

Humoral Response in Hemodialysis Patients Post-SARS-CoV-2 mRNA Vaccination: A Systematic Review of Literature
 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy and Selection Criteria
2.2. Screening Process, Study Selection and Data Extraction
2.3. Methodological Quality
2.4. Data Synthesis
3. Results
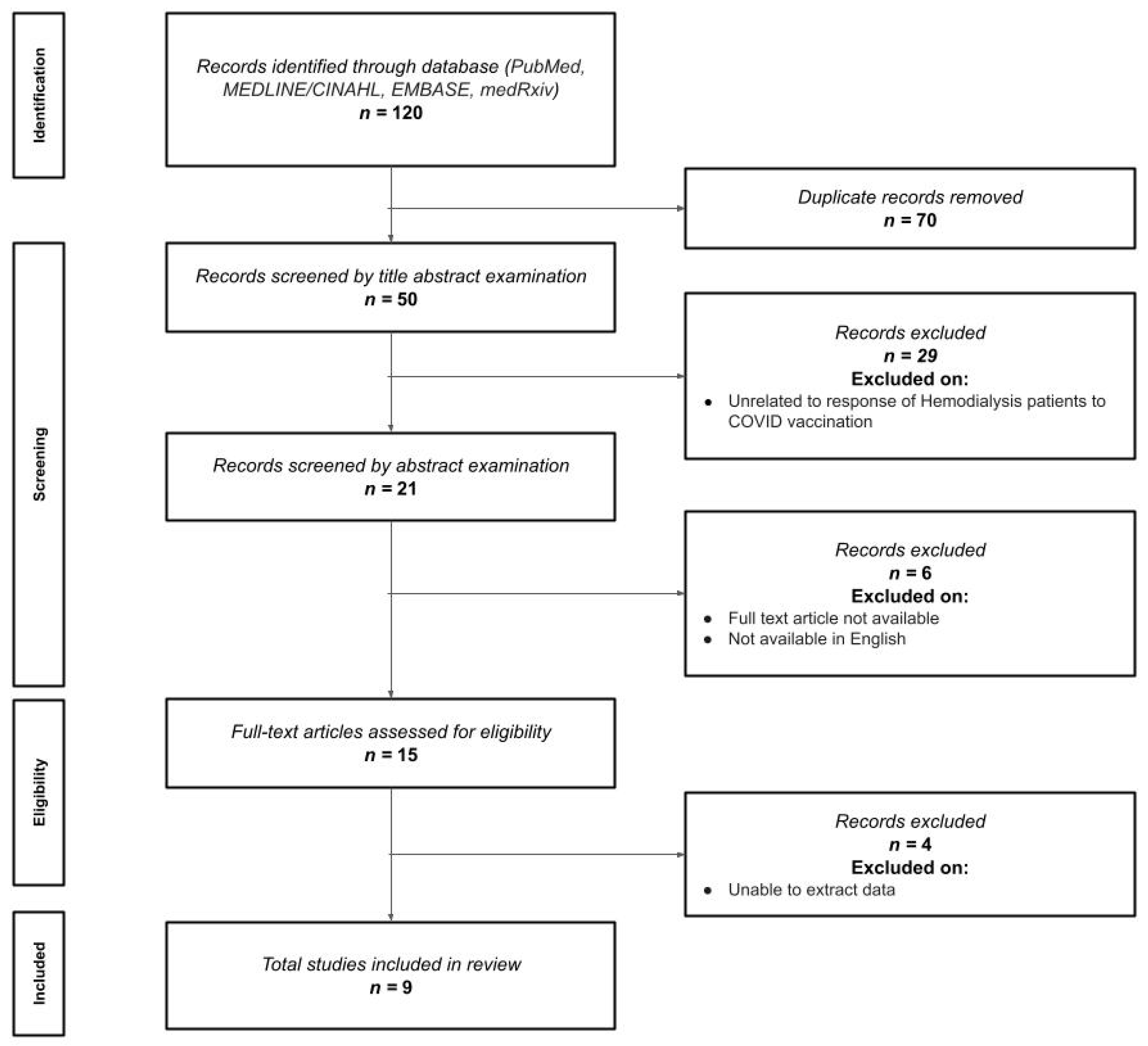
3.1. Study Selection
3.2. Sample Characteristics
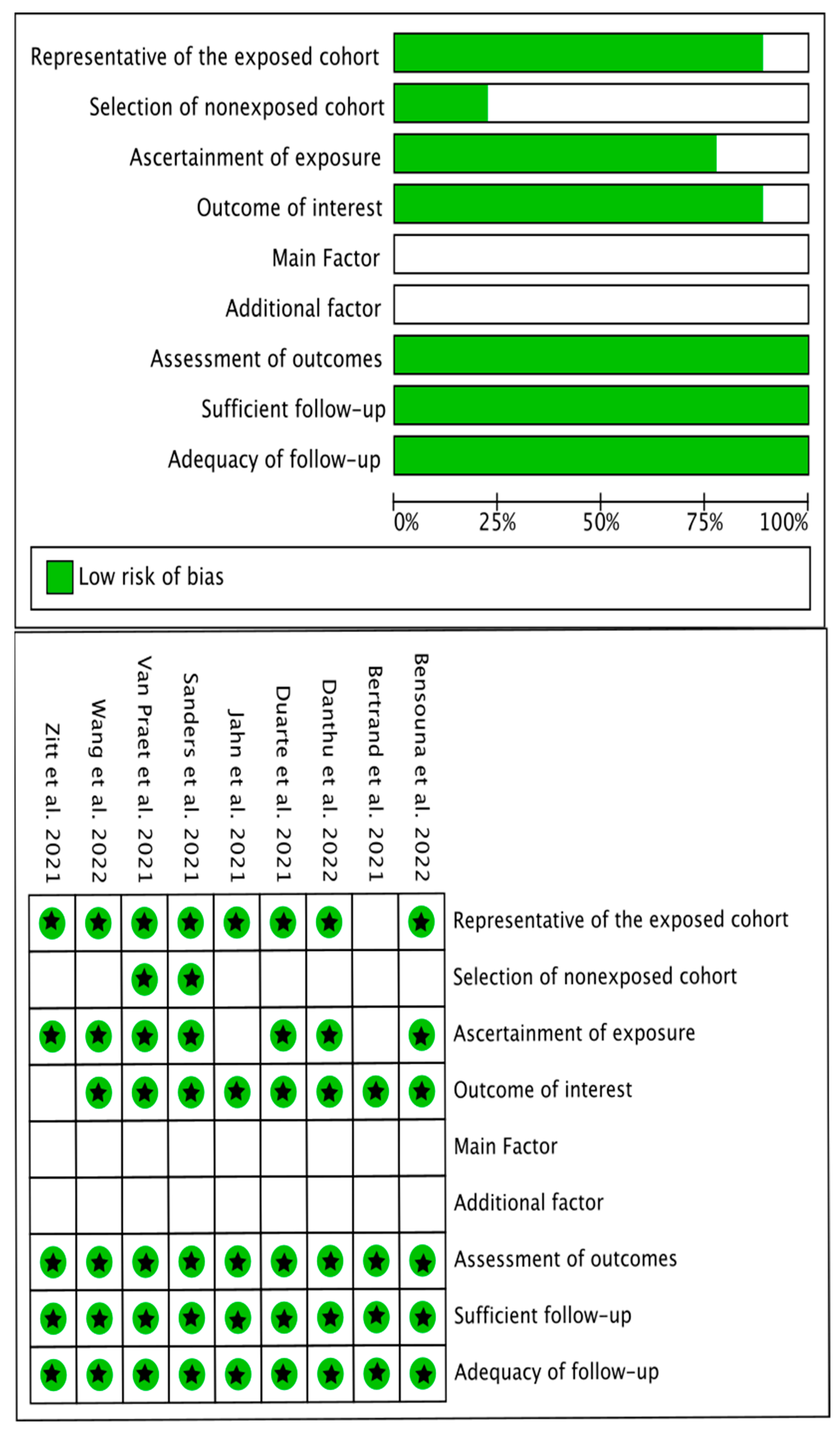
3.3. Methodological Quality
3.4. Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/ (accessed on 10 January 2023).
- Torres, R.; Toro, L.; Sanhueza, M.E.; Lorca, E.; Ortiz, M.; Pefaur, J.; Clavero, R.; Machuca, E.; Gonzalez, F.; Herrera, P.; et al. Clinical efficacy of SARS-CoV-2 vaccination in hemodialysis patients. Kidney Int. Rep. 2022, 7, 2176–2185. [Google Scholar] [CrossRef]
- Alfano, G.; Ferrari, A.; Magistroni, R.; Fontana, F.; Cappelli, G.; Basile, C. The frail world of haemodialysis patients in the COVID-19 Pandemic Era: A systematic scoping review. J. Nephrol. 2021, 34, 1387–1403. [Google Scholar] [CrossRef]
- Diaz, R.T.; Herrera, E.L. COVID-19 in chronic kidney patients: A warning. Rev. Méd. Chile 2020, 148, 707–714. [Google Scholar]
- Notarte, K.I.; Ver, A.T.; Velasco, J.V.; Pastrana, A.; Catahay, J.A.; Salvagno, G.L.; Yap, E.P.H.; Martinez-Sobrido, L.; Torrelles, J.B.; Lippi, G.; et al. Effects of age, sex, serostatus, and underlying comorbidities on humoral response post-SARS-CoV-2 Pfizer-BioNTech MRNA vaccination: A systematic review. Crit. Rev. Clin. Lab. Sci. 2022, 59, 373–390. [Google Scholar] [CrossRef]
- Notarte, K.I.; Guerrero-Arguero, I.; Velasco, J.V.; Ver, A.T.; de Oliveira, M.H.S.; Catahay, J.A.; Khan, S.R.; Pastrana, A.; Juszczyk, G.; Torrelles, J.B.; et al. Characterization of the significant decline in humoral immune response six months Post-SARS-CoV-2 MRNA Vaccination: A systematic review. J. Med. Virol. 2022, 94, 2939–2961. [Google Scholar] [CrossRef]
- Labriola, L.; Scohy, A.; Seghers, F.; Perlot, Q.; De Greef, J.; Desmet, C.; Romain, C.; Morelle, J.; Yombi, J.-C.; Kabamba, B.; et al. A longitudinal, 3-month serologic assessment of SARS-CoV-2 infections in a Belgian hemodialysis facility. Clin. J. Am. Soc. Nephrol. 2021, 16, 613–614. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 MRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Yau, K.; Abe, K.T.; Naimark, D.; Oliver, M.J.; Perl, J.; Leis, J.A.; Bolotin, S.; Tran, V.; Mullin, S.I.; Shadowitz, E.; et al. Evaluation of the SARS-CoV-2 antibody response to the BNT162b2 Vaccine in patients undergoing hemodialysis. JAMA Netw. Open 2021, 4, e2123622. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non-Randomised Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 20 January 2023).
- Danthu, C.; Hantz, S.; Dahlem, A.; Duval, M.; Ba, B.; Guibbert, M.; El Ouafi, Z.; Ponsard, S.; Berrahal, I.; Achard, J.-M.; et al. Humoral response after SARS-CoV-2 MRNA vaccination in a cohort of hemodialysis patients and kidney transplant recipients. J. Am. Soc. Nephrol. 2021, 32, 2153–2158. [Google Scholar] [CrossRef]
- Van Praet, J.; Reynders, M.; De Bacquer, D.; Viaene, L.; Schoutteten, M.K.; Caluwé, R.; Doubel, P.; Heylen, L.; De Bel, A.V.; Van Vlem, B.; et al. Predictors and dynamics of the humoral and cellular immune response to SARS-CoV-2 MRNA vaccines in hemodialysis patients: A multicenter observational study. J. Am. Soc. Nephrol. 2021, 32, 3208–3220. [Google Scholar] [CrossRef]
- Sanders, J.-S.F.; Bemelman, F.J.; Messchendorp, A.L.; Baan, C.C.; van Baarle, D.; van Binnendijk, R.; Diavatopoulos, D.A.; Frölke, S.C.; Geers, D.; GeurtsvanKessel, C.H.; et al. The RECOVAC immune-response study: The immunogenicity, tolerability, and safety of COVID-19 vaccination in patients with chronic kidney disease, on dialysis, or living with a kidney transplant. Transplantation 2022, 106, 821–834. [Google Scholar] [CrossRef]
- Bertrand, D.; Hamzaoui, M.; Lemée, V.; Lamulle, J.; Hanoy, M.; Laurent, C.; Lebourg, L.; Etienne, I.; Lemoine, M.; Le Roy, F.; et al. Antibody and T Cell Response to SARS-CoV-2 Messenger RNA BNT162b2 vaccine in kidney transplant recipients and hemodialysis patients. J. Am. Soc. Nephrol. 2021, 32, 2147–2152. [Google Scholar] [CrossRef]
- Bensouna, I.; Caudwell, V.; Kubab, S.; Acquaviva, S.; Pardon, A.; Vittoz, N.; Bozman, D.-F.; Hanafi, L.; Faucon, A.-L.; Housset, P. SARS-CoV-2 Antibody response after a third dose of the BNT162b2 vaccine in patients receiving maintenance hemodialysis or peritoneal dialysis. Am. J. Kidney Dis. 2022, 79, 185–192.e1. [Google Scholar] [CrossRef] [PubMed]
- Duarte, R.; Roldão, M.; Figueiredo, C.; Luz, I.; Ferrer, F.; Gonçalves, H.; Sofia, F.; Lopes, K. Humoral response to BNT162b2 mRNA COVID-19 vaccine in peritoneal and hemodialysis patients: A comparative study. Ther. Apher. Dial. 2022, 26, 790–796. [Google Scholar] [CrossRef]
- Jahn, M.; Korth, J.; Dorsch, O.; Anastasiou, O.E.; Sorge-Hädicke, B.; Tyczynski, B.; Gäckler, A.; Witzke, O.; Dittmer, U.; Dolff, S.; et al. Humoral response to SARS-CoV-2-vaccination with BNT162b2 (Pfizer-BioNTech) in patients on hemodialysis. Vaccines 2021, 9, 360. [Google Scholar] [CrossRef]
- Zitt, E.; Davidovic, T.; Schimpf, J.; Abbassi-Nik, A.; Mutschlechner, B.; Ulmer, H.; Benda, M.A.; Sprenger-Mähr, H.; Winder, T.; Lhotta, K. The safety and immunogenicity of the MRNA-BNT162b2 SARS-CoV-2 vaccine in hemodialysis patients. Front. Immunol. 2021, 12, 704773. [Google Scholar] [CrossRef]
- Wang, X.; Han, M.; Fuentes, L.R.; Thwin, O.; Grobe, N.; Wang, K.; Wang, Y.; Kotanko, P. SARS-CoV-2 neutralizing antibody response after three doses of MRNA1273 Vaccine and COVID-19 in hemodialysis patients. Front. Nephrol. 2022, 2, 926635. [Google Scholar] [CrossRef]
- Stumpf, J.; Siepmann, T.; Lindner, T.; Karger, C.; Schwöbel, J.; Anders, L.; Faulhaber-Walter, R.; Schewe, J.; Martin, H.; Schirutschke, H.; et al. humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using MRNA-1273 or BNT162b2 MRNA Vaccine. Lancet Reg. Health Eur. 2021, 9, 100178. [Google Scholar] [CrossRef]
- Attias, P.; Sakhi, H.; Rieu, P.; Soorkia, A.; Assayag, D.; Bouhroum, S.; Nizard, P.; El Karoui, K. Antibody response to the BNT162b2 vaccine in maintenance hemodialysis patients. Kidney Int. 2021, 99, 1490–1492. [Google Scholar] [CrossRef]
- Billany, R.E.; Selvaskandan, H.; Adenwalla, S.F.; Hull, K.L.; March, D.S.; Burton, J.O.; Bishop, N.C.; Carr, E.J.; Beale, R.; Tang, J.W.; et al. Seroprevalence of Antibody to S1 spike protein following vaccination against COVID-19 in patients receiving hemodialysis: A call to arms. Kidney Int. 2021, 99, 1492–1494. [Google Scholar] [CrossRef]
- Broseta, J.J.; Rodríguez-Espinosa, D.; Rodríguez, N.; Mosquera, M.d.M.; Marcos, M.Á.; Egri, N.; Pascal, M.; Soruco, E.; Bedini, J.L.; Bayés, B.; et al. Humoral and Cellular Responses to MRNA-1273 and BNT162b2 SARS-CoV-2 vaccines administered to hemodialysis patients. Am. J. Kidney Dis. 2021, 78, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.; Montez-Rath, M.E.; Han, J.; Garcia, P.; Cadden, L.; Hunsader, P.; Kerschmann, R.; Beyer, P.; Dittrich, M.; Block, G.A.; et al. Antibody Response to COVID-19 vaccination in patients receiving dialysis. J. Am. Soc. Nephrol. 2021, 32, 2435–2438. [Google Scholar] [CrossRef] [PubMed]
- Agur, T.; Ben-Dor, N.; Goldman, S.; Lichtenberg, S.; Herman-Edelstein, M.; Yahav, D.; Rozen-Zvi, B.; Zingerman, B. Antibody Response to MRNA SARS-CoV-2 vaccine among dialysis patients—A prospective cohort study. Nephrol. Dial. Transplant. 2021, 36, 1347–1349. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-J.; Lee, T.H.; Tian, Y.-C.; Lee, C.-C.; Fan, P.-C.; Chang, C.-H. Immunogenicity Rates After SARS-CoV-2 vaccination in people with end-stage kidney disease: A systematic review and meta-analysis. JAMA Netw. Open 2021, 4, e2131749. [Google Scholar] [CrossRef]
- Quiroga, B.; Soler, M.J.; Ortiz, A.; Vaquera, S.M.; Mantecón, C.J.J.; Useche, G.; Márquez, M.G.S.; Carnerero, M.; Rodríguez, M.T.J.; Ramos, P.M.; et al. Safety and immediate humoral response of COVID-19 vaccines in chronic kidney disease patients: The SENCOVAC Study. Nephrol. Dial. Transplant. 2022, 37, 1868–1878. [Google Scholar] [CrossRef]
- Speer, C.; Schaier, M.; Nusshag, C.; Töllner, M.; Buylaert, M.; Kälble, F.; Reichel, P.; Grenz, J.; Süsal, C.; Zeier, M.; et al. Longitudinal humoral responses after COVID-19 vaccination in peritoneal and hemodialysis patients over twelve weeks. Vaccines 2021, 9, 1130. [Google Scholar] [CrossRef]
- Buchwinkler, L.; Solagna, C.A.; Messner, J.; Pirklbauer, M.; Rudnicki, M.; Mayer, G.; Kerschbaum, J. Antibody response to MRNA vaccines against SARS-CoV-2 with chronic kidney disease, hemodialysis, and after kidney transplantation. J. Clin. Med. 2021, 11, 148. [Google Scholar] [CrossRef]
- Grupper, A.; Sharon, N.; Finn, T.; Cohen, R.; Israel, M.; Agbaria, A.; Rechavi, Y.; Schwartz, I.F.; Schwartz, D.; Lellouch, Y.; et al. Humoral response to the Pfizer BNT162b2 vaccine in patients undergoing maintenance hemodialysis. Clin. J. Am. Soc. Nephrol. 2021, 16, 1037–1042. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Pubmed Search Formula |
| #1 “Hemodialysis” [All Fields] #2 “humoral response” [All Fields] #3 “COVID vaccine” [All Fields] OR “COVID-19 Vaccines” [Mesh] OR “SARS-CoV-2 vaccine” [All Fields] OR “BNT162b2” [All Fields] OR “BNT162 Vaccine” [Mesh] OR “Pfizer-BioNTech” [All Fields] OR “mRNA-1273” [All Fields] OR “2019-nCoV Vaccine mRNA-1273” [Mesh] OR “Moderna” [All Fields] #4 #1 AND #2 #5 #1 AND #3 #6 #1 AND #2 AND #3 |
| MEDLINE/CINAHL (via EBSCO) Search Formula |
| #1 “Hemodialysis” #2 “humoral response” #3 “COVID vaccine” OR “SARS-CoV-2 vaccine” OR “BNT162b2” OR “Pfizer-BioNTech” OR “mRNA-1273” OR “Moderna” #4 #1 AND #2 #5 #1 AND #3 #6 #1 AND #2 AND #3 |
| Author | Vaccine | Country | Sample | Age | Assay | Findings | |
|---|---|---|---|---|---|---|---|
| First Dose | Second Dose | ||||||
| Danthu et al. [12] | BNT162b2/Pfizer-BioNTech | France | n = 159 HDP: n = 78 KTR: n = 74 Controls: n = 7 | Mean (SD) HDP: 73.5 (12.8) KTR: 64.8 (11.5) Control: 51.6 (6.8) | Baseline: Abbott Alinity SARS-CoV-2 IgG (Chicago, IL, USA) Post-vaccination: LIAISON SARS-CoV-2 TrimericS IgG (DiaSorin, Saluggia, Italy) | 14 days after the first injection, Ab titers in control group were 14.75-fold higher than HDP. No positive antibody levels were detected in KTR patients. | 8 days after the second dose, Ab titers in controls and HDP increased 18.34-fold, and 1.65-fold, respectively. Ab in controls was 163.94-fold higher than HDP 8 days after the second dose. 30 days after the second dose, Ab titer in controls and HDP increased 0.85-fold, and 41.82-fold, respectively, compared with 8 days after the second dose. Ab in controls was 3.35-fold higher than HDP 30 days after the second dose. |
| Van Praet et al. [13] | BNT162b2/Pfizer-BioNTech & mRNA-1273/Moderna-NIAID | Belgium | n = 618 HDP: n = 543 Pfizer-BioNTech: n = 322 Moderna-NIAID: n = 221 Controls: n = 75 Pfizer-BioNTech: n = 37 Moderna-NIAID: n = 38 | Median (range) Pfizer-BioNTech: 76 (66–82) Moderna-NIAID: 75 (65–82) | AdviseDx SARS-CoV-2 IgG II chemiluminescent microparticle immunoassay (Abbott, Ireland) | 28 days after the first BNT162b2 dose, antibody titers in controls were 22.3-fold higher than in HDP. 56 days after the first BNT162b2 dose, antibody titers in controls were 5.2-fold higher than in HDP. 35 days after the first mRNA-1273 dose, antibody titers in controls were 14.8-fold higher than in HDP 63 days after the first mRNA-1273 dose, antibody titers in controls were 4.7-fold higher than in HDP. | ND |
| Sanders et al. [14] | mRNA-1273/Moderna-NIAID | Netherlands | n = 800 Controls: n = 191 CKD G4/5: n = 162 HDP: n = 159 KTR: n = 288 | Mean (SD) Controls: 58.5 (13.0) CKD G4/5: 60.6 (13.4) HDP: 59.8 (14.3) KTR: 56.1 (14.0) | Validated fluorescent bead-based multiplex-immunoassay with a specificity and sensitivity of 99.7% and 91.6% | 28 days after the first dose, antibody titers in responders were 1.8-fold higher in controls than in CKD stage 4 or 5 (CKD 4/5) patients, 4-fold higher than in HDP and 500-fold higher than in KTR. | 28 days after the second dose, antibody titers in responders were 1.3-fold higher in controls than in CKD stage 4 or 5 (CKD 4/5) patients, 1.9-fold higher than in HDP and 127.4-fold higher than in (KTR). |
| Bertrand et al. [15] | BNT162b2/Pfizer-BioNTech | France | n = 55 HDP: n = 10 KTR: n = 45 | Mean (SD) HDP: 71.2 (16.4) KTR: 63.5 (16.3) | AdviseDx SARS-CoV-2 IgG II chemiluminescent microparticle immunoassay (Abbott, Ireland) | 21 days after the first dose, only one HDP (11.1%) and one KTR (2.2%) showed anti–SARS-CoV-2 antibodies. Antibody titers in responders were 1.74-fold higher in KTR as compared with HDP. | 30 days after the second dose, eight HDP (88.9%) and eight KTRs (17.8%) developed SARS-CoV-2 antibodies. HDP and KTR antibody titers increased 5.88-fold and 2.16-fold, respectively. HDP responders had a 1.57-fold higher response than KTR responders after the second dose. |
| Duarte et al. [17] | BNT162b2/Pfizer-BioNTech | Portugal | Total: n = 67 HDP: n = 25 PDP: n = 42 | Mean (SD) HDP: 75.1 (11.7) PDP: 60.5 (10.7) | MAGLUMI® SARS-CoV-2 S-RBD IgG chemiluminescence kit. (Snibe Diagnostic, China) | 21 days after the first dose, IgG titers in PDP were 5.45-fold higher than HDP. HDP was weakly associated with non-response after the first dose when compared with PDP | 21 days after the second dose, IgG titers in PDP and HDP increased by 31.33-fold and 66.47-fold, respectively, with titers in PDP being 2.59-fold higher than HDP. |
| Jahn et al. [18] | BNT162b2/Pfizer-BioNTech | Germany | Total: n = 88 HDP: n = 72 Controls: n = 16 | HDP: 68 (37–90) Controls: 45 (39–65) | LIAISON® SARS-CoV-2-TrimericS IgG chemiluminescent immunoassay (Diasorin S.p.A., Saluggia, Italy) | ND | 13 days after the second dose for controls and 17 days after for HDP, antibody titers were 2.1-fold higher in controls compared with HDP. |
| Zitt et al. [19] | BNT162b2/Pfizer-BioNTech | Austria | Total: n = 50 Seroconversion: n = 21 No seroconversion: n = 29 | Mean (SD) Seroconversion: 67.6 (16.1) No seroconversion: 71.2 (12.9) | LIAISON® SARS-CoV-2-TrimericS IgG chemiluminescent immunoassay (Diasorin S.p.A., Saluggia, Italy) | Compared with the baseline of being seronegative, 25 days after first dose, antibody titer in hemodialysis patients was 56.7 BAU/mL | Compared with the baseline of being seronegative, 28 days after the second dose, antibody titer in hemodialysis was 1565.0 BAU/mL |
| Author | Vaccine | Country | Sample | Age | Assay | Findings after Booster |
|---|---|---|---|---|---|---|
| Bensouna et al. [16] | BNT162b2/Pfizer-BioNTech | France | n = 69 HDP: n = 38 PDP: n = 31 | Median (range) 68 (53–76) | Elecsys Anti-SARS-CoV-2 S1 (Roche Diagnostics, Boulogne-Billancourt, France) | At least 3 weeks after the booster dose, the Ab of HDP and PDP increased by 26.6-fold as compared with the second dose. Patients with a greater increase in anti-S1 Ab levels after the third dose had lower Ab levels after the second dose, and a longer time interval between the second and the third dose. |
| Wang et al. [20] | mRNA-1273/Moderna-NIAID | United States | n = 63 Vaccination cohort: n = 42 Infection cohort: n = 21 | Vaccination cohort: 63 (42–82) Infection cohort: 62 (41–80) | GenScript SARS-CoV-2 Surrogate Virus Neutralization Test Kit (GenScript Biotech Corporation, Piscataway, NJ, USA) | Compared with levels prior to the third dose of mRNA 1273, nAb-WT increased 18-fold and nAb-Omicron increased 23-fold after 23 and 24 days from the third dose, respectively. |
| Study | Selection | Comparability | Outcome | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Representative of the Exposed Cohort | Selection of Nonexposed Cohort | Ascertainment of Exposure | Outcome of Interest | Main Factor | Additional Factor | Assessment of Outcomes | Sufficient Follow-Up | Adequacy of Follow-Up | Total Score | |
| Zitt et al. [19] | ★ | ★ | ★ | ★ | ★ | ★ | 6/9 | |||
| Jahn et al. [18] | ★ | ★ | ★ | ★ | ★ | ★ | 6/9 | |||
| Duarte et al. [17] | ★ | ★ | ★ | ★ | ★ | ★ | 6/9 | |||
| Bertrand et al. [15] | ★ | ★ | ★ | ★ | 4/9 | |||||
| Sanders et al. [14] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 7/9 | ||
| Danthu et al. [12] | ★ | ★ | ★ | ★ | ★ | ★ | 6/9 | |||
| Wang et al. [20] | ★ | ★ | ★ | ★ | ★ | ★ | 6/9 | |||
| Van Praet et al. [13] | ★ | ★ | ★ | ★ | ★ | ★ | ★ | 7/9 | ||
| Bensouna et al. [16] | ★ | ★ | ★ | ★ | ★ | ★ | 6/9 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Notarte, K.I.; Catahay, J.A.; Peligro, P.J.; Velasco, J.V.; Ver, A.T.; Guerrero, J.J.; Liu, J.; Lippi, G.; Benoit, S.W.; Henry, B.M.; et al. Humoral Response in Hemodialysis Patients Post-SARS-CoV-2 mRNA Vaccination: A Systematic Review of Literature. Vaccines 2023, 11, 724. https://doi.org/10.3390/vaccines11040724
Notarte KI, Catahay JA, Peligro PJ, Velasco JV, Ver AT, Guerrero JJ, Liu J, Lippi G, Benoit SW, Henry BM, et al. Humoral Response in Hemodialysis Patients Post-SARS-CoV-2 mRNA Vaccination: A Systematic Review of Literature. Vaccines. 2023; 11(4):724. https://doi.org/10.3390/vaccines11040724
Chicago/Turabian StyleNotarte, Kin Israel, Jesus Alfonso Catahay, Princess Juneire Peligro, Jacqueline Veronica Velasco, Abbygail Therese Ver, Jonathan Jaime Guerrero, Jin Liu, Giuseppe Lippi, Stefanie W. Benoit, Brandon Michael Henry, and et al. 2023. "Humoral Response in Hemodialysis Patients Post-SARS-CoV-2 mRNA Vaccination: A Systematic Review of Literature" Vaccines 11, no. 4: 724. https://doi.org/10.3390/vaccines11040724