
Past and Future Influenza Vaccine Uptake Motivation: A Cross-Sectional Analysis among Italian Health Sciences Students
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethical Considerations
2.3. Statistical Analysis
3. Results
3.1. Descriptive Characteristics
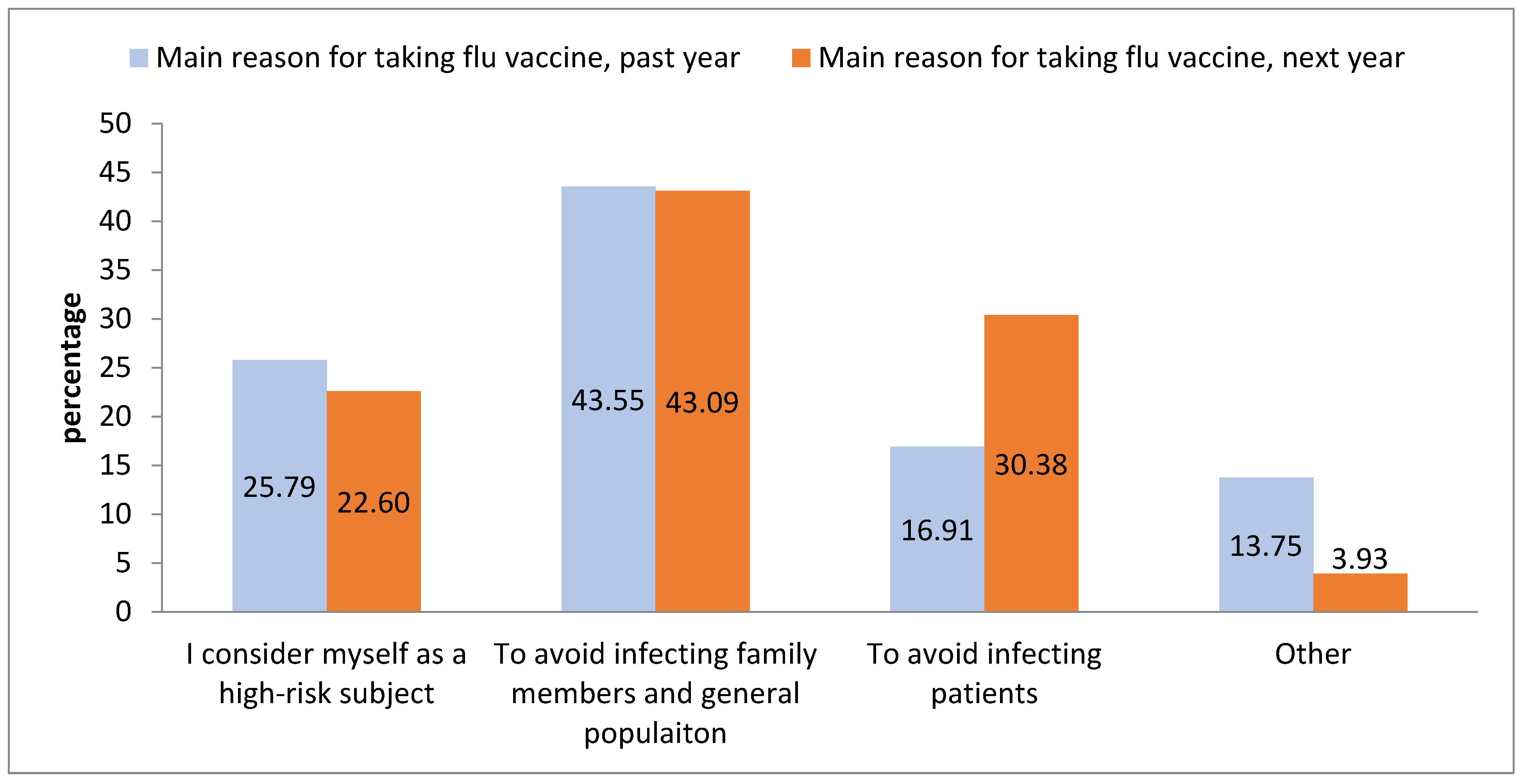
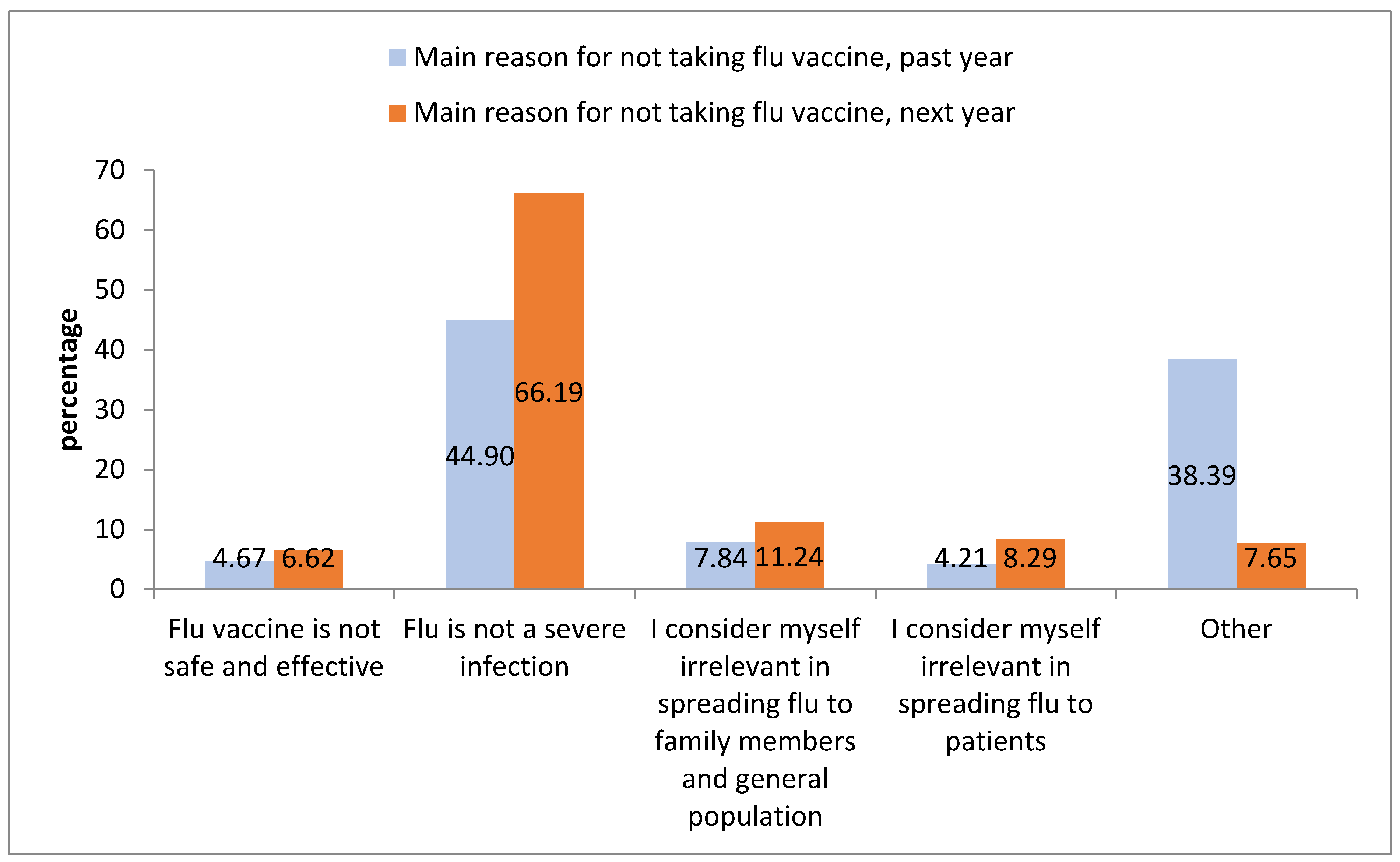
3.2. Influenza Vaccine Acceptance during the Previous Year
3.3. Influenza Vaccine Acceptance during the Following Year
4. Discussion
4.1. Implications for Public Health Policies and Practice
4.2. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Vaccines and Immunization; World Health Organization: Geneva, Switzerland, 2023; Available online: https://www.who.int/health-topics/vaccines-and-immunization#tab=tab_1 (accessed on 23 January 2023).
- Ehreth, J. The global value of vaccination. Vaccine 2003, 21, 596–600. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Immunization Coverage; World Health Organization: Geneva, Switzerland, 2023; Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 23 January 2023).
- Castrejon, M.M.; Leal, I.; de Jesus Pereira Pinto, T.; Guzman-Holst, A. The impact of COVID-19 and catch-up strategies on routine childhood vaccine coverage trends in Latin America: A systematic literature review and database analysis. Hum. Vaccines Immunother. 2022, 18, 2102353. [Google Scholar] [CrossRef] [PubMed]
- Ajejas Bazan, M.J.; Del Gallego-Lastra, R.; Marques-Vieira, C.M.A.; Lopez-Lopez, C.; Dominguez-Fernandez, S.; Rico-Blazquez, M.; Perez-Rivas, F.J. Vaccine Coverage against Influenza and SARS-CoV-2 in Health Sciences Students during COVID-19 Pandemic in Spain. Vaccines 2022, 10, 159. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Mukandavire, C.; Cucunuba, Z.M.; Echeverria Londono, S.; Abbas, K.; Clapham, H.E.; Jit, M.; Johnson, H.L.; Papadopoulos, T.; Vynnycky, E.; et al. Estimating the health impact of vaccination against ten pathogens in 98 low-income and middle-income countries from 2000 to 2030: A modelling study. Lancet 2021, 397, 398–408. [Google Scholar] [CrossRef]
- Uyeki, T.M. High-risk Groups for Influenza Complications. JAMA 2020, 324, 2334. [Google Scholar] [CrossRef]
- World Health Organization. Global Vaccine Action Plan 2011–2020; World Health Organization: Geneva, Switzerland, 2011; Available online: https://www.who.int/publications/i/item/global-vaccine-action-plan-2011-2020 (accessed on 25 February 2023).
- Larson, A.; Skolnik, A.; Bhatti, A.; Mitrovich, R. Addressing an urgent global public health need: Strategies to recover routine vaccination during the COVID-19 pandemic. Hum. Vaccines Immunother. 2022, 18, 1975453. [Google Scholar] [CrossRef]
- Gianfredi, V.; D’Ancona, F.; Maraglino, F.; Cenci, C.; Iannazzo, S. Polio and measles: Reasons of missed vaccination in Italy, 2015-2017. Ann. Ig. 2019, 31, 191–201. [Google Scholar]
- Gianfredi, V.; Moretti, M.; Fusco Moffa, I. Burden of measles using disability-adjusted life years, Umbria 2013-2018. Acta Bio Med. 2020, 91, 48–54. [Google Scholar] [CrossRef]
- Stefanizzi, P.; De Nitto, S.; Spinelli, G.; Lattanzio, S.; Stella, P.; Ancona, D.; Dell’Aera, M.; Padovano, M.; Soldano, S.; Tafuri, S.; et al. Post-Marketing Active Surveillance of Adverse Reactions Following Influenza Cell-Based Quadrivalent Vaccine: An Italian Prospective Observational Study. Vaccines 2021, 9, 456. [Google Scholar] [CrossRef]
- Sultana, J.; Caci, G.; Hyeraci, G.; Albano, L.; Gianfredi, V. COVID-19 mRNA vaccine safety, immunogenicity, and effectiveness in a hospital setting: Confronting the challenge. Intern. Emerg. Med. 2022, 17, 325–327. [Google Scholar] [CrossRef]
- Vigezzi, G.P.; Lume, A.; Minerva, M.; Nizzero, P.; Biancardi, A.; Gianfredi, V.; Odone, A.; Signorelli, C.; Moro, M. Safety surveillance after BNT162b2 mRNA COVID-19 vaccination: Results from a cross-sectional survey among staff of a large Italian teaching hospital. Acta Bio Med. 2021, 92, e2021450. [Google Scholar] [CrossRef]
- Gianfredi, V.; Paoloni, M.C.; Villarini, M.; Moretti, M. Active surveillance evaluation of anti-HPV vaccine adverse events in Umbria region. Clin. Ter. 2017, 168, e327–e332. [Google Scholar] [CrossRef]
- Verhees, R.A.F.; Thijs, C.; Ambergen, T.; Dinant, G.J.; Knottnerus, J.A. Influenza vaccination in the elderly: 25 years follow-up of a randomized controlled trial. No impact on long-term mortality. PLoS ONE 2019, 14, e0216983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galagali, P.M.; Kinikar, A.A.; Kumar, V.S. Vaccine Hesitancy: Obstacles and Challenges. Curr. Pediatr. Rep. 2022, 10, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Italian Ministry of Health. National Immunization Plan 2017–2019; Italian Ministry of Health: Rome, Italy, 2017; Available online: https://www.gazzettaufficiale.it/eli/id/2017/02/18/17A01195/sg (accessed on 23 January 2023).
- World Health Organization. Strategic Advisory Group of Experts on Immunization (SAGE). Available online: https://www.who.int/groups/strategic-advisory-group-of-experts-on-immunization (accessed on 25 February 2023).
- Centers for Disease Control and Prevention. Recommended Vaccines for Healthcare Workers; National Center for Immunization and Respiratory Diseases: Atlanta, GA, USA, 2016. Available online: https://www.cdc.gov/vaccines/adults/rec-vac/hcw.html (accessed on 23 January 2023).
- Guillari, A.; Polito, F.; Pucciarelli, G.; Serra, N.; Gargiulo, G.; Esposito, M.R.; Botti, S.; Rea, T.; Simeone, S. Influenza vaccination and healthcare workers: Barriers and predisposing factors. Acta Bio Med. 2021, 92, e2021004. [Google Scholar] [CrossRef]
- Gallone, M.S.; Infantino, V.; Ferorelli, D.; Stefanizzi, P.; De Nitto, S.; Tafuri, S. Vaccination coverage in patients affected by chronic diseases: A 2014 cross-sectional study among subjects hospitalized at Bari Policlinico General Hospital. Am. J. Infect. Control 2018, 46, e9–e11. [Google Scholar] [CrossRef]
- Italian Ministry of Health. Influenza Vaccination Coverage. 2022. Available online: https://www.salute.gov.it/portale/influenza/dettaglioContenutiInfluenza.jsp?lingua=italiano&id=679&area=influenza&menu=vuoto (accessed on 25 February 2023).
- Alicino, C.; Iudici, R.; Barberis, I.; Paganino, C.; Cacciani, R.; Zacconi, M.; Battistini, A.; Bellina, D.; Di Bella, A.M.; Talamini, A.; et al. Influenza vaccination among healthcare workers in Italy. Hum. Vaccines Immunother. 2015, 11, 95–100. [Google Scholar] [CrossRef] [Green Version]
- Barbadoro, P.; Marigliano, A.; Di Tondo, E.; Chiatti, C.; Di Stanislao, F.; D’Errico, M.M.; Prospero, E. Determinants of influenza vaccination uptake among Italian healthcare workers. Hum. Vaccines Immunother. 2013, 9, 911–916. [Google Scholar] [CrossRef]
- Ogliastro, M.; Borghesi, R.; Costa, E.; Fiorano, A.; Massaro, E.; Sticchi, L.; Domnich, A.; Tisa, V.; Durando, P.; Icardi, G.; et al. Monitoring influenza vaccination coverage among healthcare workers during the COVID-19 pandemic: A three-year survey in a large university hospital in North-Western Italy. J. Prev. Med. Hyg. 2022, 63, E405–E414. [Google Scholar] [CrossRef]
- Gianfredi, V.; Dallagiacoma, G.; Provenzano, S.; Santangelo, O.E. Factors predicting health science students’ willingness to be vaccinated against seasonal flu during the next campaign. Ann. Ist. Super. Sanita 2019, 55, 209–216. [Google Scholar] [CrossRef]
- Amodio, E.; Tramuto, F.; Maringhini, G.; Asciutto, R.; Firenze, A.; Vitale, F.; Costantino, C.; Calamusa, G. Are medical residents a “core group” for future improvement of influenza vaccination coverage in health-care workers? A study among medical residents at the University Hospital of Palermo (Sicily). Vaccine 2011, 29, 8113–8117. [Google Scholar] [CrossRef] [PubMed]
- Voglino, G.; Barbara, A.; Dallagiacoma, G.; Santangelo, O.E.; Provenzano, S.; Gianfredi, V. Do Degree Programs Affect Health Profession Students’ Attitudes and Opinions Toward Vaccinations? An Italian Multicenter Study. Saf. Health Work 2022, 13, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Rosental, H.; Shmueli, L. Integrating Health Behavior Theories to Predict COVID-19 Vaccine Acceptance: Differences between Medical Students and Nursing Students. Vaccines 2021, 9, 783. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.; Kaur, M.; Kaur, R.; Grover, A.; Nash, D.; El-Mohandes, A. Predictors of COVID-19 Vaccine Acceptance, Intention, and Hesitancy: A Scoping Review. Front. Public Health 2021, 9, 698111. [Google Scholar] [CrossRef]
- Qiu, X.; Bailey, H.; Thorne, C. Barriers and Facilitators Associated With Vaccine Acceptance and Uptake Among Pregnant Women in High Income Countries: A Mini-Review. Front. Immunol. 2021, 12, 626717. [Google Scholar] [CrossRef]
- Gonzalez-Block, M.A.; Portillo, S.P.D.; Laguna, J.A.; Comes, Y.; Crocco, P.; Fachel-Leal, A.; Noboa, L.; Knauth, D.R.; Rodriguez-Zea, B.; Ruoti, M.; et al. Barriers and facilitators to influenza vaccination observed by officers of national immunization programs in South America countries with contrasting coverage rates. Cad. Saude Publica 2022, 38, e00045721. [Google Scholar] [CrossRef]
- Gianfredi, V.; Nucci, D.; Salvatori, T.; Orlacchio, F.; Villarini, M.; Moretti, M.; PErCEIVE in Umbria Study Group. “PErCEIVE in Umbria”: Evaluation of anti-influenza vaccination’s perception among Umbrian pharmacists. J. Prev. Med. Hyg. 2018, 59, E14–E19. [Google Scholar] [CrossRef]
- Lorini, C.; Collini, F.; Galletti, G.; Ierardi, F.; Forni, S.; Gatteschi, C.; Gemmi, F.; Stacchini, L.; Papini, S.; Velpini, B.; et al. Vaccine Literacy and Source of Information about Vaccination among Staff of Nursing Homes: A Cross-Sectional Survey Conducted in Tuscany (Italy). Vaccines 2022, 10, 682. [Google Scholar] [CrossRef]
- Al-Metwali, B.Z.; Al-Jumaili, A.A.; Al-Alag, Z.A.; Sorofman, B. Exploring the acceptance of COVID-19 vaccine among healthcare workers and general population using health belief model. J. Eval. Clin. Pract. 2021, 27, 1112–1122. [Google Scholar] [CrossRef]
- Galanakis, E.; Jansen, A.; Lopalco, P.L.; Giesecke, J. Ethics of mandatory vaccination for healthcare workers. Eurosurveillance 2013, 18, 20627. [Google Scholar] [CrossRef] [Green Version]
- Cedrone, F.; Santangelo, O.E.; Provenzano, S.; Alagna, E.; Dellagiacoma, G.; D’Ambrosio, A.; Voglino, G.; Gianfredi, V. Attitude of students of health professions towards a health care workers’ mandatory vaccination: A multi-center cross-sectional survey. G. Ital. Med. Lav. Ergon. 2020, 42, 87–93. [Google Scholar] [PubMed]
- Santangelo, O.E.; Cedrone, F.; Gentile, L.; Provenzano, S.; Dallagiacoma, G.; Armetta, F.; Gianfredi, V. Reasons behind flu vaccine acceptance and suggested interventions to promote flu vaccination acceptance among healthcare workers. J. Infect. Prev. 2021, 22, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, O.E.; Di Gaspare, F.; Provenzano, S.; Ferrucci, G.; Gianfredi, V. Opinions, attitudes and knowledge of Italian health science university students on mandatory vaccinations: A cross-sectional study. Ig. Sanita Pubblica 2019, 75, 283–295. [Google Scholar]
- Dini, G.; Toletone, A.; Sticchi, L.; Orsi, A.; Bragazzi, N.L.; Durando, P. Influenza vaccination in healthcare workers: A comprehensive critical appraisal of the literature. Hum. Vaccines Immunother. 2018, 14, 772–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tafuri, S.; Fortunato, F.; Gallone, M.S.; Stefanizzi, P.; Calabrese, G.; Boccalini, S.; Martinelli, D.; Prato, R. Systematic causality assessment of adverse events following HPV vaccines: Analysis of current data from Apulia region (Italy). Vaccine 2018, 36, 1072–1077. [Google Scholar] [CrossRef]
- Gray, G.; Cooper, J. An evaluation of influenza vaccine uptake in UK medical students. Occup. Med. 2021, 71, 105–108. [Google Scholar] [CrossRef]
- Gandhi, S.; Harris Bozer, A. Factors associated with influenza vaccine noncompliance at a Rural Texas University. J. Am. Coll. Health 2022, 70, 1570–1576. [Google Scholar] [CrossRef]
- Gianfredi, V.; Grisci, C.; Nucci, D.; Parisi, V.; Moretti, M. Communication in health. Recenti. Prog. Med. 2018, 109, 374–383. [Google Scholar] [CrossRef]
- Gianfredi, V.; Odone, A.; Fiacchini, D.; Rosselu, R.; Battista, T.; Signorelli, C. Trust and reputation management, branding, social media management nelle organizzazioni sanitarie: Sfide e opportunity per la comunita igienistica italiana. J. Prev. Med. Hyg. 2019, 60, E108–E109. [Google Scholar]
- Trucchi, C.; Costantino, C.; Restivo, V.; Bertoncello, C.; Fortunato, F.; Tafuri, S.; Amicizia, D.; Martinelli, D.; Paganino, C.; Piazza, M.F.; et al. Immunization Campaigns and Strategies against Human Papillomavirus in Italy: The Results of a Survey to Regional and Local Health Units Representatives. BioMed Res. Int. 2019, 2019, 6764154. [Google Scholar] [CrossRef] [Green Version]
- Ali, I. Impact of COVID-19 on vaccination programs: Adverse or positive? Hum. Vaccines Immunother. 2020, 16, 2594–2600. [Google Scholar] [CrossRef] [PubMed]
- Chan, N.N.; Ong, K.W.; Siau, C.S.; Lee, K.W.; Peh, S.C.; Yacob, S.; Chia, Y.C.; Seow, V.K.; Ooi, P.B. The lived experiences of a COVID-19 immunization programme: Vaccine hesitancy and vaccine refusal. BMC Public Health 2022, 22, 296. [Google Scholar] [CrossRef] [PubMed]
- Kricorian, K.; Civen, R.; Equils, O. COVID-19 vaccine hesitancy: Misinformation and perceptions of vaccine safety. Hum. Vaccines Immunother. 2022, 18, 1950504. [Google Scholar] [CrossRef] [PubMed]
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 337–348. [Google Scholar] [CrossRef]
- Cella, P.; Voglino, G.; Barberis, I.; Alagna, E.; Alessandroni, C.; Cuda, A.; D’Aloisio, F.; Dallagiacoma, G.; De Nitto, S.; Di Gaspare, F.; et al. Resources for assessing parents’ vaccine hesitancy: A systematic review of the literature. J. Prev. Med. Hyg. 2020, 61, E340–E373. [Google Scholar] [CrossRef]
- Meadows, K.A. So you want to do research? 5: Questionnaire design. Br. J. Commun. Nurs. 2003, 8, 562–570. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Flu Vaccination Previous Year | Flu Vaccination Following Year | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | Total n (%) | No (%) | Yes (%) | p-Value | No (%) | Yes (%) | p-Value | |
| Gender | Female | 2132 (68.09) | 1908 (89.49) | 224 (10.51) | 0.096 | 1381 (64.77) | 751 (35.23) | 0.588 |
| Male | 999 (31.91) | 874 (87.49) | 125 (12.51) | 657 (65.77) | 342 (34.23) | |||
| Age | Mean ± SD | 23.41 ± 3.69 | 23.31 ± 3.64 | 24.23 ± 3.94 | <0.001 | 23.31 ± 3.63 | 23.59 ± 3.78 | 0.025 |
| Degree Program | Medicine and Surgery | 1219 (38.93) | 1036 (84.99) | 183 (15.01) | <0.001 | 737 (60.46) | 482 (39.54) | <0.001 |
| Other | 1912 61.07) | 1746 (91.32) | 166 (8.68) | 1301 (68.04) | 611 (31.96) | |||
| Main source of information on vaccines | Institutional webpages | 324 (10.35) | 269 (83.02) | 55 (16.98) | <0.001 | 181 (55.86) | 143 (44.14) | <0.001 |
| Scientific data | 810 (25.87) | 670 (82.71) | 140 (17.28) | 449 (55.43) | 361 (44.57) | |||
| Governmental regulation | 641 (20.47) | 595 (92.82) | 46 (7.18) | 452 (70.51) | 189 (28.76) | |||
| Blogs/social networks | 299 (9.55) | 274 (91.64) | 25 (8.36) | 213 (71.24) | 86 (28.76) | |||
| I do not care about | 1057 (33.76) | 974 (92.15) | 83 (7.85) | 743 (70.29) | 314 (29.71) | |||
| Getting Influenza Vaccine during the Previous Year | ||||
|---|---|---|---|---|
| aOR | 95% CI | p-Value | ||
| Gender | Female | 1 | ||
| Male | 0.95 | 0.81–1.11 | 0.501 | |
| Age | As the unit increases | 1.02 | 1.01–1.04 | 0.044 |
| Degree Course | Medicine and Surgery | 1 | ||
| Other | 0.72 | 0.62–0.84 | <0.001 | |
| Main source of information on vaccine | Institutional webpages | 1 | ||
| Scientific data | 1.02 | 0.79–1.33 | 0.859 | |
| Governmental regulation | 0.53 | 0.40–0.71 | <0.001 | |
| Blogs/social networks | 0.52 | 0.37–0.73 | <0.001 | |
| I do not care about | 0.54 | 0.42–0.70 | <0.001 | |
| Main reason for taking the vaccine ^ | I consider myself as a high-risk subject | 1 | ||
| To avoid infecting family members and general population | 0.62 | 0.45–0.86 | 0.004 | |
| To avoid infecting patients | 0.37 | 0.26–0.53 | <0.001 | |
| Other | 0.28 | 0.13–0.65 | 0.003 | |
| Main reason for not taking the vaccine * | Flu vaccine is not safe and effective | 0.03 | 0.01–0.09 | <0.001 |
| Flu is not a severe infection | 0.01 | 0.01–0.02 | <0.001 | |
| I consider myself irrelevant in spreading influenza to family members and general population | 0.01 | 0.01–0.04 | <0.001 | |
| I consider myself irrelevant in spreading influenza to patients | 0.02 | 0.01–0.06 | <0.001 | |
| Getting Influenza Vaccine during the Following Campaign | ||||
|---|---|---|---|---|
| Independent Variables | aOR | 95% CI | p-Value | |
| Gender | Female | 1 | ||
| Male | 1.18 | 0.94–1.50 | 0.158 | |
| Age | As the unit increases | 1.06 | 1.03–1.09 | <0.001 |
| Degree Course | Medicine and Surgery | 1 | ||
| Other | 0.58 | 0.46–0.73 | <0.001 | |
| Main source of information on vaccine | Institutional webpages | 1 | ||
| Scientific data | 1.03 | 0.73–1.46 | 0.855 | |
| Governmental regulation | 0.41 | 0.27–0.62 | <0.001 | |
| Blogs/social networks | 0.48 | 0.29–0.80 | <0.001 | |
| I do not care about | 0.43 | 0.30–0.62 | <0.001 | |
| Main reason for taking the vaccine ^ | I consider myself as a high-risk subject | 1 | ||
| To avoid infecting family members and general population | 44.56 | 16.38–121.22 | <0.001 | |
| To avoid infecting patients | 16.56 | 5.95–46.05 | <0.001 | |
| Other | 13.22 | 4.72–37.08 | <0.001 | |
| Main reason for not taking the vaccine * | Flu vaccine is not safe and effective | 0.22 | 0.13–0.35 | <0.001 |
| Flu is not a severe infection | 0.17 | 0.14–0.21 | <0.001 | |
| I consider myself irrelevant in spreading influenza to family members and general population | 0.41 | 0.30–0.57 | <0.001 | |
| I consider myself irrelevant in spreading influenza to patients | 0.45 | 0.29–0.68 | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stefanizzi, P.; Provenzano, S.; Santangelo, O.E.; Dallagiacoma, G.; Gianfredi, V. Past and Future Influenza Vaccine Uptake Motivation: A Cross-Sectional Analysis among Italian Health Sciences Students. Vaccines 2023, 11, 717. https://doi.org/10.3390/vaccines11040717
Stefanizzi P, Provenzano S, Santangelo OE, Dallagiacoma G, Gianfredi V. Past and Future Influenza Vaccine Uptake Motivation: A Cross-Sectional Analysis among Italian Health Sciences Students. Vaccines. 2023; 11(4):717. https://doi.org/10.3390/vaccines11040717
Chicago/Turabian StyleStefanizzi, Pasquale, Sandro Provenzano, Omar Enzo Santangelo, Giulia Dallagiacoma, and Vincenza Gianfredi. 2023. "Past and Future Influenza Vaccine Uptake Motivation: A Cross-Sectional Analysis among Italian Health Sciences Students" Vaccines 11, no. 4: 717. https://doi.org/10.3390/vaccines11040717