
COVID-19 Disease in Under-5 Children: Current Status and Strategies for Prevention including Vaccination

 ,
, 
Abstract
:1. Introduction
2. Epidemiology of COVID-19
2.1. Epidemiologic Patterns across Age Groups
2.2. Epidemiologic Patterns Witnessed across Time Periods
3. Pathophysiology of Severe SARS-CoV-2 Disease
4. Mechanisms Protecting Neonates and Children
- (i)
- ACE-2 receptor expression: The SARS-CoV-2 attaches to the ACE-2 receptor in the epithelium via the S-protein, similar to SARS-CoV-1 [79]. ACE-2 is found in multiple sites, including epithelial cells of the oral, nasopharyngeal, and oropharyngeal mucosal epithelium; alveolar epithelium; endothelium of blood vessels and the heart; renal tubules; and small intestinal enterocytes [80]. Virus entry into the cells is facilitated by transmembrane protease serine 2 (TMPRSS2), and cathepsin L-mediated cleavage of ACE-2 [81]. Wang et al. studied gene expression in various age groups and noted that a higher proportion of alveolar epithelial cells expressed ACE2 and TMPRSS2 in adult lungs [82]. ACE-2 expression was deficient in normal newborn lungs. Additionally, very few cells express both ACE-2 and TMPRSS2 (double-positive cells) in young children [54,83]. This could explain the lower susceptibility of neonates; however, there is conflicting data regarding this topic. ACE-2 receptors decrease in the elderly population, which has a higher susceptibility to severe COVID-19 disease [84].
- (ii)
- Placental barrier: Epidemiologic studies have ascertained that transplacental transmission from an infected mother to her baby is possible but rare [10,17,48,49,50]. The continuous cell layer over the placental surface and dense actin filament network over the brush border serve as a physical barrier to the transmission of pathogens. In addition, the placenta also secretes type 3 interferon miRNAs, which act as antiviral compounds [85,86]. None of the villous stromal cells or Hoffbauer cells (placental macrophages) express ACE2; also, expression of TMPRSS2 is weak in the syncytiotrophoblast. This may explain the low risk of congenital infection in SARS-CoV-2 disease. A study by Algarroba et al. [51] demonstrated the localization of corona virions in the placental syncytiotrophoblast of the placenta in a COVID-19-positive mother, although the neonate tested negative for COVID-19. Similar reports suggest that symptomatic neonatal infection remains uncommon despite placental infection [87,88].
- (iii)
- Immature immune system: Immune responses in fetal life are curbed so that they can co-exist with the semi-allogenic maternal immune system. In the neonate, the majority of T cells are immature. CD45RA, a marker expressed on naive T cells, is found in 90% of cord blood T cells, compared to 40% of adult T cells [58,89]. A large proportion of fetal CD4 cells develop into CD25+FOXP3+ regulatory T cells (T-reg cells). T-reg cells play an essential role in the downregulation of immune responses and promote tolerance [90,91]. The monocyte-macrophage system during infancy has an impaired ability to produce inflammatory cytokines [92]. The benefits of immune tolerance have been well described in viral infections such as hepatitis B (HBV), where acute hepatitis is rarely seen in the neonatal period [93].
- (iv)
- Maternal immunoglobulins: Maternal immunoglobulins are crucial in the first few months after birth. In a case series by Zeng et al., including mothers with recent COVID-19 disease, 5 out of 6 mothers had high IgG titers > 50 AU/mL (reference range < 10 AU/mL). All five neonates born to these mothers had IgG titers > 50 AU/mL but lower than maternal titers, suggesting transplacental transfer of antibodies. Two infants also had positive IgM titers, suggesting possible fetal antibody production 95. Other studies have also supported the mother-to-child transmission of COVID-19 antibodies [96,97,98]. The IgG transplacental transfer ratio is higher when the first maternal-positive PCR is 60–180 days before delivery compared with <60 days [98]. Typically, maternal antibodies decline rapidly after the first 3–6 months of life; however, there is limited data on how long the maternal COVID-19 IgG antibodies confer protection to the newborn.
- (v)
- Human Milk: Bioactive and cellular components of breastmilk together modulate the maturation of the neonatal immune system [99,100]. Pace and colleagues tested 37 milk samples and 70 breast swabs from 18 women recently diagnosed with COVID-19. SARS-CoV-2-specific IgA and IgG antibodies were found in all milk samples. No milk samples detected SARS-CoV-2 RNA [63]. Other reports have also shown the presence of secretory IgA and IgG in the breastmilk of SARS-CoV-2-infected mothers [64,65,101]. SARS-CoV-2 RNA was found in several breast swabs, highlighting the importance of continued efforts towards hygiene measures [63]. Based on current evidence, the benefits of breastmilk feeding far outweigh the theoretical risk of virus transmission via breastmilk.
- (vi)
- (vii)
- Melatonin: Melatonin is anti-inflammatory and can protect against ARDS and hemorrhagic shock during viral infections [103,104]. Higher melatonin levels may contribute to milder disease course in young children. Results from the ongoing randomized trials to test the efficacy of melatonin as a prophylactic agent are awaited [73,74].
- (viii)
- Live vaccine effect: Live vaccines such as BCG can have immunomodulatory properties extending beyond the usual protection against the target pathogens [105,106,107]. Epidemiologic data suggest variances in the prevalence and severity of COVID-19 disease in countries with different BCG vaccination policies [107,108,109]. Clinical trials testing this hypothesis are ongoing [78]. However, data from the second pandemic wave suggests high prevalence and mortality even in countries that give routine BCG vaccination [110,111].
- (ix)
- Microbiota: Microbiota plays a crucial role in immune regulation and inflammation. Studies have reported differences in microbiota between patients infected with COVID-19 and healthy adults [67,68]. A pilot study including 15 patients with COVID-19 infection showed enrichment of opportunistic pathogens (Streptococcus, Rothia, Clostridium, and Actinomyces) and depletion of beneficial commensals (Faecalibacterium, Bacteroides) at all timepoints during hospitalization [68]. The summary of fundamental mechanisms that may possibly confer protection to young children from COVID-19 disease is listed in Figure 2.
5. Strategies for Preventing Perinatal COVID-19
5.1. General Measures
5.2. COVID-19 Vaccines
5.2.1. COVID-19 Vaccines Applicable during Pregnancy
- (i)
- Vaccine type: Vaccines that have the most published data regarding their use in pregnancy are mRNA vaccines such as Pfizer-BioNTech’s COVID-19 vaccine and Moderna’s COVID-19 vaccine, and recombinant vector-based vaccines such as Oxford/AstraZeneca and Johnson & Johnson’s/Janssen. Other vaccines such as the protein subunit vaccine (Novavax) and inactivated-virus vaccine (Covaxin) are also considered safe in pregnancy; however, there is limited clinical data in this regard [158,159,160,161,162,163]. Current recommendations suggest that the COVID-19 vaccine, including the primary series or booster, can be given in any trimester along with routine vaccines during pregnancy, such as influenza and Tdap [153,156,158].
- (ii)
- Vaccine Efficacy—benefits to newborns: There is adequate evidence to support the claim that pregnant women produce a robust antibody response post-vaccination [164,165]. Vaccine-induced antibody titers may be similar to those produced in non-pregnant women, with antibody production starting two weeks from the first dose [166]. Benefits of the vaccine for the mother include reduced risk of infection, lower maternal hospitalization, and need for intensive care admission [167,168]. Vaccination in pregnant women also benefits the neonate due to the passive transfer of antibodies. The placental transfer of antibodies depends on the maternal antibody titer, vaccination timing, and delivery interval. A recent prospective cohort study found that 57% of infants with detectable antibodies against COVID-19 at six months of age were born to vaccinated pregnant females, compared to only 8% of infants with detectable antibodies in infants born to individuals who had COVID-19 illness during pregnancy [166]. Studies have shown that vaccination with the mRNA COVID-19 vaccine series during pregnancy may protect babies up to 6 months of age from severe COVID-19 disease and hospitalization [156]. Third trimester (27–31 weeks) vaccination is associated with higher neonatal anti-SARS-CoV-2 antibody levels, and the early third trimester may be the optimal timing for a booster dosing [169]. Passive immunity can protect neonates against severe COVID-19 disease; however, studies are still underway to determine exactly how these antibodies work [170,171].
- (iii)
- Vaccine Safety—for mother and fetus: Data from vaccine safety monitoring systems have not found any safety concerns after mRNA COVID-19 vaccination during pregnancy or lactation for females or their babies. Observational data from various countries have shown that vaccination with the mRNA COVID-19 vaccine during pregnancy before 20 weeks was not associated with an increased risk of complications, including preterm delivery, stillbirth, postpartum sepsis, or postpartum hemorrhage [153,154,172,173]. There was no association between COVID-19 vaccination in pregnant females with congenital anomalies [174]. A recently published systematic review suggested a possible reduction in the risk of stillbirth in the vaccinated population by 15% (pooled OR 0.85; 95% CI 0.73–0.99). The risk of adverse maternal outcomes such as spontaneous abortion, placental abruption, postpartum hemorrhage, increased maternal mortality, intensive care unit admission, or neonatal adverse outcomes such as preterm birth, fetal growth restriction, and NICU admission (p > 0.05 for all) was not increased in vaccinated women [160].
- (iv)
- Side effects: The side effects related to the COVID-19 vaccine during pregnancy include injection site pain, myalgia, headache, and fatigue, which are similar to those described in the non-pregnant population [153,175]. Prospective studies comparing vaccinated pregnant women matched with vaccinated female non-pregnant controls have reported minor differences in the reporting of side effects in the two groups, but the overall frequency of complaints was similar [176,177]. COVID-19 vaccination is a safe and effective method for reducing disease burden and severity in pregnant women and their babies.
5.2.2. COVID-19 Vaccines Applicable to Young Children
- (i)
- 6 m–5 years age: Two doses of 25 µg (0.25 mL) 4 weeks apart. Booster dose at least 2 months after the primary series (updated/bivalent).
- 6–11 years age: Two doses of 50 µg (0.25 mL) 4–8 weeks apart. Booster dose at least 2 months after the primary series dose (updated/bivalent).
- The Pfizer-BioNTech BNT162b2 vaccine schedule:
- 6 m–4 years age: Three doses of 3 µg (0.2 mL) first and second dose 3–8 weeks apart; third dose 8 weeks after the second dose. Third dose can be updated/bivalent vaccine. No booster dose recommended.
- 5–11 years age: Two doses of 10 µg (0.2 mL) 4–8 weeks apart. Booster dose at least two months after the primary series (updated/bivalent).
- (ii)
- Vaccine Efficacy: Observational studies post-introduction of COVID-19 vaccines in children have reported variable effectiveness of the primary series, ranging between 25% and 50% [179,180,181,182]. Unvaccinated children have two times higher cumulative hospitalization rates when compared to vaccinated children [183]. A nationwide cohort from Chile, including 490,694 children aged 3–5 years, showed vaccine efficacy of 38% (95% CI, 37–40) against symptomatic COVID-19, 65% (95% CI, 50–75) against hospitalization, and 69% (95% CI, 19–88) against ICU admission [184]. Moreover, data in the adolescent age group have shown that two doses of mRNA vaccine has an effectiveness of 91% for MISC-C [185]. In a large observational study including nearly 200,000 children and adolescents using the database in Israel, Amir and colleagues estimated rates of confirmed SARS-CoV-2 infection according to Pfizer-BioNTech vaccination status in children aged 5–15 years. The infection rates were more than two times lower in children after the second vaccine dose compared with same-aged children after the first dose. Furthermore, the infection rates in adolescents were lower 2–8 weeks after the booster dose, compared to 3–7 days after booster dose [186]. Thus, booster doses in adolescents increase protection against infection.
- (iii)
- Vaccine safety: Children who received the Pfizer-BioNTech COVID-19 vaccine reported mostly mild local (86.2%) and systemic (66.6%) reactions; no other serious adverse events were found to be associated with vaccination [187]. Febrile seizures post-COVID-19 vaccines were rarely reported in young children, and incidents happened with similar rates for both mRNA vaccines (Pfizer and Moderna COVID-19) [188]. Severe allergic reactions such as anaphylaxis are infrequent in children post-COVID-19 vaccination [189]. Among children 5–11 years, there were no cases of myocarditis. Rare cases of myocarditis and pericarditis have been reported after vaccination in older children and adolescents who received the mRNA vaccine. In these reports of myocarditis, the incidence was found to be higher after the second dose of the mRNA vaccine (Pfizer-BioNTech) [190]. Thrombosis with thrombocytopenia syndrome (TTS) has been reported in young adults following adenoviral-vector vaccines; however, there are no such reports in children [191].
- (iv)
- Side effects: According to an extensive online survey, around 50% of children reported side effects post-vaccination. The most commonly reported symptoms were injection site pain, fatigue, fever, and headache. There were no serious adverse events, and symptoms improved within 1–3 days after vaccination [192]. Another study from Saudi Arabia reported that 60% of adolescents had at least one side effect post-vaccination. The common side effects were injection site pain, fever, fatigue, headache, and nausea. Side effects were more common after the second dose [193]. The side-effect profile of the COVID-19 vaccine is mild and similar to other flu vaccines. Evolving observational reports after vaccination in younger children and infants will add to the safety data regarding COVID-19 vaccines.
5.2.3. Knowledge Gaps and Controversies Related to Pediatric COVID-19 Vaccination
- (i)
- Vaccine dose and interval: The lower antigen doses suggested for the pediatric population are based on small trials. A post-implementation trial of the 10 µg dose of Pfizer-BioNTech vaccine in 5–11-year-old children showed an effectiveness of less than 50%, with immunity rapidly waning within 3 months after vaccination [180]. The dose of 3 µg recommended for children aged 6 months to 5 years is mainly based on tolerability data, with limited evidence on efficacy [178]. Regarding the interval between two doses, studies in adults have evaluated different COVID-19 vaccine regimens and their immunological and epidemiological impact. Reports suggest that delaying the second vaccine dose up to 12 weeks may improve longer-term immunity [194,195,196]. However, data regarding optimal dosing and intervals in young children are lacking, and recommendations are extrapolated from adult and adolescent data.
- (ii)
- Age cutoff: The lower age cutoff for the primary vaccination series varies between countries, ranging from 6 months to 12 years. This is related to the paucity of data regarding vaccine safety and effectiveness in younger children, optimal dosage schedule, and lower risk of severe illness. The Center for Disease Control and Prevention (CDC) in America recommends universal COVID-19 vaccination above the age of 6 months [178], China provides vaccination to children above 3 years of age [197], Australia recommends routine COVID-19 vaccination above 5 years [198] or children between 6 months and 5 years meeting the high-risk criteria, whereas in many countries such as India only children above 12 years are eligible for the vaccine [199].
- (iii)
- Mixed vaccine strategy: A mixed-vaccine strategy was initially proposed in view of limited vaccine supplies. A recently published single-blinded, randomized, non-inferiority trial from the UK aimed to determine the safety, immunogenicity, and reactogenicity of heterologous primary vaccination including mRNA, viral vector, and protein adjuvant vaccine, included 1072 adults and found that heterologous second dosing with m1273 (Moderna) increases systemic reactogenicity compared with homologous schedules [200]. Ongoing trials are being carried out in the adult population to explore heterologous vaccination; however, extrapolating this to the pediatric population is probably not justified [201]. For the primary vaccination series in adults and for all doses in young children, using the same product and brand is preferable [178].
- (iv)
- Immunocompromised children: Due to the complex pathogenesis of infection and altered immune response, immunocompromised children are a unique cohort at higher risk of severe COVID-19 disease. The role of the COVID-19 vaccine is crucial in this cohort. Although the initial COVID-19 vaccine trials excluded immunocompromised children, the general expert consensus recommends that non-live vaccines can be safely administered to such patients [202]. The CDC also suggests that immunocompromised children must receive an additional primary dose of the COVID-19 vaccine as they may not respond adequately to the standard two-dose series. The Australian Technical Advisory Group on Immunization has identified children at higher risk of severe COVID-19 disease such as those with primary/secondary immunodeficiency, use of immunosuppressive drugs, bone marrow transplant recipients, complex cyanotic heart disease, chronic lung disease, and type 1 diabetes mellitus [203]. However, many areas need further evaluation, such as optimal dosage, timing of vaccination, and consideration regarding the withholding of immunosuppressive medications after vaccination [204].
- (v)
- Variants of concern: Studies have shown that mRNA vaccines effectively reduce infection and transmission of SARS-CoV-2 variants of concern (VOC), such as the Alpha, Beta, and Delta variants [205,206]. The Omicron variant described in November 2021 contains around 50 mutations, 32 of which are located in spike protein, which is the primary target for mRNA vaccines. This creates an unstable binding affinity of the receptor domain to ACE2 receptors, hence making mRNA vaccines less effective [207,208]. Since the immune response in children is very much distinct from the adult population, it is necessary to demonstrate VOC susceptibility to neutralization antibodies in the pediatric population. Data published from Hong Kong suggested that children had lower neutralizing antibody titers against the Omicron variant than those against the ancestral viral strains [209]. Although booster doses may improve the neutralizing antibody levels for VOC, they remain lower than those for the original strain [210]. These findings suggest that the pediatric age group may be more susceptible to vaccine breakthrough infections caused by Omicron or a newer VOC. Repeated mutations and the appearance of new VOC can affect vaccine efficacy in children and warrant continuous surveillance of the risk–benefit balance [211].
5.2.4. Ethical Issues Related to COVID-19 Vaccine
- (i)
- Vaccine Hesitancy: Early reports suggested that a significant portion of the population including healthcare workers were hesitant to take vaccination [212,213]. There are noticeable racial/ethnic differences in the likelihood of vaccine uptake in the general population [214]. Current immunization regimes have shown modest efficacy and rapidly waning protection in 5–11-year-old children post-vaccination [180]. An online survey of 411 female guardians of children aged 1–4 years reported determinants of COVID-19 vaccine hesitancy across diverse ethnic and geographic backgrounds. Only 31% of parents expressed their intention to vaccinate their child; 23% of parents were unsure; and 46% intended not to vaccinate. The main reasons for vaccine hesitancy were concerns about side effects in young children, the hasty nature of vaccine approval, and distrust in pharmaceutical companies. For parents who were unsure about vaccination, there was a belief that children were not susceptible to infection and that the vaccine was not effective against new variants. Other published studies have also reported that lack of high-quality clinical evidence, accelerated vaccine approvals, and misleading information over social networking sites were significant factors for resistance to COVID-19 vaccines [215,216,217]. There is an urgent need for improved public health messaging, transparency regarding vaccine trials and approval, community outreach programs, and increased involvement of pediatricians or family physicians to address family concerns [218].
- (ii)
- Vaccine mandates: Healthcare institutions were the first to implement vaccine mandates for healthcare professionals (HCP). Vaccine mandate has been previously practiced in the healthcare sector, as HCPs are required to receive immunization against diseases such as influenza, pertussis, and hepatitis B [219]. The initial voluntary COVID-19 vaccination drives did not achieve the coverage necessary to protect the community, and outbreaks were frequent. Many institutions and regulatory bodies have since implemented mandates, with the vision to pursue the health and well-being of as many individuals as possible and to avoid harm. For example, the justification for vaccination mandates in schools may be the risk of frequent school disruption and the well-being of other students. Restricting the use of public transport, entry to closed public spaces (theatres, malls), and denying entry to countries have been measures to implement vaccine mandates. The ethical principle of autonomy conflicts with vaccination mandates, as it can override individual choices [220]. Measures such as effective dissemination of vaccine safety data with a mass-educational approach; making school vaccination camps accessible and safe; availability of pediatricians and emergency facilities for those who need them; and providing positive reinforcement for participants in the vaccine programs will improve compliance rates. Creating policies that respect and accommodate the autonomy of the parent and child remains the key method for moving forward.
- (iii)
- Vaccine Research: The norm for performing vaccination research involving children is to commence clinical trials only when a vaccine has been shown to be safe and effective in adults. However, this will lead to a delay in vaccine approval, which could impact the global measures to curb the pandemic. Conducting vaccine trials in children has many issues. The trials need to involve children living with high-risk health conditions and disabilities (whether neurological, genetic, physical, developmental, or emotional), as they are the population most likely to benefit from the vaccine. Whether future vaccine trials should be placebo-controlled or not is another matter of controversy. This is relevant in countries where emergency approval is granted for certain vaccines, as it is difficult to justify continuing with a placebo-controlled trial in the context of the current pandemic [221,222]. For vaccination research in children, the guiding principles should be transparency in data reporting (broken down raw data from clinical trials), inclusiveness (of high-risk children), and external validity.
5.2.5. Implementation of Childhood Vaccine Program
- (i)
- Prioritization: Vaccination of younger children should be considered only if the region/country has achieved high immunization coverage rates for older children (6–11 years) and adolescents. Initially, children aged 2–5 years with high-risk conditions should be immunized on a priority basis. The next priority could be for children living with high-risk individuals. Lastly, children less than 2 years should be included. An age de-escalation approach should be used once sufficient vaccine coverage has occurred in higher age groups.
- (ii)
- Involvement of Pediatricians: Pediatricians and family physicians are an integral part of childhood vaccination programs, as they have good rapport with the child and family. Families may be most comfortable getting the COVID-19 vaccine in Pediatric clinics. The protocols for cold chain maintenance, recognition and management of vaccine-related adverse events, and disposal of biomedical waste are well established in such centers.
- (iii)
- School-based vaccination program: Conducting school- or college-based vaccination camps is a quick and effective tactic to maximize coverage; however, these centers should have adequately trained personnel to handle the vaccine administration and adverse events. This should be voluntary with the informed consent of the child and guardian. These centers should have facilities for quick transport to referral hospitals if required.
- (iv)
- Mandates: With current evidence, less intrusive measures should be used to encourage voluntary vaccination against COVID-19 in children. Current risk–benefit analysis does not support vaccine mandates for children as an ethically justifiable option.
- (v)
- Surveillance: An ongoing active and passive surveillance system must be set up to monitor and report any adverse events related to the vaccine. This will also provide long-term data on the safety of these vaccines for children.
6. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 16 January 2021).
- Parri, N.; Lenge, M.; Buonsenso, D. Coronavirus Infection in Pediatric Emergency Departments (CONFIDENCE) Research Group Children with COVID-19 in Pediatric Emergency Departments in Italy. N. Engl. J. Med. 2020, 383, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Shekerdemian, L.S.; Mahmood, N.R.; Wolfe, K.K.; Riggs, B.J.; Ross, C.E.; McKiernan, C.A.; Heidemann, S.M.; Kleinman, L.C.; Sen, A.I.; Hall, M.W.; et al. Characteristics and Outcomes of Children With Coronavirus Disease 2019 (COVID-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units. JAMA Pediatr. 2020, 174, 868–873. [Google Scholar] [CrossRef] [PubMed]
- Hashan, M.R.; Smoll, N.; King, C.; Ockenden-Muldoon, H.; Walker, J.; Wattiaux, A.; Graham, J.; Booy, R.; Khandaker, G. Epidemiology and Clinical Features of COVID-19 Outbreaks in Aged Care Facilities: A Systematic Review and Meta-Analysis. EClinicalMedicine 2021, 33, 100771. [Google Scholar] [CrossRef] [PubMed]
- Kamdar, S.; Hutchinson, R.; Laing, A.; Stacey, F.; Ansbro, K.; Millar, M.R.; Costeloe, K.; Wade, W.G.; Fleming, P.; Gibbons, D.L. Perinatal Inflammation Influences but Does Not Arrest Rapid Immune Development in Preterm Babies. Nat. Commun. 2020, 11, 1284. [Google Scholar] [CrossRef] [Green Version]
- Viner, R.M.; Mytton, O.T.; Bonell, C.; Melendez-Torres, G.J.; Ward, J.; Hudson, L.; Waddington, C.; Thomas, J.; Russell, S.; van der Klis, F.; et al. Susceptibility to SARS-CoV-2 Infection Among Children and Adolescents Compared With Adults: A Systematic Review and Meta-Analysis. JAMA Pediatr. 2021, 175, 143–156. [Google Scholar] [CrossRef]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiology of COVID-19 Among Children in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [Green Version]
- Trevisanuto, D.; Cavallin, F.; Cavicchiolo, M.E.; Borellini, M.; Calgaro, S.; Baraldi, E. Coronavirus Infection in Neonates: A Systematic Review. Arch. Dis. Child Fetal Neonatal Ed. 2020, 106, 330–335. [Google Scholar] [CrossRef]
- Kalamdani, P.; Kalathingal, T.; Manerkar, S.; Mondkar, J. Clinical Profile of SARS-CoV-2 Infected Neonates From a Tertiary Government Hospital in Mumbai, India. Indian Pediatr. 2020, 57, 1143–1146. [Google Scholar] [CrossRef]
- Chmielewska, B.; Barratt, I.; Townsend, R.; Kalafat, E.; van der Meulen, J.; Gurol-Urganci, I.; O’Brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; et al. Effects of the COVID-19 Pandemic on Maternal and Perinatal Outcomes: A Systematic Review and Meta-Analysis. Lancet Glob. Health 2021, 9, e759–e772. [Google Scholar] [CrossRef]
- Norman, M.; Navér, L.; Söderling, J.; Ahlberg, M.; Hervius Askling, H.; Aronsson, B.; Byström, E.; Jonsson, J.; Sengpiel, V.; Ludvigsson, J.F.; et al. Association of Maternal SARS-CoV-2 Infection in Pregnancy With Neonatal Outcomes. JAMA 2021, 325, 2076–2086. [Google Scholar] [CrossRef]
- Delahoy, M.J.; Ujamaa, D.; Whitaker, M.; O’Halloran, A.; Anglin, O.; Burns, E.; Cummings, C.; Holstein, R.; Kambhampati, A.K.; Milucky, J.; et al. Hospitalizations Associated with COVID-19 Among Children and Adolescents—COVID-NET, 14 States, March 1, 2020–August 14, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1255–1260. [Google Scholar] [CrossRef]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Sobolewska-Pilarczyk, M.; Pokorska-Śpiewak, M.; Stachowiak, A.; Marczyńska, M.; Talarek, E.; Ołdakowska, A.; Kucharek, I.; Sybilski, A.; Mania, A.; Figlerowicz, M.; et al. COVID-19 Infections in Infants. Sci. Rep. 2022, 12, 7765. [Google Scholar] [CrossRef]
- Devin, J.; Marano, R.; Mikhael, M.; Feaster, W.; Sanger, T.; Ehwerhemuepha, L. Epidemiology of Neonatal COVID-19 in the United States. Pediatrics 2022, 150, e2022056297. [Google Scholar] [CrossRef]
- Robaina-Castellanos, G.R.; de la Caridad Riesgo-Rodriguez, S. Congenital and Intrapartum SARS-CoV-2 Infection in Neonates: Hypotheses, Evidence and Perspectives. MEDICC Rev. 2021, 23, 72–83. [Google Scholar] [CrossRef]
- Zimmermann, P.; Curtis, N. Why Is COVID-19 Less Severe in Children? A Review of the Proposed Mechanisms Underlying the Age-Related Difference in Severity of SARS-CoV-2 Infections. Arch. Dis. Child. 2020, 106, 429–439. [Google Scholar] [CrossRef]
- Li, M.; Wang, H.; Tian, L.; Pang, Z.; Yang, Q.; Huang, T.; Fan, J.; Song, L.; Tong, Y.; Fan, H. COVID-19 Vaccine Development: Milestones, Lessons and Prospects. Signal Transduct. Target Ther. 2022, 7, 146. [Google Scholar] [CrossRef]
- COVID-19 Vaccine Tracker and Landscape. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 19 January 2023).
- Interim Statement on COVID-19 Vaccination for Children. Available online: https://www.who.int/news/item/11-08-2022-interim-statement-on-covid-19-vaccination-for-children (accessed on 7 January 2023).
- Are Children Eligible for COVID-19 Vaccination? Available online: https://ourworldindata.org/grapher/covid-vaccine-age (accessed on 8 January 2023).
- Badal, S.; Thapa Bajgain, K.; Badal, S.; Thapa, R.; Bajgain, B.B.; Santana, M.J. Prevalence, Clinical Characteristics, and Outcomes of Pediatric COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Virol. 2021, 135, 104715. [Google Scholar] [CrossRef]
- Götzinger, F.; Santiago-García, B.; Noguera-Julián, A.; Lanaspa, M.; Lancella, L.; Calò Carducci, F.I.; Gabrovska, N.; Velizarova, S.; Prunk, P.; Osterman, V.; et al. COVID-19 in Children and Adolescents in Europe: A Multinational, Multicentre Cohort Study. Lancet Child Adolesc. Health 2020, 4, 653–661. [Google Scholar] [CrossRef]
- Götzinger, F.; Santiago-Garcia, B.; Fumadó-Pérez, V.; Brinkmann, F.; Tebruegge, M. The Ability of the Neonatal Immune Response to Handle SARS-CoV-2 Infection. Lancet Child Adolesc. Health 2021, 5, e6–e7. [Google Scholar] [CrossRef] [PubMed]
- Bhuiyan, M.U.; Stiboy, E.; Hassan, M.Z.; Chan, M.; Islam, M.S.; Haider, N.; Jaffe, A.; Homaira, N. Epidemiology of COVID-19 Infection in Young Children under Five Years: A Systematic Review and Meta-Analysis. Vaccine 2021, 39, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Dona’, D.; Montagnani, C.; Di Chiara, C.; Venturini, E.; Galli, L.; Lo Vecchio, A.; Denina, M.; Olivini, N.; Bruzzese, E.; Campana, A.; et al. COVID-19 in Infants Less than 3 Months: Severe or Not Severe Disease? Viruses 2022, 14, 2256. [Google Scholar] [CrossRef] [PubMed]
- Allotey, J.; Chatterjee, S.; Kew, T.; Gaetano, A.; Stallings, E.; Fernández-García, S.; Yap, M.; Sheikh, J.; Lawson, H.; Coomar, D.; et al. SARS-CoV-2 Positivity in Offspring and Timing of Mother-to-Child Transmission: Living Systematic Review and Meta-Analysis. BMJ 2022, 376, e067696. [Google Scholar] [CrossRef]
- Di Toro, F.; Gjoka, M.; Di Lorenzo, G.; De Santo, D.; De Seta, F.; Maso, G.; Risso, F.M.; Romano, F.; Wiesenfeld, U.; Levi-D’Ancona, R.; et al. Impact of COVID-19 on Maternal and Neonatal Outcomes: A Systematic Review and Meta-Analysis. Clin. Microbiol. Infect. 2021, 27, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Hudak, M.L.; Flannery, D.D.; Barnette, K.; Getzlaff, T.; Gautam, S.; Dhudasia, M.B.; Mukhopadhyay, S.; Pfeifer, M.R.; Ellington, S.R.; Galang, R.R.; et al. Maternal and Newborn Hospital Outcomes of Perinatal SARS-CoV-2 Infection: A National Registry. Pediatrics 2023, 151, e2022059595. [Google Scholar] [CrossRef]
- Iftimie, S.; López-Azcona, A.F.; Vallverdú, I.; Hernández-Flix, S.; de Febrer, G.; Parra, S.; Hernández-Aguilera, A.; Riu, F.; Joven, J.; Andreychuk, N.; et al. First and Second Waves of Coronavirus Disease-19: A Comparative Study in Hospitalized Patients in Reus, Spain. PLoS ONE 2021, 16, e0248029. [Google Scholar] [CrossRef] [PubMed]
- Kadiwar, S.; Smith, J.J.; Ledot, S.; Johnson, M.; Bianchi, P.; Singh, N.; Montanaro, C.; Gatzoulis, M.; Shah, N.; Ukor, E.-F. Were Pregnant Women More Affected by COVID-19 in the Second Wave of the Pandemic? Lancet 2021, 397, 1539–1540. [Google Scholar] [CrossRef]
- Tandon, P.; Leibner, E.S.; Hackett, A.; Maguire, K.; Mashriqi, N.; Kohli-Seth, R. The Third Wave: Comparing Seasonal Trends in COVID-19 Patient Data at a Large Hospital System in New York City. Crit. Care Explor. 2022, 4, e0653. [Google Scholar] [CrossRef]
- Koshy, J. Fewer Hospitalisations in India’s Third COVID-19 Wave, Data Show; 2.8 Lakh Fresh COVID-19 Cases on 26 January 2022. The Hindu 2022. Available online: https://www.thehindu.com/news/national/fewer-hospitalisations-in-indias-third-covid-19-wave-data-show-28-lakh-fresh-covid-19-cases-on-january-26-2022/article38330529.ece (accessed on 30 January 2022).
- Wang, L.; Berger, N.A.; Kaelber, D.C.; Davis, P.B.; Volkow, N.D.; Xu, R. COVID Infection Severity in Children under 5 Years Old before and after Omicron Emergence in the US. medRxiv 2022. [Google Scholar] [CrossRef]
- Dougherty, K.; Mannell, M.; Naqvi, O.; Matson, D.; Stone, J. SARS-CoV-2 B.1.617.2 (Delta) Variant COVID-19 Outbreak Associated with a Gymnastics Facility—Oklahoma, April–May 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1004–1007. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. HLH Across Speciality Collaboration, UK COVID-19: Consider Cytokine Storm Syndromes and Immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Consiglio, C.R.; Cotugno, N.; Sardh, F.; Pou, C.; Amodio, D.; Rodriguez, L.; Tan, Z.; Zicari, S.; Ruggiero, A.; Pascucci, G.R.; et al. The Immunology of Multisystem Inflammatory Syndrome in Children with COVID-19. Cell 2020, 183, 968–981.e7. [Google Scholar] [CrossRef]
- Carsana, L.; Sonzogni, A.; Nasr, A.; Rossi, R.S.; Pellegrinelli, A.; Zerbi, P.; Rech, R.; Colombo, R.; Antinori, S.; Corbellino, M.; et al. Pulmonary Post-Mortem Findings in a Series of COVID-19 Cases from Northern Italy: A Two-Centre Descriptive Study. Lancet Infect. Dis. 2020, 20, 1135–1140. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.E.; Akmatbekov, A.; Harbert, J.L.; Li, G.; Quincy Brown, J.; Vander Heide, R.S. Pulmonary and Cardiac Pathology in African American Patients with COVID-19: An Autopsy Series from New Orleans. Lancet Respir. Med. 2020, 8, 681–686. [Google Scholar] [CrossRef]
- Tian, S.; Hu, W.; Niu, L.; Liu, H.; Xu, H.; Xiao, S.-Y. Pulmonary Pathology of Early-Phase 2019 Novel Coronavirus (COVID-19) Pneumonia in Two Patients With Lung Cancer. J. Thorac. Oncol. 2020, 15, 700–704. [Google Scholar] [CrossRef]
- Moro-García, M.A.; Mayo, J.C.; Sainz, R.M.; Alonso-Arias, R. Influence of Inflammation in the Process of T Lymphocyte Differentiation: Proliferative, Metabolic, and Oxidative Changes. Front. Immunol. 2018, 9, 339. [Google Scholar] [CrossRef] [Green Version]
- Mikacenic, C.; Hansen, E.E.; Radella, F.; Gharib, S.A.; Stapleton, R.D.; Wurfel, M.M. Interleukin-17A Is Associated With Alveolar Inflammation and Poor Outcomes in Acute Respiratory Distress Syndrome. Crit. Care Med. 2016, 44, 496–502. [Google Scholar] [CrossRef] [Green Version]
- Aberdein, J.D.; Cole, J.; Bewley, M.A.; Marriott, H.M.; Dockrell, D.H. Alveolar Macrophages in Pulmonary Host Defence the Unrecognized Role of Apoptosis as a Mechanism of Intracellular Bacterial Killing. Clin. Exp. Immunol. 2013, 174, 193–202. [Google Scholar] [CrossRef]
- Yang, C.-Y.; Chen, C.-S.; Yiang, G.-T.; Cheng, Y.-L.; Yong, S.-B.; Wu, M.-Y.; Li, C.-J. New Insights into the Immune Molecular Regulation of the Pathogenesis of Acute Respiratory Distress Syndrome. Int. J. Mol. Sci. 2018, 19, 588. [Google Scholar] [CrossRef] [Green Version]
- Zuo, Y.; Yalavarthi, S.; Shi, H.; Gockman, K.; Zuo, M.; Madison, J.A.; Blair, C.; Weber, A.; Barnes, B.J.; Egeblad, M.; et al. Neutrophil Extracellular Traps in COVID-19. JCI Insight 2020, 5, e13899. [Google Scholar] [CrossRef] [Green Version]
- Von Hundelshausen, P.; Koenen, R.R.; Sack, M.; Mause, S.F.; Adriaens, W.; Proudfoot, A.E.I.; Hackeng, T.M.; Weber, C. Heterophilic Interactions of Platelet Factor 4 and RANTES Promote Monocyte Arrest on Endothelium. Blood 2005, 105, 924–930. [Google Scholar] [CrossRef] [Green Version]
- Kotlyar, A.M.; Grechukhina, O.; Chen, A.; Popkhadze, S.; Grimshaw, A.; Tal, O.; Taylor, H.S.; Tal, R. Vertical Transmission of Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Am. J. Obstet. Gynecol. 2021, 224, 35–53.e3. [Google Scholar] [CrossRef]
- Salvatore, C.M.; Han, J.Y.; Acker, K.P.; Tiwari, P.; Jin, J.; Brandler, M.; Cangemi, C.; Gordon, L.; Parow, A.; DiPace, J.; et al. Neonatal Management and Outcomes during the COVID-19 Pandemic: An Observation Cohort Study. Lancet Child Adolesc. Health 2020, 4, 721–727. [Google Scholar] [CrossRef]
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; Do Cao, J.; Benachi, A.; De Luca, D. Transplacental Transmission of SARS-CoV-2 Infection. Nat. Commun. 2020, 11, 3572. [Google Scholar] [CrossRef]
- Algarroba, G.N.; Rekawek, P.; Vahanian, S.A.; Khullar, P.; Palaia, T.; Peltier, M.R.; Chavez, M.R.; Vintzileos, A.M. Visualization of Severe Acute Respiratory Syndrome Coronavirus 2 Invading the Human Placenta Using Electron Microscopy. Am. J. Obstet. Gynecol. 2020, 223, 275–278. [Google Scholar] [CrossRef]
- Valdés, G.; Neves, L.A.A.; Anton, L.; Corthorn, J.; Chacón, C.; Germain, A.M.; Merrill, D.C.; Ferrario, C.M.; Sarao, R.; Penninger, J.; et al. Distribution of Angiotensin-(1-7) and ACE2 in Human Placentas of Normal and Pathological Pregnancies. Placenta 2006, 27, 200–207. [Google Scholar] [CrossRef]
- Hecht, J.L.; Quade, B.; Deshpande, V.; Mino-Kenudson, M.; Ting, D.T.; Desai, N.; Dygulska, B.; Heyman, T.; Salafia, C.; Shen, D.; et al. SARS-CoV-2 Can Infect the Placenta and Is Not Associated with Specific Placental Histopathology: A Series of 19 Placentas from COVID-19-Positive Mothers. Mod. Pathol. 2020, 33, 2092–2103. [Google Scholar] [CrossRef]
- Saheb Sharif-Askari, N.; Saheb Sharif-Askari, F.; Alabed, M.; Temsah, M.-H.; Al Heialy, S.; Hamid, Q.; Halwani, R. Airways Expression of SARS-CoV-2 Receptor, ACE2, and TMPRSS2 Is Lower in Children Than Adults and Increases with Smoking and COPD. Mol. Ther. Methods Clin. Dev. 2020, 18, 1–6. [Google Scholar] [CrossRef]
- Hannet, I.; Erkeller-Yuksel, F.; Lydyard, P.; Deneys, V.; DeBruyère, M. Developmental and Maturational Changes in Human Blood Lymphocyte Subpopulations. Immunol. Today 1992, 13, 215–218. [Google Scholar] [CrossRef]
- Cupedo, T.; Nagasawa, M.; Weijer, K.; Blom, B.; Spits, H. Development and Activation of Regulatory T Cells in the Human Fetus. Eur. J. Immunol. 2005, 35, 383–390. [Google Scholar] [CrossRef]
- Darrasse-Jèze, G.; Marodon, G.; Salomon, B.L.; Catala, M.; Klatzmann, D. Ontogeny of CD4+CD25+ Regulatory/Suppressor T Cells in Human Fetuses. Blood 2005, 105, 4715–4721. [Google Scholar] [CrossRef] [Green Version]
- Schultz, C.; Reiss, I.; Bucsky, P.; Göpel, W.; Gembruch, U.; Ziesenitz, S.; Gortner, L. Maturational Changes of Lymphocyte Surface Antigens in Human Blood: Comparison between Fetuses, Neonates and Adults. Neonatology 2000, 78, 77–82. [Google Scholar] [CrossRef]
- Harris, D.T.; Schumacher, M.J.; Locascio, J.; Besencon, F.J.; Olson, G.B.; DeLuca, D.; Shenker, L.; Bard, J.; Boyse, E.A. Phenotypic and Functional Immaturity of Human Umbilical Cord Blood T Lymphocytes. Proc. Natl. Acad. Sci. USA 1992, 89, 10006–10010. [Google Scholar] [CrossRef] [Green Version]
- Grimsholm, O.; Piano Mortari, E.; Davydov, A.N.; Shugay, M.; Obraztsova, A.S.; Bocci, C.; Marasco, E.; Marcellini, V.; Aranburu, A.; Farroni, C.; et al. The Interplay between CD27dull and CD27bright B Cells Ensures the Flexibility, Stability, and Resilience of Human B Cell Memory. Cell Rep. 2020, 30, 2963–2977.e6. [Google Scholar] [CrossRef] [Green Version]
- Flannery, D.D.; Gouma, S.; Dhudasia, M.B.; Mukhopadhyay, S.; Pfeifer, M.R.; Woodford, E.C.; Triebwasser, J.E.; Gerber, J.S.; Morris, J.S.; Weirick, M.E.; et al. Assessment of Maternal and Neonatal Cord Blood SARS-CoV-2 Antibodies and Placental Transfer Ratios. JAMA Pediatr. 2021, 175, 594–600. [Google Scholar] [CrossRef]
- Paul, G.; Chad, R. Newborn Antibodies to SARS-CoV-2 Detected in Cord Blood after Maternal Vaccination—A Case Report. BMC Pediatr. 2021, 21, 138. [Google Scholar] [CrossRef]
- Pace, R.M.; Williams, J.E.; Järvinen, K.M.; Belfort, M.B.; Pace, C.D.; Lackey, K.A.; Gogel, A.C.; Nguyen-Contant, P.; Kanagaiah, P.; Fitzgerald, T.; et al. COVID-19 and Human Milk: SARS-CoV-2, Antibodies, and Neutralizing Capacity. MedRxiv Prepr. Serv. Health Sci. 2020. [Google Scholar] [CrossRef]
- Fox, A.; Marino, J.; Amanat, F.; Krammer, F.; Hahn-Holbrook, J.; Zolla-Pazner, S.; Powell, R. Evidence of a Significant Secretory-IgA-Dominant SARS-CoV-2 Immune Response in Human Milk Following Recovery from COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Yu, Y.; Li, Y.; Hu, Y.; Li, B.; Xu, J. Breastfed 13 Month-Old Infant of a Mother with COVID-19 Pneumonia: A Case Report. Int. Breastfeed. J. 2020, 15, 68. [Google Scholar] [CrossRef]
- Yang, I.; Corwin, E.J.; Brennan, P.A.; Jordan, S.; Murphy, J.R.; Dunlop, A. The Infant Microbiome: Implications for Infant Health and Neurocognitive Development. Nurs. Res. 2016, 65, 76–88. [Google Scholar] [CrossRef] [Green Version]
- Gu, S.; Chen, Y.; Wu, Z.; Chen, Y.; Gao, H.; Lv, L.; Guo, F.; Zhang, X.; Luo, R.; Huang, C.; et al. Alterations of the Gut Microbiota in Patients With Coronavirus Disease 2019 or H1N1 Influenza. Clin. Infect. Dis. 2020, 71, 2669–2678. [Google Scholar] [CrossRef]
- Zuo, T.; Zhang, F.; Lui, G.C.Y.; Yeoh, Y.K.; Li, A.Y.L.; Zhan, H.; Wan, Y.; Chung, A.C.K.; Cheung, C.P.; Chen, N.; et al. Alterations in Gut Microbiota of Patients With COVID-19 During Time of Hospitalization. Gastroenterology 2020, 159, 944–955.e8. [Google Scholar] [CrossRef]
- Im, D.; Shi, W.; Driscoll, B. Pediatric Acute Respiratory Distress Syndrome: Fibrosis versus Repair. Front. Pediatr. 2016, 4, 28. [Google Scholar] [CrossRef] [Green Version]
- Ying, L.; Alvira, C.M.; Cornfield, D.N. Developmental Differences in Focal Adhesion Kinase Expression Modulate Pulmonary Endothelial Barrier Function in Response to Inflammation. Am. J. Physiol.—Lung Cell. Mol. Physiol. 2018, 315, L66–L77. [Google Scholar] [CrossRef]
- Zhdanova, I.V.; Wurtman, R.J.; Balcioglu, A.; Kartashov, A.I.; Lynch, H.J. Endogenous Melatonin Levels and the Fate of Exogenous Melatonin: Age Effects. J. Gerontol. Ser. A 1998, 53A, B293–B298. [Google Scholar] [CrossRef] [Green Version]
- Wurtman, R.J. Age-Related Decreases in Melatonin Secretion—Clinical Consequences. J. Clin. Endocrinol. Metab. 2000, 85, 2135–2136. [Google Scholar] [CrossRef]
- García, I.G.; Rodriguez-Rubio, M.; Mariblanca, A.R.; de Soto, L.M.; García, L.D.; Villatoro, J.M.; Parada, J.Q.; Meseguer, E.S.; Rosales, M.J.; González, J.; et al. A Randomized Multicenter Clinical Trial to Evaluate the Efficacy of Melatonin in the Prophylaxis of SARS-CoV-2 Infection in High-Risk Contacts (MeCOVID Trial): A Structured Summary of a Study Protocol for a Randomised Controlled Trial. Trials 2020, 21, 466. [Google Scholar] [CrossRef]
- Ameri, A.; Asadi, M.F.; Kamali, M.; Vatankhah, M.; Ziaei, A.; Safa, O.; Mahmudi, M.; Fathalipour, M. Evaluation of the Effect of Melatonin in Patients with COVID-19-Induced Pneumonia Admitted to the Intensive Care Unit: A Structured Summary of a Study Protocol for a Randomized Controlled Trial. Trials 2021, 22, 194. [Google Scholar] [CrossRef]
- Giamarellos-Bourboulis, E.J.; Tsilika, M.; Moorlag, S.; Antonakos, N.; Kotsaki, A.; Domínguez-Andrés, J.; Kyriazopoulou, E.; Gkavogianni, T.; Adami, M.-E.; Damoraki, G.; et al. Activate: Randomized Clinical Trial of BCG Vaccination against Infection in the Elderly. Cell 2020, 183, 315–323.e9. [Google Scholar] [CrossRef]
- Moorlag, S.J.C.F.M.; Arts, R.J.W.; van Crevel, R.; Netea, M.G. Non-Specific Effects of BCG Vaccine on Viral Infections. Clin. Microbiol. Infect. 2019, 25, 1473–1478. [Google Scholar] [CrossRef] [PubMed]
- Faustman, D.L.; Lee, A.; Hostetter, E.R.; Aristarkhova, A.; Ng, N.C.; Shpilsky, G.F.; Tran, L.; Wolfe, G.; Takahashi, H.; Dias, H.F.; et al. Multiple BCG Vaccinations for the Prevention of COVID-19 and Other Infectious Diseases in Type 1 Diabetes. Cell Rep. Med. 2022, 3, 100728. [Google Scholar] [CrossRef] [PubMed]
- Murdoch Childrens Research Institute. BCG Vaccination to Reduce the Impact of COVID-19 in Healthcare Workers (BRACE) Trial. 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT04327206 (accessed on 19 January 2023).
- Shang, J.; Ye, G.; Shi, K.; Wan, Y.; Luo, C.; Aihara, H.; Geng, Q.; Auerbach, A.; Li, F. Structural Basis of Receptor Recognition by SARS-CoV-2. Nature 2020, 581, 221–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, R.; Preston, G.; Yosypiv, I.V. Ontogeny of Angiotensin-Converting Enzyme 2. Pediatr. Res. 2012, 71, 13–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Wang, A.; Chiou, J.; Poirion, O.; Buchanan, J.; Valdez, M.; Verheyden, J.; Hou, X.; Guo, M.; Newsome, J.; Kudtarkar, P.; et al. Single Nucleus Multiomic Profiling Reveals Age-Dynamic Regulation of Host Genes Associated with SARS-CoV-2 Infection. bioRxiv 2020. [Google Scholar] [CrossRef]
- Steinman, J.B.; Lum, F.M.; Ho, P.P.K.; Kaminski, N.; Steinman, L. Reduced Development of COVID-19 in Children Reveals Molecular Checkpoints Gating Pathogenesis Illuminating Potential Therapeutics. Proc. Natl. Acad. Sci. USA 2020, 117, 24620–24626. [Google Scholar] [CrossRef]
- Mancia, G.; Rea, F.; Ludergnani, M.; Apolone, G.; Corrao, G. Renin-Angiotensin-Aldosterone System Blockers and the Risk of COVID-19. N. Engl. J. Med. 2020, 382, 2431–2440. [Google Scholar] [CrossRef]
- Bayer, A.; Delorme-Axford, E.; Sleigher, C.; Frey, T.K.; Trobaugh, D.W.; Klimstra, W.B.; Emert-Sedlak, L.A.; Smithgall, T.E.; Kinchington, P.R.; Vadia, S.; et al. Human Trophoblasts Confer Resistance to Viruses Implicated in Perinatal Infection. Am. J. Obstet. Gynecol. 2015, 212, 71.e1–71.e8. [Google Scholar] [CrossRef] [Green Version]
- Bayer, A.; Lennemann, N.J.; Ouyang, Y.; Bramley, J.C.; Morosky, S.; Marques, E.T.D.A.; Cherry, S.; Sadovsky, Y.; Coyne, C.B. Type III Interferons Produced by Human Placental Trophoblasts Confer Protection against Zika Virus Infection. Cell Host Microbe 2016, 19, 705–712. [Google Scholar] [CrossRef] [Green Version]
- Mulvey, J.J.; Magro, C.M.; Ma, L.X.; Nuovo, G.J.; Baergen, R.N. Analysis of Complement Deposition and Viral RNA in Placentas of COVID-19 Patients. Ann. Diagn. Pathol. 2020, 46, 151530. [Google Scholar] [CrossRef]
- Penfield, C.A.; Brubaker, S.G.; Limaye, M.A.; Lighter, J.; Ratner, A.J.; Thomas, K.M.; Meyer, J.A.; Roman, A.S. Detection of Severe Acute Respiratory Syndrome Coronavirus 2 in Placental and Fetal Membrane Samples. Am. J. Obstet. Gynecol. MFM 2020, 2, 100133. [Google Scholar] [CrossRef]
- Zhao, Y.; Dai, Z.P.; Lv, P.; Gao, X.M. Phenotypic and Functional Analysis of Human T Lymphocytes in Early Second- and Third-Trimester Fetuses. Clin. Exp. Immunol. 2002, 129, 302–308. [Google Scholar] [CrossRef]
- Randolph, D.A. The Neonatal Adaptive Immune System. NeoReviews 2005, 6, e454–e462. [Google Scholar] [CrossRef]
- Izcue, A.; Powrie, F. Prenatal Tolerance—A Role for Regulatory T Cells? Eur. J. Immunol. 2005, 35, 379–382. [Google Scholar] [CrossRef]
- Sanchez-Schmitz, G.; Morrocchi, E.; Cooney, M.; Soni, D.; Khatun, R.; Palma, P.; Dowling, D.J.; Levy, O. Neonatal Monocytes Demonstrate Impaired Homeostatic Extravasation into a Microphysiological Human Vascular Model. Sci. Rep. 2020, 10, 17836. [Google Scholar] [CrossRef]
- Yim, H.J.; Lok, A.S.F. Natural History of Chronic Hepatitis B Virus Infection: What We Knew in 1981 and What We Know in 2005. Hepatology 2006, 43, S173–S181. [Google Scholar] [CrossRef] [Green Version]
- Holodick, N.E.; Rodríguez-Zhurbenko, N.; Hernández, A.M. Defining Natural Antibodies. Front. Immunol. 2017, 8, 872. [Google Scholar] [CrossRef] [Green Version]
- Zeng, H.; Xu, C.; Fan, J.; Tang, Y.; Deng, Q.; Zhang, W.; Long, X. Antibodies in Infants Born to Mothers with COVID-19 Pneumonia. JAMA—J. Am. Med. Assoc. 2020, 323, 1848–1849. [Google Scholar] [CrossRef]
- Gao, X.; Wang, S.; Zeng, W.; Chen, S.; Wu, J.; Lin, X.; Liu, Y.; Sun, Z.; Feng, L. Clinical and Immunologic Features among COVID-19–Affected Mother–Infant Pairs: Antibodies to SARS-CoV-2 Detected in Breast Milk. New Microbes New Infect. 2020, 37, 100752. [Google Scholar] [CrossRef]
- Atyeo, C.G.; Shook, L.L.; Brigida, S.; De Guzman, R.M.; Demidkin, S.; Muir, C.; Akinwunmi, B.; Baez, A.M.; Sheehan, M.L.; McSweeney, E.; et al. Maternal Immune Response and Placental Antibody Transfer after COVID-19 Vaccination across Trimester and Platforms. Nat. Commun. 2022, 13, 3571. [Google Scholar] [CrossRef] [PubMed]
- Song, D.; Prahl, M.; Gaw, S.L.; Narasimhan, S.R.; Rai, D.S.; Huang, A.; Flores, C.V.; Lin, C.Y.; Jigmeddagva, U.; Wu, A.; et al. Passive and Active Immunity in Infants Born to Mothers with SARS-CoV-2 Infection during Pregnancy: Prospective Cohort Study. BMJ Open 2021, 11, e053036. [Google Scholar] [CrossRef] [PubMed]
- Ballard, O.; Morrow, A.L. Human Milk Composition. Nutrients and Bioactive Factors. Pediatr. Clin. North Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witkowska-Zimny, M.; Kaminska-El-Hassan, E. Cells of Human Breast Milk. Cell. Mol. Biol. Lett. 2017, 22, 11. [Google Scholar] [CrossRef] [Green Version]
- Szczygioł, P.; Łukianowski, B.; Kościelska-Kasprzak, K.; Jakuszko, K.; Bartoszek, D.; Krajewska, M.; Królak-Olejnik, B. Antibodies in the Breastmilk of COVID-19 Recovered Women. BMC Pregnancy Childbirth 2022, 22, 635. [Google Scholar] [CrossRef]
- Schittny, J.C. Development of the Lung. Cell Tissue Res. 2017, 367, 427–444. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.H.; Cao, X.J.; Liu, W.; Shi, X.Y.; Wei, W. Inhibitory Effect of Melatonin on Lung Oxidative Stress Induced by Respiratory Syncytial Virus Infection in Mice. J. Pineal Res. 2010, 48, 109–116. [Google Scholar] [CrossRef]
- Reiter, R.J.; Ma, Q.; Sharma, R. Treatment of Ebola and Other Infectious Diseases: Melatonin “Goes Viral”. Melatonin Res. 2020, 3, 43–57. [Google Scholar] [CrossRef]
- Pollard, A.J.; Finn, A.; Curtis, N. Non-Specific Effects of Vaccines: Plausible and Potentially Important, but Implications Uncertain. Arch. Dis. Child. 2017, 102, 1077–1081. [Google Scholar] [CrossRef] [Green Version]
- Freyne, B.; Donath, S.; Germano, S.; Gardiner, K.; Casalaz, D.; Robins-Browne, R.M.; Amenyogbe, N.; Messina, N.L.; Netea, M.G.; Flanagan, K.L.; et al. Neonatal BCG Vaccination Influences Cytokine Responses to Toll-like Receptor Ligands and Heterologous Antigens. J. Infect. Dis. 2018, 217, 1798–1808. [Google Scholar] [CrossRef]
- Escobar, L.E.; Molina-Cruz, A.; Barillas-Mury, C. BCG Vaccine Protection from Severe Coronavirus Disease 2019 (COVID-19). Proc. Natl. Acad. Sci. USA 2020, 117, 17720–17726. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.; Reandelar, M.J.; Fasciglione, K.; Roumenova, V.; Li, Y.; Otazu, G. Correlation between Universal BCG Vaccination Policy and Reduced Morbidity and Mortality for COVID-19: An Epidemiological Study. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Shet, A.; Ray, D.; Malavige, N.; Santosham, M.; Bar-Zeev, N. Differential COVID-19-Attributable Mortality and BCG Vaccine Use in Countries. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Goyal, P.; Sikary, A.K.; Sachdeva, R.A.; Parashar, L.; Tarique, A. Mortality Analysis of COVID-19 Cases during the Second Wave and Its Comparison with the First Wave: A Hospital-Based Study. J. Family Med. Prim. Care 2022, 11, 6091–6095. [Google Scholar] [CrossRef]
- Zirpe, K.G.; Dixit, S.; Kulkarni, A.P.; Pandit, R.A.; Ranganathan, P.; Prasad, S.; Amanulla, Z.K.; Kothari, V.; Ambapkar, S.; Gurav, S.K.; et al. The Second- vs First-Wave COVID-19: More of the Same or a Lot Worse? A Comparison of Mortality between the Two Waves in Patients Admitted to Intensive Care Units in Nine Hospitals in Western Maharashtra. Indian J. Crit. Care Med. 2021, 25, 1343–1348. [Google Scholar] [CrossRef]
- Li, X.; Xu, W.; Dozier, M.; He, Y.; Kirolos, A.; Lang, Z.; Song, P.; Theodoratou, E. The Role of Children in the Transmission of SARS-CoV2: Updated Rapid Review. J. Glob. Health 2020, 10, 021101. [Google Scholar] [CrossRef]
- Brown, A.; Shenker, N. Experiences of Breastfeeding during COVID-19: Lessons for Future Practical and Emotional Support. Matern. Child. Nutr. 2021, 17, e13088. [Google Scholar] [CrossRef]
- Minckas, N.; Medvedev, M.M.; Adejuyigbe, E.A.; Brotherton, H.; Chellani, H.; Estifanos, A.S.; Ezeaka, C.; Gobezayehu, A.G.; Irimu, G.; Kawaza, K.; et al. Preterm Care during the COVID-19 Pandemic: A Comparative Risk Analysis of Neonatal Deaths Averted by Kangaroo Mother Care versus Mortality Due to SARS-CoV-2 Infection. EClinicalMedicine 2021, 33, 100733. [Google Scholar] [CrossRef]
- Viner, R.; Russell, S.; Saulle, R.; Croker, H.; Stansfield, C.; Packer, J.; Nicholls, D.; Goddings, A.-L.; Bonell, C.; Hudson, L.; et al. School Closures During Social Lockdown and Mental Health, Health Behaviors, and Well-Being Among Children and Adolescents During the First COVID-19 Wave: A Systematic Review. JAMA Pediatr. 2022, 176, 400–409. [Google Scholar] [CrossRef]
- Ortega Pacheco, Y.J.; Barrero Toncel, V.I. The Impact of School Closure on Children’s Well-Being during the COVID-19 Pandemic. Asian J. Psychiatr. 2022, 67, 102957. [Google Scholar] [CrossRef]
- Cavicchiolo, M.E.; Trevisanuto, D.; Lolli, E.; Mardegan, V.; Saieva, A.M.; Franchin, E.; Plebani, M.; Donato, D.; Baraldi, E. Universal Screening of High-Risk Neonates, Parents, and Staff at a Neonatal Intensive Care Unit during the SARS-CoV-2 Pandemic. Eur. J. Pediatr. 2020, 179, 1949–1955. [Google Scholar] [CrossRef] [PubMed]
- Trahan, M.-J.; Mitric, C.; Malhamé, I.; Abenhaim, H.A. Screening and Testing Pregnant Patients for SARS-CoV-2: First-Wave Experience of a Designated COVID-19 Hospitalization Centre in Montréal. J. Obstet. Gynaecol. Can. 2021, 43, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Hashim, N.A.F.; Mahdy, Z.A.; Abdul Rahman, R.; Kalok, A.H.M.; Sutan, R. Universal Testing Policy for COVID-19 in Pregnancy: A Systematic Review. Front. Public Health 2022, 10, 588269. [Google Scholar] [CrossRef]
- Martinelli, L.; Kopilaš, V.; Vidmar, M.; Heavin, C.; Machado, H.; Todorović, Z.; Buzas, N.; Pot, M.; Prainsack, B.; Gajović, S. Face Masks During the COVID-19 Pandemic: A Simple Protection Tool With Many Meanings. Front. Public Health 2021, 8, 606635. [Google Scholar] [CrossRef] [PubMed]
- Natnael, T.; Adane, M.; Goraw, S. Hand Hygiene Practices during the COVID-19 Pandemic and Associated Factors among Barbers and Beauty Salon Workers in Ethiopia. PLoS ONE 2022, 17, e0269225. [Google Scholar] [CrossRef] [PubMed]
- Vardhelli, V.; Pandita, A.; Pillai, A.; Badatya, S.K. Perinatal COVID-19: Review of Current Evidence and Practical Approach towards Prevention and Management. Eur. J. Pediatr. 2020, 180, 1009–1031. [Google Scholar] [CrossRef]
- Villar, J.; Ariff, S.; Gunier, R.B.; Thiruvengadam, R.; Rauch, S.; Kholin, A.; Roggero, P.; Prefumo, F.; do Vale, M.S.; Cardona-Perez, J.A.; et al. Maternal and Neonatal Morbidity and Mortality Among Pregnant Women With and Without COVID-19 Infection: The INTERCOVID Multinational Cohort Study. JAMA Pediatr. 2021, 175, 817–826. [Google Scholar] [CrossRef]
- Chawla, D.; Chirla, D.; Dalwai, S.; Deorari, A.K.; Ganatra, A.; Gandhi, A.; Kabra, N.S.; Kumar, P.; Mittal, P.; Parekh, B.J.; et al. Perinatal-Neonatal Management of COVID-19 Infection—Guidelines of the Federation of Obstetric and Gynaecological Societies of India (FOGSI), National Neonatology Forum of India (NNF), and Indian Academy of Pediatrics (IAP). Indian Pediatr. 2020, 57, 536–548. [Google Scholar] [CrossRef]
- Mullins, E.; Hudak, M.L.; Banerjee, J.; Getzlaff, T.; Townson, J.; Barnette, K.; Playle, R.; Perry, A.; Bourne, T.; Lees, C.C.; et al. Pregnancy and Neonatal Outcomes of COVID-19: Coreporting of Common Outcomes from PAN-COVID and AAP-SONPM Registries. Ultrasound Obstet. Gynecol. 2021, 57, 573–581. [Google Scholar] [CrossRef]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical Manifestations, Risk Factors, and Maternal and Perinatal Outcomes of Coronavirus Disease 2019 in Pregnancy: Living Systematic Review and Meta-Analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef]
- Sutton, D.; Fuchs, K.; D’Alton, M.; Goffman, D. Universal Screening for SARS-CoV-2 in Women Admitted for Delivery. N. Engl. J. Med. 2020, 382, 2163–2164. [Google Scholar] [CrossRef] [PubMed]
- Hcini, N.; Maamri, F.; Picone, O.; Carod, J.-F.; Lambert, V.; Mathieu, M.; Carles, G.; Pomar, L. Maternal, Fetal and Neonatal Outcomes of Large Series of SARS-CoV-2 Positive Pregnancies in Peripartum Period: A Single-Center Prospective Comparative Study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 257, 11–18. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins—Obstetrics ACOG Practice Bulletin. Clinical Management Guidelines for Obstetrician-Gynecologists. Number 30, September 2001 (Replaces Technical Bulletin Number 200, December 1994). Gestational Diabetes. Obstet. Gynecol. 2001, 98, 525–538. [Google Scholar]
- Cai, J.; Tang, M.; Gao, Y.; Zhang, H.; Yang, Y.; Zhang, D.; Wang, H.; Liang, H.; Zhang, R.; Wu, B. Cesarean Section or Vaginal Delivery to Prevent Possible Vertical Transmission From a Pregnant Mother Confirmed With COVID-19 to a Neonate: A Systematic Review. Front. Med. 2021, 8, 634949. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; More, K.; Chawla, D.; Murki, S.; Tandur, B.; Deorari, A.K.; Dontamala, S.; Sundaram, M.; Anitha, M.; Laxmikant, D.; et al. Outcomes of Neonates Born to Mothers With Coronavirus Disease 2019 (COVID-19)—National Neonatology Forum (NNF) India COVID-19 Registry. Indian Pediatr. 2021, 58, 525–531. [Google Scholar] [CrossRef]
- Prabhu, M.; Cagino, K.; Matthews, K.C.; Friedlander, R.L.; Glynn, S.M.; Kubiak, J.M.; Yang, Y.J.; Zhao, Z.; Baergen, R.N.; DiPace, J.I.; et al. Pregnancy and Postpartum Outcomes in a Universally Tested Population for SARS-CoV-2 in New York City: A Prospective Cohort Study. BJOG 2020, 127, 1548–1556. [Google Scholar] [CrossRef]
- Centeno-Tablante, E.; Medina-Rivera, M.; Finkelstein, J.L.; Rayco-Solon, P.; Garcia-Casal, M.N.; Rogers, L.; Ghezzi-Kopel, K.; Ridwan, P.; Peña-Rosas, J.P.; Mehta, S. Transmission of SARS-CoV-2 through Breast Milk and Breastfeeding: A Living Systematic Review. Ann. N. Y. Acad. Sci. 2021, 1484, 32–54. [Google Scholar] [CrossRef]
- Krogstad, P.; Contreras, D.; Ng, H.; Tobin, N.; Chambers, C.D.; Bertrand, K.; Bode, L.; Aldrovandi, G.M. No Infectious SARS-CoV-2 in Breast Milk from a Cohort of 110 Lactating Women. Pediatr. Res. 2022, 92, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Zozaya, C.; Zhou, Q.; De Castro, C.; Shah, P.S. SARS-CoV-2 Genome and Antibodies in Breastmilk: A Systematic Review and Meta-Analysis. Arch. Dis. Child Fetal Neonatal Ed. 2021, 106, 514–521. [Google Scholar] [CrossRef]
- Unger, S.; Christie-Holmes, N.; Guvenc, F.; Budylowski, P.; Mubareka, S.; Gray-Owen, S.D.; O’Connor, D.L. Holder Pasteurization of Donated Human Milk Is Effective in Inactivating SARS-CoV-2. CMAJ 2020, 192, E871–E874. [Google Scholar] [CrossRef]
- Walker, G.J.; Clifford, V.; Bansal, N.; Stella, A.O.; Turville, S.; Stelzer-Braid, S.; Klein, L.D.; Rawlinson, W. SARS-CoV-2 in Human Milk Is Inactivated by Holder Pasteurisation but Not Cold Storage. J. Paediatr. Child Health 2020, 56, 1872–1874. [Google Scholar] [CrossRef]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; COVID-19 Systematic Urgent Review Group Effort (SURGE) study authors. Physical Distancing, Face Masks, and Eye Protection to Prevent Person-to-Person Transmission of SARS-CoV-2 and COVID-19: A Systematic Review and Meta-Analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Iannone, P.; Castellini, G.; Coclite, D.; Napoletano, A.; Fauci, A.J.; Iacorossi, L.; D’Angelo, D.; Renzi, C.; La Torre, G.; Mastroianni, C.M.; et al. The Need of Health Policy Perspective to Protect Healthcare Workers during COVID-19 Pandemic. A GRADE Rapid Review on the N95 Respirators Effectiveness. PLoS ONE 2020, 15, e0234025. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Ma, N.; Witt, C.; Rapp, S.; Wild, P.S.; Andreae, M.O.; Pöschl, U.; Su, H. Face Masks Effectively Limit the Probability of SARS-CoV-2 Transmission. Science 2021, 372, 1439–1443. [Google Scholar] [CrossRef] [PubMed]
- When and How to Wash Your Hands | Handwashing | CDC. Available online: https://www.cdc.gov/handwashing/when-how-handwashing.html (accessed on 20 January 2023).
- Viner, R.M.; Russell, S.J.; Croker, H.; Packer, J.; Ward, J.; Stansfield, C.; Mytton, O.; Bonell, C.; Booy, R. School Closure and Management Practices during Coronavirus Outbreaks Including COVID-19: A Rapid Systematic Review. Lancet Child Adolesc. Health 2020, 4, 397–404. [Google Scholar] [CrossRef]
- Considerations for School-Related Public Health Measures in the Context of COVID-19. Available online: https://www.who.int/publications-detail-redirect/considerations-for-school-related-public-health-measures-in-the-context-of-covid-19 (accessed on 20 January 2023).
- Suk, J.E.; Vardavas, C.; Nikitara, K.; Phalkey, R.; Leonardi-Bee, J.; Pharris, A.; Wiltshire, E.; Funk, T.; Ferland, L.; Bundle, N.; et al. The Role of Children in the Transmission Chain of SARS-CoV-2: A Systematic Review and Update of Current Evidence. Public Glob. Health 2020, 10, 021101. [Google Scholar]
- Nanavati, R.; Mascarenhas, D.; Goyal, M.; Haribalakrishna, A.; Nataraj, G. A Single-Center Observational Study on Clinical Features and Outcomes of 21 SARS-CoV-2-Infected Neonates from India. Eur. J. Pediatr. 2021, 180, 1895–1906. [Google Scholar] [CrossRef]
- Tao, N.P.H.; Makram, A.M.; Khanh, P.N.Q.; An, N.T.; Safi, A.; Huy, N.T. Negative Impact from School Closures on Children and Parents in Vietnam during COVID-19. Lancet Respir. Med. 2022, 10, 736–738. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.S.; Hill, M.; Antezano, J.; Vilven, D.; Rutner, T.; Bogdanow, L.; Claflin, C.; Kracalik, I.T.; Fields, V.L.; Dunn, A.; et al. Transmission Dynamics of COVID-19 Outbreaks Associated with Child Care Facilities—Salt Lake City, Utah, April–July 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1319–1323. [Google Scholar] [CrossRef]
- Kwok, C.S.; Dashti, M.; Tafuro, J.; Nasiri, M.; Muntean, E.-A.; Wong, N.; Kemp, T.; Hills, G.; Mallen, C.D. Methods to Disinfect and Decontaminate SARS-CoV-2: A Systematic Review of in Vitro Studies. Ther. Adv. Infect. 2021, 8, 2049936121998548. [Google Scholar] [CrossRef]
- Bedrosian, N.; Mitchell, E.; Rohm, E.; Rothe, M.; Kelly, C.; String, G.; Lantagne, D. A Systematic Review of Surface Contamination, Stability, and Disinfection Data on SARS-CoV-2 (Through July 10, 2020). Environ. Sci. Technol. 2021, 55, 4162–4173. [Google Scholar] [CrossRef] [PubMed]
- Shimabukuro, P.M.S.; Duarte, M.L.; Imoto, A.M.; Atallah, Á.N.; Franco, E.S.B.; Peccin, M.S.; Taminato, M. Environmental Cleaning to Prevent COVID-19 Infection. A Rapid Systematic Review. Sao Paulo Med. J. 2020, 138, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Moghadas, S.M.; Vilches, T.N.; Zhang, K.; Wells, C.R.; Shoukat, A.; Singer, B.H.; Meyers, L.A.; Neuzil, K.M.; Langley, J.M.; Fitzpatrick, M.C.; et al. The Impact of Vaccination on Coronavirus Disease 2019 (COVID-19) Outbreaks in the United States. Clin. Infect. Dis. 2021, 73, 2257–2264. [Google Scholar] [CrossRef]
- Gao, P.; Liu, J.; Liu, M. Effect of COVID-19 Vaccines on Reducing the Risk of Long COVID in the Real World: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 12422. [Google Scholar] [CrossRef]
- Badell, M.L.; Dude, C.M.; Rasmussen, S.A.; Jamieson, D.J. COVID-19 Vaccination in Pregnancy. BMJ 2022, 378, e069741. [Google Scholar] [CrossRef]
- Magnus, M.C.; Gjessing, H.K.; Eide, H.N.; Wilcox, A.J.; Fell, D.B.; Håberg, S.E. COVID-19 Vaccination during Pregnancy and First-Trimester Miscarriage. N. Engl. J. Med. 2021, 385, 2008–2010. [Google Scholar] [CrossRef]
- Sadarangani, M.; Soe, P.; Shulha, H.P.; Valiquette, L.; Vanderkooi, O.G.; Kellner, J.D.; Muller, M.P.; Top, K.A.; Isenor, J.E.; McGeer, A.; et al. Safety of COVID-19 Vaccines in Pregnancy: A Canadian National Vaccine Safety (CANVAS) Network Cohort Study. Lancet Infect. Dis. 2022, 22, 1553–1564. [Google Scholar] [CrossRef] [PubMed]
- Halasa, N.B.; Olson, S.M.; Staat, M.A.; Newhams, M.M.; Price, A.M.; Boom, J.A.; Sahni, L.C.; Cameron, M.A.; Pannaraj, P.S.; Bline, K.E.; et al. Effectiveness of Maternal Vaccination with MRNA COVID-19 Vaccine During Pregnancy Against COVID-19-Associated Hospitalization in Infants Aged <6 Months—17 States, July 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 264–270. [Google Scholar] [CrossRef]
- Tian, F.; Yang, R.; Chen, Z. Safety and Efficacy of COVID-19 Vaccines in Children and Adolescents: A Systematic Review of Randomized Controlled Trials. J. Med. Virol. 2022, 94, 4644–4653. [Google Scholar] [CrossRef]
- Safety of MRNA COVID-19 Vaccines during Pregnancy—The Lancet Infectious Diseases. Available online: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(22)00443-1/fulltext (accessed on 19 January 2023).
- COVID-19 Vaccines and Pregnancy: Conversation Guide for Clinicians. Available online: https://www.acog.org/en/covid-19/covid-19-vaccines-and-pregnancy-conversation-guide-for-clinicians (accessed on 19 January 2023).
- Prasad, S.; Kalafat, E.; Blakeway, H.; Townsend, R.; O’Brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; Le Doare, K.; Ladhani, S.; et al. Systematic Review and Meta-Analysis of the Effectiveness and Perinatal Outcomes of COVID-19 Vaccination in Pregnancy. Nat. Commun. 2022, 13, 2414. [Google Scholar] [CrossRef]
- Blakeway, H.; Prasad, S.; Kalafat, E.; Heath, P.T.; Ladhani, S.N.; Le Doare, K.; Magee, L.A.; O’Brien, P.; Rezvani, A.; von Dadelszen, P.; et al. COVID-19 Vaccination during Pregnancy: Coverage and Safety. Am. J. Obstet. Gynecol. 2022, 226, 236.e1–236.e14. [Google Scholar] [CrossRef]
- COVID-19 Protein Subunit Vaccine (Novavax). In Mother To Baby | Fact Sheets; Organization of Teratology Information Specialists (OTIS): Brentwood, TN, USA, 1994. Available online: https://www.ncbi.nlm.nih.gov/books/NBK584981 (accessed on 19 January 2023).
- Vadrevu, K.M.; Reddy, S.; Jogdand, H.; Ganneru, B.; Mirza, N.; Tripathy, V.N.; Singh, C.; Khalatkar, V.; Prasanth, S.; Rai, S.; et al. Immunogenicity and Reactogenicity of an Inactivated SARS-CoV-2 Vaccine (BBV152) in Children Aged 2–18 Years: Interim Data from an Open-Label, Non-Randomised, Age de-Escalation Phase 2/3 Study. Lancet Infect. Dis. 2022, 22, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Citu, I.M.; Citu, C.; Gorun, F.; Sas, I.; Tomescu, L.; Neamtu, R.; Motoc, A.; Gorun, O.M.; Burlea, B.; Bratosin, F.; et al. Immunogenicity Following Administration of BNT162b2 and Ad26.COV2.S COVID-19 Vaccines in the Pregnant Population during the Third Trimester. Viruses 2022, 14, 307. [Google Scholar] [CrossRef] [PubMed]
- Collier, A.-R.Y.; McMahan, K.; Yu, J.; Tostanoski, L.H.; Aguayo, R.; Ansel, J.; Chandrashekar, A.; Patel, S.; Apraku Bondzie, E.; Sellers, D.; et al. Immunogenicity of COVID-19 MRNA Vaccines in Pregnant and Lactating Women. JAMA 2021, 325, 2370–2380. [Google Scholar] [CrossRef]
- Gray, K.J.; Bordt, E.A.; Atyeo, C.; Deriso, E.; Akinwunmi, B.; Young, N.; Baez, A.M.; Shook, L.L.; Cvrk, D.; James, K.; et al. Coronavirus Disease 2019 Vaccine Response in Pregnant and Lactating Women: A Cohort Study. Am. J. Obstet. Gynecol. 2021, 225, 303.e1–303.e17. [Google Scholar] [CrossRef]
- Stock, S.J.; Carruthers, J.; Calvert, C.; Denny, C.; Donaghy, J.; Goulding, A.; Hopcroft, L.E.M.; Hopkins, L.; McLaughlin, T.; Pan, J.; et al. SARS-CoV-2 Infection and COVID-19 Vaccination Rates in Pregnant Women in Scotland. Nat. Med. 2022, 28, 504–512. [Google Scholar] [CrossRef]
- Guedalia, J.; Lipschuetz, M.; Calderon-Margalit, R.; Cohen, S.M.; Goldman-Wohl, D.; Kaminer, T.; Melul, E.; Shefer, G.; Sompolinsky, Y.; Walfisch, A.; et al. Effectiveness of a Third BNT162b2 MRNA COVID-19 Vaccination during Pregnancy: A National Observational Study in Israel. Nat. Commun. 2022, 13, 6961. [Google Scholar] [CrossRef]
- Rottenstreich, A.; Zarbiv, G.; Oiknine-Djian, E.; Vorontsov, O.; Zigron, R.; Kleinstern, G.; Wolf, D.G.; Porat, S. The Effect of Gestational Age at BNT162b2 MRNA Vaccination on Maternal and Neonatal Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Antibody Levels. Clin. Infect. Dis. 2022, 75, e603–e610. [Google Scholar] [CrossRef]
- Yang, Y.J.; Murphy, E.A.; Singh, S.; Sukhu, A.C.; Wolfe, I.; Adurty, S.; Eng, D.; Yee, J.; Mohammed, I.; Zhao, Z.; et al. Association of Gestational Age at Coronavirus Disease 2019 (COVID-19) Vaccination, History of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection, and a Vaccine Booster Dose With Maternal and Umbilical Cord Antibody Levels at Delivery. Obstet. Gynecol. 2022, 139, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Nir, O.; Schwartz, A.; Toussia-Cohen, S.; Leibovitch, L.; Strauss, T.; Asraf, K.; Doolman, R.; Sharabi, S.; Cohen, C.; Lustig, Y.; et al. Maternal-Neonatal Transfer of SARS-CoV-2 Immunoglobulin G Antibodies among Parturient Women Treated with BNT162b2 Messenger RNA Vaccine during Pregnancy. Am. J. Obstet. Gynecol. MFM 2022, 4, 100492. [Google Scholar] [CrossRef]
- Lipkind, H.S.; Vazquez-Benitez, G.; DeSilva, M.; Vesco, K.K.; Ackerman-Banks, C.; Zhu, J.; Boyce, T.G.; Daley, M.F.; Fuller, C.C.; Getahun, D.; et al. Receipt of COVID-19 Vaccine During Pregnancy and Preterm or Small-for-Gestational-Age at Birth—Eight Integrated Health Care Organizations, United States, 15 December 2020–22 July 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 26–30. [Google Scholar] [CrossRef]
- Fell, D.B.; Dhinsa, T.; Alton, G.D.; Török, E.; Dimanlig-Cruz, S.; Regan, A.K.; Sprague, A.E.; Buchan, S.A.; Kwong, J.C.; Wilson, S.E.; et al. Association of COVID-19 Vaccination in Pregnancy With Adverse Peripartum Outcomes. JAMA 2022, 327, 1478–1487. [Google Scholar] [CrossRef]
- Ruderman, R.S.; Mormol, J.; Trawick, E.; Perry, M.F.; Allen, E.C.; Millan, D.; Miller, E.S. Association of COVID-19 Vaccination During Early Pregnancy With Risk of Congenital Fetal Anomalies. JAMA Pediatr. 2022, 176, 717–719. [Google Scholar] [CrossRef] [PubMed]
- SeyedAlinaghi, S.; MohsseniPour, M.; Saeidi, S.; Habibi, P.; Dashti, M.; Nazarian, N.; Noori, T.; Pashaei, Z.; Bagheri, A.; Ghasemzadeh, A.; et al. Complications of COVID-19 Vaccines during Pregnancy; a Systematic Review. Arch. Acad. Emerg. Med. 2022, 10, e76. [Google Scholar] [CrossRef] [PubMed]
- Shimabukuro, T.T.; Kim, S.Y.; Myers, T.R.; Moro, P.L.; Oduyebo, T.; Panagiotakopoulos, L.; Marquez, P.L.; Olson, C.K.; Liu, R.; Chang, K.T.; et al. Preliminary Findings of MRNA COVID-19 Vaccine Safety in Pregnant Persons. N. Engl. J. Med. 2021, 384, 2273–2282. [Google Scholar] [CrossRef]
- Bookstein Peretz, S.; Regev, N.; Novick, L.; Nachshol, M.; Goffer, E.; Ben-David, A.; Asraf, K.; Doolman, R.; Gal Levin, E.; Regev Yochay, G.; et al. Short-term Outcome of Pregnant Women Vaccinated with BNT162b2 MRNA COVID-19 Vaccine. Ultrasound Obstet. Gynecol. 2021, 58, 450–456. [Google Scholar] [CrossRef] [PubMed]
- CDC COVID-19 Vaccination. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/stay-up-to-date.html (accessed on 30 January 2023).
- Amir, O.; Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Ash, N.; Alroy-Preis, S.; Huppert, A.; Milo, R. Protection Following BNT162b2 Booster in Adolescents Substantially Exceeds That of a Fresh 2-Dose Vaccine. Nat. Commun. 2022, 13, 1971. [Google Scholar] [CrossRef]
- Chemaitelly, H.; AlMukdad, S.; Ayoub, H.H.; Altarawneh, H.N.; Coyle, P.; Tang, P.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Hasan, M.R.; et al. COVID-19 Vaccine Protection among Children and Adolescents in Qatar. N. Engl. J. Med. 2022, 387, 1865–1876. [Google Scholar] [CrossRef]
- Irving, S.A.; Klein, N.P. COVID-19 Vaccination Protects Children and Adolescents. Lancet Infect. Dis. 2023, 23, 5–6. [Google Scholar] [CrossRef]
- Fowlkes, A.L.; Yoon, S.K.; Lutrick, K.; Gwynn, L.; Burns, J.; Grant, L.; Phillips, A.L.; Ellingson, K.; Ferraris, M.V.; LeClair, L.B.; et al. Effectiveness of 2-Dose BNT162b2 (Pfizer BioNTech) MRNA Vaccine in Preventing SARS-CoV-2 Infection Among Children Aged 5–11 Years and Adolescents Aged 12–15 Years—PROTECT Cohort, July 2021–February 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 422–428. [Google Scholar] [CrossRef]
- Shi, D.S.; Whitaker, M.; Marks, K.J.; Anglin, O.; Milucky, J.; Patel, K.; Pham, H.; Chai, S.J.; Kawasaki, B.; Meek, J.; et al. Hospitalizations of Children Aged 5–11 Years with Laboratory-Confirmed COVID-19—COVID-NET, 14 States, March 2020–February 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 574–581. [Google Scholar] [CrossRef]
- Jara, A.; Undurraga, E.A.; Zubizarreta, J.R.; González, C.; Acevedo, J.; Pizarro, A.; Vergara, V.; Soto-Marchant, M.; Gilabert, R.; Flores, J.C.; et al. Effectiveness of CoronaVac in Children 3-5 Years of Age during the SARS-CoV-2 Omicron Outbreak in Chile. Nat. Med. 2022, 28, 1377–1380. [Google Scholar] [CrossRef] [PubMed]
- Zambrano, L.D. Effectiveness of BNT162b2 (Pfizer-BioNTech) MRNA Vaccination Against Multisystem Inflammatory Syndrome in Children Among Persons Aged 12–18 Years—United States, July–December 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Amir, O.; Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Ash, N.; Alroy-Preis, S.; Huppert, A.; Milo, R. Initial Protection against SARS-CoV-2 Omicron Lineage Infection in Children and Adolescents by BNT162b2 in Israel: An Observational Study. Lancet Infect. Dis. 2023, 23, 67–73. [Google Scholar] [CrossRef]
- Hause, A.M. COVID-19 Vaccine Safety in Children Aged 5–11 Years—United States, 3 November–19December 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1755–1760. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, R.; Dubey, S.; Roy, D.; Mandal, A.; Naga, D.; Benito-León, J. Focal Onset Non-Motor Seizure Following COVID-19 Vaccination: A Mere Coincidence? Diabetes Metab. Syndr. 2021, 15, 1023–1024. [Google Scholar] [CrossRef]
- Fernandez-Davila, N.; Taylor, M.G.; Anvari, S. Hypersensitivity Reactions to COVID-19 Vaccines—Identify High-Risk Children and Vaccinate the Rest. JAMA Pediatr. 2022, 176, 443–444. [Google Scholar] [CrossRef]
- Oster, M.E.; Shay, D.K.; Su, J.R.; Gee, J.; Creech, C.B.; Broder, K.R.; Edwards, K.; Soslow, J.H.; Dendy, J.M.; Schlaudecker, E.; et al. Myocarditis Cases Reported After MRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021. JAMA 2022, 327, 331–340. [Google Scholar] [CrossRef] [PubMed]
- See, I.; Lale, A.; Marquez, P.; Streiff, M.B.; Wheeler, A.P.; Tepper, N.K.; Woo, E.J.; Broder, K.R.; Edwards, K.M.; Gallego, R.; et al. Case Series of Thrombosis With Thrombocytopenia Syndrome After COVID-19 Vaccination—United States, December 2020 to August 2021. Ann. Intern. Med. 2022, 175, 513–522. [Google Scholar] [CrossRef]
- Alwafi, H.; Naser, A.Y.; Aldhahir, A.M.; Alhazmi, A.; Alosaimi, A.N.; Mandili, R.A.; Majeed, Z.; Salawati, E.; Ekram, R.; Samannodi, M.; et al. COVID-19 Vaccination Side Effects among the Child Age Group: A Large Cross-Sectional Online Based Survey in Saudi Arabia. BMC Infect. Dis. 2022, 22, 911. [Google Scholar] [CrossRef]
- Alamer, E.; Alhazmi, A.; Qasir, N.A.; Alamer, R.; Areeshi, H.; Gohal, G.; Qadri, M.; Hashem, A.M.; Algaissi, A. Side Effects of COVID-19 Pfizer-BioNTech MRNA Vaccine in Children Aged 12–18 Years in Saudi Arabia. Vaccines 2021, 9, 1297. [Google Scholar] [CrossRef]
- Baraniuk, C. COVID-19: How the UK Vaccine Rollout Delivered Success, so Far. BMJ 2021, 372, n421. [Google Scholar] [CrossRef]
- Saad-Roy, C.M.; Morris, S.E.; Metcalf, C.J.E.; Mina, M.J.; Baker, R.E.; Farrar, J.; Holmes, E.C.; Pybus, O.G.; Graham, A.L.; Levin, S.A.; et al. Epidemiological and Evolutionary Considerations of SARS-CoV-2 Vaccine Dosing Regimes. Science 2021, 372, 363–370. [Google Scholar] [CrossRef]
- COVID-19: New Data on Oxford AstraZeneca Vaccine Backs 12 Week Dosing Interval. Available online: https://en.x-mol.com/paper/article/1357103759308996608 (accessed on 31 January 2023).
- Times, G. Vaccination for Children Aged 3–11 Launched across China amid Rebound of COVID-19 Cases—Global Times. Available online: https://www.globaltimes.cn/page/202110/1237372.shtml (accessed on 30 January 2023).
- Department of Health and Aged Care. COVID-19 Vaccines for Children. Available online: https://www.health.gov.au/our-work/covid-19-vaccines/who-can-get-vaccinated/children (accessed on 30 January 2023).
- Kasi, S.G.; Dhir, S.K.; Shah, A.; Shivananda, S.; Verma, S.; Marathe, S.; Chatterjee, K.; Agarwalla, S.; Srirampur, S.; Kalyani, S.; et al. Coronavirus Disease 2019 (COVID-19) Vaccination for Children: Position Statement of Indian Academy of Pediatrics Advisory Committee on Vaccination and Immunization Practices. Indian Pediatr. 2022, 59, 51–57. [Google Scholar] [CrossRef]
- Stuart, A.S.V.; Shaw, R.H.; Liu, X.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Immunogenicity, Safety, and Reactogenicity of Heterologous COVID-19 Primary Vaccination Incorporating MRNA, Viral-Vector, and Protein-Adjuvant Vaccines in the UK (Com-COV2): A Single-Blind, Randomised, Phase 2, Non-Inferiority Trial. Lancet 2022, 399, 36–49. [Google Scholar] [CrossRef]
- R-Pharm A Phase I/II Single-Blinded Randomized Safety and Immunogenicity Study in Adults of AZD1222 and RAd26-S Administered as Heterologous Prime Boost Regimen for the Prevention of COVID 19. Available online: https://www.clinicaltrials.gov/ct2/show/NCT04760730 (accessed on 2 February 2023).
- D’Amico, F.; Rabaud, C.; Peyrin-Biroulet, L.; Danese, S. SARS-CoV-2 Vaccination in IBD: More Pros than Cons. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 211–213. [Google Scholar] [CrossRef]
- Department of Health and Aged Care. ATAGI Recommendations on COVID-19 Vaccine Use in Children Aged 6 Months To <5 Year. Available online: https://www.health.gov.au/news/atagi-recommendations-on-covid-19-vaccine-use-in-children-aged-6-months-to (accessed on 2 February 2023).
- Sonani, B.; Aslam, F.; Goyal, A.; Patel, J.; Bansal, P. COVID-19 Vaccination in Immunocompromised Patients. Clin. Rheumatol. 2021, 40, 797–798. [Google Scholar] [CrossRef] [PubMed]
- Reis, B.Y.; Barda, N.; Leshchinsky, M.; Kepten, E.; Hernán, M.A.; Lipsitch, M.; Dagan, N.; Balicer, R.D. Effectiveness of BNT162b2 Vaccine against Delta Variant in Adolescents. N. Engl. J. Med. 2021, 385, 2101–2103. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-N.; Huang, Y.; Wang, W.; Jing, Q.-L.; Zhang, C.-H.; Qin, P.-Z.; Guan, W.-J.; Gan, L.; Li, Y.-L.; Liu, W.-H.; et al. Effectiveness of Inactivated SARS-CoV-2 Vaccines against the Delta Variant Infection in Guangzhou: A Test-Negative Case-Control Real-World Study. Emerg. Microbes. Infect. 2021, 10, 1751–1759. [Google Scholar] [CrossRef]
- Lu, L.; Mok, B.W.Y.; Chen, L.L.; Chan, J.M.C.; Tsang, O.T.Y.; Lam, B.H.S.; Chuang, V.W.M.; Chu, A.W.H.; Chan, W.M.; Ip, J.D.; et al. Neutralization of Severe Acute Respiratory Syndrome Coronavirus 2 Omicron Variant by Sera From BNT162b2 or CoronaVac Vaccine Recipients. Clin. Infect. Dis. 2022, 75, e822–e826. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Li, Q.; Liang, Z.; Li, T.; Liu, S.; Cui, Q.; Nie, J.; Wu, Q.; Qu, X.; Huang, W.; et al. The Significant Immune Escape of Pseudotyped SARS-CoV-2 Variant Omicron. Emerg. Microbes. Infect. 2022, 11, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-L.; Chua, G.T.; Lu, L.; Chan, B.P.-C.; Wong, J.S.-C.; Chow, C.C.-K.; Yu, T.-C.; Leung, A.S.-Y.; Lam, S.-Y.; Wong, T.-W.; et al. Omicron Variant Susceptibility to Neutralizing Antibodies Induced in Children by Natural SARS-CoV-2 Infection or COVID-19 Vaccine. Emerg. Microbes Infect. 2022, 11, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Chen, L.; Shi, Y. Booster COVID-19 Vaccination against the SARS-CoV-2 Omicron Variant: A Systematic Review. Hum. Vaccin. Immunother. 2022, 18, 2062983. [Google Scholar] [CrossRef]
- Zimmermann, P.; Pittet, L.F.; Finn, A.; Pollard, A.J.; Curtis, N. Should Children Be Vaccinated against COVID-19? Arch. Dis. Child. 2022, 107, e1–e8. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A Global Survey of Potential Acceptance of a COVID-19 Vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Latkin, C.; Dayton, L.A.; Yi, G.; Konstantopoulos, A.; Park, J.; Maulsby, C.; Kong, X. COVID-19 Vaccine Intentions in the United States, a Social-Ecological Framework. Vaccine 2021, 39, 2288–2294. [Google Scholar] [CrossRef]
- Grumbach, K.; Judson, T.; Desai, M.; Jain, V.; Lindan, C.; Doernberg, S.B.; Holubar, M. Association of Race/Ethnicity With Likeliness of COVID-19 Vaccine Uptake Among Health Workers and the General Population in the San Francisco Bay Area. JAMA Intern. Med. 2021, 181, 1008–1011. [Google Scholar] [CrossRef]
- Momplaisir, F.; Haynes, N.; Nkwihoreze, H.; Nelson, M.; Werner, R.M.; Jemmott, J. Understanding Drivers of Coronavirus Disease 2019 Vaccine Hesitancy Among Blacks. Clin. Infect. Dis. 2021, 73, 1784–1789. [Google Scholar] [CrossRef]
- Riad, A.; Pokorná, A.; Antalová, N.; Krobot, M.; Zviadadze, N.; Serdiuk, I.; Koščík, M.; Klugar, M. Prevalence and Drivers of COVID-19 Vaccine Hesitancy among Czech University Students: National Cross-Sectional Study. Vaccines 2021, 9, 948. [Google Scholar] [CrossRef]
- Skeens, M.A.; Hill, K.; Olsavsky, A.; Buff, K.; Stevens, J.; Akard, T.F.; Shah, N.; Gerhardt, C.A. Factors Affecting COVID-19 Vaccine Hesitancy in Parents of Children with Cancer. Pediatr. Blood Cancer 2022, 69, e29707. [Google Scholar] [CrossRef]
- Fisher, C.B.; Bragard, E.; Jaber, R.; Gray, A. COVID-19 Vaccine Hesitancy among Parents of Children under Five Years in the United States. Vaccines 2022, 10, 1313. [Google Scholar] [CrossRef] [PubMed]
- Olick, R.S.; Shaw, J.; Yang, Y.T. Ethical Issues in Mandating COVID-19 Vaccination for Health Care Personnel. Mayo Clin. Proc. 2021, 96, 2958–2962. [Google Scholar] [CrossRef] [PubMed]
- Bardosh, K.; de Figueiredo, A.; Gur-Arie, R.; Jamrozik, E.; Doidge, J.; Lemmens, T.; Keshavjee, S.; Graham, J.E.; Baral, S. The Unintended Consequences of COVID-19 Vaccine Policy: Why Mandates, Passports and Restrictions May Cause More Harm than Good. BMJ Glob. Health 2022, 7, e008684. [Google Scholar] [CrossRef] [PubMed]
- Atuire, C.A.; Salas, S.P.; Wright, K.; Ambe, J.R.; de Vries, J. COVID-19 Vaccine Trials with Children: Ethics Pointers. BMJ Glob. Health 2022, 7, e007466. [Google Scholar] [CrossRef]
- Cabiedes-Miragaya, L.; Galende-Domínguez, I. COVID-19 Vaccines: A Look at the Ethics of the Clinical Research Involving Children. J. Med. Ethics 2022, 48, 666–671. [Google Scholar] [CrossRef]



{kind=link}
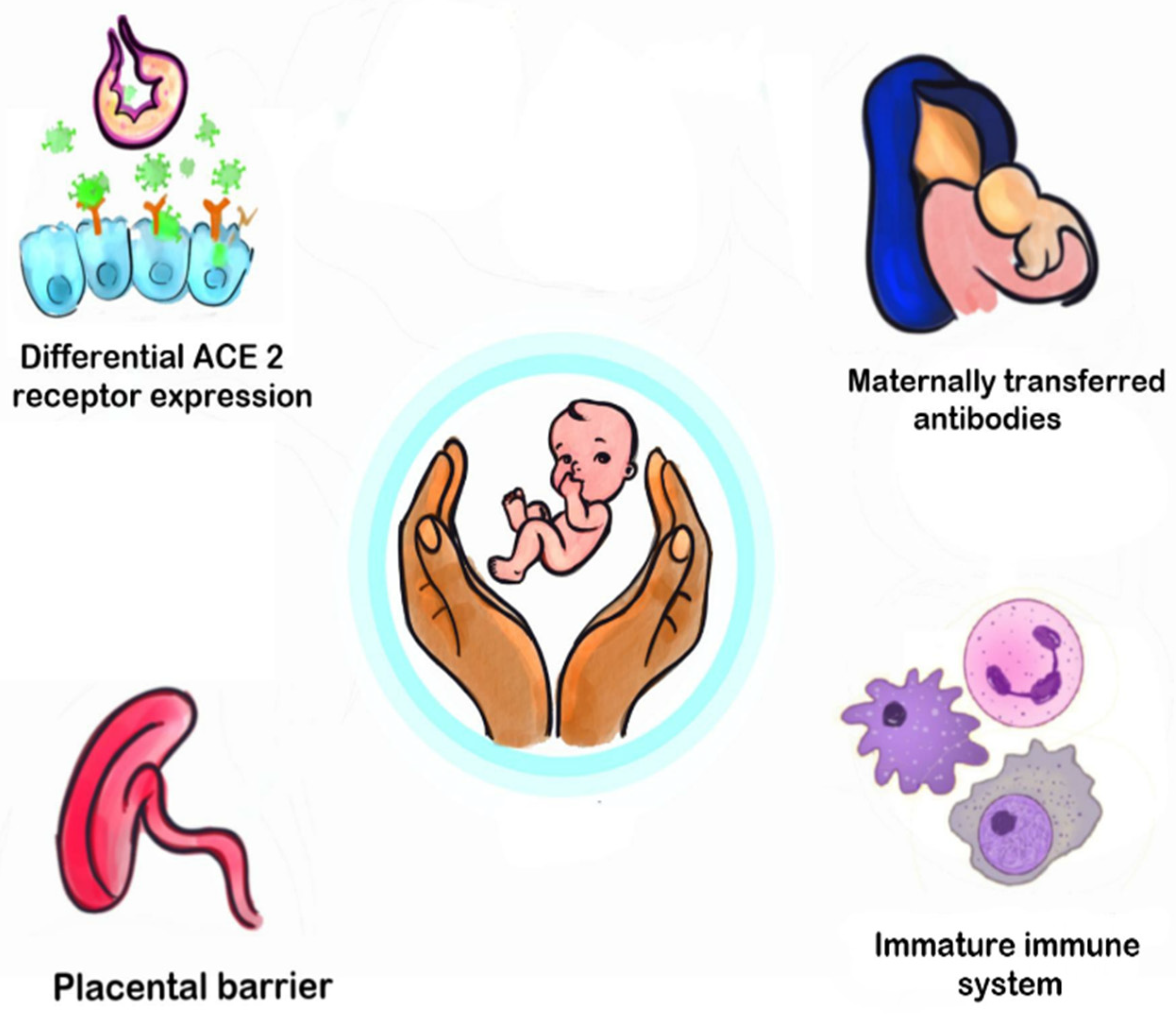{kind=link}
| Mechanism | Evidence (Direct/Indirect) | Knowledge Gaps |
|---|---|---|
| Placenta—barrier for preventing viral transmission |
|
|
| Receptor expression—decreased attachment of virus |
| |
| Immature Immune system—immune tolerance and faster response to novel antigens |
| |
| Maternal Immune transfer—transfer of protective antibodies |
| |
| Breast milk—transfer of antibodies and live cells |
| |
| Microbiota—presence of beneficial commensal microbes |
|
|
| Developing lung—better healing and less fibrosis |
| |
| Melatonin-anti-inflammatory and antioxidant |
| |
| Vaccine off-target effect—trained immunity |
|
|
| Strategy | Evidence (Direct/Indirect) | Recommendations |
|---|---|---|
| Universal screening for COVID-19 disease in pregnant women |
| |
| Mode and timing of delivery |
|
|
| Protected rooming-in of newborn | Rooming-in with COVID-19-positive mother confers a higher risk of infection in the newborn [131]. Infection control measures can reduce the risk of postnatal transmission [132]. Benefits of rooming-in are based on the following Rooming-in promotes exclusive breast feeding Breastfeeding reduces neonatal mortality Neonatal infection is mostly mild/asymptomatic. |
|
| Breastfeeding |
|
|
| Pasteurization of milk |
| |
| Face masks |
| |
| Hand hygiene |
|
|
| School closure/lockdown strategy |
| |
| Isolation of positive neonates |
|
|
| Environmental disinfection |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pillai, A.; Nayak, A.; Tiwari, D.; Pillai, P.K.; Pandita, A.; Sakharkar, S.; Balasubramanian, H.; Kabra, N. COVID-19 Disease in Under-5 Children: Current Status and Strategies for Prevention including Vaccination. Vaccines 2023, 11, 693. https://doi.org/10.3390/vaccines11030693
Pillai A, Nayak A, Tiwari D, Pillai PK, Pandita A, Sakharkar S, Balasubramanian H, Kabra N. COVID-19 Disease in Under-5 Children: Current Status and Strategies for Prevention including Vaccination. Vaccines. 2023; 11(3):693. https://doi.org/10.3390/vaccines11030693
Chicago/Turabian StylePillai, Anish, Anuja Nayak, Deepika Tiwari, Pratichi Kadam Pillai, Aakash Pandita, Sachin Sakharkar, Haribalakrishna Balasubramanian, and Nandkishor Kabra. 2023. "COVID-19 Disease in Under-5 Children: Current Status and Strategies for Prevention including Vaccination" Vaccines 11, no. 3: 693. https://doi.org/10.3390/vaccines11030693