

Clinical and Serological Follow-Up of 216 Patients with Hematological Malignancies after Vaccination with Pfizer-BioNT162b2 mRNA COVID-19 in a Real-World Study
Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Population
2.2. Monitoring of Post-Vaccination Tolerance by Telemedicine
2.3. Serological Follow-Up
2.4. Bio-Medical Follow-Up and Effectiveness
2.5. Statistical Analysis
3. Results
3.1. Patient Population
3.2. Early Assessment of Tolerance Post-Vaccination Follow-Up by Telemedicine
3.3. Comparison between the Tests for Measuring SARS-CoV-2 Spike Antibodies
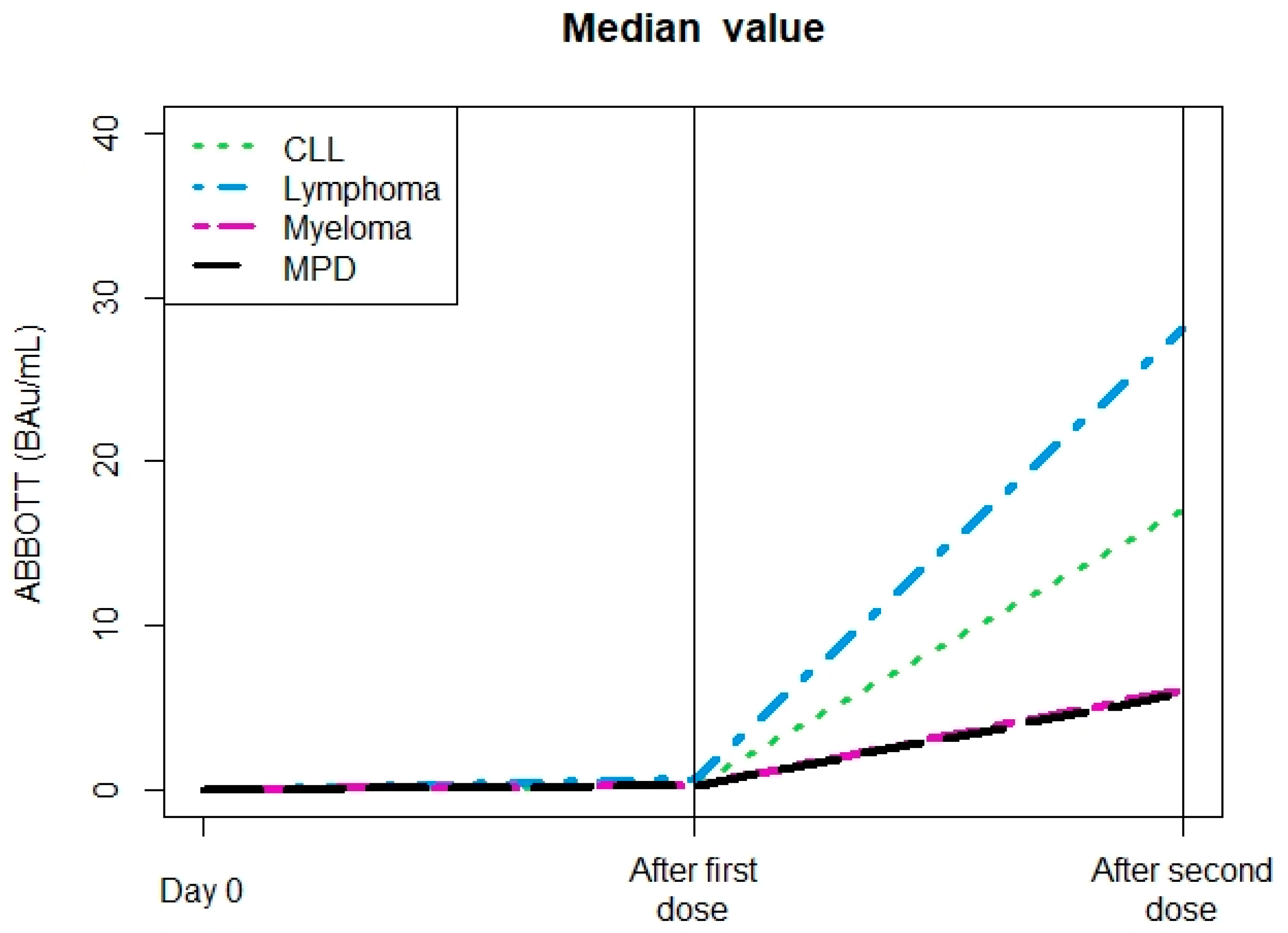
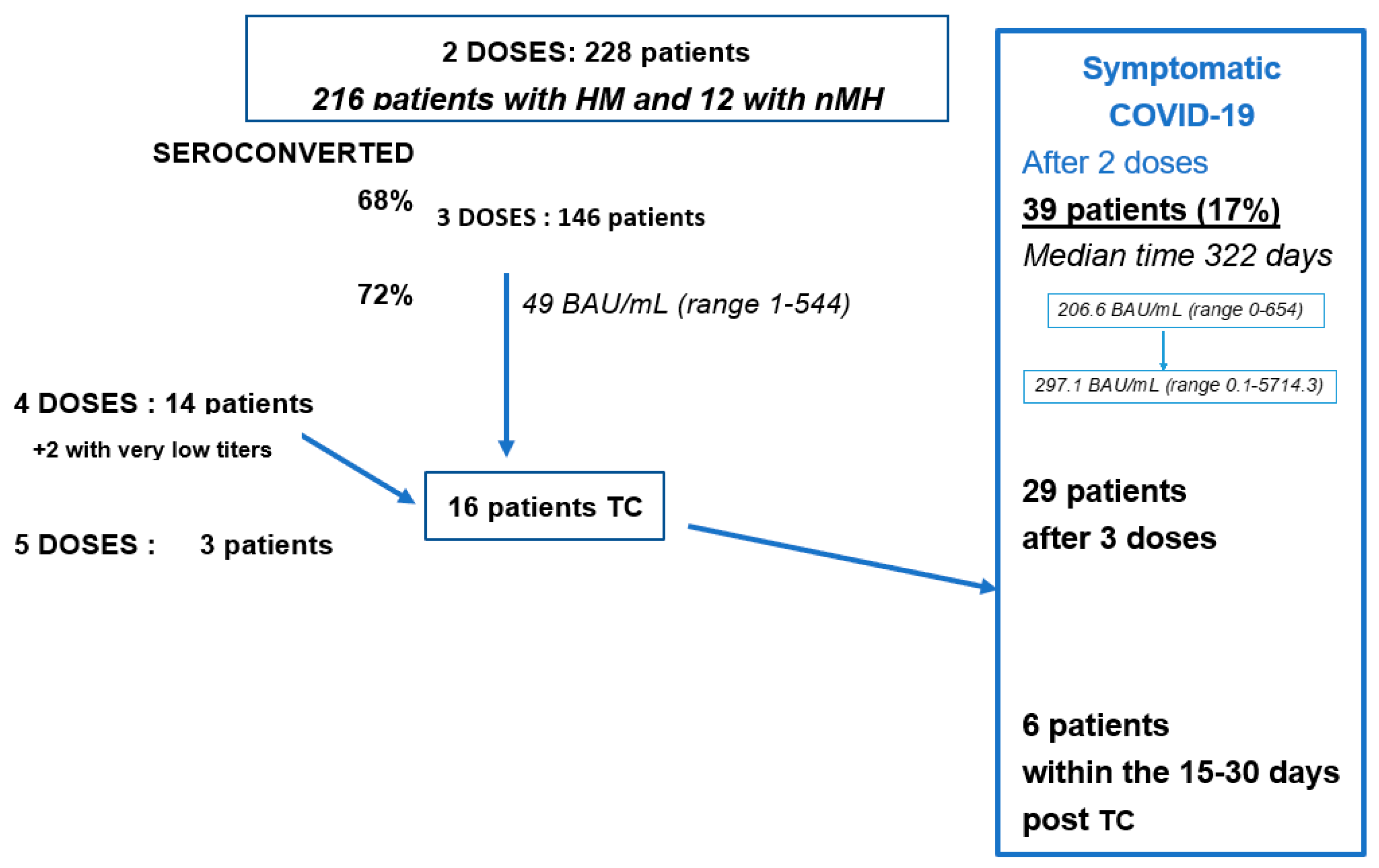
3.4. Seroconversion Levels
3.5. Factors Influencing the Seroconversion
3.6. Bio-Medical Follow-Up and Efficacy
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines/advice (accessed on 17 February 2023).
- Buske, C.; Dreyling, M.; Alvarez-Larrán, A.; Apperley, J.; Arcaini, L.; Besson, C.; Bullinger, L.; Corradini, P.; Della Porta, M.G.; Dimopoulos, M.; et al. Managing hematological cancer patients during the COVID-19 pandemic: An ESMO-EHA Interdisciplinary Expert Consensus. ESMO Open 2022, 7, 100403. [Google Scholar] [CrossRef]
- Issa, N.C.; Baden, L.R. Current issues in vaccines for adult patients with hematological malignancies. J. Natl. Compr. Canc. Netw. 2012, 10, 1447–1454. [Google Scholar] [CrossRef]
- Malard, F.; Gaugler, B.; Gozlan, J.; Bouquet, L.; Fofana, D.; Siblany, L.; Eshagh, D.; Adotevi, O.; Laheurte, C.; Ricard, L.; et al. Weak immunogenicity of SARS-CoV-2 vaccine in patients with hematological malignancies. Blood Cancer J. 2021, 11, 142. [Google Scholar] [CrossRef]
- Perry, C.; Luttwak, E.; Balaban, R.; Shefer, G.; Morales, M.M.; Aharon, A.; Tabib, Y.; Cohen, Y.C.; Benyamini, N.; Beyar-Katz, O.; et al. Efficacy of the BNT 162b2 mRNA COVID-19 vaccine in patients with B-cell non-Hodgkin lymphoma. Blood Adv. 2021, 5, 3053–3061. [Google Scholar] [CrossRef]
- Maneikis, K.; Šablauskas, K.; Ringelevičiūtė, U.; Vaitekėnaitė, V.; Čekauskienė, R.; Kryžauskaitė, L.; Naumovas, D.; Banys, V.; Pečeliūnas, V.; Beinortas, T.; et al. Immunogenicity of the BNT162b2 COVID-19 mRNA vaccine and early clinical outcomes in patients with haematological malignancies in Lithuania: A national prospective cohort study. Lancet Haematol. 2021, 8, e583–e592. [Google Scholar] [CrossRef]
- Nicoli, F.; Clave, E.; Wanke, K.; von Braun, A.; Bondet, V.; Alanio, C.; Douay, C.; Baque, M.; Lependu, C.; Marconi, P.; et al. Primary immune responses are negatively impacted by persistent herpesvirus infections in older people: Results from an observational study on healthy subjects and a vaccination trial on subjects aged more than 70 years old. EBioMedicine 2022, 76, 103852. [Google Scholar] [CrossRef]
- Peireira, B.; Xu, X.N.; Akbar, A.N. Targeting inflammation and immunosenescence to improve vaccine responses in the elderly. Front Immunol. 2020, 11, 583019. [Google Scholar] [CrossRef]
- Ikeda, D.; Terao, T.; Fukumoto, A.; Uesugi, Y.; Tabata, R.; Kuzume, A.; Tsushima, T.; Miura, D.; Narita, K.; Takeuchi, M.; et al. Antibody status following booster vaccination against SARS-CoV-2 virus in patients with hematologic malignancies. Br. J. Haematol. 2023. [Google Scholar] [CrossRef]
- Cook, L.B.; O’Dell, G.; Vourvou, E.; Palanicawandar, R.; Marks, S.; Milojkovic, D.; Apperley, J.F.; Loaiza, S.; Claudiani, S.; Bua, M.; et al. Third primary SARS-CoV-2 mRNA vaccines enhance antibody responses in most patients with haematological malignancies. Nat Comm. 2022, 13, 6922. [Google Scholar] [CrossRef]
- Makady, A.; de Boer, A.; Hillege, H.; Klungel, O.; Goettsch, W.; on behalf of GetReal Work Package 1. What Is Real-World Data? A Review of Definitions Based on Literature and Stakeholder Interviews. Value Health 2017, 20, 858–865. [Google Scholar] [CrossRef] [Green Version]
- Romio, S.; Sturkenboom, M.; Corrao, G. Real-world data from the health decision maker perspective. What are we talking about? Epidemiol. Biostat. Public Health 2013, 10, e8979-1-9. [Google Scholar]
- Pfrommer, L.R.; Schoeps, M.; Blettner, M.; Wollschläger, D.; Herm-Stapelberg, N.; Mittnacht, L.; Kachel, P.; Jahn, K.; von Loewenich, F.D.; Gianicolo, E.A.L. Self-Reported Reactogenicity After Different COVID-19 Vaccination Regimens–An Analysis of Registry-Based Data. Dtsch Arztebl Int. 2022. [Google Scholar] [CrossRef]
- Available online: https://www.senat.fr/fileadmin/Fichiers/Images/opecst/OPECST_2022_rapport_659.pdf (accessed on 17 February 2023).
- Monin, L.; Laing, A.G.; Muñoz-Ruiz, M.; McKenzie, D.R.; del Molino del Barrio, I.; Alaguthurai, T.; Domingo-Vila, C.; Hayday, T.S.; Graham, C.; Seow, J.; et al. Safety and immunogenicity of one versus two doses of the COVID-19 vaccine BNT162b2 for patients with cancer: Interim analysis of a prospective observational study. Lancet Oncol. 2021, 22, 765–778. [Google Scholar] [CrossRef] [PubMed]
- Benitez Fuentes, J.D. Adverse drug reactions to the three doses of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) mRNA-173 vaccine in a cohort of cancer patients under active treatment of a tertiary hospital in Madrid, Spain. F1000Research 2022, 11, 434. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 52, 3127–3141. [Google Scholar] [CrossRef]
- Rinaldi, I.; Pratama, S.; Wiyono, L.; Tandaju, J.R.; Wardhana, I.L.; Winston, K. Serological response to BNT162b2 anti-SARS-CoV-2 vaccination in patients with inflammatory rheumatic diseases: Results from the RHEUVAX cohort. Front. Immunol. 2022, 13, 901055. [Google Scholar]
- Schultz, K.; Jannat-Khah, D.; Spiera, R. B cell reconstitution is associated with COVID-19 booster vaccine responsiveness in patients previously seronegative treated with rituximab. J. Rheumtol. 2023. [Google Scholar] [CrossRef]
- Tolf, A.; Wiberg, A.; Müller, M.; Nazir, F.H.; Pavlovic, I.; Laurén, I.; Mangsbo, S.; Burman, J. Factors associated with serological response to SARS-CoV-2 vaccination in patients with multiple sclerosis treated with rituximab. JAMA Netw Open. 2022, 55, e2211497. [Google Scholar] [CrossRef]
- Rinaldi, I.; Pratama, S.; Wiyono, L.; Tandaju, J.R.; Wardhana, I.L.; Winston, K. Efficacy and safety profile of COVID-19 mRNA vaccine in patients with hematological malignancies: Systematic review and meta-analysis. Front Oncol. 2022, 12, 951215. [Google Scholar] [CrossRef]
- Pinato, D.J.; Tabernero, J.; Bower, M.; Scotti, L.; Patel, M.; Colomba, E.; Dolly, S.; Loizidou, A.; Chester, J.; Mukherjee, U.; et al. Prevalence and impact of COVID-19 sequelae on treatment and survival of patients with cancer who recovered from SARS-CoV-2 infection: Evidence from the OnCovid retrospective, multicentre registry study. Lancet Oncol. 2021, 22, 1669.e80. [Google Scholar] [CrossRef]
- Pinato, D.J.; Ferrante, D.; Aguilar-Company, J.; Bower, M.; Salazar, R.; Mirallas, O.; Sureda, A.; Bertuzzi, A.; Brunet, J.; Lambertini, M.; et al. Vaccination against SARS-CoV-2 protects from morbidity, mortality and sequelae from COVID19 in patients with cancer. Eur. J. Cancer. 2022, 171, 64.e74. [Google Scholar] [CrossRef]
- Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/immuno.html (accessed on 17 February 2023).
- Available online: https://www.ontariohealth.ca/sites/ontariohealth/files/2022-05/Information%20for%20health%20care%20providers%20-%20Evusheld.pdf (accessed on 17 February 2023).
- Available online: https://www.gov.uk/government/news/uks-most-vulnerable-people-to-receive-life-saving-covid-19-treatments-in-the-community (accessed on 17 February 2023).
- Available online: https://ehaweb.org/covid-19/eha-statement-on-covid-19-vaccines/recommendations-for-covid-19-vaccination-in-patients-with-hematologic-cancer/ (accessed on 17 February 2023).
- Levin, M.J. Intramuscular AZD7442 (Tixagevimab-Cilgavimab) for prevention of COVID-19.; PROVENT study group. N. Engl. J. Med. 2022, 386, 2188–2200. [Google Scholar] [CrossRef]
- Akinosoglou, K.; Rigopoulos, E.-A.; Kaiafa, G.; Daios, S.; Karlafti, E.; Ztriva, E.; Polychronopoulos, G.; Gogos, C.; Savopoulos, C. Tixagevimab/cilgavimab in SARS-CoV-2 prophylaxis and therapy: A comprehensive review of clinical experience. Viruses 2023, 15, 118. [Google Scholar] [CrossRef] [PubMed]
- de Lavallade, H.; Garland, P.; Sekine, T.; Hoschler, K.; Marin, D.; Stringaris, K.; Loucaides, E.; Howe, K.; Szydlo, R.; Kanfer, E.; et al. Repeated vaccination is required to optimize seroprotection against H1N1 in the immunocompromised host. Haematologica 2011, 96, 307–314. [Google Scholar] [CrossRef] [Green Version]
- Stuver, R.; Shah, G.L.; Korde, N.S.; Roeker, L.E.; Mato, A.R.; Batlevi, C.L.; Chung, D.J.; Doddi, S.; Falchi, L.; Gyurkocza, B.; et al. Activity of AZD7442 (tixagevimab-cilgavimab) against Omicron SARS-CoV-2 in patients with hematologic malignancies. Cancer Cell. 2022, 40, 590–591. [Google Scholar] [CrossRef]
- Mariotti, J.; Spina, F.; Carniti, C.; Anselmi, G.; Lucini, D.; Vendramin, A.; Pregliasco, F.; Corradini, P. Long-term patterns of humoral and cellular response after vaccination against influenza A (H1N1) in patients with hematological malignancies. Eur. J. Haematol. 2012, 89, 111–119. [Google Scholar] [CrossRef]
- Lee, D.; Jordan, A.I.; Menges, M.A.; Lazaryan, A.; Nishihori, T.; Gaballa, S.R.; Shah, B.D.; Pinilla-Ibarz, J.; Baluch, A.; Klinkova, O.V.; et al. Pneumococcal conjugate vaccine does not induce humoral response when administered within the six months after CD19 CAR T-cell therapy. Transplant Cell Ther. 2022. [Google Scholar] [CrossRef] [PubMed]
- Kos, I.A.; Kiefer, M.; Brill, K.; Cetin, O.; Bittenbring, J.T.; Ahlgrimm, M.; Smola, S.; Lohse, S.; Christofyllakis, K.; Kaddu-Mulindwa, D.; et al. Adaptative humoral response and cellular immune status in cancer patients and patients under immunosuppression vaccinated against SARS-CoV-2. Expert Rev. Vaccines 2022, 21, 1683–1689. [Google Scholar] [CrossRef] [PubMed]
- Zaleska, J.; Kwasnik, P.; Paziewska, M.; Purkot, J.; Szabelak, A.; Jurek, M.; Masny, N.; Dziatkiewicz, I.; Pronobis-Szczylik, B.; Piebiak, A.; et al. Response to anti-SARS-CoV-2 mRNA vaccines in multiple myeloma and chronic lymphocytic leukemia patients. Int. J. Cancer 2022, 152, 705–712. [Google Scholar] [CrossRef]
- Schwarz, M.; Mzoughi, S.; Lozano-Ojalvo, D.; Tan, A.T.; Bertoletti, A.; Guccione, E. T cell immunity is key to the pandemic endgame: How to measure and monitor it. Curr. Res. Immunol. 2022, 3, 215–221. [Google Scholar] [CrossRef]
- Lee, L.Y.; Ionescu, M.C.; Starkey, T.; Little, M.; Tilby, M.; Tripathy, A.R.; Mckenzie, H.S.; Al-Hajji, Y.; Appanna, N.; Barnard, M.; et al. Commercialized kits to assess T-cell responses against SARS-CoV-2 S peptides. A pilot study in health care workers. Med. Clin. 2022, 159, 116–123. [Google Scholar]
- Lee, L.Y.; Ionescu, M.C.; Starkey, T.; Little, M.; Tilby, M.; Tripathy, A.R.; Mckenzie, H.S.; Al-Hajji, Y.; Appanna, N.; Barnard, M.; et al. COVID-19: Third dose booster vaccine effectiveness against breakthrough coronavirus infection, hospitalisations and death in patients with cancer: A population-based study. Eur. J. Cancer 2022, 175, 1–10. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Lymphoma n = 96 | Myeloma n = 33 | MGUS n = 27 | CLL n = 27 | MPD n = 33 | Others n = 12 | Total n = 228 | |
|---|---|---|---|---|---|---|---|
| Age | 71 | 75 | 73 | 72 | 77 | 71 | 73 |
| Median (range) at the second dose | 63–77 | 72–80 | 66–77 | 66–76 | 66–82 | 58–95 | 58–82 |
| Sex M | 54 (56%) | 13 (39%) | 15 (56%) | 18 (67%) | 19 (58%) | 5 (42%) | 124 (54%) |
| Treatment Yes | 43 (55%) | 26 (79%) | 4 (15%) * | 6 (22%) | 21 (64%) | 5 (41%) | 105 (46%) |
| Daratumumab | 7 | 4 * | |||||
| Rituximab | 30 | ||||||
| Nb of pts/dose | |||||||
| Only 2 | 26 (27%) | 9 (27%) | 4 (15%) | 8 (30%) | 17 (52%) | 6 (50%) | 70 (30%) |
| Only 3 | 67 (70%) | 20 (61%) | 23 (85%) | 15 (56%) | 13 (39%) | 6 (50%) | 144 (63%) |
| 4 doses | 3 | 4 | 0 | 4 | 3 | 0 | 14 (6%) |
| Seroconverted after the second dose | 57 (66%) | 19 (61%) | 20 (91%) | 13 (62%) | 24 (80%) | 14 (100%) | 14 (63%) |
| Missing data | 10 | 2 | 5 | 6 | 3 | ||
| Levels of Anti-S Ab Median (IQR) after the second dose (BAU/mL) | 39 0–274 | 15 1–68 | 204 70–896 | 121 1–266 | 50 12–425 | 217 16–1889 | 59 3–319 |
| Seroconverted After Two Doses | Quant® Assay (Roche) | ||||
|---|---|---|---|---|---|
| No | Yes | Total | |||
| Elecsys Quant® Assay (Abbott) | No | 42 (23%) | 12 (6.6%) | 54 (30%) | p < 0.001 |
| Yes | 3 (1.6%) | 125 (69%) | 128 (70%) | ||
| Total | 45 (25%) | 137 (75%) | 182 (100%) | ||
| 97 Samples RST. | Quant® Assay (Mean, Range BAU/mL) | Elecsys® Assay (Mean, Range BAU/mL) | |
|---|---|---|---|
| Negative 52/97 (54%) | 11+ (8.9, 5.8–15.3) | 8+ (8.1, 1.4–24.3) | |
| Positive 45/97 (46%) | 160.7 (0.34–2291.0) | 232.5 (0–>2432) | |
| Reference TITER (Neutralization test 50%) | |||
| 60 | 17/45 (38%) | 23.5 (0.34–66.7) | 46.1 (2.3–220.9) |
| 120 | 7/45 (16%) | 54.1 (19.5–142.3) | 84.9 (8.6–271.4) |
| 300 | 21/45 (46%) | 407.5 (44.5–2291.0) | 465.8 (0–>2432) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, J.-F.; Bonnet, E.; Castelli, C.; Velensek, M.; Wisniewski, E.; Heraud, S.; Boustany, R.; David, C.; Dinet, J.; Sicard, R.; et al. Clinical and Serological Follow-Up of 216 Patients with Hematological Malignancies after Vaccination with Pfizer-BioNT162b2 mRNA COVID-19 in a Real-World Study. Vaccines 2023, 11, 493. https://doi.org/10.3390/vaccines11030493
Rossi J-F, Bonnet E, Castelli C, Velensek M, Wisniewski E, Heraud S, Boustany R, David C, Dinet J, Sicard R, et al. Clinical and Serological Follow-Up of 216 Patients with Hematological Malignancies after Vaccination with Pfizer-BioNT162b2 mRNA COVID-19 in a Real-World Study. Vaccines. 2023; 11(3):493. https://doi.org/10.3390/vaccines11030493
Chicago/Turabian StyleRossi, Jean-François, Emmanuel Bonnet, Christel Castelli, Marion Velensek, Emma Wisniewski, Sophie Heraud, Rania Boustany, Céleste David, Jérôme Dinet, Roland Sicard, and et al. 2023. "Clinical and Serological Follow-Up of 216 Patients with Hematological Malignancies after Vaccination with Pfizer-BioNT162b2 mRNA COVID-19 in a Real-World Study" Vaccines 11, no. 3: 493. https://doi.org/10.3390/vaccines11030493