
Driving Paediatric Vaccine Recovery in Europe

Abstract
:1. Introduction
2. Materials and Methods
2.1. Vaccines Analysed
2.2. Literature Analysis
3. Results
3.1. DTP Vaccine
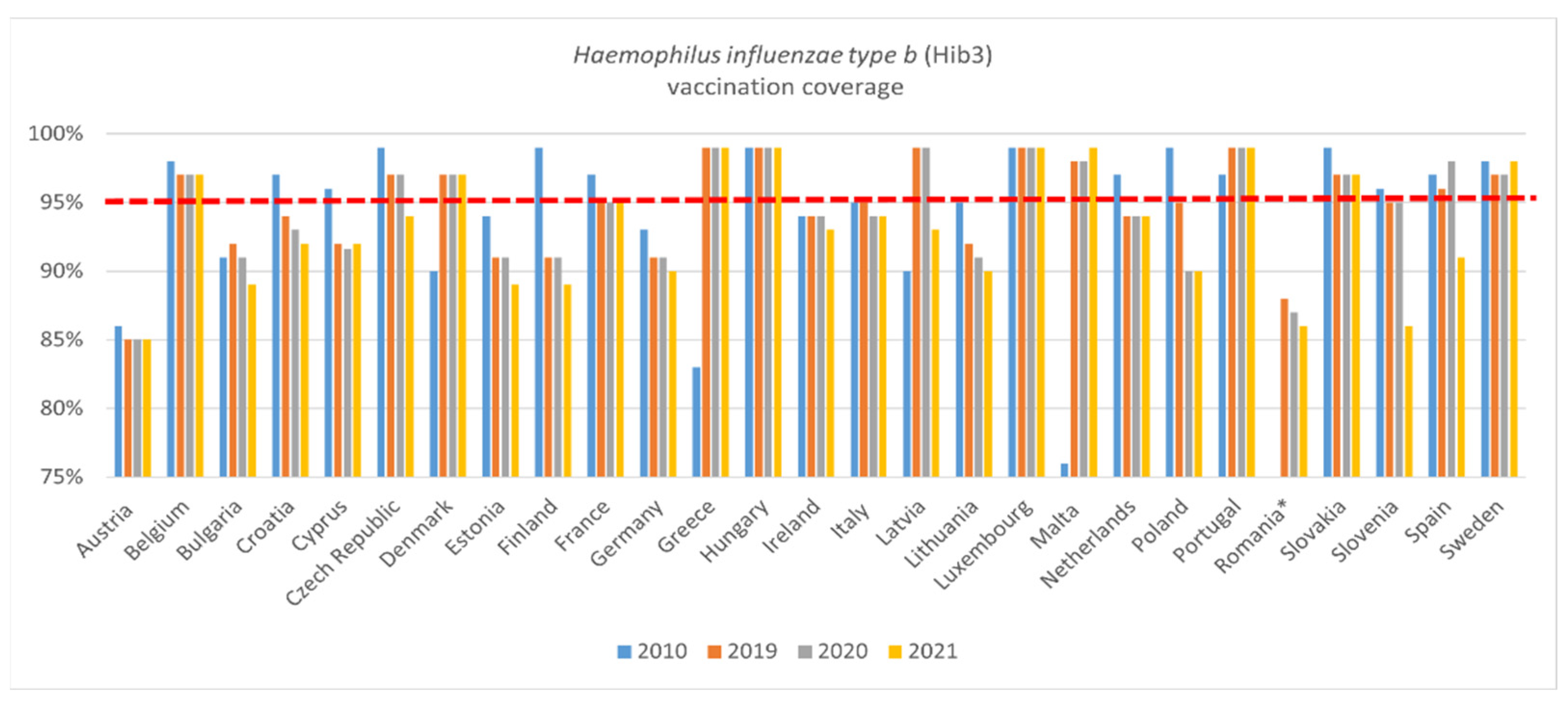
3.2. Hib3 Vaccine
3.3. HepB3 Vaccine
3.4. Measles Vaccine
3.5. Polio Vaccine
4. Discussion
4.1. Vulnerability of Vaccination Systems
4.1.1. Vaccine Misinformation
4.1.2. Vaccine Policies
4.1.3. Vaccine Accessibility
4.2. Current Challenges: The Pandemic and the Ukraine Crisis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Commission. State of Health in the EU: Companion Report. 2017. Available online: https://health.ec.europa.eu/system/files/2017-11/2017_companion_en_0.pdf (accessed on 1 June 2022).
- Rodrigues, C.; Plotkin, S. Impact of Vaccines; Health, Economic and Social Perspectives. Front. Microbiol. 2020, 11, 1526. [Google Scholar] [CrossRef] [PubMed]
- MSD. The Value of Paediatric Vaccination: Protecting Current and Future Generations Across Europe. 2020. Available online: http://www.activecitizenship.net/multimedia/import/files/patients_rights/The_value_of_paediatric_vaccination.pdf (accessed on 1 June 2022).
- Kim, T.H.; Johnstone, J.; Loeb, M. Vaccine herd effect. Scand. J. Infect. Dis. 2011, 43, 683–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bechini, A.; Boccalini, S.; Ninci, A.; Zanobini, P.; Sartor, G.; Bonaccorsi, G. Childhood vaccination coverage in Europe: Impact of different public health policies. Expert Rev. Vaccines 2019, 18, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Thornton, J. Measles cases in Europe tripled from 2017 to 2018. BMJ 2019, 364, I634. [Google Scholar] [CrossRef] [PubMed]
- WHO Europe. Immunisation Strengthens the Fight against Antimicrobial Resistance. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/337523/WHO-EURO-2020-1650-41401-56437-eng.pdf (accessed on 1 June 2022).
- ECDC. Outbreak of Measles in Ukraine and Potential for Spread in the EU. 2012. Available online: https://www.ecdc.europa.eu/sites/default/files/media/en/publications/Publications/20120314_RA_Measles_Ukraine.pdf (accessed on 1 June 2022).
- UNICEF. The Challenge: Moldova Is Facing an Alarming Trend of Declining Vaccine Coverage. Available online: https://www.unicef.org/moldova/en/what-we-do/health/immunization (accessed on 1 June 2022).
- Chiappini, E.; Parigi, S.; Galli, L.; Licari, A.; Brambilla, I.; Tosca, M.A.; Ciprandi, G.; Marseglia, G. Impact that the COVID-19 pandemic on routine childhood vaccinations and challenges ahead: A narrative review. Acta Paediatr. 2021, 110, 2529–2535. [Google Scholar] [CrossRef] [PubMed]
- WHO. COVID-19 Pandemic Fuels Largest Continued Backslide in Vaccinations in Three Decades. 2022. Available online: https://www.who.int/news/item/15-07-2022-covid-19-pandemic-fuels-largest-continued-backslide-in-vaccinations-in-three-decades (accessed on 5 June 2022).
- WHO. Guidance on Vaccination and Prevention of Vaccine-Preventable Disease Outbreaks for Countries Hosting Refugees from Ukraine. 2022. Available online: https://apps.who.int/iris/bitstream/handle/10665/353408/WHO-EURO-2022-5321-45085-64306-eng.pdf (accessed on 5 June 2022).
- WHO. The Guide to Tailoring Immunisation Programmes (TIP). 2013. Available online: https://www.euro.who.int/__data/assets/pdf_file/0003/187347/The-Guide-to-Tailoring-Immunization-Programmes-TIP.pdf (accessed on 5 June 2022).
- UN. Vaccinations Create ‘Umbrella of Immunity’ against Global Measles Outbreaks. 2019. Available online: https://news.un.org/en/story/2019/04/1037271 (accessed on 1 July 2022).
- WHO. Immunization Data. Available online: https://immunizationdata.who.int/listing.html?topic=&location= (accessed on 1 July 2022).
- European Observatory on Health Systems and Policies. The Organisation and Delivery of Vaccination Services in the European Union. ISBN 978-92-890-5173-6. 2018. Available online: https://health.ec.europa.eu/system/files/2018-11/2018_vaccine_services_en_0.pdf (accessed on 5 June 2022).
- European Commission. State of Vaccine Confidence in the EU 2018; European Commission: Brussels, Belgium, 2018. [Google Scholar] [CrossRef]
- Deleanu, D.; Petricau, C.; Leru, P.; Chiorean, I.; Muntean, A.; Dumitrascu, D.; Nedelea, I. Knowledge influences attitudes toward vaccination in Romania. Exp. Ther. Med. 2019, 18, 5088–5094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Commission. State of Vaccine Confidence in the European Union 2022; European Commission: Brussels, Belgium, 2022. [Google Scholar] [CrossRef]
- Del Duca, E.; Chini, L.; Graziani, S.; Sgrulletti, M.; Moschese, V.; The Italian Pediatric Immunology and Allergology Society (SIAIP) Vaccine Committee. Pediatric health care professionals’ vaccine knowledge, awareness and attitude: A survey within the Italian Society of Pediatric Allergy and Immunology. Ital. J. Pediatr. 2021, 47, 183. [Google Scholar] [CrossRef] [PubMed]
- Facciola, A.; Visalli, G.; Orlando, A.; Bertuccio, M.P.; Spataro, P.; Squeri, R.; Picerno, I.; Di Pietro, A. Vaccine Hesitancy: An Overview on Parents’ Opinions about Vaccination and Possible Reasons of Vaccine Refusal. J. Public Health Res. 2019, 8, 13–18. [Google Scholar] [CrossRef] [PubMed]
- ASSET. Vaksinko: An Informational Campaign about Vaccines in Bulgaria. Available online: http://www.asset-scienceinsociety.eu/outputs/best-practice-platform/vaksinko-informational-campaign-about-vaccines-bulgaria (accessed on 1 June 2022).
- ECDC. Vaccine Scheduler—Malta: Recommended Vaccinations. Available online: https://vaccine-schedule.ecdc.europa.eu/ (accessed on 1 June 2022).
- Kuznetsova, L.; Cortassa, G.; Trilla, A. Effectiveness of Mandatory and Incentive-Based Routine Childhood Immunisation Programs in Europe: A Systematic Review of the Literature. Vaccines 2021, 9, 1173. [Google Scholar] [CrossRef] [PubMed]
- Sindoni, A.; Baccolini, V.; Adamoa, G.; Massimi, A.; Migliaraa, G.; De Vito, C.; Marzuilloa, C.; Villari, P. Effect of the mandatory vaccination law on measles and rubella incidence and vaccination coverage in Italy (2013–2019). Hum. Vaccines Immunother. 2021, 18, e1950505. [Google Scholar] [CrossRef] [PubMed]
- Danish Health Authority. The Danish Childhood Vaccination Programme. 2018. Available online: https://www.sst.dk/-/media/Udgivelser/2019/Boernevaccinationsprogrammet-pjece/Boernevaccinationsprogrammet-pjece-engelsk.ashx?la=da&hash=AD719DD0708DD179EF7BC39D2F180D44D11F0211 (accessed on 1 June 2022).
- WHO. Vaccination and Trust: How Concerns Arise and the Role of Communication in Mitigating Crises. 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/204500/9789241510103_eng.pdf (accessed on 1 June 2022).
- Romanian Ministry of Health. Ordinul nr. 386/2015 Privind Aprobarea Normelor Tehnice de Realizare a Programelor Naţionale de Sănătate Publică Pentru anii 2015 şi 2016. 2015. Available online: https://www.dspbihor.gov.ro/legislatie/Ordin%20386%202015%20si%20Norma%20tehnica%20actualizat%2013022017.pdf (accessed on 1 June 2022).
- Baldo, V.; Bonanni, P.; Castro, M.; Gabutti, G.; Franco, E.; Marchetti, F.; Prato, R.; Vitale, F. Combined hexavalent diphtheria-tetanus-acellular pertussis-hepatitis B-inactivated poliovirus-Haemophilus influenzae type b vaccine; Infanrix™ hexa. Hum. Vaccines Immunother. 2014, 10, 129–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Global Routine Immunisation Strategies and Practices (GRISP). 2016. Available online: https://apps.who.int/iris/bitstream/handle/10665/204500/9789241510103_eng.pdf (accessed on 5 June 2022).
- Guthmann, J.P.; Fonteneau, L.; Collet, M.; Vilain, A.; Ragot, M.; Boutieb, M.B.; Guignon, N.; Urcun, J.-M.; Lévy-Bruhl, D. Hepatitis B vaccination coverage among children in France in 2014: Substantial progress in infants, stagnation in adolescents. Bull. Épidémiologique Hebd. 2015, 26, 499–504. Available online: http://beh.santepubliquefrance.fr/beh/2015/26-27/pdf/2015_26-27_4.pdf (accessed on 1 June 2022).
- EPI-PHARE. COVID-19: Usage des Médicaments de Ville en France—Point de Situation Jusqu’au 25 avril 2021. 2021. Available online: https://www.epi-phare.fr/app/uploads/2021/05/epi-phare_rapport_6_medicaments_covid_20210527.pdf (accessed on 1 June 2022).
- Ethnos. Dramatic Reduction in Coronavirus Vaccinations in Children—Expert Warnings. 29 March 2021. Available online: https://www.ethnos.gr/health/article/151432/dramatikhmeioshstoysemboliasmoystonpaidionlogokoronoioyoiproeidopoihseistoneidikon (accessed on 5 June 2022).
- WHO. COVID-19 Continues to Disrupt Essential Health Services in 90% of Countries. 21 April 2021. Available online: https://www.who.int/news/item/23-04-2021-covid-19-continues-to-disrupt-essential-health-services-in-90-of-countries (accessed on 5 June 2022).
- WHO Europe. Emergency in Ukraine: External Situation Report #7; WHO Europe: København, Denmark, 2022. [Google Scholar]
- Shet, A.; Carr, K.; Danovaro-Holliday, C.; Sodha, S.; Prosperi, C.; Wunderlich, J.; Wonodi, C.; Reynolds, H.; Mirza, I.; Gacic-Dobo, M.; et al. Impact of the SARS-CoV-2 pandemic on routine immunisation services: Evidence of disruption and recovery from 170 countries and territories. Lancet 2022, 10, e186–e194. [Google Scholar] [CrossRef] [PubMed]
- Stefanati, A.; d’Anchera, E.; De Motoli, F.; Savio, M.; Toffoletto, M.V.; Gabutti, G. Value of Immunisations during the COVID-19 Emergency. Int. J. Environ. Res. Public Health 2021, 18, 778. [Google Scholar] [CrossRef] [PubMed]
- World Federation of Public Health Associations. Policy Statement: Driving Pediatric Vaccines Recovery in Europe. Available online: https://kdrive.infomaniak.com/app/share/141741/8c4e56c4-6620-4c77-8095-e967707d8c8a/files/40333/preview/pdf/47204 (accessed on 1 November 2022).
- Romanian Ministry of Health. Ordin Nr. 422 din 29 Martie 2013 Privind Aprobarea Normelor Tehnice de Realizare a Programelor Naţionale de Sănătate Publică Pentru Anii 2013 şi 2014*, 201. Available online: https://www.rndvcsh.ro/files/documents/MO%20173bis_2013.pdf (accessed on 5 June 2022).
- European Commission. Fighting Disinformation. Available online: https://ec.europa.eu/info/live-work-travel-eu/coronavirus-response/fighting-disinformation_en (accessed on 1 June 2022).
- Romanian Ministry of Health. Information on Mandatory Vaccinations in the Vaccination Calendar. 26 January 2017. Available online: https://www.ms.ro/2017/01/26/informare-privind-situatia-imunizarii-copiilor-cu-vaccinurile-obligatorii-din-calendarul-de-vaccinare-se-desfasoara-cu-unele-deficiente/ (accessed on 1 June 2022).
- Causey, K.; Fullman, N.; Sorensen, R.; Galles, N.; Zheng, P.; Aravkin, A.; Danovaro-Holliday, C.; Martinez-Piedra, R.; Sodha, S.; Velandia-González, M.P.; et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: A modelling study. Lancet 2021, 398, 522–534. [Google Scholar] [CrossRef] [PubMed]
- Partouche, H.; Gilberg, S.; Renard, V.; Saint-Lary, O. Mandatory vaccination of infants in France: Is that the way forward? Eur. J. Gen. Pract. 2019, 25, 49–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vojtek, I.; Larson, H.; Plotkin, S.; Van Damme, P. Evolving measles status and immunisation policy development in six European countries. Hum. Vaccines Immunother. 2022, 18, 2031776. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Protecting Children against Measles in Romania. 2019. Available online: https://www.unicef.org/eca/stories/protecting-children-against-measles-romania (accessed on 1 June 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Barriers | Enablers |
|---|---|
| Structural barriers (e.g., having to take time off work to get a child vaccinated) [27] | Easy access to vaccine administration [16,39] |
| Delays in vaccine procurement [16,40,41] | Outreach services and catch-up campaigns [16,42] |
| Vaccine hesitancy (among public and/or health care professional) [16,40] | Vaccination policies (depending on local context) [24,40,43,44] |
| Spread of misinformation about vaccination [16] | Real-time systematic data collection [37] |
| Communication between individuals and healthcare workers regarding vaccines [16,22] | |
| Sending vaccine reminders to parents [26] | |
| Awareness raising and education campaigns [16] | |
| Easily accessible and reliable information materials about vaccination [22,45] |
| Recommendations | |
|---|---|
| General | Specific |
| Facilitate access to vaccination | Increase range of providers to administer vaccination |
| Enable providers to administer vaccinations outside of the site where they are employed (e.g., administer vaccines at childcare facilities) | |
| Additional hours to access vaccinations (e.g., outside of regular work hours) | |
| Develop mitigation strategies and plans to respond to VPD outbreak | Ensure sufficient infrastructure and health worker capacity |
| Increase use of digital technologies | Improve real-time data collection and disease surveillance systems |
| Electronic immunisation records | |
| Automated vaccination reminders | |
| Improve education and awareness regarding the value of vaccination | Public awareness and communication campaigns |
| Public health education programmes | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alexander, C.; Cabrera, M.; Moore, M.; Lomazzi, M. Driving Paediatric Vaccine Recovery in Europe. Vaccines 2023, 11, 184. https://doi.org/10.3390/vaccines11010184
Alexander C, Cabrera M, Moore M, Lomazzi M. Driving Paediatric Vaccine Recovery in Europe. Vaccines. 2023; 11(1):184. https://doi.org/10.3390/vaccines11010184
Chicago/Turabian StyleAlexander, Claire, Mariel Cabrera, Michael Moore, and Marta Lomazzi. 2023. "Driving Paediatric Vaccine Recovery in Europe" Vaccines 11, no. 1: 184. https://doi.org/10.3390/vaccines11010184