

COVID-19 Vaccine Booster Shot Preserves T Cells Immune Response Based on Interferon-Gamma Release Assay in Inflammatory Bowel Disease (IBD) Patients on Anti-TNFα Treatment
 , , , , , ,
, , , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. IBD Patient Cohort
2.3. SARS-CoV-2 Humoral Immune Response
2.4. SARS-CoV-2 Cellular Immune Response
2.5. Statistical Analysis
3. Results
3.1. Cohort Characteristics
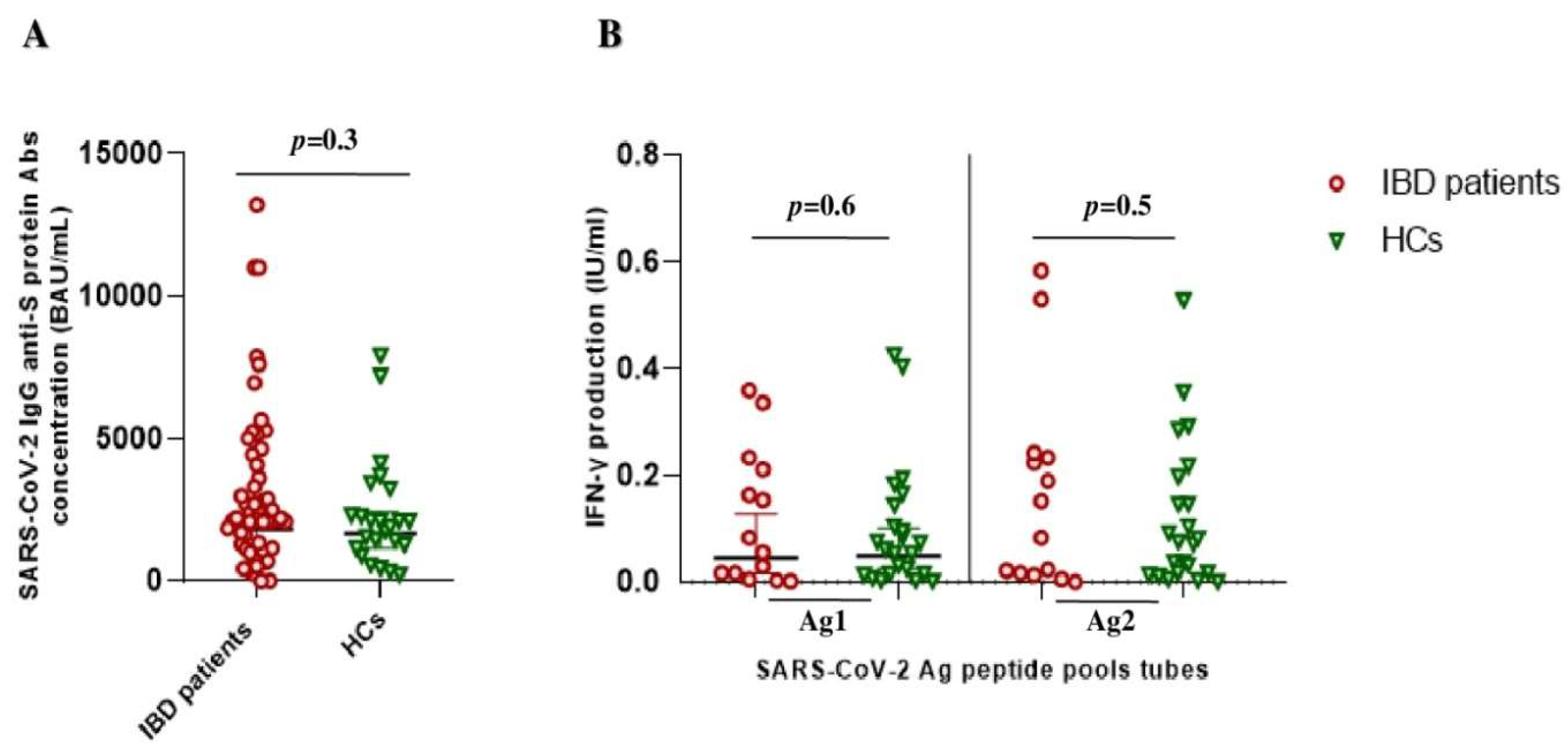
3.2. SARS-CoV-2 Vaccine-Induced Immune Response in IBD Patients vs. HCs
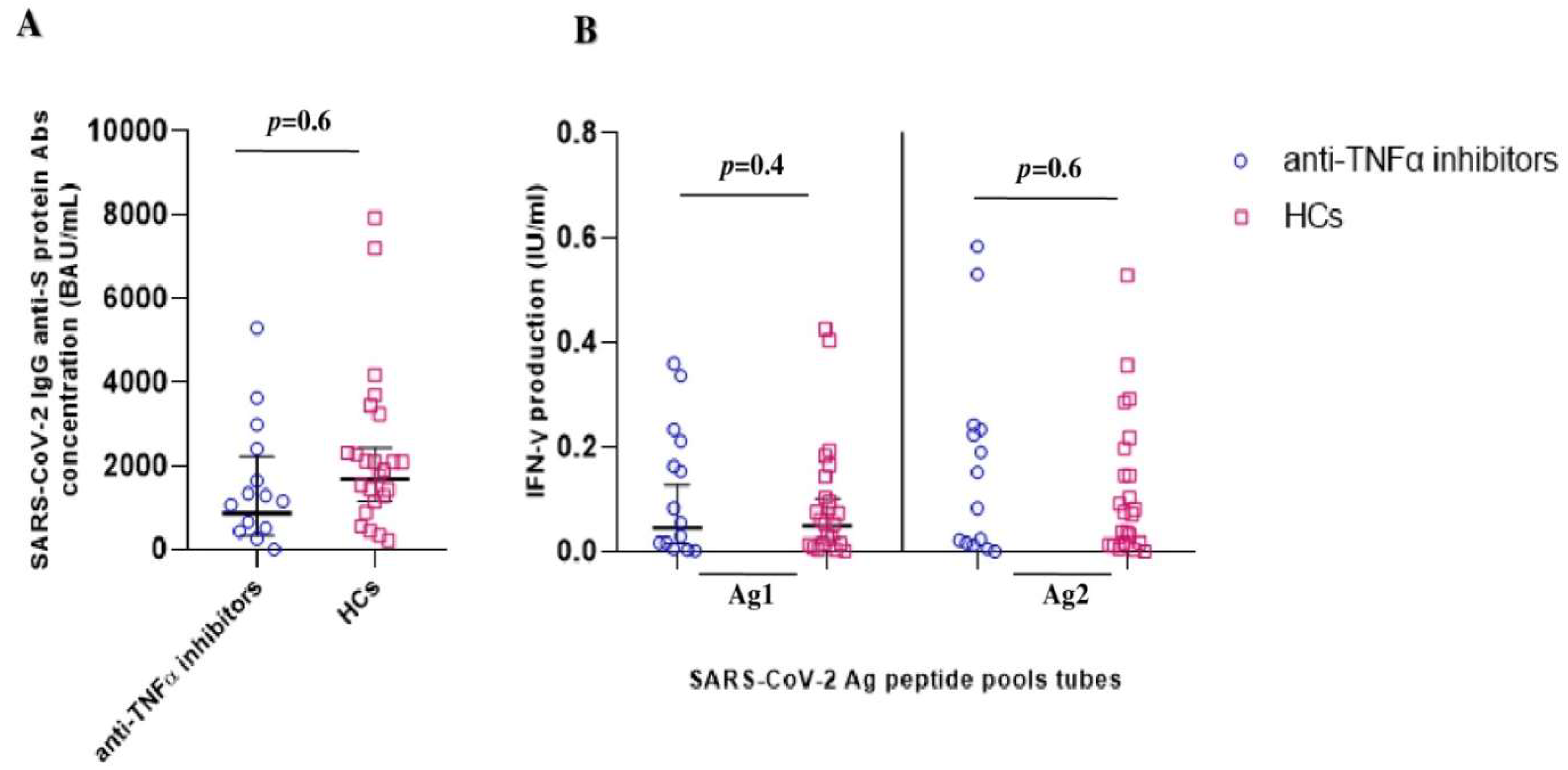
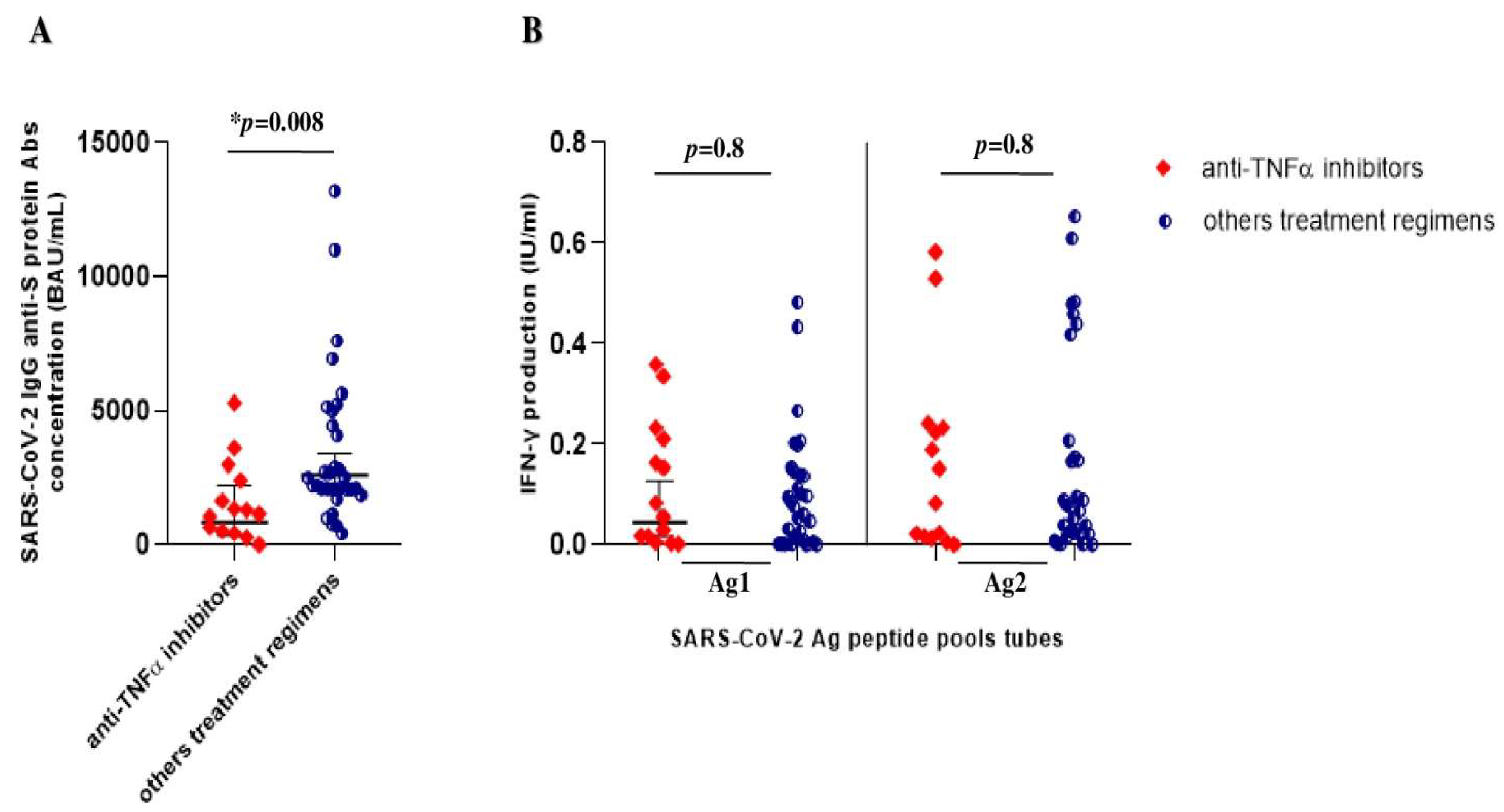
3.3. SARS-CoV-2 Vaccine-Induced Immune Response in IBD Patients on TNFα Inhibitors vs. Others Treatment Regimens
3.4. Correlation between COVID-19 Vaccine-Elicited Humoral and Cellular Immune Responses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abraham, C.; Cho, J.H. Inflammatory bowel disease. N. Engl. J. Med. 2009, 361, 2066–2078. [Google Scholar] [CrossRef]
- Focà, A.; Liberto, M.C.; Quirino, A.; Marascio, N.; Zicca, E.; Pavia, G. Gut inflammation and immunity: What is the role of the human gut virome? Mediat. Inflamm. 2015, 2015, 326032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Ungaro, R.; Mehandru, S.; Allen, P.B.; Peyrin-Biroulet, L.; Colombel, J.F. Ulcerative colitis. Lancet 2017, 389, 1756–1770. [Google Scholar] [CrossRef] [PubMed]
- Zundler, S.; Günther, C.; Kremer, A.E.; Zaiss, M.M.; Rothhammer, V.; Neurath, M.F. Gut immune cell trafficking: Inter-organ communication and immune-mediated inflammation. Nat. Rev. Gastroenterol. Hepatol. 2023, 20, 50–64. [Google Scholar] [CrossRef] [PubMed]
- Spagnuolo, R.; Basile, A.; Corea, A.; Iaquinta, F.S.; Milić, N.; Doldo, P.; Luzza, F.; Abenavoli, L. Measuring Mood and Anxiety Disorders by Patient Reported Outcomes in Inflammatory Bowel Disease: A Literature Review Update. Rev. Recent Clin. Trials 2022. published online ahead of print. [Google Scholar] [CrossRef]
- Liuzza, M.T.; Spagnuolo, R.; Antonucci, G.; Grembiale, R.D.; Cosco, C.; Iaquinta, F.S.; Funari, V.; Dastoli, S.; Nistico, S.; Doldo, P. Psychometric evaluation of an Italian custom 4-item short form of the PROMIS anxiety item bank in immune-mediated inflammatory diseases: An item response theory analysis. PeerJ 2021, 9, e12100. [Google Scholar] [CrossRef]
- Singh, S.; Fumery, M.; Sandborn, W.J.; Murad, M.H. Systematic review with network meta-analysis: First- and second-line pharmacotherapy for moderate-severe ulcerative colitis. Aliment. Pharmacol. Ther. 2018, 47, 162–175. [Google Scholar] [CrossRef]
- Cai, Z.; Wang, S.; Li, J. Treatment of Inflammatory Bowel Disease: A Comprehensive Review. Front. Med. 2021, 8, 765474. [Google Scholar] [CrossRef]
- Singh, S.; Murad, M.H.; Fumery, M.; Sedano, R.; Jairath, V.; Panaccione, R.; Sandborn, W.J.; Ma, C. Comparative efficacy and safety of biologic therapies for moderate-to-severe Crohn’s disease: A systematic review and network meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 1002–1014. [Google Scholar] [CrossRef]
- Quirino, A.; Marascio, N.; Barreca, G.S.; Gallo, L.; Giancotti, A.; Lamberti, A.G.; Peronace, C.; Trecarichi, E.M.; Fusco, P.; Mazzitelli, M.; et al. SARS-CoV-2: Some Aspects of Molecular Evolution, Cellular Pathogenesis, and Immune System Mechanism Elusion. Appl. Sci. 2021, 11, 11605. [Google Scholar] [CrossRef]
- Spagnuolo, R.; Larussa, T.; Iannelli, C.; Cosco, C.; Nisticò, E.; Manduci, E.; Bruno, A.; Boccuto, L.; Abenavoli, L.; Luzza, F.; et al. COVID-19 and Inflammatory Bowel Disease: Patient Knowledge and Perceptions in a Single Center Survey. Medicina 2020, 56, 407. [Google Scholar] [CrossRef] [PubMed]
- Pratt, P.K., Jr.; David, N.; Weber, H.C.; Little, F.F.; Kourkoumpetis, T.; Patts, G.J.; Weinberg, J.; Farraye, F.A. Antibody response to hepatitis B virus vaccine is impaired in patients with inflammatory bowel disease on infliximab therapy. Inflamm. Bowel. Dis. 2018, 24, 380–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiorino, G.; Peyrin-Biroulet, L.; Naccarato, P.; Szabò, H.; Sociale, O.R.; Vetrano, S.; Fries, W.; Montanelli, A.; Repici, A.; Malesci, A.; et al. Effects of immunosuppression on immune response to pneumococcal vaccine in inflammatory bowel disease: A prospective study. Inflamm. Bowel. Dis. 2012, 18, 1042–1047. [Google Scholar] [CrossRef] [PubMed]
- Melmed, G.Y.; Agarwal, N.; Frenck, R.W.; Ippoliti, A.F.; Ibanez, P.; Papadakis, K.A.; Simpson, P.; Barolet-Garcia, C.; Ward, J.; Targan, S.R.; et al. Immunosuppression impairs response to pneumococcal polysaccharide vaccination in patients with inflammatory bowel disease. Am. J. Gastroenterol. 2010, 105, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Mamula, P.; Markowitz, J.E.; Piccoli, D.A.; Klimov, A.; Cohen, L.; Baldassano, R.N. Immune response to influenza vaccine in pediatric patients with inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2007, 5, 851–856. [Google Scholar] [CrossRef]
- Park, S.H.; Yang, S.K.; Park, S.K.; Kim, J.W.; Yang, D.H.; Jung, K.W.; Kim, K.J.; Ye, B.D.; Byeon, J.S.; Myung, S.J.; et al. Efficacy of hepatitis A vaccination and factors impacting on seroconversion in patients with inflammatory bowel disease. Inflamm. Bowel. Dis. 2014, 20, 69–74. [Google Scholar] [CrossRef]
- Hagihara, Y.; Ohfuji, S.; Watanabe, K.; Yamagami, H.; Fukushima, W.; Maeda, K.; Kamata, N.; Sogawa, M.; Shiba, M.; Tanigawa, T.; et al. Infliximab and/or immunomodulators inhibit immune responses to trivalent influenza vaccination in adults with inflammatory bowel disease. J. Crohn’s Colitis 2014, 8, 223–233. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Jacobson, D.L.; Ashworth, L.A.; Grand, R.J.; Meyer, A.L.; McNeal, M.M.; Gregas, M.C.; Burchett, S.K.; Bousvaros, A. Immune response to influenza vaccine in children with inflammatory bowel disease. Am. J. Gastroenterol. 2009, 104, 444–453. [Google Scholar] [CrossRef]
- Wyant, T.; Leach, T.; Sankoh, S.; Wang, Y.; Paolino, J.; Pasetti, M.F.; Feagan, B.G.; Parikh, A. Vedolizumab affects antibody responses to immunisation selectively in the gastrointestinal tract: Randomised controlled trial results. Gut 2015, 64, 77–83. [Google Scholar] [CrossRef]
- Doornekamp, L.; Goetgebuer, R.L.; Schmitz, K.S.; Goeijenbier, M.; van der Woude, C.J.; Fouchier, R.; van Gorp, E.C.M.; de Vries, A.C. High immunogenicity to influenza vaccination in Crohn’s disease patients treated with ustekinumab. Vaccines 2020, 8, 455. [Google Scholar] [CrossRef]
- Kappelman, M.D.; Weaver, K.N.; Boccieri, M.; Firestine, A.; Zhang, X.; Long, M.D.; PREVENT-COVID Study Group. Humoral Immune Response to Messenger RNA COVID-19 Vaccines Among Patients With Inflammatory Bowel Disease. Gastroenterology 2021, 161, 1340–1343.e2. [Google Scholar] [CrossRef]
- Kennedy, N.A.; Goodhand, J.R.; Bewshea, C.; Nice, R.; Chee, D.; Lin, S.; Chanchlani, N.; Butterworth, J.; Cooney, R.; Croft, N.M.; et al. Anti-SARS-CoV-2 antibody responses are attenuated in patients with IBD treated with infliximab. Gut 2021, 70, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.L.; Kennedy, N.A.; Ibraheim, H.; Anandabaskaran, S.; Saifuddin, A.; Castro Seoane, R.; Liu, Z.; Nice, R.; Bewshea, C.; D’Mello, A.; et al. COVID-19 vaccine-induced antibody responses in immunosuppressed patients with inflammatory bowel disease (VIP): A multicentre, prospective, case-control study. Lancet Gastroenterol. Hepatol. 2022, 7, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Macaluso, F.S.; Principi, M.; Facciotti, F.; Contaldo, A.; Todeschini, A.; Saibeni, S.; Bezzio, C.; Castiglione, F.; Nardone, O.M.; Spagnuolo, R.; et al. Reduced humoral response to two doses of COVID-19 vaccine in patients with inflammatory bowel disease: Data from ESCAPE-IBD, an IG-IBD study. Dig. Liver Dis. 2022, 55, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Kennedy, N.A.; Saifuddin, A.; Sandoval, D.M.; Reynolds, C.J.; Seoane, R.C.; Kottoor, S.H.; Pieper, F.P.; Lin, K.M.; Butler, D.K.; et al. Antibody decay, T cell immunity and breakthrough infections following two SARS-CoV-2 vaccine doses in inflammatory bowel disease patients treated with infliximab and vedolizumab. Nat. Commun. 2022, 13, 1379. [Google Scholar] [CrossRef]
- Jena, A.; James, D.; Singh, A.K.; Dutta, U.; Sebastian, S.; Sharma, V. Effectiveness and durability of COVID-19 vaccination in 9447 patients with IBD: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2022, 20, 1456–1479.e18. [Google Scholar] [CrossRef] [PubMed]
- Frey, S.; Chowdhury, R.; Connolly, C.M.; Werbel, W.A.; Segev, D.L.; Parian, A.M.; IBD GROUP. Antibody Response Six Months after SARS-CoV-2 mRNA Vaccination in Patients with Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2022, 20, 1609–1612.e1. [Google Scholar] [CrossRef]
- DiPiazza, A.T.; Graham, B.S.; Ruckwardt, T.J. T Cell Immunity to SARS-CoV-2 Following Natural Infection and Vaccination. Biochem. Biophys. Res. Commun. 2021, 538, 211–217. [Google Scholar] [CrossRef]
- McMahan, K.; Yu, J.; Mercado, N.B.; Loos, C.; Tostanoski, L.H.; Chandrashekar, A.; Liu, J.; Peter, L.; Atyeo, C.; Zhu, A.; et al. Correlates of protection against SARS-CoV-2 in rhesus macaques. Nature 2021, 590, 630–634. [Google Scholar] [CrossRef]
- Reuken, P.A.; Andreas, N.; Grunert, P.C.; Glöckner, S.; Kamradt, T.; Stallmach, A. T Cell Response After SARS-CoV-2 Vaccination in Immunocompromised Patients With Inflammatory Bowel Disease. J. Crohns Colitis. 2022, 16, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Vollenberg, R.; Tepasse, P.R.; Kühn, J.E.; Hennies, M.; Strauss, M.; Rennebaum, F.; Schomacher, T.; Boeckel, G.; Lorentzen, E.; Bokemeyer, A.; et al. Humoral Immune Response in IBD Patients Three and Six Months After Vaccination With the SARS-CoV-2 mRNA Vaccines mRNA-1273 and BNT162b2. Biomedicines 2022, 10, 171. [Google Scholar] [CrossRef] [PubMed]
- Cerna, K.; Duricova, D.; Hindos, M.; HindosHrebackova, J.; Lukas, M.; Machkova, N.; Hruba, V.; Mitrova, K.; Kubickova, K.; Kastylova, K.; et al. Cellular and Humoral Immune Responses to SARS-CoV-2 Vaccination in Inflammatory Bowel Disease Patients. J. Crohns Colitis. 2022, 16, 1347–1353. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Xu, A.; Mengesha, E.; Elyanow, R.; Gittelman, R.M.; Chapman, H.; Prostko, J.C.; Frias, E.C.; Stewart, J.L.; Pozdnyakova, V.; et al. The T-Cell Response to SARS-CoV-2 Vaccination in Inflammatory Bowel Disease is Augmented with Anti-TNF Therapy. Inflamm. Bowel Dis. 2022, 28, 1130–1133. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.L.; Liu, Z.; Muñoz Sandoval, D.; Reynolds, C.; Ibraheim, H.; Anandabaskaran, S.; Saifuddin, A.; Castro Seoane, R.; Anand, N.; Nice, R.; et al. COVID-19 vaccine-induced antibody and T-cell responses in immunosuppressed patients with inflammatory bowel disease after the third vaccine dose (VIP): A multicentre, prospective, case-control study. Lancet Gastroenterol. Hepatol. 2022, 8, 1005–1015. [Google Scholar] [CrossRef]
- Jaganathan, S.; Stieber, F.; Rao, S.N.; Nikolayevskyy, V.; Manissero, D.; Allen, N.; Boyle, J.; Howard, J. Preliminary Evaluation of QuantiFERON SARS-CoV-2 and QIAreach Anti- SARS-CoV-2 Total Test in Recently Vaccinated Individuals. Infect. Dis. Ther. 2021, 10, 2765–2776. [Google Scholar] [CrossRef]
- Martínez-Gallo, M.; Esperalba, J.; Pujol-Borrell, R.; Sandá, V.; Arrese-Muñoz, I.; Fernández-Naval, C.; Antón, A.; Cardona, V.; Labrador-Horrillo, M.; Pumarola, T.; et al. Commercialized Kits to Assess T-Cell Responses Against SARS-CoV-2 S Peptides. A Pilot Study in Health Care Workers. Med. Clin. 2022, 159, 116–123. [Google Scholar] [CrossRef]
- Pedersen, R.M.; Tornby, D.S.; Bistrup, C.; Johansen, I.S.; Andersen, T.E.; Justesen, U.S. Negative SARS-CoV-2 Antibodies, T-Cell Response and Virus Neutralization Following Full Vaccination in a Renal Transplant Recipient: A Call for Vigilance. Clin. Microbiol. Infect. 2021, 27, 1371–1373. [Google Scholar] [CrossRef]
- Van Praet, J.T.; Vandecasteele, S.; De Roo, A.; De Vriese, A.S.; Reynders, M. Humoral and Cellular Immunogenicity of the BNT162b2 Messenger RNA Coronavirus Disease 2019Vaccine in Nursing Home Residents. Clin. Infect. Dis. 2021, 73, 2145–2147. [Google Scholar] [CrossRef]
- Elliott, P.R.; Lennard-Jones, J.E.; Hathway, N. Simple index of Crohn’s disease activity. Lancet 1980, 1, 876. [Google Scholar] [CrossRef]
- Schroeder, K.W.; Tremaine, W.J.; Ilstrup, D.M. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N. Engl. J. Med. 1987, 317, 1625–1629. [Google Scholar] [CrossRef] [PubMed]
- Infantino, M.; Pieri, M.; Nuccetelli, M.; Grossi, V.; Lari, B.; Tomassetti, F.; Calugi, G.; Pancani, S.; Benucci, M.; Casprini, P.; et al. The WHO International Standard for COVID-19 Serological Tests: Towards Harmonization of Anti-Spike Assays. Int. Immunopharmacol. 2021, 100, 108095. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | IBD Patients (n = 53) | HCs (n = 24) |
|---|---|---|
| Gender, male (n, %) | 35 (66) | 14 (58) |
| Age (median [IQR], years) | 52 [42–65] | 50 [39–63] |
| BMI (median [IQR], kg/m2) | 25 [22–28] | 24 [23–26] |
| Active smokers (n, %) | 5 (9) | 5 (21) |
| Type of disease (n, %) | ||
| Crohn’sdisease | 19 (36) | |
| Ulcerative colitis | 34 (64) | |
| Disease activity (median [IQR]) | ||
| HBI score | 4 [0–8] | |
| MS score | 0 [0–0] | |
| Disease localization (n, %) | ||
| Crohn’s disease | ||
| L1 (ileal) | 1 (47) | |
| L2 (colonic) | 4 (21) | |
| L3 (ileocolonic) | 6 (32) | |
| Ulcerative colitis | ||
| E1 (proctitis) | 7 (21) | |
| E2 (left-sided) | 4 (12) | |
| E3 (extensive) | 23 (68) | |
| Disease duration (median [IQR], years) | 11 [5–22] | |
| Treatment regimens (n, %) | ||
| aminosalicylates * | 28 (53) | |
| systemic steroids | 3 (6) | |
| azathioprine | 3 (6) | |
| anti-TNFα | 14 (27) | |
| infliximab | 5 (10) | |
| adalimumab | 3 (6) | |
| golimumab | 6 (11) | |
| vedolizumab | 5 (9) | |
| Comorbidities (n,%) | ||
| None | 32 (60) | 18 (75) |
| 1 | 13 (25) | 5 (21) |
| 2 | 7 (13) | 1 (4) |
| 3 | 1 (2) | 0 (0) |
| Study Cohort Groups | Spearman’s Rank (R, p-Value) | |
|---|---|---|
| IgG/Ag1 | IgG/Ag2 | |
| Healthy controls | 0.5 | 0.6 |
| (p = 0.009) | (p = 0.001) | |
| IBD on anti-TNFαagents | 0.3 | 0.3 |
| (p = 0.2) | (p = 0.4) | |
| IBD on vedolizumab | 0.4 | 0.4 |
| (p = 0.01) | (p = 0.04) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavia, G.; Spagnuolo, R.; Quirino, A.; Marascio, N.; Giancotti, A.; Simeone, S.; Cosco, C.; Tino, E.; Carrabetta, F.; Di Gennaro, G.; et al. COVID-19 Vaccine Booster Shot Preserves T Cells Immune Response Based on Interferon-Gamma Release Assay in Inflammatory Bowel Disease (IBD) Patients on Anti-TNFα Treatment. Vaccines 2023, 11, 591. https://doi.org/10.3390/vaccines11030591
Pavia G, Spagnuolo R, Quirino A, Marascio N, Giancotti A, Simeone S, Cosco C, Tino E, Carrabetta F, Di Gennaro G, et al. COVID-19 Vaccine Booster Shot Preserves T Cells Immune Response Based on Interferon-Gamma Release Assay in Inflammatory Bowel Disease (IBD) Patients on Anti-TNFα Treatment. Vaccines. 2023; 11(3):591. https://doi.org/10.3390/vaccines11030591
Chicago/Turabian StylePavia, Grazia, Rocco Spagnuolo, Angela Quirino, Nadia Marascio, Aida Giancotti, Silvio Simeone, Cristina Cosco, Elena Tino, Federico Carrabetta, Gianfranco Di Gennaro, and et al. 2023. "COVID-19 Vaccine Booster Shot Preserves T Cells Immune Response Based on Interferon-Gamma Release Assay in Inflammatory Bowel Disease (IBD) Patients on Anti-TNFα Treatment" Vaccines 11, no. 3: 591. https://doi.org/10.3390/vaccines11030591