.A. Understanding influenza vaccine perspectives and hesitancy in university students to promote increased vaccine uptake. Heliyon 2019, 5, e02604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, A.V.; Vasudevan, V.; Honn, S.E.; Spitz, M.R.; Chamberlain, R.M. Sociodemographic characteristics, health beliefs, and the accuracy of cancer knowledge. J. Cancer Educ. 2009, 24, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Shon, E.J.; Choe, S.; Lee, L.; Ki, Y. Influenza Vaccination Among U.S. College or University Students: A Systematic Review. Am. J. Health Promot. 2021, 35, 708–719. [Google Scholar] [CrossRef] [PubMed]
- White, S.; Chen, J.; Atchison, R. Relationship of preventive health practices and health literacy: A national study. Am. J. Health Behav. 2008, 32, 227–242. [Google Scholar] [CrossRef] [PubMed]
- Howard, D.H.; Sentell, T.; Gazmararian, J.A. Impact of health literacy on socioeconomic and racial differences in health in an elderly population. J. Gen. Intern. Med. 2006, 21, 857–861. [Google Scholar] [CrossRef]
- Sentell, T.; Vamos, S.; Okan, O. Interdisciplinary Perspectives on Health Literacy Research Around the World: More Important Than Ever in a Time of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 3010. [Google Scholar] [CrossRef] [PubMed]
- Biasio, L.R. Vaccine hesitancy and health literacy. Hum. Vaccines Immunother. 2017, 13, 701–702. [Google Scholar] [CrossRef]
- Panahi, R.; Hosseini, N.; Ramezankhani, A.; Anbari, M.; Amjadian, M.; Dehghankar, L.; Niknami, S. Measuring the Structures of the Health Belief Model Integrated with Health Literacy in Predicting University Students’ Adoption of Smoking Preventive Behaviors. J. Prev. Med. Hyg. 2022, 63, E51–E58. [Google Scholar] [CrossRef]
- Panahi, R.; Ramezankhani, A.; Tavousi, M.; Niknami, S. Adding Health Literacy to the Health Belief Model: Effectiveness of an Educational Intervention on Smoking Preventive Behaviors Among University Students. Iran. Red Crescent Med. J. 2018, 20, e13773. [Google Scholar] [CrossRef]
- Niu, Z.; Qin, Z.; Hu, P.; Wang, T. Health Beliefs, Trust in Media Sources, Health Literacy, and Preventive Behaviors among High-Risk Chinese for COVID-19. Health Commun. 2022, 37, 1004–1012. [Google Scholar] [CrossRef]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef]
- Veldwijk, J.; van der Heide, I.; Rademakers, J.; Schuit, A.J.; de Wit, G.A.; Uiters, E.; Lambooij, M.S. Preferences for Vaccination: Does Health Literacy Make a Difference? Med. Decis. Mak. 2015, 35, 948–958. [Google Scholar] [CrossRef] [PubMed]
- Peretti-Watel, P.; Raude, J.; Sagaon-Teyssier, L.; Constant, A.; Verger, P.; Beck, F. Attitudes toward vaccination and the H1N1 vaccine: Poor people’s unfounded fears or legitimate concerns of the elite? Soc. Sci. Med. 2014, 109, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Börjesson, M.; Enander, A. Perceptions and sociodemographic factors influencing vaccination uptake and precautionary behaviours in response to the A/H1N1 influenza in Sweden. Scand. J. Public Health 2014, 42, 215–222. [Google Scholar] [CrossRef]
- Uddin, M.; Cherkowski, G.C.; Liu, G.; Zhang, J.; Monto, A.S.; Aiello, A.E. Demographic and socioeconomic determinants of influenza vaccination disparities among university students. J. Epidemiol. Community Health 2010, 64, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Poehling, K.A.; Blocker, J.; Ip, E.H.; Peters, T.R.; Wolfson, M. 2009–2010 seasonal influenza vaccination coverage among college students from 8 universities in North Carolina. J. Am. Coll. Health 2012, 60, 541–547. [Google Scholar] [CrossRef] [Green Version]
- Shon, E.J.; Ki, Y.; Lee, L. Effects of Health Beliefs on Flu Vaccination and Physical Health among Under/Graduate Students in the U.S.: Racial Differences (Whites, African Americans, Hispanics, and Asians). Soc. Work. Public Health 2021, 36, 377–391. [Google Scholar] [CrossRef]
- Kawachi, I.; Daniels, N.; Robinson, D.E. Health disparities by race and class: Why both matter. Health Aff. 2005, 24, 343–352. [Google Scholar] [CrossRef]
- Undurraga, E.A.; Nyberg, C.; Eisenberg, D.T.A.; Magvanjav, O.; Reyes-García, V.; Huanca, T.; Leonard, W.R.; McDade, T.W.; Tanner, S.; Vadez, V.; et al. Individual Wealth Rank, Community Wealth Inequality, and Self-Reported Adult Poor Health: A Test of Hypotheses with Panel Data (2002–2006) from Native Amazonians, Bolivia. Med. Anthropol. Q. 2010, 24, 522–548. [Google Scholar] [CrossRef]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J. Strategies for addressing vaccine hesitancy—A systematic review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [Green Version]
- Biasio, L.R.; Corsello, G.; Costantino, C.; Fara, G.M.; Giammanco, G.; Signorelli, C.; Vecchio, D.; Vitale, F. Communication about vaccination: A shared responsibility. Hum. Vaccines Immunother. 2016, 12, 2984–2987. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Items | Response Option | |
| (1) | “I do not want to be vaccinated” (i.e., with the flu vaccine) | Participants were asked to rate their agreement with each item on a 5-point scale ranging from “strongly disagree” (1)~“strongly agree” (5). |
| (2) | “Flu vaccination has unpleasant side-effects” | |
| (3) | “In general I am opposed to vaccinations” | |
| (4) | “It is too much trouble for me to go to the doctor to be vaccinated” | |
| (5) | “Flu vaccinations weaken the natural immune system” | |
| (6) | “Flu vaccinations are too expensive” | |
| (7) | “Flu vaccinations are an effective protection against the flu” | |
| (8) | “I have an increased risk of falling ill with flu” | |
| (9) | “I am concerned about the risk of falling seriously ill” | |
| (10) | “I get sick more easily than other people my age” | |
| (11) | “Flu infection may lead to serious health problems” | |
| (12) | “If I had the flu, I would not be able to manage daily activities” | |
| (13) | “I am afraid the flu will make me very sick” | |
| (14) | “I am very worried about catching the flu” | |
| (15) | “Whenever I get sick it seems to be serious” | |
| (16) | “I cannot stand a flu infection because of my general health” |
| Category | Response Options | N or M | % or SD |
|---|---|---|---|
| Flu vaccination | Yes | 187 | 49.00 |
| No | 195 | 51.00 | |
| Race | Whites | 143 | 37.40 |
| African Americans | 59 | 15.40 | |
| Hispanics | 69 | 18.10 | |
| Asians | 111 | 29.10 | |
| Gender | Male | 100 | 26.2 |
| Female | 282 | 73.8 | |
| Age | 22.37 | 5.97 | |
| Family income (annual) | USD 0 to USD 44,999, | 92 | 24.10 |
| USD 45,000 to USD 139,999 | 164 | 42.90 | |
| above USD 140,000 | 126 | 33.00 | |
| Education (on average) | (0 = no formal education, 1 = 1st year, 2 = 2nd year, 3 = 3rd year, 4 = 4th year, 5 = 5th year, 6 = graduate school) | 3.33 (on average, 3rd year) | 1.60 |
| Parent’s education (Mum; on average) | (0 = no formal education, 1 = elementary school, 2 = middle school, 3 = high school, 4 = some college, 5 = 2 years college, 6 = 4 years university, 7 = master’s degree, 8 = doctorate or higher) | 5.45 (on average, 2 years college level) | 1.69 |
| Parent’s education (Dad; on average) | (0 = no formal education, 1 = elementary school, 2 = middle school, 3 = high school, 4 = some college, 5 = 2 years college, 6 = 4 years university, 7 = master’s degree, 8 = doctorate or higher) | 5.45 (on average, 2 years college level) | 2.02 |
| Insurance | Insured | 344 | 90.10 |
| Uninsured | 38 | 9.90 | |
| Health Belief | Barrier (range: 6–30) | 11.53 | 4.64 |
| Benefit (range: 1–5) | 3.57 | 1.186 | |
| Susceptibility (range: 3–15) | 6.76 | 2.82 | |
| Severity (range: 6–30) | 16.42 | 4.73 | |
| Perceived Health Status | (range: 1–5) | 3.71 | 0.88 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shon, E.-J.; Lee, L. Effects of Vaccine Literacy, Health Beliefs, and Flu Vaccination on Perceived Physical Health Status among Under/Graduate Students. Vaccines 2023, 11, 765. https://doi.org/10.3390/vaccines11040765
Shon E-J, Lee L. Effects of Vaccine Literacy, Health Beliefs, and Flu Vaccination on Perceived Physical Health Status among Under/Graduate Students. Vaccines. 2023; 11(4):765. https://doi.org/10.3390/vaccines11040765
Chicago/Turabian StyleShon, En-Jung, and Lena Lee. 2023. "Effects of Vaccine Literacy, Health Beliefs, and Flu Vaccination on Perceived Physical Health Status among Under/Graduate Students" Vaccines 11, no. 4: 765. https://doi.org/10.3390/vaccines11040765