
Vaccinated Yet Booster-Hesitant: Perspectives from Boosted, Non-Boosted, and Unvaccinated Individuals

Abstract
:1. Introduction
2. Methods
2.1. Participant Screening and Recruitment
2.2. Interview Protocol and Strategy
2.3. Data Analysis
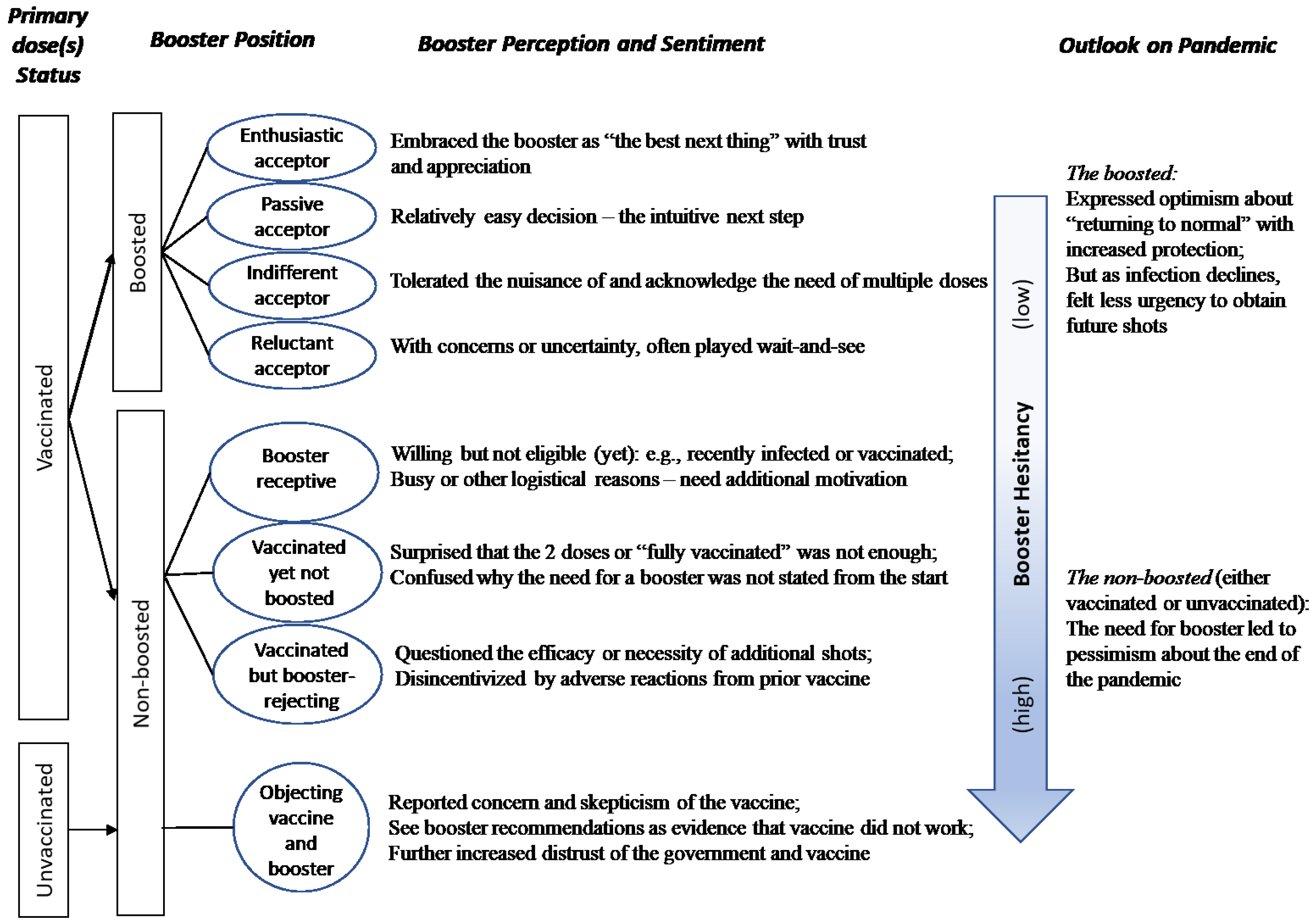
3. Results
3.1. Booster Acceptance & Motivations
“I feel like the booster is literally like (hand motion of blowing up) … we actually get a little dose of superpowers, and we’re able to survive our enemy for a little bit longer.”—Participant #1
“When I heard about the third shot, I said, okay, I want to go ahead and do it.”—#5
“I was very grateful… I want to be under the most protection I can be to be with them [my parents] and not to make them sick.”—#10
“I already got two, so I was like [shrugs shoulders].”—FG1-#2
“Like, oh, I guess I gotta do this right now, ‘cause why did I already did all of the other ones? So why not just finish it up.”—FG1-#5
“I feel like I have been in a way, primed to be okay with getting yearly vaccinations, just because growing up, my parents always took me to my flu shot appointment.”—#11
“It’s sort of like cousins of common cold, the regular flu that you know, an annual booster shot was like… just made sense to me from the get-go.”—#7
“I wonder if we have to take this every year now, like the flu vaccine. Are we going to have to do this every year ….”—FG1-#1
“I’m waiting to see whether there’s something else [side effects] that may come up, then if there’s nothing, then I’ll just take the booster.”—FG2-#3
3.2. Attitudes Surrounding Booster Hesitancy and Rejection
“I was like, okay, is this really necessary? Was this not good enough at first?”—#2
“I understand that it [the booster] can definitely be helpful, but, after a while getting the same exact shots, it’s going to be... I don’t know how efficient that can be.”—#9
“I don’t think it was as important as the initial round of vaccination.”—#4
“I was going to get it, but then I got COVID that same night, so I have to wait 90 days until I’m able to get it.”—FG4-#5
“Other things in life just, just popped into my head… I think after this conversation with everybody, I’m going to go right down on my calendar to make arrangements to get this done.”—FG2-#4
“I have personal concerns because I was affected by the original vaccinations, I had a health issue, and then I just thought about it because it did kind of come on two months after I was fully vaccinated.”—#4
Consequences of the Booster—Increased Distrust
“Why are we forced to do both of them if it [the vaccine] is good?”—FC3-#5
“I think if they had taken the time to develop something, we would just need the vaccine once, and we’d be comfortable with it.”—#6
“I think the booster is just a way of trying to convince us that the COVID-19 vaccine is actually working, which isn’t true.”—FG3-#2
“They thought, well, I’m covered, you know. So, when they came out later on and are like, ‘no, you get to get another booster,’ and I think that just was… a little fishy.”—#3
“I think probably it [the vaccine] is water, drip water or something, because if it has to be topped up every time, then … the effectiveness of it is something that I can question.”—#6
3.3. Booster’s Influence on Perceptions toward the Pandemic and Subsequent Shots
“I feel like after getting a booster and then seeing life return, or like at least life on campus return relatively back to normal.”—#11
“When we got the booster, it was in the height of when the Omicron variant was really rampaging, and that was kind of a rough one. So, I think we were all a little bit more willing to get it because of the variant … I don’t feel as worried about that one. So that’s why I’m not as eager to get my fourth [shot].”—#12
“Anytime you hear booster, it just makes it feel like this is never going to end.”—#3
“I feel like basically, if one shot wasn’t enough to, like, I guess survive the pandemic, then it basically means that you’re gonna need more ‘cause they also don’t see it going anywhere.”—FC3-#4
“Everything is going to go back to normal. And then it’s like, oh, just kidding. We need a booster.”—FC1-#2
4. Discussion
Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- COVID-19 Vaccinations in the United States. Available online: https://covid.cdc.gov/COVID-data-tracker/#vaccinations_vacc-people-additional-dose-totalpop (accessed on 25 October 2022).
- U.S. COVID-19 Map: What Do the Trends Mean for You? Available online: https://www.mayoclinic.org/coronavirus-covid-19/map (accessed on 25 October 2022).
- Klugar, M.; Riad, A.; Mohanan, L.; Pokorná, A. COVID-19 Vaccine Booster Hesitancy (VBH) of Healthcare Workers in Czechia: National Cross-Sectional Study. Vaccines 2021, 9, 1437. [Google Scholar] [CrossRef] [PubMed]
- Kimball, S. Omicron Makes up 95% of Sequenced COVID Cases in U.S. as Infections Hit Pandemic Record. Available online: https://www.cnbc.com/2022/01/04/omicron-makes-up-95percent-of-sequenced-covid-cases-in-us-as-infections-hit-pandemic-record.html (accessed on 17 January 2022).
- Mueller, B. Another COVID Surge May Be Coming. Are We Ready for It? New York Times, 2022. [Google Scholar]
- Omicron BA.5: What We Know about This COVID-19 Strain. Available online: https://health.ucdavis.edu/coronavirus/covid-19-information/omicron-variant (accessed on 25 October 2022).
- FDA Commissioner’s Office FDA Authorizes Booster Dose of Pfizer-BioNTech COVID-19 Vaccine for Certain Populations. Available online: https://www.fda.gov/news-events/press-announcements/fda-authorizes-booster-dose-pfizer-biontech-covid-19-vaccine-certain-populations (accessed on 14 January 2023).
- CDC Strengthens Recommendations and Expands Eligibility for COVID-19 Booster Shots. Available online: https://www.cdc.gov/media/releases/2022/s0519-covid-booster-acip.html (accessed on 2 January 2023).
- Stay up to Date with COVID-19 Vaccines Including Boosters. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/stay-up-to-date.html (accessed on 16 November 2022).
- Pfizer and BioNTech Announce Phase 3 Trial Data Showing High Efficacy of a Booster Dose of Their COVID-19 Vaccine. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-announce-phase-3-trial-data-showing (accessed on 9 February 2023).
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine: A Survey of U.S. Adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once We Have It, Will We Use It? A European Survey on Willingness to Be Vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 Vaccine Acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef] [PubMed]
- Thunstrom, L.; Ashworth, M.; Finnoff, D.; Newbold, S. Hesitancy Towards a COVID-19 Vaccine and Prospects for Herd Immunity. SSRN J. 2020, 1–51. [Google Scholar] [CrossRef]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef]
- Dodd, R.H.; Pickles, K.; Nickel, B.; Cvejic, E.; Ayre, J.; Batcup, C.; Bonner, C.; Copp, T.; Cornell, S.; Dakin, T.; et al. Concerns and Motivations about COVID-19 Vaccination. Lancet Infect. Dis. 2021, 21, 161–163. [Google Scholar] [CrossRef]
- Larson, H.J.; Clarke, R.M.; Jarrett, C.; Eckersberger, E.; Levine, Z.; Schulz, W.S.; Paterson, P. Measuring Trust in Vaccination: A Systematic Review. Hum. Vaccines Immunother. 2018, 14, 1599–1609. [Google Scholar] [CrossRef] [Green Version]
- Vasudevan, V.; Gnanasekaran, A.; Bansal, B.; Lahariya, C.; Parameswaran, G.G.; Zou, J. Assessment of COVID-19 Data Reporting in 100+ Websites and Apps in India. PLoS Glob. Public Health 2022, 2, e0000329. [Google Scholar] [CrossRef]
- Larson, H.J.; de Figueiredo, A.; Xiahong, Z.; Schulz, W.S.; Verger, P.; Johnston, I.G.; Cook, A.R.; Jones, N.S. The State of Vaccine Confidence 2016: Global Insights Through a 67-Country Survey. EBioMedicine 2016, 12, 295–301. [Google Scholar] [CrossRef] [Green Version]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Larson, H.J.; Jarrett, C.; Schulz, W.S.; Chaudhuri, M.; Zhou, Y.; Dube, E.; Schuster, M.; MacDonald, N.E.; Wilson, R. SAGE Working Group on Vaccine Hesitancy Measuring Vaccine Hesitancy: The Development of a Survey Tool. Vaccine 2015, 33, 4165–4175. [Google Scholar] [CrossRef] [Green Version]
- Kumar, D.; Mathur, M.; Kumar, N.; Rana, R.K.; Tiwary, R.C.; Raghav, P.R.; Kumar, A.; Kapoor, N.; Mathur, M.; Tanu, T.; et al. Understanding the Phases of Vaccine Hesitancy during the COVID-19 Pandemic. Isr. J. Health Policy Res. 2022, 11, 16. [Google Scholar] [CrossRef]
- Lahariya, C. Vaccine Epidemiology: A Review. J. Fam. Med. Prim. Care 2016, 5, 7. [Google Scholar] [CrossRef]
- Lahariya, C. A Brief History of Vaccines & Vaccination in India. Indian J. Med. Res. 2014, 139, 491–511. [Google Scholar]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J.A. Vaccine Hesitancy: An Overview. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [Green Version]
- Sorell, T.; Butler, J. The Politics of COVID Vaccine Hesitancy and Opposition. Political Q. 2022, 93, 347–351. [Google Scholar] [CrossRef]
- Troiano, G.; Nardi, A. Vaccine Hesitancy in the Era of COVID-19. Public Health 2021, 194, 245–251. [Google Scholar] [CrossRef]
- Dubé, E.; MacDonald, N.E. How Can a Global Pandemic Affect Vaccine Hesitancy? Expert Rev. Vaccines 2020, 19, 899–901. [Google Scholar] [CrossRef]
- Lai, X.; Zhu, H.; Wang, J.; Huang, Y.; Jing, R.; Lyu, Y.; Zhang, H.; Feng, H.; Guo, J.; Fang, H. Public Perceptions and Acceptance of COVID-19 Booster Vaccination in China: A Cross-Sectional Study. Vaccines 2021, 9, 1461. [Google Scholar] [CrossRef]
- Yadete, T.; Batra, K.; Netski, D.M.; Antonio, S.; Patros, M.J.; Bester, J.C. Assessing Acceptability of COVID-19 Vaccine Booster Dose among Adult Americans: A Cross-Sectional Study. Vaccines 2021, 9, 1424. [Google Scholar] [CrossRef] [PubMed]
- Aboulenein, A.; Kahn, C. Most Vaccinated Americans Want COVID-19 Booster Shots -Reuters/Ipsos Poll. Available online: https://www.reuters.com/business/healthcare-pharmaceuticals/most-vaccinated-americans-want-covid-19-booster-shots-reutersipsos-poll-2021-09-01/ (accessed on 15 January 2023).
- Global Attitudes on COVID-19 Vaccine Booster Shots; Game Changers; Ipsos: Paris, France, 2021.
- Sønderskov, K.M.; Vistisen, H.T.; Dinesen, P.T.; Østergaard, S.D. COVID-19 Booster Vaccine Willingness. Dan. Med. J. 2022, 69, A10210765. [Google Scholar]
- Pal, S.; Shekhar, R.; Kottewar, S.; Upadhyay, S.; Singh, M.; Pathak, D.; Kapuria, D.; Barrett, E.; Sheikh, A.B. COVID-19 Vaccine Hesitancy and Attitude toward Booster Doses among US Healthcare Workers. Vaccines 2021, 9, 1358. [Google Scholar] [CrossRef] [PubMed]
- Perlis, R.H.; Baum, M.; Trujillo, K.L.; Lazer, D.; Safarpour, A.; Druckman, J.; Ognyanova, K.; Santillana, M.; Quintana, A.; Uslu, A.; et al. The COVID States Project #75: Attitudes toward COVID-19 Boosters before and after Omicron; Open Science Framework: Charlottesville, VA, USA, 2021. [Google Scholar]
- Rzymski, P.; Poniedziałek, B.; Fal, A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines 2021, 9, 1286. [Google Scholar] [CrossRef] [PubMed]
- Paul, E.; Fancourt, D. Predictors of Uncertainty and Unwillingness to Receive the COVID-19 Booster Vaccine: An Observational Study of 22,139 Fully Vaccinated Adults in the UK. Lancet Reg. Health-Eur. 2022, 14, 100317. [Google Scholar] [CrossRef]
- Smith-Schoenwalder, C. Slow Updated Booster Shot Uptake Deepens Worry over Future U.S. COVID-19 Surge. Available online: https://www.usnews.com/news/articles/2022-10-14/slow-updated-booster-shot-uptake-deepens-worry-over-future-u-s-covid-19-surge (accessed on 27 October 2022).
- Palinkas, L.A.; Horwitz, S.M.; Green, C.A.; Wisdom, J.P.; Duan, N.; Hoagwood, K. Purposeful Sampling for Qualitative Data Collection and Analysis in Mixed Method Implementation Research. Adm. Policy Ment. Health 2015, 42, 533–544. [Google Scholar] [CrossRef] [Green Version]
- Moser, A.; Korstjens, I. Practical Guidance to Qualitative Research. Part 3: Sampling, Data Collection and Analysis. Eur. J. Gen. Pract. 2018, 24, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Hennink, M.; Kaiser, B.N. Sample Sizes for Saturation in Qualitative Research: A Systematic Review of Empirical Tests. Soc. Sci. Med. 2022, 292, 114523. [Google Scholar] [CrossRef]
- Hennink, M.M.; Kaiser, B.N.; Weber, M.B. What Influences Saturation? Estimating Sample Sizes in Focus Group Research. Qual. Health Res. 2019, 29, 1483–1496. [Google Scholar] [CrossRef]
- Hennink, M.M.; Kaiser, B.N.; Marconi, V.C. Code Saturation Versus Meaning Saturation: How Many Interviews Are Enough? Qual. Health Res. 2017, 27, 591–608. [Google Scholar] [CrossRef]
- QSR International Pty Ltd. NVivo-12; QSR International Pty Ltd.: Burlington, MA, USA, 2020. [Google Scholar]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Alobaidi, S.; Hashim, A. Predictors of the Third (Booster) Dose of COVID-19 Vaccine Intention among the Healthcare Workers in Saudi Arabia: An Online Cross-Sectional Survey. Vaccines 2022, 10, 987. [Google Scholar] [CrossRef]
- Weekly Flu Vaccination Dashboard. Available online: https://www.cdc.gov/flu/fluvaxview/dashboard/vaccination-dashboard.html (accessed on 17 February 2023).
- Mayo Clinic Staff Fully Vaccinated? Get the Facts. Available online: https://www.mayoclinic.org/coronavirus-covid-19/fully-vaccinated (accessed on 29 January 2023).
- Kirzinger, A.; Kearney, A.; Hamel, L.; Brodie, M. KFF COVID-19 Vaccine Monitor: Early Omicron Update. Available online: https://www.kff.org/coronavirus-covid-19/poll-finding/kff-covid-19-vaccine-monitor-early-omicron-update/ (accessed on 21 December 2022).
- Shmueli, L. Predicting Intention to Receive COVID-19 Vaccine among the General Population Using the Health Belief Model and the Theory of Planned Behavior Model. BMC Public Health 2021, 21, 804. [Google Scholar] [CrossRef]
- Dai, H.; Saccardo, S.; Han, M.A.; Roh, L.; Raja, N.; Vangala, S.; Modi, H.; Pandya, S.; Sloyan, M.; Croymans, D.M. Behavioural Nudges Increase COVID-19 Vaccinations. Nature 2021, 597, 404–409. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Variable | n (%) * | |
|---|---|---|
| Age | 18–22 | 4 (12.5%) |
| 23–29 | 8 (25.0%) | |
| 30–39 | 10 (31.3%) | |
| 40–49 | 4 (12.5%) | |
| 50–59 | 6 (18.8%) | |
| Gender | Female | 17 (53.1%) |
| Male | 14 (43.8%) | |
| Prefer not to answer | 1 (3.1%) | |
| Race | African American | 13 (40.6%) |
| Hispanic | 9 (28.1%) | |
| Asian | 5 (15.6%) | |
| White | 4 (12.5%) | |
| Native American | 1 (3.1%) | |
| Household Income (US$) | <$25,000 | 1 (3.1%) |
| $25,000–49,999 | 7 (21.9%) | |
| $50,000–99,999 | 9 (28.1%) | |
| $100,000–$199,999 | 10 (31.2%) | |
| >$200,000 | 4 (12.5%) | |
| Prefer not to answer | 1 (3.1%) |
| Vaccination Status | FG n = 21 | IDI n = 11 | Total n = 32 |
|---|---|---|---|
| Fully vaccinated and received at least one booster | 9 (42.9%) * | 6 (54.5%) | 15 (46.9%) |
| Vaccinated, non-boosted | 6 (28.6%) | 3 (27.3%) | 9 (28.1%) |
| Not vaccinated (non-boosted) | 6 (28.6%) | 2 (18.2%) | 8 (25.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.; Bier, B.; Tu, R.; Paat, J.J.; Tu, P. Vaccinated Yet Booster-Hesitant: Perspectives from Boosted, Non-Boosted, and Unvaccinated Individuals. Vaccines 2023, 11, 550. https://doi.org/10.3390/vaccines11030550
Lin C, Bier B, Tu R, Paat JJ, Tu P. Vaccinated Yet Booster-Hesitant: Perspectives from Boosted, Non-Boosted, and Unvaccinated Individuals. Vaccines. 2023; 11(3):550. https://doi.org/10.3390/vaccines11030550
Chicago/Turabian StyleLin, Cheryl, Brooke Bier, Rungting Tu, John J. Paat, and Pikuei Tu. 2023. "Vaccinated Yet Booster-Hesitant: Perspectives from Boosted, Non-Boosted, and Unvaccinated Individuals" Vaccines 11, no. 3: 550. https://doi.org/10.3390/vaccines11030550