
Analysis of Knowledge, Attitudes and Behaviours of Health Care Workers towards Vaccine-Preventable Diseases and Recommended Vaccinations: An Observational Study in a Teaching Hospital

 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting and Sample
2.3. The Questionnaire
2.4. Sample Size
2.5. Statistical Analysis
3. Results
3.1. Study Population
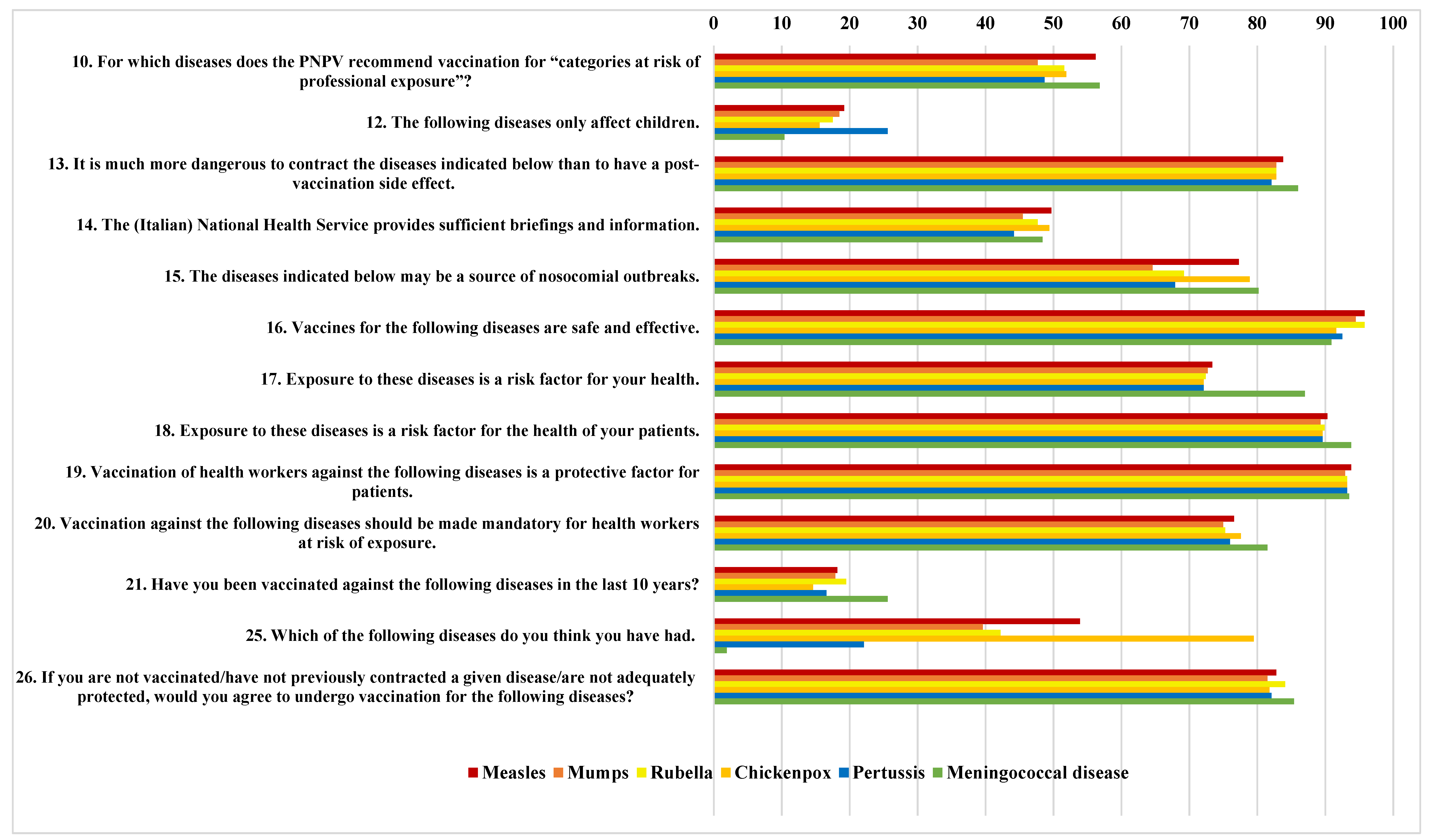
3.2. Descriptive Analysis
3.3. Univariate Analysis
3.4. Multivariate Analysis
3.4.1. Measles
3.4.2. Mumps
3.4.3. Rubella
3.4.4. Chickenpox
3.4.5. Pertussis
3.4.6. Meningococcal Disease
3.4.7. Source of Information
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Durando, P.; Dini, G.; Massa, E.; La Torre, G. Tackling Biological Risk in the Workplace: Updates and Prospects Regarding Vaccinations for Subjects at Risk of Occupational Exposure in Italy. Vaccines 2019, 7, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theodoridou, M. Professional and ethical responsibilities of health-care workers in regard to vaccinations. Vaccine 2014, 32, 4866–4868. [Google Scholar] [CrossRef] [PubMed]
- Sydnor, E.; Perl, T.M. Healthcare providers as sources of vaccine-preventable diseases. Vaccine 2014, 32, 4814–4822. [Google Scholar] [CrossRef] [PubMed]
- Haviari, S.; Bénet, T.; Saadatian-Elahi, M.; André, P.; Loulergue, P.; Vanhems, P. Vaccination of healthcare workers: A review. Hum. Vaccin. Immunother. 2015, 11, 2522–2537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maltezou, H.C.; Botelho-Nevers, E.; Brantsæter, A.B.; Carlsson, R.M.; Heininger, U.; Hübschen, J.M.; Josefsdottir, K.S.; Kassianos, G.; Kyncl, J.; Ledda, C.; et al. Vaccination Policies for HCP in Europe Study Group. Vaccination of healthcare personnel in Europe: Update to current policies. Vaccine 2019, 37, 7576–7584. [Google Scholar] [CrossRef]
- Prato, R.; Tafuri, S.; Fortunato, F.; Martinelli, D. Vaccination in healthcare workers: An Italian perspective. Expert Rev. Vaccines 2010, 9, 277–283. [Google Scholar] [CrossRef]
- Pittet, L.F.; Abbas, M.; Siegrist, C.A.; Pittet, D. Missed vaccinations and critical care admission: All you may wish to know or rediscover—A narrative review. Intensive Care Med. 2020, 46, 202–214. [Google Scholar] [CrossRef]
- Ministerial Circular, Ministry of Health. Ufficio V Prevenzione delle malattie trasmissibili e profilassi internazionale, n. 25223 16/08/2017.
- Karnaki, P.; Baka, A.; Petralias, A.; Veloudaki, A.; Zota, D.; Linos, A. HProImmune Partnership. Immunization related behaviour among healthcare workers in Europe: Results of the HProImmune survey. Cent. Eur. J. Public Health 2019, 27, 204–211. [Google Scholar] [CrossRef] [Green Version]
- Maltezou, H.C.; Theodoridou, K.; Ledda, C.; Rapisarda, V.; Theodoridou, M. Vaccination of healthcare workers: Is mandatory vaccination needed? Expert Rev. Vaccines 2019, 18, 5–13. [Google Scholar] [CrossRef]
- Fefferman, N.H.; Naumova, E.N. Dangers of vaccine refusal near the herd immunity threshold: A modelling study. Lancet Infect Dis. 2015, 15, 922–926. [Google Scholar] [CrossRef]
- Available online: https://cdn.who.int/media/docs/default-source/immunization/immunization_schedules/immunization-routine-table4.pdf?sfvrsn=714e38d6_14&download=true (accessed on 12 January 2023).
- Persone a Rischio per Esposizione Professionale. Available online: https://www.salute.gov.it/portale/vaccinazioni/dettaglioContenutiVaccinazioni.jsp?lingua=italiano&id=4822&area=vaccinazioni&menu=fasce (accessed on 12 January 2023).
- Omer, S.B.; Salmon, D.A.; Orenstein, W.A.; deHart, M.P.; Halsey, N. Vaccine refusal, mandatory immunization, and the risks of vaccine-preventable diseases. N. Engl. J. Med. 2009, 360, 1981–1988. [Google Scholar] [CrossRef]
- Torracinta, L.; Tanner, R.; Vanderslott, S. MMR Vaccine Attitude and Uptake Research in the United Kingdom: A Critical Review. Vaccines 2021, 9, 402. [Google Scholar] [CrossRef]
- Giambi, C.; Fabiani, M.; D’Ancona, F.; Ferrara, L.; Fiacchini, D.; Gallo, T.; Martinelli, D.; Pascucci, M.G.; Prato, R.; Filia, A.; et al. Parental vaccine hesitancy in Italy—Results from a national survey. Vaccine 2018, 36, 779–787. [Google Scholar] [CrossRef]
- Tal, O.; Ne’eman, Y.; Sadia, R.; Shmuel, R.; Schejter, E.; Bitan, M. Parents’ attitudes toward children’s vaccination as a marker of trust in health systems. Hum. Vaccin. Immunother. 2021, 17, 4518–4528. [Google Scholar] [CrossRef]
- Smith, L.E.; Amlôt, R.; Weinman, J.; Yiend, J.; Rubin, G.J. A systematic review of factors affecting vaccine uptake in young children. Vaccine 2017, 35, 6059–6069. [Google Scholar] [CrossRef] [Green Version]
- MacDougall, D.M.; Halperin, B.A.; Langley, J.M.; McNeil, S.A.; MacKinnon-Cameron, D.; Li, L.; Halperin, S.A. Knowledge, attitudes, beliefs, and behaviors of pregnant women approached to participate in a Tdap maternal immunization randomized, controlled trial. Hum. Vaccin. Immunother. 2016, 12, 879–885. [Google Scholar] [CrossRef] [Green Version]
- Lefebvre, M.; Grossi, O.; Chalopin, M.; Ferré, C.; Prel, E.; Coutherut, J.; Briend-Godet, V.; Biron, C.; Raffi, F. Acceptance of pregnant women’s vaccination against pertussis among French women and health professionals: PREVACOQ-1 and -2 studies. Med. Mal. Infect 2019, 49, 593–601. [Google Scholar] [CrossRef]
- Adeyanju, G.C.; Engel, E.; Koch, L.; Ranzinger, T.; Shahid, I.B.M.; Head, M.G.; Elitze, S.; Betsch, C. Determinants of influenza vaccine hesitancy among pregnant women in Europe: A systematic review. Eur. J. Med. Res. 2021, 26, 116. [Google Scholar] [CrossRef]
- Napolitano, F.; Bianco, A.; D’Alessandro, A.; Papadopoli, R.; Angelillo, I.F. Healthcare workers’ knowledge, beliefs, and coverage regarding vaccinations in critical care units in Italy. Vaccine 2019, 37, 6900–6906. [Google Scholar] [CrossRef]
- Pelullo, C.P.; Della Polla, G.; Napolitano, F.; Di Giuseppe, G.; Angelillo, I.F. Healthcare Workers’ Knowledge, Attitudes, and Practices about Vaccinations: A Cross-Sectional Study in Italy. Vaccines 2020, 8, 148. [Google Scholar] [CrossRef]
- La Torre, G.; Scalingi, S.; Garruto, V.; Siclari, M.; Chiarini, M.; Mannocci, A. Knowledge, Attitude and Behaviours towards Recommended Vaccinations among Healthcare Workers. Healthcare 2017, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, N.; Brand, A.; Forstner, C.; Tobudic, S.; Burgmann, K.; Burgmann, H. Knowledge, risk perception and attitudes toward vaccination among Austrian health care workers: A cross-sectional study. Hum. Vaccin. Immunother. 2016, 12, 2459–2463. [Google Scholar] [CrossRef] [Green Version]
- Von Linstow, M.L.; Nordmann Winther, T.; Eltvedt, A.; Bybeck Nielsen, A.; Yde Nielsen, A.; Poulsen, A. Self-reported immunity and opinions on vaccination of hospital personnel among paediatric healthcare workers in Denmark. Vaccine 2020, 38, 6570–6577. [Google Scholar] [CrossRef] [PubMed]
- Tafuri, S.; Gallone, M.S.; Cappelli, M.G.; Martinelli, D.; Prato, R.; Germinario, C. Addressing the anti-vaccination movement and the role of HCWs. Vaccine 2014, 32, 4860–4865. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Poland, G.A. Immunization of Health-Care Providers: Necessity and Public Health Policies. Healthcare 2016, 4, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, S.B.; Skull, S.A. Poor health care worker vaccination coverage and knowledge of vaccination recommendations in a tertiary Australia hospital. Aust. N. Z. J. Public Health 2002, 26, 65–68. [Google Scholar] [CrossRef]
- Montagna, M.T.; De Giglio, O.; Napoli, C.; Fasano, F.; Diella, G.; Donnoli, R.; Caggiano, G.; Tafuri, S.; Lopalco, P.L.; Agodi, A. Gisio-SItI Working Group. Adherence to Vaccination Policy among Public Health Professionals: Results of a National Survey in Italy. Vaccines 2020, 8, 379. [Google Scholar] [CrossRef]
- Tuckerman, J.L.; Collins, J.E.; Marshall, H.S. Factors affecting uptake of recommended immunizations among health care workers in South Australia. Hum. Vaccin. Immunother. 2015, 11, 704–712. [Google Scholar] [CrossRef] [Green Version]
- Betsch, C.; Wicker, S. Personal attitudes and misconceptions, not official recommendations guide occupational physicians’ vaccination decisions. Vaccine 2014, 32, 4478–4484. [Google Scholar] [CrossRef]
- Duong, M.; Mahy, S.; Binois, R.; Buisson, M.; Piroth, L.; Chavanet, P. Couverture vaccinale des professionnels de santé dans un service d’infectiologie [Vaccination coverage of healthcare professionals in an infectious diseases department]. Med. Mal. Infect 2011, 41, 135–139. [Google Scholar] [CrossRef]
- Scatigna, M.; Fabiani, L.; Micolucci, G.; Santilli, F.; Mormile, P.; Giuliani, A.R. Attitudinal variables and a possible mediating mechanism for vaccination practice in health care workers of a local hospital in L’Aquila (Italy). Hum. Vaccin. Immunother. 2017, 13, 198–205. [Google Scholar] [CrossRef]
- Little, K.E.; Goodridge, S.; Lewis, H.; Lingard, S.W.; Din, S.; Tidley, M.; Roberts, R.J.; Williams, N.S.; Hayes, S. Occupational vaccination of health care workers: Uptake, attitudes and potential solutions. Public Health 2015, 129, 755–762. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Katerelos, P.; Poufta, S.; Pavli, A.; Maragos, A.; Theodoridou, M. Attitudes toward mandatory occupational vaccinations and vaccination coverage against vaccine-preventable diseases of health care workers in primary health care centers. Am. J. Infect Control. 2013, 41, 66–70. [Google Scholar] [CrossRef]
- Di Martino, G.; Di Giovanni, P.; Di Girolamo, A.; Scampoli, P.; Cedrone, F.; D’Addezio, M.; Meo, F.; Romano, F.; Di Sciascio, M.B.; Staniscia, T. Knowledge and Attitude towards Vaccination among Healthcare Workers: A Multicenter Cross-Sectional Study in a Southern Italian Region. Vaccines 2020, 8, 248. [Google Scholar] [CrossRef]
- Witteman, H.O. Addressing Vaccine Hesitancy with Values. Pediatrics 2015, 136, 215–217. [Google Scholar] [CrossRef] [Green Version]
- Riccò, M.; Cattani, S.; Casagranda, F.; Gualerzi, G.; Signorelli, C. Knowledge, attitudes, beliefs and practices of occupational physicians towards vaccinations of health care workers: A cross sectional pilot study in North-Eastern Italy. Int. J. Occup. Med. Environ. Health 2017, 30, 775–790. [Google Scholar] [CrossRef]
- Chen, I.H.; Hsu, S.M.; Wu, J.J.; Wang, Y.T.; Lin, Y.K.; Chung, M.H.; Huang, P.H.; Miao, N.F. Determinants of nurses’ willingness to receive vaccines: Application of the health belief model. J. Clin. Nurs. 2019, 28, 3430–3440. [Google Scholar] [CrossRef]
- Lehmann, B.A.; Ruiter, R.A.; van Dam, D.; Wicker, S.; Kok, G. Sociocognitive predictors of the intention of healthcare workers to receive the influenza vaccine in Belgian, Dutch and German hospital settings. J. Hosp. Infect 2015, 89, 202–209. [Google Scholar] [CrossRef]
- Paranthaman, K.; McCarthy, N.; Rew, V.; van Zoelen, S.; Cockerill, L. Pertussis vaccination for healthcare workers: Staff attitudes and perceptions associated with high coverage vaccination programmes in England. Public Health 2016, 137, 196–199. [Google Scholar] [CrossRef]
- Brewer, N.T.; Chapman, G.B.; Gibbons, F.X.; Gerrard, M.; McCaul, K.D.; Weinstein, N.D. Meta-analysis of the relationship between risk perception and health behavior: The example of vaccination. Health Psychol. 2007, 26, 136–145. [Google Scholar] [CrossRef]
- Visser, O.; Hulscher, M.E.J.L.; Antonise-Kamp, L.; Akkermans, R.; van der Velden, K.; Ruiter, R.A.C.; Hautvast, J.L.A. Assessing determinants of the intention to accept a pertussis cocooning vaccination: A survey among healthcare workers in maternity and paediatric care. Vaccine 2018, 36, 736–743. [Google Scholar] [CrossRef] [PubMed]
- Taddei, C.; Ceccherini, V.; Niccolai, G.; Porchia, B.R.; Boccalini, S.; Levi, M.; Tiscione, E.; Santini, M.G.; Baretti, S.; Bonanni, P.; et al. Attitude toward immunization and risk perception of measles, rubella, mumps, varicella, and pertussis in health care workers working in 6 hospitals of Florence, Italy 2011. Hum. Vaccin. Immunother. 2014, 10, 2612–2622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FitzSimons, D.; Hendrickx, G.; Lernout, T.; Badur, S.; Vorsters, A.; Van Damme, P. Incentives and barriers regarding immunization against influenza and hepatitis of health care workers. Vaccine 2014, 32, 4849–4854. [Google Scholar] [CrossRef] [PubMed]
- Borggreve, S.J.; Timen, A. Barriers encountered during the implementation of a policy guideline on the vaccination of health care workers during the 2013–2014 measles outbreak in the Netherlands: A qualitative study. BMC Res. Notes 2015, 14, 780. [Google Scholar] [CrossRef] [Green Version]
- Fortunato, F.; Tafuri, S.; Cozza, V.; Martinelli, D.; Prato, R. Low vaccination coverage among italian healthcare workers in 2013. Hum. Vaccin. Immunother. 2015, 11, 133–139. [Google Scholar] [CrossRef] [Green Version]
- Hakim, H.; Gaur, A.H.; McCullers, J.A. Motivating factors for high rates of influenza vaccination among healthcare workers. Vaccine 2011, 29, 5963–5969. [Google Scholar] [CrossRef]
- Prematunge, C.; Corace, K.; McCarthy, A.; Nair, R.C.; Pugsley, R.; Garber, G. Factors influencing pandemic influenza vaccination of healthcare workers—A systematic review. Vaccine 2012, 30, 4733. [Google Scholar] [CrossRef]


{kind=link}
| Variable | N (%) or Average (DS) |
|---|---|
| Gender | |
| Female | 213 (69.2) |
| Male | 95 (30.8) |
| Age | |
| 20–29 | 76 (24.7) |
| 30–39 | 95 (30–8) |
| 40–49 | 53 (17.2) |
| >50 | 84 (27.3) |
| Marital status | |
| Married/Cohabitant | 131 (42.5) |
| Divorced | 25 (8.1) |
| Unmarried | 147 (47.7) |
| Widowed | 5 (1.6) |
| Children N° | 0.8 (0.4) |
| Occupation | |
| Physicians | 47 (15.3) |
| Nurses | 179 (58.1) |
| Residents | 53 (17.2) |
| Other | 29 (9.4) |
| Employer | |
| Public/University | 270 (87.7) |
| Private | 38 (12.3) |
| Care Unit | |
| Pediatric ICU | 40 (13) |
| Neonatal ICU | 74 (24) |
| Cardiac Surgery ICU | 26 (8.4) |
| General ICU | 93 (30.2) |
| Infectious Disease | 75 (24.4) |
| Years of Service | |
| 0–5 | 128 (41.6) |
| 6–10 | 38 (12.3) |
| 11–20 | 55 (17.9) |
| >20 | 87 (28.2) |
| Years of Service C.U. | |
| 0–5 | 199 (64.6) |
| 6–10 | 26 (8.4) |
| 11–20 | 44 (14.3) |
| >20 | 39 (12.7) |
| Outcome Variable OR–CI 95% | Gender | Age | Marital Status ^ | Occupation * | Care Unit ** | Children | Years of Service | EMPL *** | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | Over 40 | Married/ Cohabitant | Physicians | Nurses | Residents | Gen. ICU | Cardiac | Neon. | Ped. | Yes | Over 10 | Public/Univ | |
| 10_yes | 0.41 (0.24–0.71) | 4.35 (1.56–12.10) | 2.51 (1.05–6.02) | 3.83 (1.32–11.15) | 1.77 (1.02–3.08) | ||||||||
| 12_agree | 3.66 (1.73–7.75) | 0.17 (0.05–0.61) | 0.40 (0.18–0.91) | 0.52 (0.25–1.11) | |||||||||
| 13_agree | 2.29 (1.18–4.46) | 0.42 (0.156–1.128) | 18.02 (2.35–138.36) | 8.52 (1.89–38.45) | 4.03 (0.89–18.23) | 2.79 (1.04–7.50) | |||||||
| 14_agree | 0.31 (0.14 – 0.66) | 2.28 (1.06–4.89) | |||||||||||
| 15_agree | 13.77 (2.39–79.32) | 9.17 (1.88–44.72) | 21.92 (3.74–128.40) | 0.44 (0.19–1.06) | 3.07 (0.89–10.59) | 0.16 (0.03–0.86) | |||||||
| 16_agree | 0.26 (0.05–1.32) | 9.20 (0.94–90.02) | 5.28 (1.34–20.78) | ||||||||||
| 17_agree | 2.16 (0.94–4.97) | 2.60 (0.96–6.99) | 0.36 (0.21–0.61) | ||||||||||
| 18_agree | 8.75 (1.99–38.44) | 0.33 (0.14–0.79) | |||||||||||
| 19_agree | 0.28 (0.08–1.01) | 4.96 (1.10–22.42) | |||||||||||
| 20_agree | 0.38 (0.20–0.73). | 0.45 (0.19–1.06) | 1.78 (0.92–3.45) | ||||||||||
| 21_yes | 1.96 (0.96–4.01) | 0.11 (0.04–0.28) | |||||||||||
| 25_yes | 6.20 (3.61–10.64) | 2.74 (1.15–6.55) | 1.91 (1.05–3.48) | 0.40 (0.18–0.88) | |||||||||
| 26_agree | 0.24 (0.13–0.48) | 0.23 (0.09–0.56) | |||||||||||
| Outcome Variable OR–CI 95% | Gender | Age | Marital Status ^ | Occupation * | Care Unit ** | Children | Years of Service | EMPL *** | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | Over 40 | Married/ Cohabitant | Physicians | Nurses | Residents | Gen. ICU | Cardiac | Neon. | Ped. | Yes | Over 10 | Public/Univ | |
| 10_yes | 1.75 (1.04–2.92) | 3.19 (1.53–6.63) | 0.59 (0.35–0.97) | ||||||||||
| 12_agree | 2.22 (1.09–4.55) | 2.16 (1.10–4.28) | 0.35 (0.13–0.97) | 0.44 (0.20–0.98) | |||||||||
| 13_agree | 2.37 (1.24–4.54) | 5.19 (1.49–18.09) | 11.37 (2.55–50.60) | 4.75 (1.06–21.20) | 1.95 (1.02–3.73) | ||||||||
| 14_agree | 0.39 (0.18–0.83) | 2.34 (1.11–4.95) | |||||||||||
| 15_agree | 9.15 (1.72–48.69) | 7.74 (1.64–36.50) | 17.88 (3.33–96.01) | 0.54 (0.32–0.92) | 2.36 (0.91–6.12) | 0.15 (0.03–0.73) | |||||||
| 16_agree | 3.48 (0.45–26.84) | ||||||||||||
| 17_agree | 0.46 (0.25–0.86) | 1.61 (0.91–2.84) | 3.35 (1.22–9.16) | 0.33 (0.19–0.58) | |||||||||
| 18_agree | 0.40 (0.17–0.91) | 8.35 (1.09–64.22) | 8.47 (1.94–36.97) | ||||||||||
| 19_agree | 0.30 (0.09–0.95) | 2.92 (1.06–8.05) | 0.27 (0.08–0.90) | 5.01 (1.08–23.17) | |||||||||
| 20_agree | 0.47 (0.20–1.08) | 2.74 (1.35–5.56) | 0.37 (0.15–0.91) | ||||||||||
| 21_yes | 0.53 (0.26–1.08) |
2.78 (1.06–7.27) | 4.59 (1.61–13.10) | 0.10 (0.04–0.28) | |||||||||
| 25_yes | 4.58 (2.81–7.48) | ||||||||||||
| 26_agree | 0.24 (0.12–0.45) | 0.25 (0.10–0.62) | |||||||||||
| Outcome Variable OR–CI 95% | Gender | Age | Marital Status ^ | Occupation * | Care Unit ** | Children | Years of Service | EMPL *** | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | Over 40 | Married/ Cohabitant | Physicians | Nurses | Residents | Gen. ICU | Cardiac | Neon. | Ped. | Yes | Over 10 | Public/Univ | |
| 10_yes | 1.65 (0.96–2.84) | 0.61 (0.35–1.08) | 6.81 (1.70–27.20) | 3.11 (0.89–10.93) | 9.38 (2.07–42.41) | 1.87 (1.07–3.29) | 2.20 (0.89–5.39) | 0.42 (0.14–1.22) | |||||
| 12_agree | 0.54 (0.28–1.03) | 2.63 (1.22–5.65) | 2.02 (0.98–4.16) | 0.36 (0.15–0.83) | |||||||||
| 13_agree | 2.13 (1.12–4.07) | 5.01 (1.45–17.37) | 10.71 (2.41–47.61) | 4.64 (1.05–20.59) | 1.75 (0.92–3.33) | ||||||||
| 14_agree | 0.37 (0.18–0.79) | 2.16 (1.02–4.55) | |||||||||||
| 15_agree | 6.46 (1.45–28.71) | 5.15 (1.35–19.67) | 11.49 (2.55–51.84) | 3.08 (1.14–8.33) | 0.29 (0.08–1.09) | ||||||||
| 16_agree | 0.23 (0.06–0.84) | ||||||||||||
| 17_agree | \ | 2.36 (0.94–5.97) | 0.32 (0.19–0.55) | ||||||||||
| 18_agree | 0.39 (0.17–0.90) | 3.56 (0.80–15.90) | 4.88 (1.41–16.85) | ||||||||||
| 19_agree | 0.34 (0.11–1.10) | 2.43 (0.86–6.84) | 0.26 (0.08–0.88) | 4.49 (0.97–20.79) | |||||||||
| 20_agree | 2.43 (1.21–4.87) | 0.25 (0.12–0.49) | |||||||||||
| 21_yes | 2.66 (1.07–6.58) | 3.93 (1.45–10.64) | 0.14 (0.02–1.12) | 0.13 (0.26–1.08) | |||||||||
| 25_yes | 4.71 (2.84–7.79) | 1.62 (0.98–2.69) | 0.48 (0.22–1.05) | ||||||||||
| 26_agree | 0.22 (0.11–0.45) | 0.19 (0.08–0.49) | |||||||||||
| Outcome Variable OR–CI 95% | Gender | Age | Marital Status ^ | Occupation * | Care Unit ** | Children | Years of Service | Empl *** | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | Over 40 | Married/ Cohabitant | Physicians | Nurses | Residents | Gen. ICU | Cardiac | Neon. | Ped. | Yes | Over 10 | Public/Univ | |
| 10_yes | 1.70 (1.02–2.82) | 0.44 (0.27–0.74) | 2.25 (1.08–4.66) | ||||||||||
| 12_agree | 0.37 (0.19–0.71) | 2.79 (1.44–5.40) | 0.37 (0.13–1.04) | ||||||||||
| 13_agree | 4.43 (1.26–15.63) | 4.92 (1.14–21.35) | 0.42 (0.19–0.92) | 2.31 (1.04–5.13) | |||||||||
| 14_agree | 0.49 (0.29–0.80) | 0.51 (0.26–0.98) | |||||||||||
| 15_agree | 10.78 (1.88–61.82) | 10.45 (2.11–51.74) | 20.58 (3.47–121.97) | 0.40 (0.17–0.95) | 4.55 (1.04–19.93) | 0.18 (0.03–0.10) | |||||||
| 16_agree | 0.34 (0.15–0.80) | 3.09 (0.69–13.84) | |||||||||||
| 17_agree | 2.36 (0.94–5.97) | 0.32 (0.19–0.55) | |||||||||||
| 18_agree | 3.32 (0.74–14.79) | 5.48 (1.58–18.96) | 0.46 (0.20–1.04) | ||||||||||
| 19_agree | 0.35 (0.11–1.10) | 2.43 (0.86–6.84) | 0.26 (0.08–0.88) | 4.45 (0.97–20.79) | |||||||||
| 20_agree | 5.08 (1.06–24.37) | 5.34 (1.27–22.49) | 6.52 (1.36–31.32) | 0.41 (0.18–0.97) | 0.15 (0.03–0.69) | ||||||||
| 21_yes | 0.51 (0.24–1.07) | 2.91 (0.99–8.55) | 5.67 (1.79–17.96) | 0.16 (0.02–1.34) | 0.17 (0.06–0.43) | ||||||||
| 25_yes | 1.91 (0.77–4.72) | ||||||||||||
| 26_agree | 0.41 (0.20–0.82) | 3.32 (0.89–12.31) | 0.49 (0.24–1.01) | 0.17 (0.07–0.45) | |||||||||
| Outcome Variable OR–CI 95% | Gender | Age | Marital Status ^ | Occupation * | Care Unit ** | Children | Years of Service | Empl *** | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | Over 40 | Married/ Cohabitant | Physicians | Nurses | Residents | Gen. ICU | Cardiac | Neon. | Ped. | Yes | Over 10 | Public/Univ | |
| 10_yes | 3.02 (1.09–8.37) | 2.38 (0.98–5.78) | 7.02 (2.44–20.20) | 0.45 (0.29–0.82) | |||||||||
| 12_agree | 2.73 (1.15–6.50) | 2.39 (1.19–4.77) | |||||||||||
| 13_agree | 2.32 (1.23–4.39) | 8.51 (1.95–37.07) | 8.68 (2.02–37.23) | 2.71 (0.78–9.41) | |||||||||
| 14_agree | 0.44 (0.21–0.93) | 2.11 (1.01–4.39) | |||||||||||
| 15_agree | 7.12 (1.57–32.19) | 4.60 (1.19–17.77) | 12.75 (2.79–58.35) | 0.61 (0.35–1.07) | 0.46 (0.19–1.11) | 4.62 (1.32–16.12) | 0.28 (0.07–1.10) | ||||||
| 16_agree | 0.46 (0.19–1.15) | 0.42 (0.17–1.06) | |||||||||||
| 17_agree | 1.92 (1.08–3.41) | 4.19 (1.56–11.25) | 2.34 (0.90–6.05) | 0.31 (0.17–0.54) | |||||||||
| 18_agree | 0.38 (0.16–0.90) | 3.53 (0.79–15.87) | 5.88 (0.72–48.28) | 7.93 (1.82–34.57) | |||||||||
| 19_agree | 0.25 (0.07–0.88) | 2.64 (0.94–7.44) | 0.23 (0.07–0.79) | 2.83 (0.76–10.56) | |||||||||
| 20_agree | 4.68 (0.10–22.02) | 4.01 (0.98–16.38) | 3.89 (0.76–19.85) | 0.58 (0.31–1.09) | 0.19 (0.04–0.88) | ||||||||
| 21_yes | 3.12 (1.50–6.47) | 0.11 (0.04–0.33) | |||||||||||
| 25_yes | 1.83 (0.96–3.52) | 2.86 (1.62–5.04) | 0.61 (0.35–1.09) | ||||||||||
| 26_agree | 0.43 (0.17–1.08) | 0.38 (0.17–0.82) | 0.19 (0.08–0.50) | 0.40 (0.15–1.06) | |||||||||
| Outcome Variable OR–CI 95% | Gender | Age | Marital Status ^ | Occupation * | Care Unit ** | Children | Years of Service | Empl *** | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | Over 40 | Married/ Cohabitant | Physicians | Nurses | Residents | Gen. ICU | Cardiac | Neon. | Ped. | Yes | Over 10 | Public/Univ | |
| 10_yes | 1.98 (1.17–3.33) | 0.36 (0.22–0.60) | 2.59 (1.28–5.26) | 3.01 (1.17–7.76) | |||||||||
| 12_agree | 0.37 (0.17–0.80) | 2.2 (0.98–4.94) | 2.47 (0.94–6.51) | ||||||||||
| 13_agree | 2.72 (1.333–5.54) | 2.28 (0.96–5.41) | 9.24 (2.02–42.19) | 0.37 (0.13–1.05) | |||||||||
| 14_agree | 0.42 (0.20–0.87) | 1.87 (0.90–3.88) | |||||||||||
| 15_agree | 6.31 (2.01–19.80) | 4.68 (2.01–10.90) | 5.26 (1.84–15.07) | 0.45 (0.18–1.09) | 3.32 (0.95–11.60) | ||||||||
| 16_agree | 14.29 (1.64–124.23) | 2.78 (1.04–7.43) | 17.32 (1.10–150.17) | 4.39 (0.57–33.95) | |||||||||
| 17_agree | 2.15 (0.89–5.10) | 2.50 (1.04–5.99) | 0.53 (0.25–1.12) | ||||||||||
| 18_agree | 0.35 (0.12–0.02) | ||||||||||||
| 19_agree | 4.19 (0.55–31.98) | ||||||||||||
| 20_agree | 7.08 (1.39–36.00) | 6.73 (1.55–29.19) | 6.94 (1.40–34.39) | 0.38 (0.16–0.92) | 0.16 (0.03–0.80) | ||||||||
| 21_yes | 0.49 (0.26–0.92) | 7.18 (1.40–36.86) | 6.47 (1.38–30.28) | 14.9 (2.10–74.11) | 0.51 (0.27–0.96) | 0.12 (0.02–0.62) | 0.23 (0.12–0.47) | ||||||
| 25_yes | 0.14 (0.02–0.87) | 5.36 (0.96–29.87) | |||||||||||
| 26_agree | 0.23 (0.11–0.48) | 0.22 (0.09–0.54) | |||||||||||
| Outcome Variable OR–CI 95% | Gender | Age | Marital Status ^ | Occupation * | Care Unit ** | Children | Years of Service | Empl *** | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | Over 40 | Married/ Cohabitant | Physicians | Nurses | Residents | Gen. ICU | Cardiac | Neon. | Ped. | Yes | Over 10 | Public/Univ | |
| colleagues_11_yes | 0.64 (0.40–1.02) | 0.63 (0.39–1.02) | 2.55 (1.03–6.28) | 1.72 (0.97–3.03) | 2.76 (1.28–5.92) | ||||||||
| societies_11_yes | 0.41 (0.23–0.74) | 1.74 (1.02–2.95) | 5.16 (1.66–16.05) | 14.35 (3.92–52.48) | |||||||||
| journals_11_yes | 0.41 (0.23–0.76) | 88.81 (18.97–415.72) | 5.46 (1.57–19.00) | 7.73 (1.99–30.04) | 0.54 (0.30–0.96) | ||||||||
| physician_11_yes | 3.98 (2.08–7.65) | 1.96 (0.89–4.32) | 0.52 (0.31–0.90) | 3.76 (1.31–10.43) | 0.24 (0.09–0.64) | ||||||||
| mass_11_yes | 0.30 (0.12–0.74) | 0.13 (0.04–0.43) | 1.66 (0.92–3.00) | ||||||||||
| social_11_yes | 0.15 (0.04–0.67) | 0.16 (0.05–0.55) | 0.48 (0.25–0.92) | ||||||||||
| websites_11_yes | 0.41 (0.21–0.81) | 4.15 (1.42–12.10) | 3.58 (1.53–8.36) | 7.75 (1.81–33.27) | 0.47 (0.21–1.07) | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riccio, M.; Marte, M.; Imeshtari, V.; Vezza, F.; Barletta, V.I.; Shaholli, D.; Colaprico, C.; Di Chiara, M.; Caresta, E.; Terrin, G.; et al. Analysis of Knowledge, Attitudes and Behaviours of Health Care Workers towards Vaccine-Preventable Diseases and Recommended Vaccinations: An Observational Study in a Teaching Hospital. Vaccines 2023, 11, 196. https://doi.org/10.3390/vaccines11010196
Riccio M, Marte M, Imeshtari V, Vezza F, Barletta VI, Shaholli D, Colaprico C, Di Chiara M, Caresta E, Terrin G, et al. Analysis of Knowledge, Attitudes and Behaviours of Health Care Workers towards Vaccine-Preventable Diseases and Recommended Vaccinations: An Observational Study in a Teaching Hospital. Vaccines. 2023; 11(1):196. https://doi.org/10.3390/vaccines11010196
Chicago/Turabian StyleRiccio, Marianna, Mattia Marte, Valentin Imeshtari, Francesca Vezza, Vanessa India Barletta, David Shaholli, Corrado Colaprico, Maria Di Chiara, Elena Caresta, Gianluca Terrin, and et al. 2023. "Analysis of Knowledge, Attitudes and Behaviours of Health Care Workers towards Vaccine-Preventable Diseases and Recommended Vaccinations: An Observational Study in a Teaching Hospital" Vaccines 11, no. 1: 196. https://doi.org/10.3390/vaccines11010196