
Pandemic Fatigue and Vaccine Hesitancy among People Who Have Recovered from COVID-19 Infection in the Post-Pandemic Era: Cross-Sectional Study in China

 ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Pandemic Fatigue
2.3. Attitude toward the Next Dose of COVID-19 Vaccines
2.4. Covariates
2.5. Statistics Analysis
3. Results
3.1. Characteristics of Participants
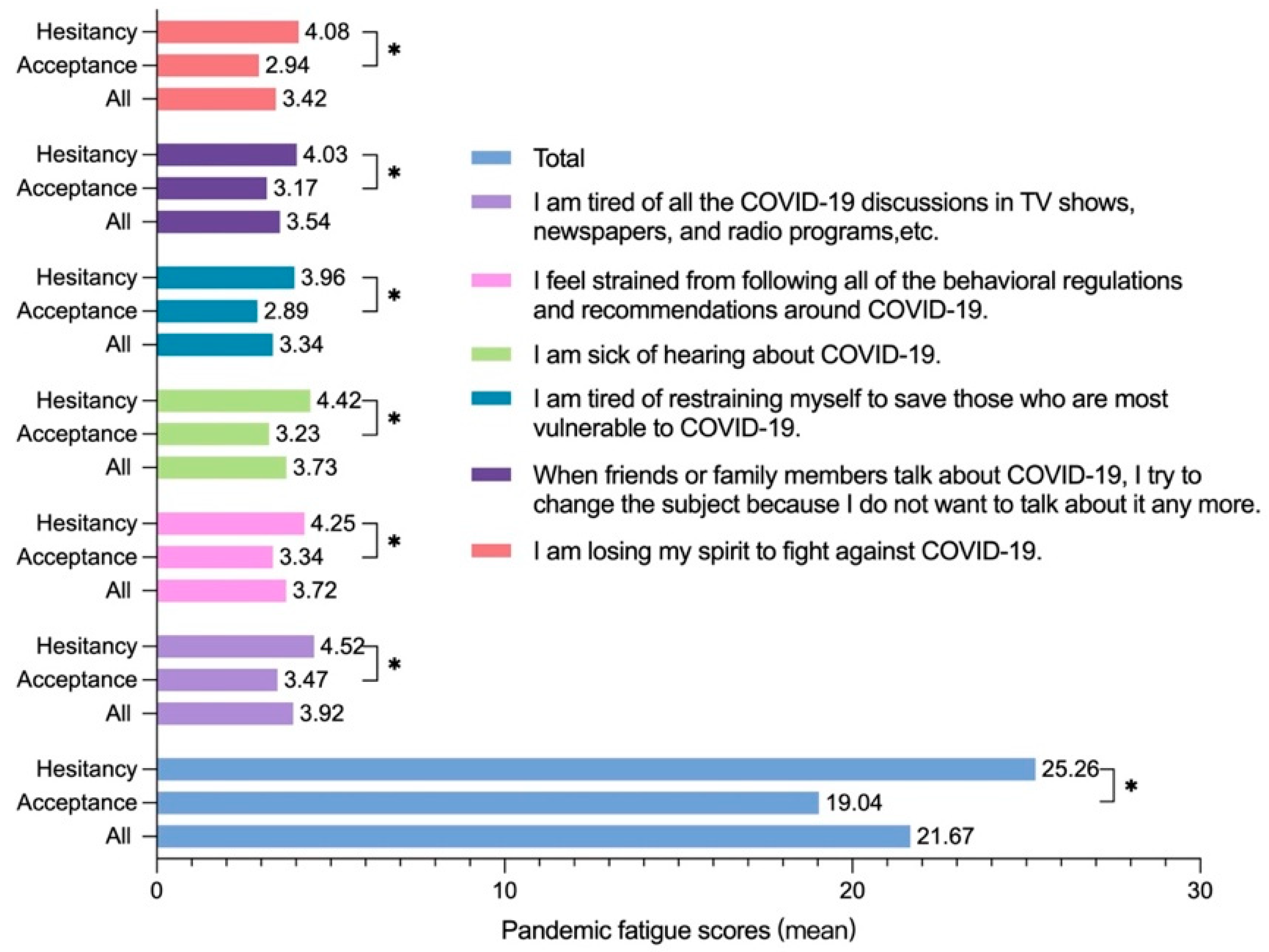
3.2. Pandemic Fatigue in the Post-Pandemic Era
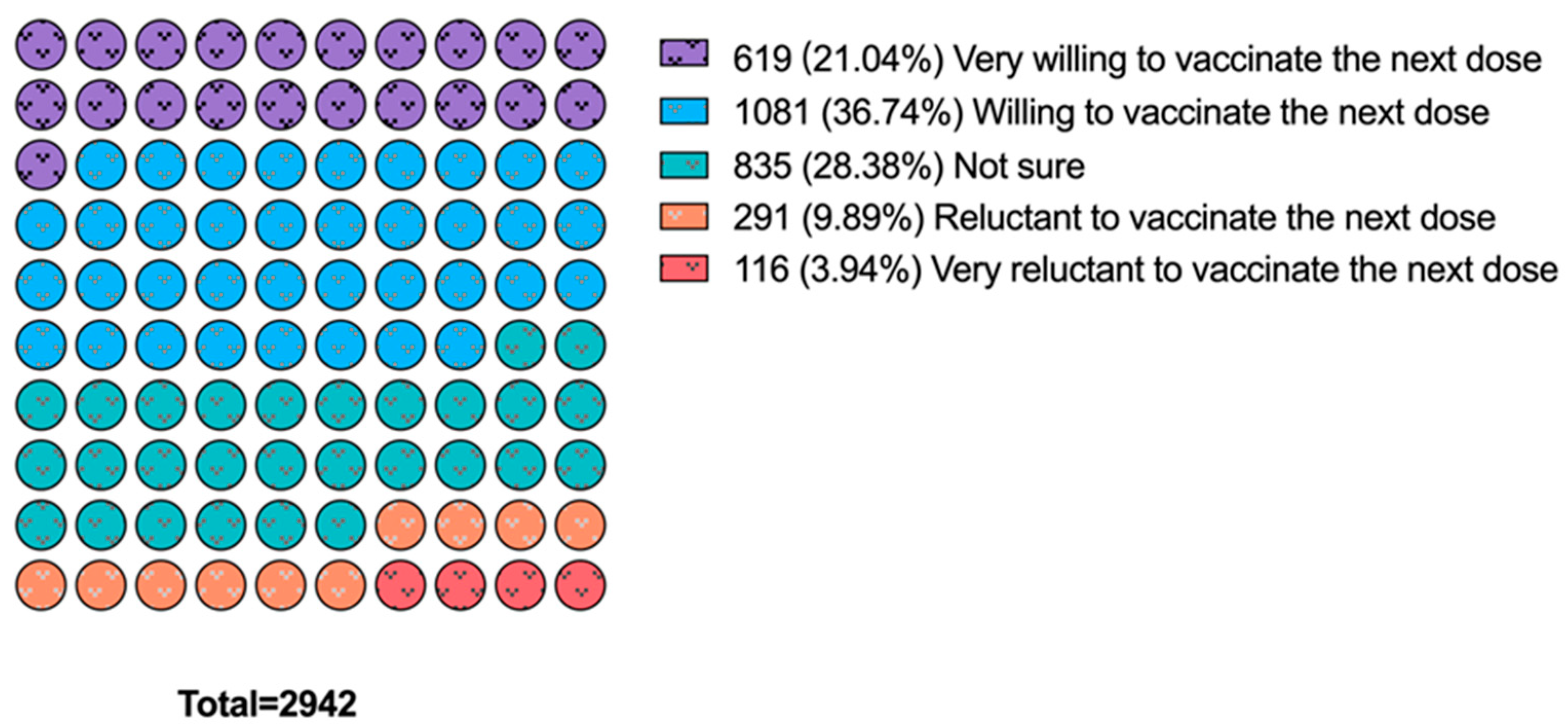
3.3. Vaccine Hesitancy toward the Next Dose of COVID-19 Vaccines
3.4. Association between Pandemic Fatigue and Vaccine Hesitancy toward the Next Dose of COVID-19 Vaccines
3.5. Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. COVID-19 Variants. 2023. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants (accessed on 23 August 2023).
- WHO. COVID-19 Dashboard. 2023. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 23 August 2023).
- The Joint Prevention and Control Mechanism of the State Council. Press Conference of the State Council Joint Prevention and Control Mechanism on 8 May 2023. 2023. Available online: http://www.nhc.gov.cn/xwzb/webcontroller.do?titleSeq=11516&gecstype=1 (accessed on 23 August 2023).
- Fu, D.; He, G.; Li, H.; Tan, H.; Ji, X.; Lin, Z.; Hu, J.; Liu, T.; Xiao, J.; Liang, X.; et al. Effectiveness of COVID-19 Vaccination Against SARS-CoV-2 Omicron Variant Infection and Symptoms—China, December 2022–February 2023. China CDC Wkly. 2023, 5, 369–373. [Google Scholar] [CrossRef] [PubMed]
- WHO. Statement on the Fifteenth Meeting of the IHR (2005) Emergency Committee on the COVID-19 Pandemic. 2023. Available online: https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic (accessed on 23 August 2023).
- Haynes, B.F.; Corey, L.; Fernandes, P.; Gilbert, P.B.; Hotez, P.J.; Rao, S.; Santos, M.R.; Schuitemaker, H.; Watson, M.; Arvin, A. Prospects for a safe COVID-19 vaccine. Sci. Transl. Med. 2020, 12, eabe0948. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J.A. Vaccine hesitancy: An overview. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhang, L.; Fu, J.; Wu, Y.; Wang, H.; Xiao, W.; Xin, Y.; Dai, Z.; Si, M.; Chen, X.; et al. COVID-19 Vaccine Hesitancy Among Patients Recovered From COVID-19 Infection in Wuhan, China: Cross-Sectional Questionnaire Study. JMIR Public Health Surveill. 2023, 9, e42958. [Google Scholar] [CrossRef]
- WHO. Ten Threats to Global Health in 2019. 2020. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 23 August 2023).
- Nuwarda, R.F.; Ramzan, I.; Weekes, L.; Kayser, V. Vaccine Hesitancy: Contemporary Issues and Historical Background. Vaccines 2022, 10, 1595. [Google Scholar] [CrossRef]
- Letizia, A.G.; Ge, Y.; Vangeti, S.; Goforth, C.; Weir, D.L.; Kuzmina, N.A.; Balinsky, C.A.; Chen, H.W.; Ewing, D.; Soares-Schanoski, A.; et al. SARS-CoV-2 seropositivity and subsequent infection risk in healthy young adults: A prospective cohort study. Lancet Respir. Med. 2021, 9, 712–720. [Google Scholar] [CrossRef]
- El-Ghitany, E.M.; Ashour, A.; Omran, E.A.; Farghaly, A.G.; Hassaan, M.A.; Azzam, N.F.A.E.-M. COVID-19 vaccine acceptance rates and predictors among the Egyptian general population and Healthcare workers, the intersectionality of age and other factors. Sci. Rep. 2022, 12, 19832. [Google Scholar] [CrossRef]
- Nguyen, K.H.; Huang, J.; Mansfield, K.; Corlin, L.; Allen, J.D. COVID-19 Vaccination Coverage, Behaviors, and Intentions among Adults with Previous Diagnosis, United States. Emerg. Infect. Dis. 2022, 28, 631–638. [Google Scholar] [CrossRef]
- Bodas, M.; Kaim, A.; Velan, B.; Ziv, A.; Jaffe, E.; Adini, B. Overcoming the effect of pandemic fatigue on vaccine hesitancy—Will belief in science triumph? J. Nurs. Sch. 2023, 55, 262–271. [Google Scholar] [CrossRef]
- Al-Tammemi, A.B.; Tarhini, Z.; Akour, A. A swaying between successive pandemic waves and pandemic fatigue: Where does Jordan stand? Ann. Med. Surg. 2021, 65, 102298. [Google Scholar] [CrossRef]
- Xin, L.; Wang, L.; Cao, X.; Tian, Y.; Yang, Y.; Wang, K.; Kang, Z.; Zhao, M.; Feng, C.; Wang, X.; et al. Prevalence and influencing factors of pandemic fatigue among Chinese public in Xi’an city during COVID-19 new normal: A cross-sectional study. Front. Public Health 2022, 10, 971115. [Google Scholar] [CrossRef]
- Asimakopoulou, E.; Paoullis, P.; Shegani, A.; Argyriadis, A.; Argyriadi, A.; Patelarou, E.; Patelarou, A. Translation, Adaptation and Validation of the Pandemic Fatigue Scale (PFS) in the Greek Language. Healthcare 2022, 10, 2118. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.P.; Alias, H.; Siaw, Y.-L.; Muslimin, M.; Lai, L.L.; Lin, Y.; Hu, Z. Intention to receive a COVID-19 vaccine booster dose and associated factors in Malaysia. Hum. Vaccines Immunother. 2022, 18, 2078634. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Wang, R.; Tao, L.; Liu, M.; Liu, J. Association Between Risk Perception and Acceptance for a Booster Dose of COVID-19 Vaccine to Children Among Child Caregivers in China. Front. Public Health 2022, 10, 834572. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Yan, W.; Du, M.; Liu, Q.; Tao, L.; Liu, M.; Liu, J. Acceptance of the COVID-19 vaccine booster dose and associated factors among the elderly in China based on the health belief model (HBM): A national cross-sectional study. Front. Public Health 2022, 10, 986916. [Google Scholar] [CrossRef]
- Daud, S. The COVID-19 Pandemic Crisis in Malaysia and the Social Protection Program. J. Dev. Soc. 2021, 37, 480–501. [Google Scholar] [CrossRef]
- Star Survey. Sample Service. 2023. Available online: https://www.wjx.cn/sample/service.aspx (accessed on 23 August 2023).
- Qin, C.; Du, M.; Wang, Y.; Liu, Q.; Yan, W.; Tao, L.; Liu, M.; Liu, J. Assessing acceptability of the fourth dose against COVID-19 among Chinese adults: A population-based survey. Hum. Vaccines Immunother. 2023, 19, 2186108. [Google Scholar] [CrossRef]
- Lilleholt, L.; Zettler, I.; Betsch, C.; Böhm, R. Pandemic fatigue: Measurement, correlates, and consequences. PsyArXiv 2020, 1–36. [Google Scholar] [CrossRef]
- Marsella, A.J.; Leong, F.T.L. Cross-Cultural Issues in Personality and Career Assessment. J. Career Assess. 1995, 3, 202–218. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A Decade Later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef]
- Qin, C.; Wang, R.; Tao, L.; Liu, M.; Liu, J. Acceptance of a Third Dose of COVID-19 Vaccine and Associated Factors in China Based on Health Belief Model: A National Cross-Sectional Study. Vaccines 2022, 10, 89. [Google Scholar] [CrossRef]
- Baccolini, V.; Renzi, E.; Isonne, C.; Migliara, G.; Massimi, A.; De Vito, C.; Marzuillo, C.; Villari, P. COVID-19 Vaccine Hesitancy among Italian University Students: A Cross-Sectional Survey during the First Months of the Vaccination Campaign. Vaccines 2021, 9, 1292. [Google Scholar] [CrossRef]
- Liu, Y.; Han, J.; Li, X.; Chen, D.; Zhao, X.; Qiu, Y.; Zhang, L.; Xiao, J.; Li, B.; Zhao, H. COVID-19 Vaccination in People Living with HIV (PLWH) in China: A Cross Sectional Study of Vaccine Hesitancy, Safety, and Immunogenicity. Vaccines 2021, 9, 1458. [Google Scholar] [CrossRef]
- Hong, J.; Xu, X.-W.; Yang, J.; Zheng, J.; Dai, S.-M.; Zhou, J.; Zhang, Q.-M.; Ruan, Y.; Ling, C.-Q. Knowledge about, attitude and acceptance towards, and predictors of intention to receive the COVID-19 vaccine among cancer patients in Eastern China: A cross-sectional survey. J. Integr. Med. 2022, 20, 34–44. [Google Scholar] [CrossRef]
- Hu, S.; Liu, J.; Li, S.; Wu, Q.; Wang, X.; Xu, D.; Chen, Y. Patients with IBD have a more cautious attitude towards COVID-19 vaccination. Front. Immunol. 2023, 13, 1077308. [Google Scholar] [CrossRef]
- Qin, C.; Yan, W.; Tao, L.; Liu, M.; Liu, J. The Association between Risk Perception and Hesitancy toward the Booster Dose of COVID-19 Vaccine among People Aged 60 Years and Older in China. Vaccines 2022, 10, 1112. [Google Scholar] [CrossRef]
- Gerussi, V.; Peghin, M.; Palese, A.; Bressan, V.; Visintini, E.; Bontempo, G.; Graziano, E.; De Martino, M.; Isola, M.; Tascini, C. Vaccine Hesitancy among Italian Patients Recovered from COVID-19 Infection towards Influenza and Sars-Cov-2 Vaccination. Vaccines 2021, 9, 172. [Google Scholar] [CrossRef] [PubMed]
- Petravić, L.; Arh, R.; Gabrovec, T.; Jazbec, L.; Rupčić, N.; Starešinič, N.; Zorman, L.; Pretnar, A.; Srakar, A.; Zwitter, M.; et al. Factors Affecting Attitudes towards COVID-19 Vaccination: An Online Survey in Slovenia. Vaccines 2021, 9, 247. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Yue, Y.; Li, L.; Liu, R.; Zhang, Y.; Zhang, S.; Sang, H.; Tang, M.; Zou, T.; Shah, S.M.; Shen, X.; et al. The dynamic changes of psychosomatic symptoms in three waves of COVID-19 outbreak and fatigue caused by enduring pandemic in China. J. Affect. Disord. 2023, 331, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Ali-Saleh, O.; Bord, S.; Basis, F. Factors Associated with Decisions of Arab Minority Parents in Israel to Vaccinate Their Children against COVID-19. Vaccines 2022, 10, 870. [Google Scholar] [CrossRef] [PubMed]
- WHO. Pandemic Fatigue: Reinvigorating the Public to Prevent COVID-19. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/335820/WHO-EURO-2020-1160-40906-55390-eng.pdf (accessed on 23 August 2023).
- Reicher, S.; Drury, J. Pandemic fatigue? How adherence to covid-19 regulations has been misrepresented and why it matters. BMJ 2021, 372, n137. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics † | Number (%) | Hesitancy Toward the Next Dose of COVID-19 Vaccine | ||
|---|---|---|---|---|
| n (%) | 95% CI | p Value | ||
| Total | 2942 (100) | 1242 (42.2) | 40.4–44.0 | |
| Sex | 0.06 | |||
| Male | 1185 (40.3) | 525 (44.3) | 41.5–47.1 | |
| Female | 1757 (59.7) | 717 (40.8) | 38.5–43.1 | |
| Age (years) | 0.502 | |||
| <30 | 1390 (47.2) | 575 (41.4) | 38.8–44.0 | |
| 30–34 | 790 (26.9) | 337 (42.7) | 39.2–46.1 | |
| 35–39 | 421 (14.3) | 174 (41.3) | 36.7–46.1 | |
| ≥40 | 341 (11.6) | 156 (45.7) | 40.5–51.1 | |
| Location | 0.629 | |||
| Urban | 2662 (90.5) | 1120 (42.1) | 40.2–44.0 | |
| Rural | 280 (9.5) | 122 (43.6) | 37.9–49.4 | |
| Education | 0.960 | |||
| High school and below | 765 (26.0) | 324 (42.4) | 38.9–45.9 | |
| Bachelor’s degree | 1928 (65.5) | 811 (42.1) | 39.9–44.3 | |
| Master’s degree | 249 (8.5) | 107 (43.0) | 36.9–49.2 | |
| Relationship status | 0.001 * | |||
| Without partner | 627 (21.3) | 301 (48.0) | 44.1–51.9 | |
| With partner | 2315 (78.7) | 941 (40.6) | 38.7–42.7 | |
| Smoking | 0.019 * | |||
| No | 2493 (84.7) | 1075 (43.1) | 41.2–45.1 | |
| Yes | 449 (15.3) | 167 (37.2) | 32.8–41.7 | |
| Drinking | 0.488 | |||
| No | 1660 (56.4) | 710 (42.8) | 40.4–45.2 | |
| Yes | 1282 (43.6) | 532 (41.5) | 38.8–44.2 | |
| Chronic disease | 0.880 | |||
| No | 1954 (66.4) | 823 (42.1) | 39.9–44.3 | |
| Yes | 988 (33.6) | 419 (42.4) | 39.4–45.5 | |
| Perceived susceptibility | 0.056 | |||
| Low | 1358 (46.2) | 540 (39.8) | 37.2–42.4 | |
| Moderate | 1204 (40.9) | 531 (44.1) | 41.3–46.9 | |
| High | 380 (12.9) | 171 (45.0) | 40.1–50.0 | |
| Perceived severity | 0.038 * | |||
| Low | 1657 (56.3) | 706 (42.6) | 40.2–45.0 | |
| Moderate | 1000 (34.0) | 439 (43.9) | 40.8–47.0 | |
| High | 285 (9.7) | 97 (34.0) | 28.7–39.7 | |
| Time of the most recent vaccination | <0.001 * | |||
| <6 months | 255 (8.7) | 60 (23.5) | 18.6–29.0 | |
| 6–12 months | 1245 (42.3) | 482 (38.7) | 36.0–41.4 | |
| 12–24 months | 1260 (42.8) | 586 (46.5) | 43.8–49.3 | |
| ≥24 months | 182 (6.2) | 114 (62.6) | 55.5–69.4 | |
| Self-reported long COVID | 0.031 * | |||
| No | 792 (26.9) | 360 (45.5) | 42.0–48.9 | |
| Yes | 2150 (73.1) | 882 (41.0) | 39.0–43.1 | |
| Pandemic fatigue | <0.001 * | |||
| Low | 1196 (40.7) | 290 (24.2) | 21.9–26.7 | |
| Moderate | 1166 (39.6) | 560 (48.0) | 45.2–50.9 | |
| High | 580 (19.7) | 392 (67.6) | 63.7–71.3 | |
| Characteristics † | Pandemic Fatigue (M ± SD) | p Value | Low Pandemic Fatigue | Moderate Pandemic Fatigue | High Pandemic Fatigue | p Value |
|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||||
| Sex | <0.001 * | 0.007 * | ||||
| Male | 22.58 ± 9.01 | 448 (37.8) | 475 (40.1) | 262 (22.1) | ||
| Female | 21.05 ± 8.71 | 748 (42.6) | 691 (39.3) | 318 (18.1) | ||
| Age (years) | 0.447 | 0.019 * | ||||
| <30 | 21.68 ± 8.68 | 538 (38.7) | 598 (43.0) | 254 (18.3) | ||
| 30–34 | 21.93 ± 8.99 | 324 (41.0) | 291 (36.8) | 175 (22.2) | ||
| 35–39 | 21.10 ± 9.18 | 189 (44.9) | 149 (35.4) | 83 (19.7) | ||
| ≥40 | 21.73 ± 8.93 | 145 (42.5) | 128 (37.5) | 68 (19.9) | ||
| Location | 0.004 * | 0.043 * | ||||
| Urban | 21.81 ± 8.90 | 1067 (40.1) | 1056 (39.7) | 539 (20.2) | ||
| Rural | 20.28 ± 8.39 | 129 (46.1) | 110 (39.3) | 41 (14.6) | ||
| Education | 0.160 | 0.030 * | ||||
| High school and below | 21.26 ± 8.74 | 306 (40.0) | 330 (43.1) | 129 (16.9) | ||
| Bachelor’s degree | 21.73 ± 8.90 | 795 (41.2) | 744 (38.6) | 389 (20.2) | ||
| Master’s degree | 22.45 ± 8.93 | 95 (38.2) | 92 (36.9) | 62 (24.9) | ||
| Relationship status | 0.251 | 0.545 | ||||
| Without partner | 21.31 ± 8.95 | 258 (41.1) | 255 (40.7) | 114 (18.2) | ||
| With partner | 21.77 ± 8.84 | 938 (40.5) | 911 (39.4) | 466 (20.1) | ||
| Smoking | 0.002 * | 0.060 | ||||
| No | 21.45 ± 8.84 | 1035 (41.5) | 979 (39.3) | 479 (19.2) | ||
| Yes | 22.86 ± 8.89 | 161 (35.9) | 187 (41.6) | 101 (22.5) | ||
| Drinking | <0.001 * | 0.001 * | ||||
| No | 21.00 ± 8.80 | 712 (42.9) | 658 (39.6) | 290 (17.5) | ||
| Yes | 22.53 ± 8.88 | 484 (37.8) | 508 (39.6) | 290 (22.6) | ||
| Chronic disease | <0.001 * | <0.001 * | ||||
| No | 21.14 ± 8.82 | 837 (42.8) | 780 (39.9) | 337 (17.2) | ||
| Yes | 22.72 ± 8.85 | 359 (36.3) | 386 (39.1) | 243 (24.6) | ||
| Perceived susceptibility | <0.001 * | <0.001 * | ||||
| Low | 21.01 ± 8.97 | 594 (43.7) | 512 (37.7) | 252 (18.6) | ||
| Moderate | 21.78 ± 8.56 | 474 (39.4) | 509 (42.3) | 221 (18.4) | ||
| High | 23.67 ± 9.14 | 128 (33.7) | 145 (38.2) | 107 (28.2) | ||
| Perceived severity | 0.944 | 0.011* | ||||
| Low | 21.63 ± 9.17 | 692 (41.8) | 616 (37.2) | 349 (21.1) | ||
| Moderate | 21.69 ± 8.38 | 385 (38.5) | 440 (44.0) | 175 (17.5) | ||
| High | 21.81 ± 8.73 | 119 (41.8) | 110 (38.6) | 56 (19.6) | ||
| Time of the most recent vaccination | <0.001 * | 0.001 * | ||||
| <6 months | 19.80 ± 8.99 | 129 (50.6) | 87 (34.1) | 39 (15.3) | ||
| 6–12 months | 21.62 ± 8.74 | 510 (41.0) | 495 (39.8) | 240 (19.3) | ||
| 12–24 months | 21.78 ± 8.87 | 505 (40.1) | 502 (39.8) | 253 (20.1) | ||
| ≥24 months | 23.83 ± 9.03 | 52 (28.6) | 82 (45.1) | 48 (26.4) | ||
| Self-reported long COVID | <0.001 * | <0.001 * | ||||
| No | 20.34 ± 9.05 | 386 (48.7) | 266 (33.6) | 140 (17.7) | ||
| Yes | 22.16 ± 8.75 | 810 (37.7) | 900 (41.9) | 440 (20.5) | ||
| Vaccine hesitancy | <0.001 * | <0.001 * | ||||
| No | 19.04 ± 8.17 | 906 (53.3) | 606 (35.6) | 188 (11.1) | ||
| Yes | 25.26 ± 8.52 | 290 (23.3) | 560 (45.1) | 392 (31.6) | ||
| Models | Low Pandemic Fatigue | Moderate Pandemic Fatigue | High Pandemic Fatigue |
|---|---|---|---|
| OR (95%CI) | OR (95%CI) | OR (95%CI) | |
| Model A | 1 (Reference) | 2.89 (2.42, 3.44) * | 6.51 (5.24, 8.11) * |
| Model B | 1 (Reference) | 2.91 (2.44, 3.47) * | 6.56 (5.27, 8.17) * |
| Model C | 1 (Reference) | 2.96 (2.48, 3.53) * | 6.79 (5.44, 8.48) * |
| Model D | 1 (Reference) | 2.92 (2.45, 3.49) * | 6.80 (5.44, 8.50) * |
| Model E | 1 (Reference) | 2.94 (2.46, 3.53) * | 6.88 (5.49, 8.64) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qin, C.; Deng, J.; Du, M.; Liu, Q.; Wang, Y.; Yan, W.; Liu, M.; Liu, J. Pandemic Fatigue and Vaccine Hesitancy among People Who Have Recovered from COVID-19 Infection in the Post-Pandemic Era: Cross-Sectional Study in China. Vaccines 2023, 11, 1570. https://doi.org/10.3390/vaccines11101570
Qin C, Deng J, Du M, Liu Q, Wang Y, Yan W, Liu M, Liu J. Pandemic Fatigue and Vaccine Hesitancy among People Who Have Recovered from COVID-19 Infection in the Post-Pandemic Era: Cross-Sectional Study in China. Vaccines. 2023; 11(10):1570. https://doi.org/10.3390/vaccines11101570
Chicago/Turabian StyleQin, Chenyuan, Jie Deng, Min Du, Qiao Liu, Yaping Wang, Wenxin Yan, Min Liu, and Jue Liu. 2023. "Pandemic Fatigue and Vaccine Hesitancy among People Who Have Recovered from COVID-19 Infection in the Post-Pandemic Era: Cross-Sectional Study in China" Vaccines 11, no. 10: 1570. https://doi.org/10.3390/vaccines11101570